

Abstract
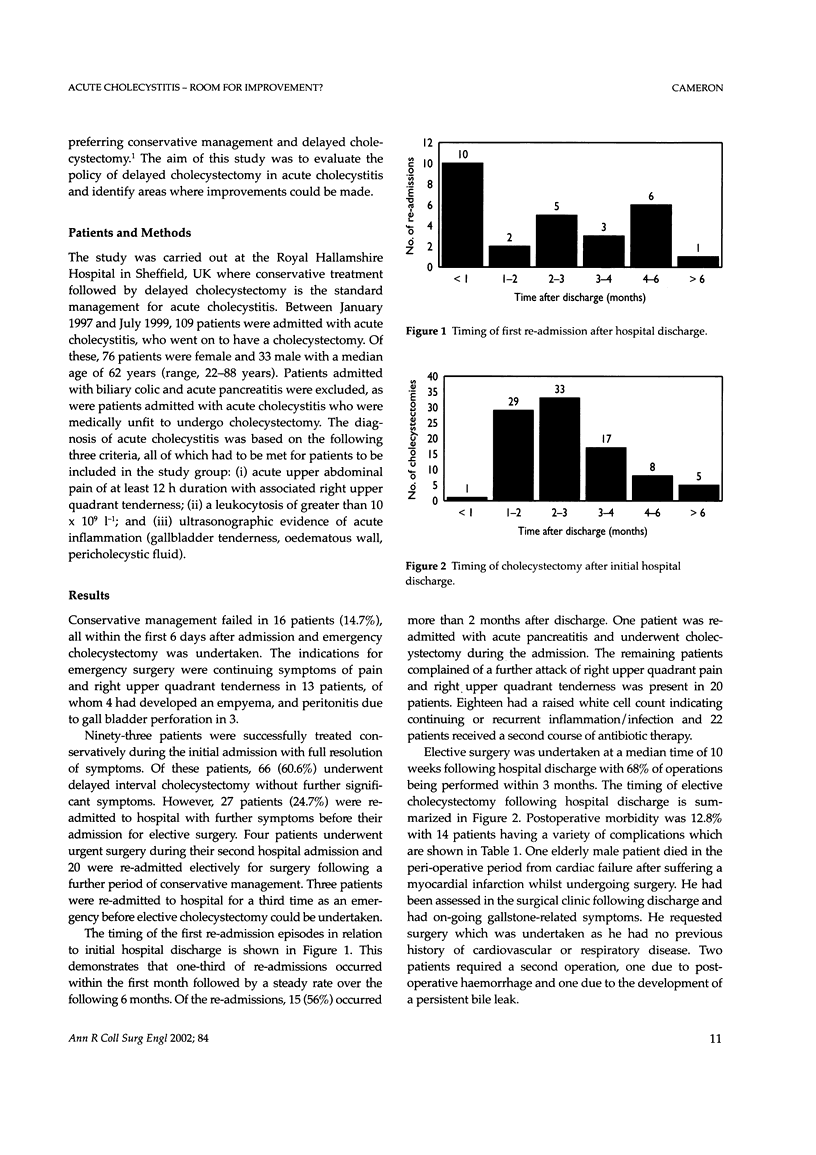
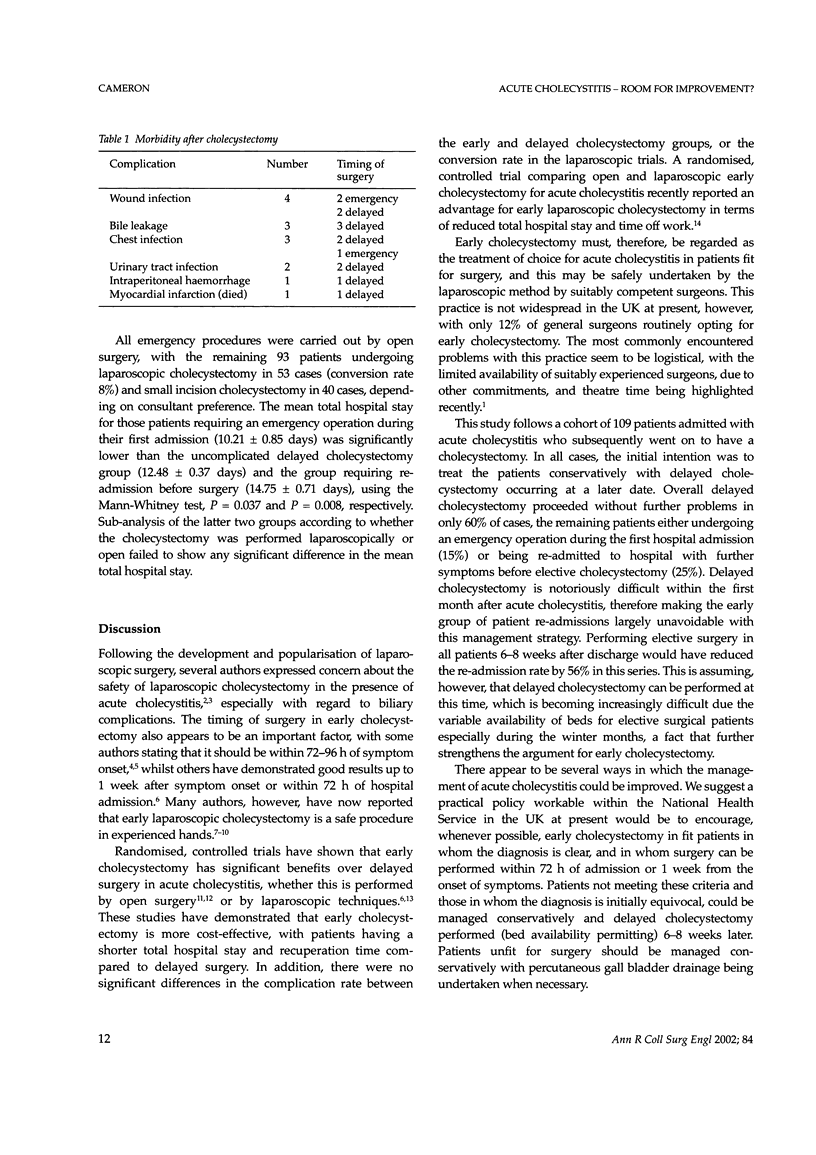
AIMS: A recent survey of UK general surgeons showed that almost 90% prefer to manage patients with acute cholecystitis by initial conservative management and delayed cholecystectomy (DC). The aim of this study was to assess the effectiveness of this management policy in a large university hospital. PATIENTS AND METHODS: All patients admitted with acute cholecystitis between January 1997 and June 1999 who went on to have a cholecystectomy were identified. Patients were required to have right upper quadrant pain for > 12 h, a raised white cell count and findings consistent with acute cholecystitis on ultrasound to be included in the study. RESULTS: 109 patients were admitted with acute cholecystitis (76 female, 33 male) with a median age of 62 years (range, 22-88 years). Conservative management failed in 16 patients (14.7%) who underwent emergency cholecystectomy due to continuing symptoms (9), empyema (4) and peritonitis (3). Symptoms settled in 93 patients and delayed cholecystectomy was performed without further problems in 66 (60.6%). 27 patients were re-admitted with further symptoms before their elective surgery and, of these, 3 were admitted for a third time before surgical intervention. Ten of the 30 re-admission episodes (33%) occurred within 3 weeks of discharge but 15 (56%) occurred more than 2 months after discharge. Elective surgery was undertaken at a median of 10 weeks post-discharge with 67% of operations occurring within 3 months. Mean total hospital stay (days) +/- SEM, for the three groups were: emergency surgery group, 10.21 +/- 0.85; uncomplicated DC group, 12.48 +/- 0.37; re-admitted group, 14.75 +/- 0.71. CONCLUSIONS: The policy of conservative management and DC was successful in 60.6% of cases but 14.7% of