

Abstract
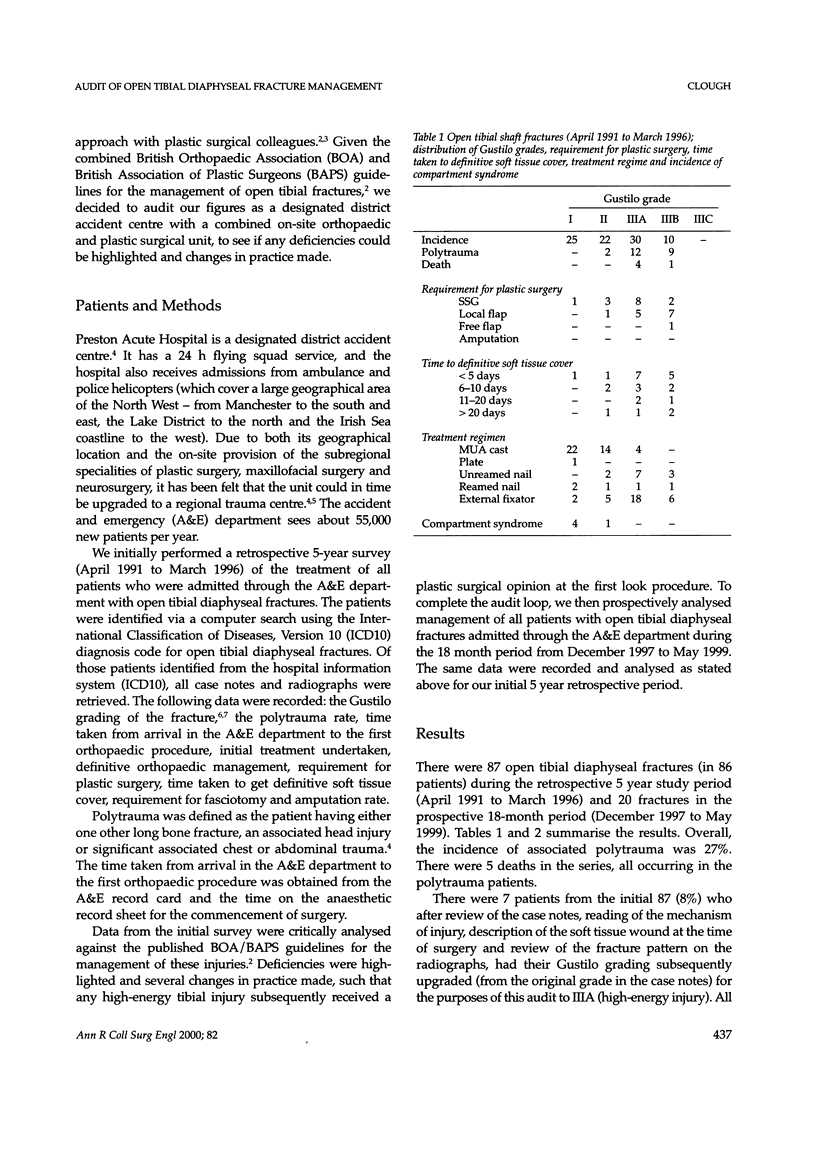
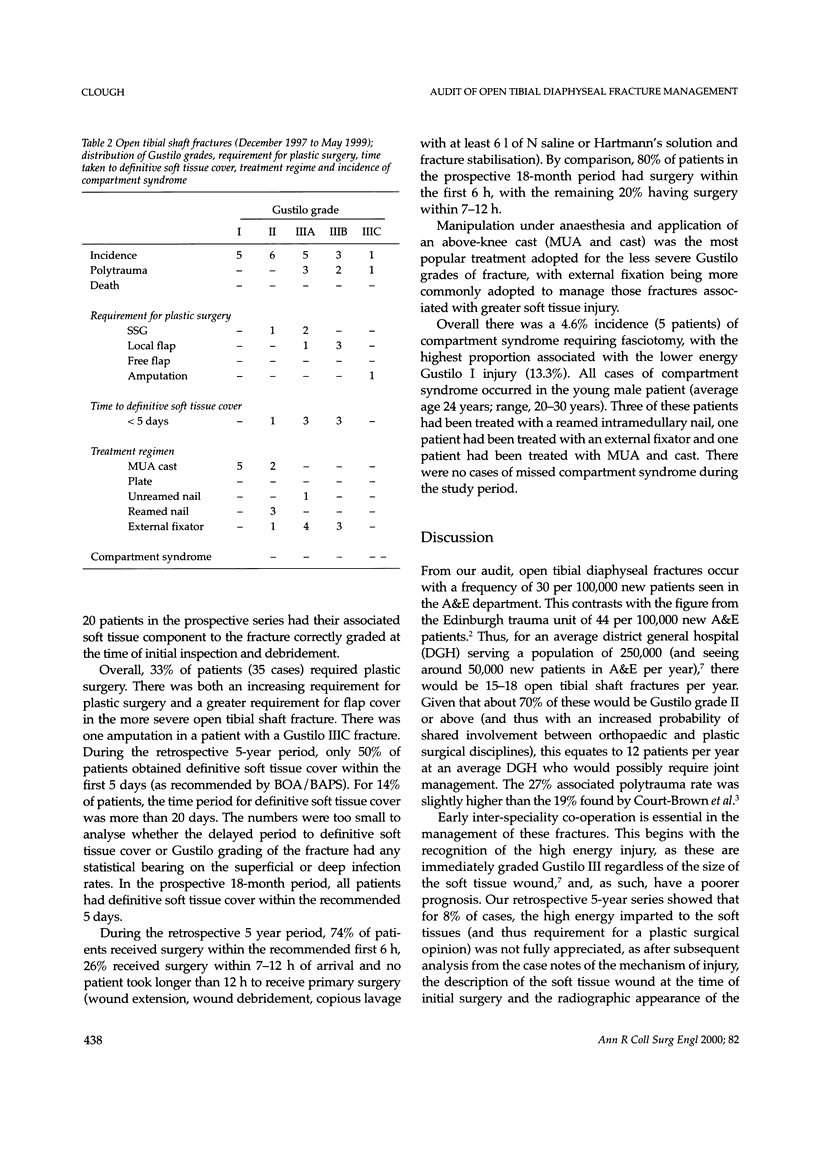
Preston Acute Hospital is a designated district accident centre with a 24 h flying squad and on-site plastic and orthopaedic units. We performed a retrospective 5-year survey of open tibial shaft fracture management at our unit and compared our treatment to the guidelines of the British Orthopaedic Association (BOA) and British Association of Plastic Surgeons (BAPS). Deficiencies were highlighted and changes in practice made. We then re-audited our figures over an 18-month period to see if clinical improvements had been made. The audit demonstrated an incidence of open tibial shaft fractures of 15 per 50,000 new patients per year in accident and emergency. Gustilo grading, and thus full appreciation of soft tissues injury, was being underestimated, with 8% of the injuries undergraded at the time of surgery: 17% of Gustilo IIIA and 85% Gustilo IIIB required flap cover. Seventy-four percent of patients received their first orthopaedic procedure within the recommended 6 h of admission, but despite the on-site plastics unit, only 50% of cases in the initial survey had their soft tissue defect covered by the recommended 5 days. After changes to practice, 80% patients received their first orthopaedic procedure within the recommended 6 h of admission, and all had their soft tissue defect covered