

Abstract
In North America, the most common causes of benign esophageal stricture are hiatal hernia and reflux esophagitis. These are localized to the lower end of the esophagus.
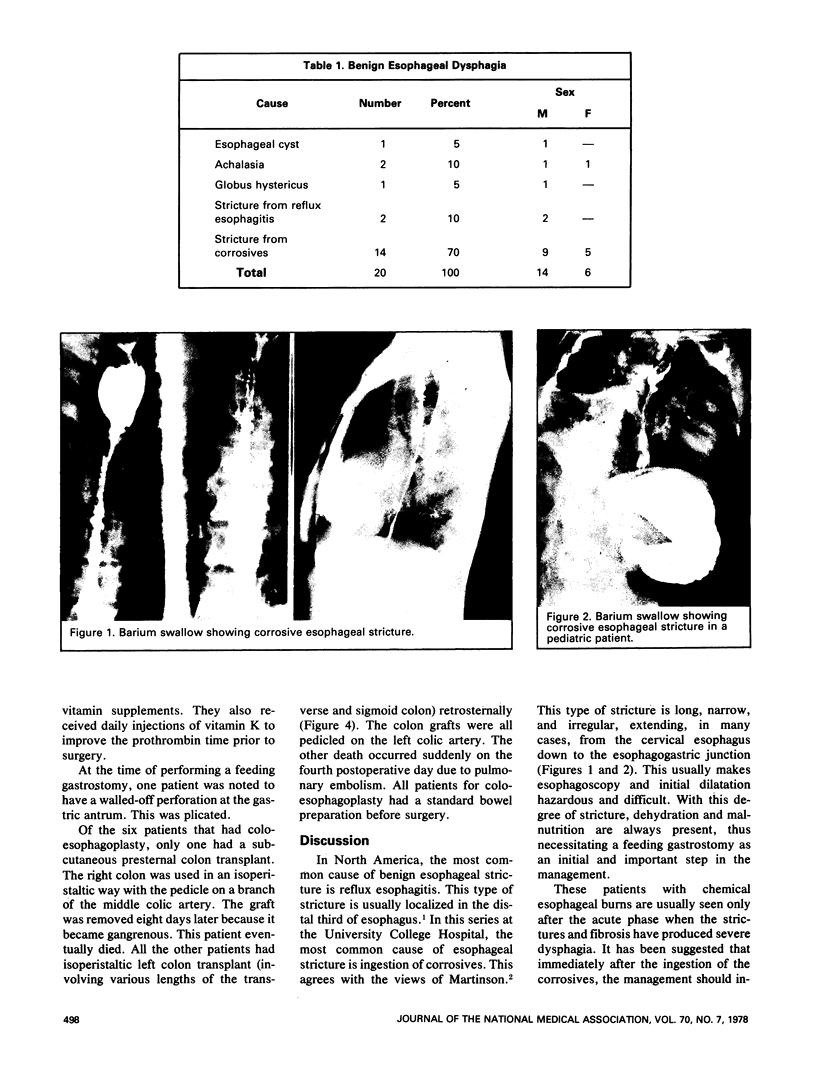
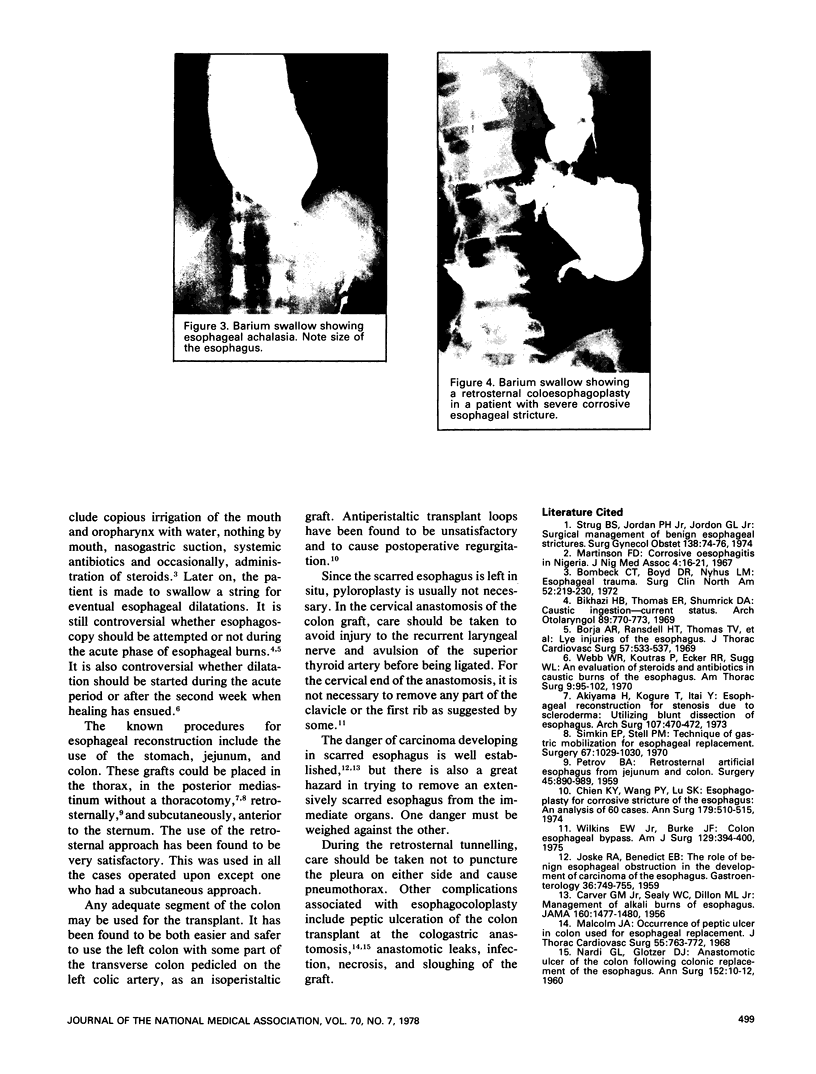
At the University College Hospital, Ibadan, Nigeria, the most common cause of benign esophageal stricture is ingestion of corrosives. The ingestion is accidental, suicidal, or for medicinal purposes. This stricture is long, narrow, and irregular. Most extend from the cervical esophagus to the cardioesophageal junction.
A surgical procedure that has given good results is the use of left colon pedicled on the left colic artery for retrosternal isoperistaltic esophagocoloplasty.
Full text
PDF
Images in this article



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Akiyama H., Kogure T., Itai Y. Esophageal reconstruction for stenosis due to diffuse scleroderma. Utilizing blunt dissection of esophagus. Arch Surg. 1973 Sep;107(3):470–472. doi: 10.1001/archsurg.1973.01350210100027. [DOI] [PubMed] [Google Scholar]
- Bikhazi H. B., Thompson E. R., Shumrick D. A. Caustic ingestion: current status. A report of 105 cases. Arch Otolaryngol. 1969 May;89(5):770–773. doi: 10.1001/archotol.1969.00770020772019. [DOI] [PubMed] [Google Scholar]
- Bombeck C. T., Boyd D. R., Nyhus L. M. Esophageal trauma. Surg Clin North Am. 1972 Feb;52(1):219–230. doi: 10.1016/s0039-6109(16)39644-x. [DOI] [PubMed] [Google Scholar]
- Borja A. R., Ransdell H. T., Jr, Thomas T. V., Johnson W. Lye injuries of the esophagus. Analysis of ninety cases of lye ingestion. J Thorac Cardiovasc Surg. 1969 Apr;57(4):533–538. [PubMed] [Google Scholar]
