

Abstract
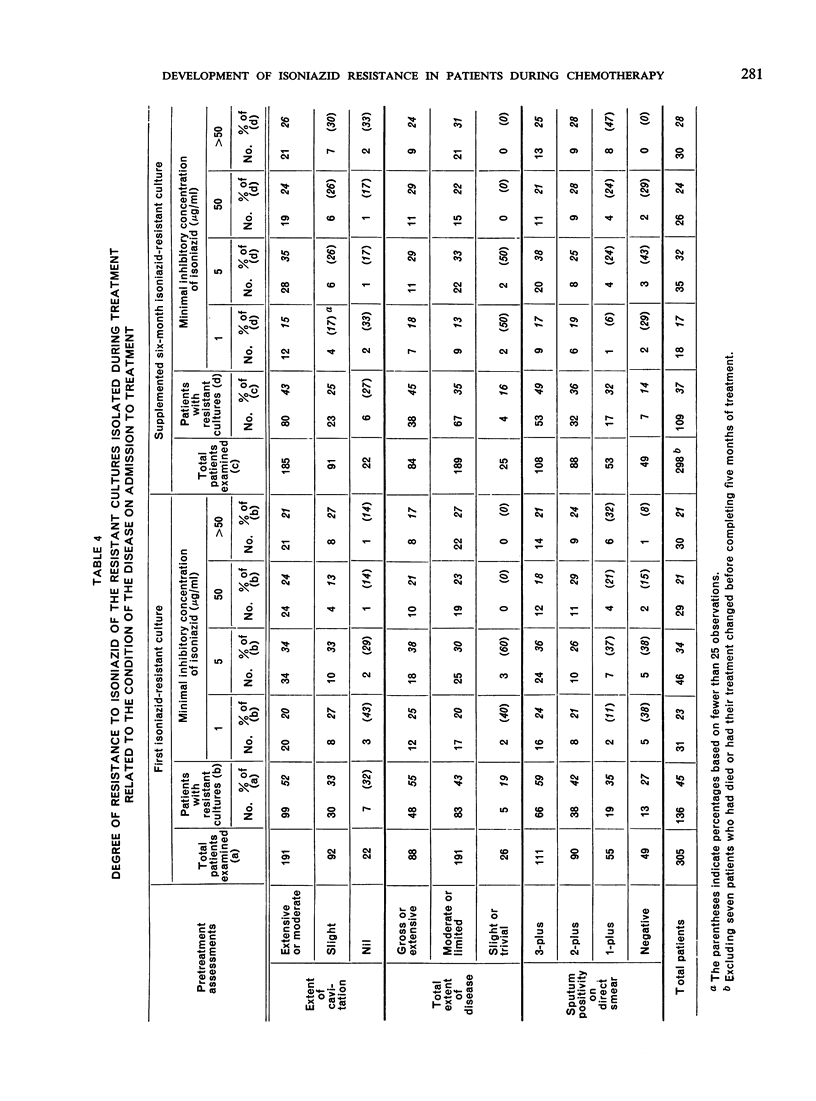
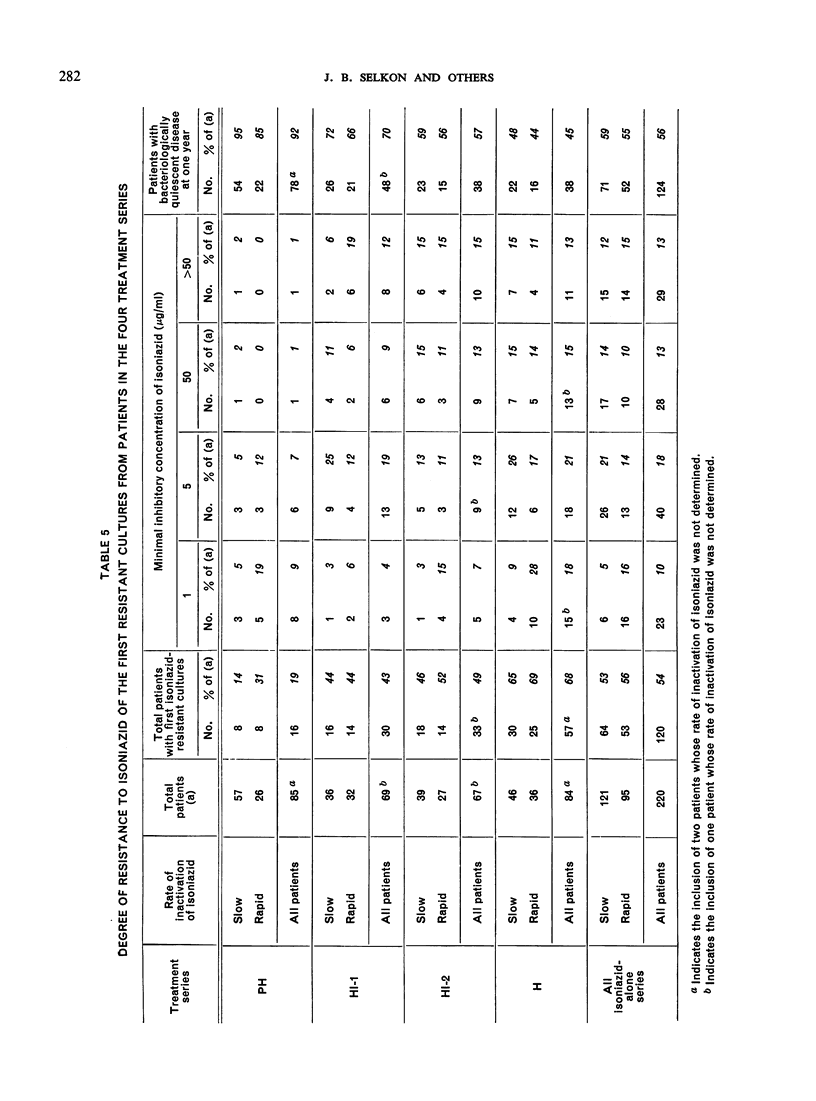
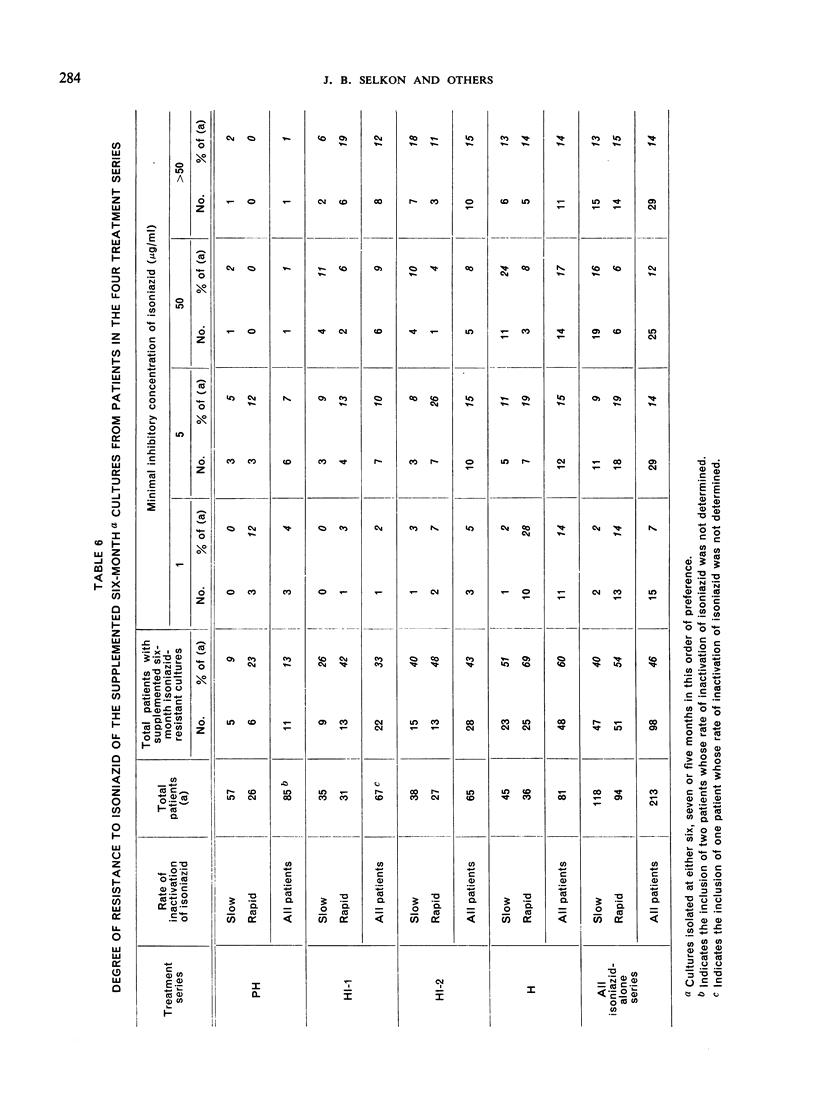
Previous reports from the Tuberculosis Chemotherapy Centre, Madras, have described a comparison of four regimens (three of isoniazid alone and one of isoniazid plus PAS) in the treatment of pulmonary tuberculosis and an investigation of the serum isoniazid levels in the patients concerned. The present report studies the emergence of isoniazid-resistant organisms in these patients during treatment. All patients with an unsatisfactory response to treatment yielded resistant cultures, showing that the isoniazid dosage was never too low to inhibit sensitive organisms. From the degree of resistance of the first resistant cultures and of the six-month cultures from the patients treated with isoniazid alone it was concluded that resistance emerged in two stages. In the first stage, very earlyin treatment, highly resistant mutant bacilli grew freely whatever the isoniazid dosage, but mutants of lower resistance were prevented from growing to an extent dependent on the peak isoniazid concentration in the serum. Consequently, when the isoniazid dosage was increased the proportion of patients with resistant organisms decreased, since fewer low-resistance strains were able to develop. In the second stage, organisms with relatively low resistance continued to multiply, though still partially inhibited by isoniazid, and became more resistant, particularly in slow inactivators. The first-stage events determined the results of treatment since, once resistance had emerged, its extent was unrelated to the patient's