patients required emergency surgery and 24.8% were re-admitted prior to elective surgery with a resultant increase in total hospital stay. Performing elective surgery within 2 months of discharge in all cases would have reduced the re-admission rate by 56% and this along with the increased use of early cholecystectomy during the first admission are areas where the treatment of acute cholecystitis could be significantly improved.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bickel A., Rappaport A., Kanievski V., Vaksman I., Haj M., Geron N., Eitan A. Laparoscopic management of acute cholecystitis. Prognostic factors for success. Surg Endosc. 1996 Nov;10(11):1045–1049. doi: 10.1007/s004649900237. [DOI] [PubMed] [Google Scholar]
- Eldar S., Sabo E., Nash E., Abrahamson J., Matter I. Laparoscopic cholecystectomy for acute cholecystitis: prospective trial. World J Surg. 1997 Jun;21(5):540–545. doi: 10.1007/pl00012283. [DOI] [PubMed] [Google Scholar]
- Flowers J. L., Bailey R. W., Scovill W. A., Zucker K. A. The Baltimore experience with laparoscopic management of acute cholecystitis. Am J Surg. 1991 Mar;161(3):388–392. doi: 10.1016/0002-9610(91)90604-c. [DOI] [PubMed] [Google Scholar]
- Järvinen H. J., Hästbacka J. Early cholecystectomy for acute cholecystitis: a prospective randomized study. Ann Surg. 1980 Apr;191(4):501–505. doi: 10.1097/00000658-198004000-00018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiviluoto T., Sirén J., Luukkonen P., Kivilaakso E. Randomised trial of laparoscopic versus open cholecystectomy for acute and gangrenous cholecystitis. Lancet. 1998 Jan 31;351(9099):321–325. doi: 10.1016/S0140-6736(97)08447-X. [DOI] [PubMed] [Google Scholar]
- Koo K. P., Thirlby R. C. Laparoscopic cholecystectomy in acute cholecystitis. What is the optimal timing for operation? Arch Surg. 1996 May;131(5):540–545. doi: 10.1001/archsurg.1996.01430170086016. [DOI] [PubMed] [Google Scholar]
