

Abstract
The longest component of the total delay in coming under coronary care is patient delay, and it has been suggested that public education might be used to make it shorter. The patterns of patient delay were studied in 450 patients with acute myocardial infarction uncomplicated by cardiac arrest out of hospital, of whom 243 had a previous history of ischaemic heart disease. Patient delays had a skewed distribution with a modal delay of up to one hour, a median delay of two hours, and a mean delay of 10 hours. Two thirds of patients had sought help from their general practitioners within four hours of the onset of symptoms. During the first four hours the longer that patients delayed the lower was the subsequent mortality (27%, 18%, and 9% for delays of one hour or less, up to two hours, and up to four hours, respectively), but patients who delayed four to eight hours had the highest mortality of all (38%). Neither the median value nor the pattern of patient delays was altered by a previous history of ischaemic heart disease.
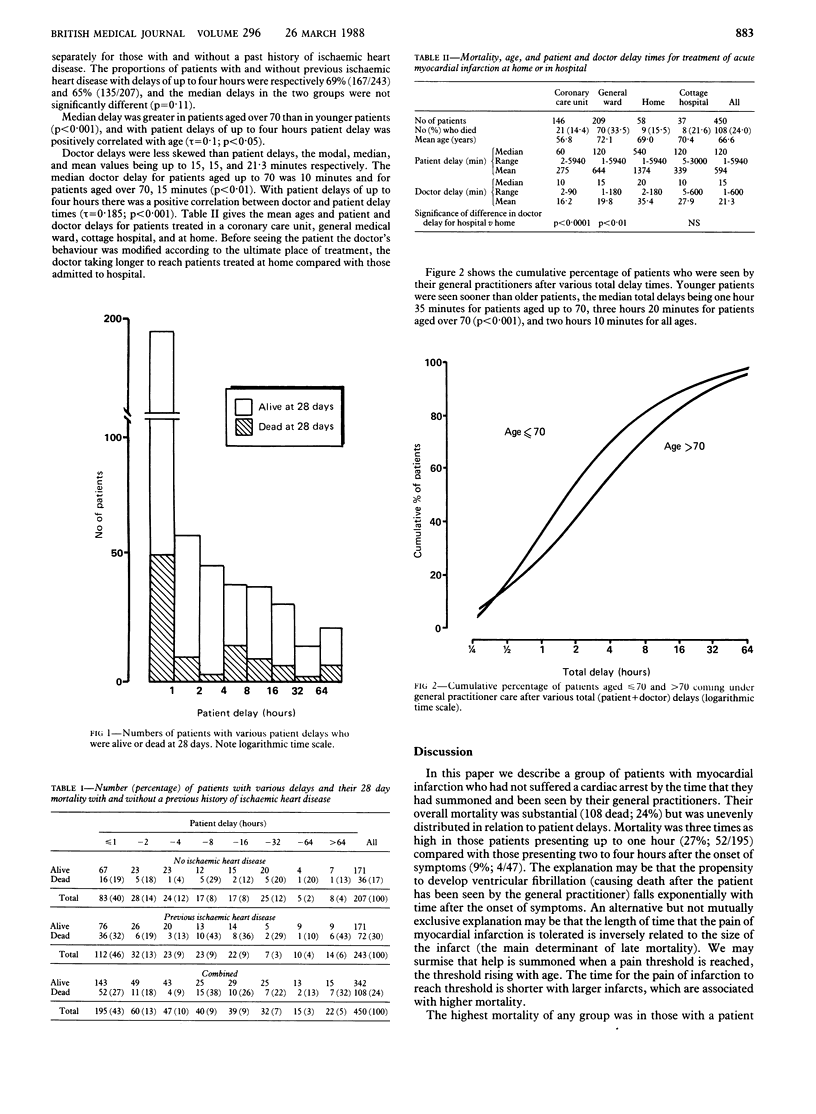
There were pronounced differences in doctor delays, depending on the patient's age, delay time, and ultimate place of treatment, showing that the doctors' behaviour was influenced before they had seen their patients. Nevertheless, the median total delay for patients aged up to 70 was one hour 35 minutes, and a higher proportion of patients were seen early after infarction than in recent hospital trials of thrombolytic treatment.