eventual progress. These findings emphasize the importance of early intensive chemotherapy and adjustment of the isoniazid dosage according to peak serum concentrations rather than concentrations measured three or six hours after the dose. Concomitant administration of PAS prevented emergence of isoniazid resistance in many patients and in others delayed its emergence and reduced its degree, possibly because growth in the second stage was slow.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BARCLAY W. R., KOCH-WESER D., EBERT R. H. Mode of action of isoniazid. II. Am Rev Tuberc. 1954 Nov;70(5):784–792. doi: 10.1164/art.1954.70.5.784. [DOI] [PubMed] [Google Scholar]
- CANETTI G., GROSSET J. [Percentage of isoniazid-resistant and streptomycin-resistant variants in wild strains of Mycobacterium tuberculosis on Loewenstein-Jensen medium]. Ann Inst Pasteur (Paris) 1961 Jul;101:28–46. [PubMed] [Google Scholar]
- FOX W., SUTHERLAND I. The clinical significance of positive cultures and of isoniazid-resistant tubercle bacilli during the treatment of pulmonary tuberculosis; report to the Tuberculosis Chemotherapy Trials Committee of the Medical Research Council. Thorax. 1955 Jun;10(2):85–98. doi: 10.1136/thx.10.2.85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GANGADHARAM P. R., BHATIA A. L., RADHAKRISHNA S., SELKON J. B. Rate of inactivation of isoniazid in South Indian patients with pulmonary tuberculosis. Bull World Health Organ. 1961;25:765–777. [PMC free article] [PubMed] [Google Scholar]