- Kum C. K., Eypasch E., Lefering R., Paul A., Neugebauer E., Troidl H. Laparoscopic cholecystectomy for acute cholecystitis: is it really safe? World J Surg. 1996 Jan;20(1):43–49. doi: 10.1007/s002689900008. [DOI] [PubMed] [Google Scholar]
- Lai P. B., Kwong K. H., Leung K. L., Kwok S. P., Chan A. C., Chung S. C., Lau W. Y. Randomized trial of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br J Surg. 1998 Jun;85(6):764–767. doi: 10.1046/j.1365-2168.1998.00708.x. [DOI] [PubMed] [Google Scholar]
- Lo C. M., Liu C. L., Fan S. T., Lai E. C., Wong J. Prospective randomized study of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Ann Surg. 1998 Apr;227(4):461–467. doi: 10.1097/00000658-199804000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lujan J. A., Parrilla P., Robles R., Torralba J. A., Garcia Ayllon J., Liron R., Sanchez-Bueno F. Laparoscopic cholecystectomy in the treatment of acute cholecystitis. J Am Coll Surg. 1995 Jul;181(1):75–77. [PubMed] [Google Scholar]
- Norrby S., Herlin P., Holmin T., Sjödahl R., Tagesson C. Early or delayed cholecystectomy in acute cholecystitis? A clinical trial. Br J Surg. 1983 Mar;70(3):163–165. doi: 10.1002/bjs.1800700309. [DOI] [PubMed] [Google Scholar]
- Russell J. C., Walsh S. J., Mattie A. S., Lynch J. T. Bile duct injuries, 1989-1993. A statewide experience. Connecticut Laparoscopic Cholecystectomy Registry. Arch Surg. 1996 Apr;131(4):382–388. doi: 10.1001/archsurg.1996.01430160040007. [DOI] [PubMed] [Google Scholar]
- Willsher P. C., Sanabria J. R., Gallinger S., Rossi L., Strasberg S., Litwin D. E. Early laparoscopic cholecystectomy for acute cholecystitis: a safe procedure. J Gastrointest Surg. 1999 Jan-Feb;3(1):50–53. doi: 10.1016/s1091-255x(99)80008-0. [DOI] [PubMed] [Google Scholar]