These findings suggest that the patients' call for help and the doctors' response may be at an instinctive level according to the patients' distress; these patterns of behaviour may be difficult to modify by public education.
Full text
PDF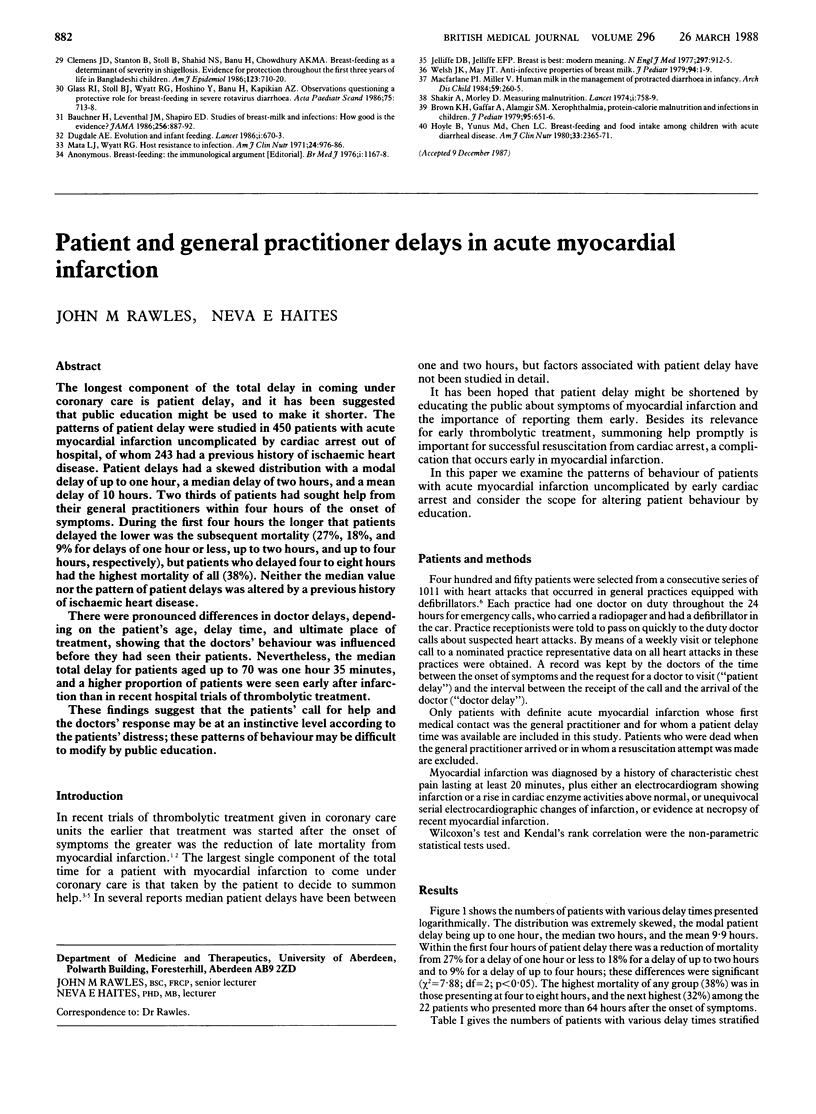
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Armstrong A., Duncan B., Oliver M. F., Julian D. G., Donald K. W., Fulton M., Lutz W., Morrison S. L. Natural history of acute coronary heart attacks. A community study. Br Heart J. 1972 Jan;34(1):67–80. doi: 10.1136/hrt.34.1.67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colling A., Dellipiani A. W., Donaldson R. J., MacCormack P. Teesside coronary survey: an epidemiological study of acute attacks of myocardial infarction. Br Med J. 1976 Nov 13;2(6045):1169–1172. doi: 10.1136/bmj.2.6045.1169. [DOI] [PMC free article] [PubMed] [Google Scholar]