within 5 days; 5% of cases required fasciotomy to relieve compartment syndrome. We highlight features to alert the high energy (Gustilo III) status and recommend immediate involvement of plastic surgical colleagues with these injuries. We also highlight a high incidence of compartment syndrome in the young male patient with the lower energy Gustilo I injury.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Court-Brown C. M., Rimmer S., Prakash U., McQueen M. M. The epidemiology of open long bone fractures. Injury. 1998 Sep;29(7):529–534. doi: 10.1016/s0020-1383(98)00125-9. [DOI] [PubMed] [Google Scholar]
- Gustilo R. B., Anderson J. T. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976 Jun;58(4):453–458. [PubMed] [Google Scholar]
- Gustilo R. B., Mendoza R. M., Williams D. N. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984 Aug;24(8):742–746. doi: 10.1097/00005373-198408000-00009. [DOI] [PubMed] [Google Scholar]
- Keating J. F., O'Brien P. I., Blachut P. A., Meek R. N., Broekhuyse H. M. Reamed interlocking intramedullary nailing of open fractures of the tibia. Clin Orthop Relat Res. 1997 May;(338):182–191. doi: 10.1097/00003086-199705000-00025. [DOI] [PubMed] [Google Scholar]
- McQueen M. M., Court-Brown C. M. Compartment monitoring in tibial fractures. The pressure threshold for decompression. J Bone Joint Surg Br. 1996 Jan;78(1):99–104. [PubMed] [Google Scholar]