- Chien K. Y., Wang P. Y., Lu K. S. Esophagoplasty for corrosive stricutre of the esophagus: an analysis of 60 cases. Ann Surg. 1974 Apr;179(4):510–515. doi: 10.1097/00000658-197404000-00023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- JOSKE R. A., BENEDICT E. B. The role of benign esophageal obstruction in the development of carcinoma of the esophagus. Gastroenterology. 1959 Jun;36(6):749–755. [PubMed] [Google Scholar]
- Malcolm J. A. Occurrence of peptic ulcer in colon used for esophageal replacement. J Thorac Cardiovasc Surg. 1968 Jun;55(6):763–772. [PubMed] [Google Scholar]
- NARDI G. L., GLOTZER D. J. Anastomotic ulcer of the colon following colonic replacement of the esophagus. Ann Surg. 1960 Jul;152:10–12. doi: 10.1097/00000658-196007000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- PETROV B. A. Retrosternal artificial esophagus from jejunum and colon. Surgery. 1959 Jun;45(6):890–898. [PubMed] [Google Scholar]
- Simkin E. P., Stell P. M. Technique of gastric mobilization for esophageal replacement. Surgery. 1970 Jun;67(6):1029–1030. [PubMed] [Google Scholar]
- Strug B. S., Jordan P. H., Jr, Jordan G. L., Jr Surgical management of benign esophageal strictures. Surg Gynecol Obstet. 1974 Jan;138(1):74–76. [PubMed] [Google Scholar]
- Webb W. R., Koutras P., Ecker R. R., Sugg W. L. An evaluation of steroids and antibiotics in caustic burns of the esophagus. Ann Thorac Surg. 1970 Feb;9(2):95–102. doi: 10.1016/s0003-4975(10)65781-5. [DOI] [PubMed] [Google Scholar]
- Wilkins E. W., Jr, Burke J. F. Colon esophageal bypass. Am J Surg. 1975 Apr;129(4):394–400. doi: 10.1016/0002-9610(75)90183-x. [DOI] [PubMed] [Google Scholar]