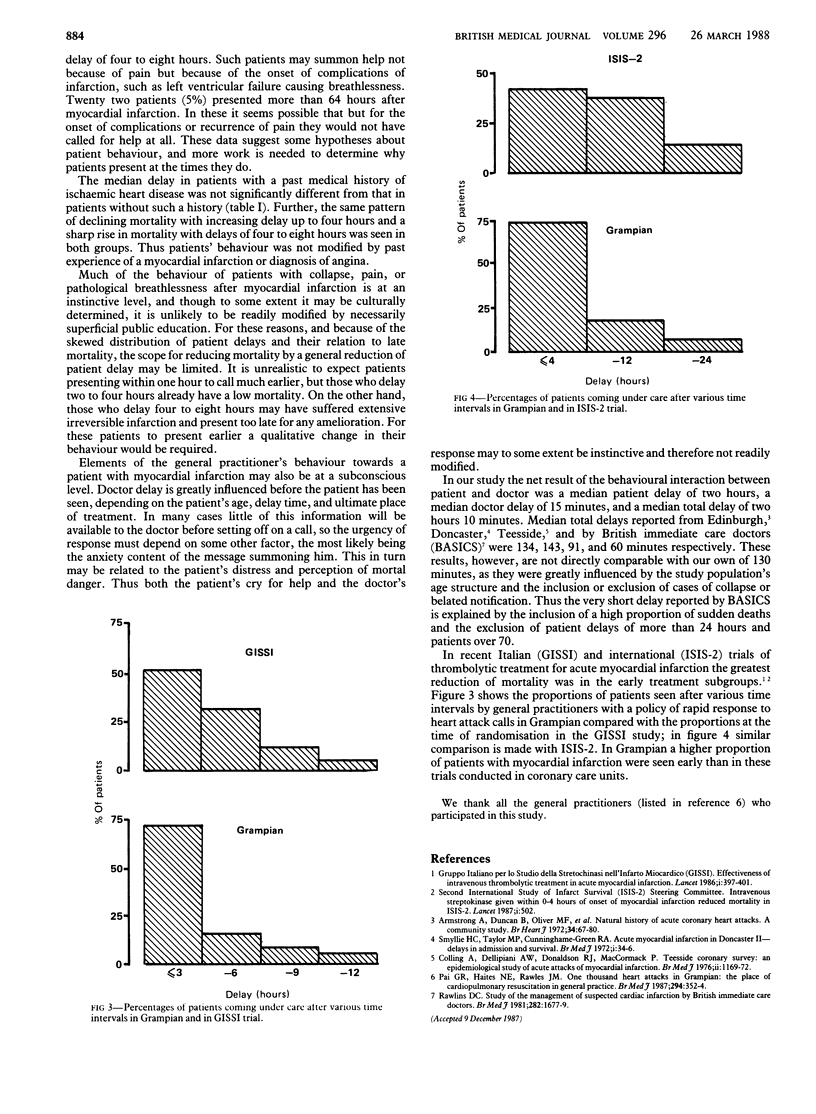
- Pai G. R., Haites N. E., Rawles J. M. One thousand heart attacks in Grampian: the place of cardiopulmonary resuscitation in general practice. Br Med J (Clin Res Ed) 1987 Feb 7;294(6568):352–354. doi: 10.1136/bmj.294.6568.352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rawlins D. C. Study of the management of suspected cardiac infarction by British immediate care doctors. Br Med J (Clin Res Ed) 1981 May 23;282(6277):1677–1679. doi: 10.1136/bmj.282.6277.1677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smyllie H. C., Taylor M. P., Cuninghame-Green R. A. Acute myocardial infarction in Doncaster. II. Delays in admission and survival. Br Med J. 1972 Jan 1;1(5791):34–36. doi: 10.1136/bmj.1.5791.34. [DOI] [PMC free article] [PubMed] [Google Scholar]