- GANGADHARAM P. R., DEVADATTA S., FOX W., NAIR C. N., SELKON J. B. Rate of inactivation of isoniazid in South Indian patients with pulmonary tuberculosis. 3. Serum concentrations of isoniazid produced by three regimens of isoniazid alone and one of isoniazid plus PAS. Bull World Health Organ. 1961;25:793–806. [PMC free article] [PubMed] [Google Scholar]
- MIDDLEBROOK G. Sterilization of tubercle bacilli by isonicotinic acid hydrazide and the incidence of variants resistant to the drug in vitro. Am Rev Tuberc. 1952 Jun;65(6):765–767. [PubMed] [Google Scholar]
- SELKON J. B., FOX W., GANGADHARAM P. R., RAMACHANDRAN K., RAMAKRISHNAN C. V., VELU S. Rate of inactivation of isoniazid in South Indian patients with pulmonary tuberculosis. 2. Clinical implications in the treatment of pulmonary tuberculosis with isoniazid either alone or in combination with PAS. Bull World Health Organ. 1961;25:779–792. [PMC free article] [PubMed] [Google Scholar]
- TSUKAMURA M., TSUKAMURA S., NAKANO E. The uptake of isoniazid by mycobacteria and its relation to isoniazid susceptibility. Am Rev Respir Dis. 1963 Feb;87:269–275. doi: 10.1164/arrd.1963.87.2.269. [DOI] [PubMed] [Google Scholar]
- VELU S., ANDREWS R. H., ANGEL J. H., DEVADATTA S., FOX W., GANGADHARAM P. R., NARAYANA A. S., RAMAKRISHNAN C. V., SELKON J. B., SOMASUNDARAM P. R. Progress in the second year of patients with quiescent pulmonary tuberculosis after a year of domiciliary chemotherapy, and influence of further chemotherapy on the relapse rate. Bull World Health Organ. 1961;25:409–429. [PMC free article] [PubMed] [Google Scholar]
- YOUATT J. The uptake of isoniazid by washed cell suspensions of Mycobacteria and other organisms. Aust J Exp Biol Med Sci. 1958 Jun;36(3):223–233. doi: 10.1038/icb.1958.24. [DOI] [PubMed] [Google Scholar]