

Abstract
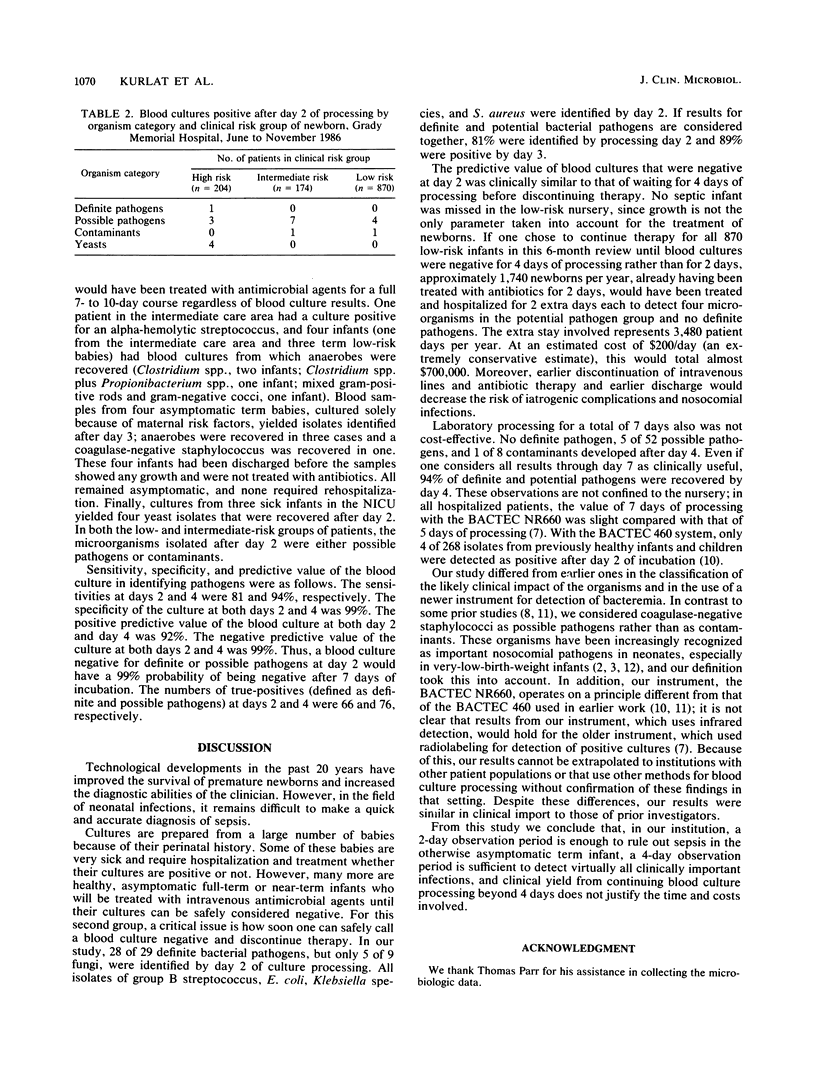
The blood culture results of all samples obtained from newborns at Grady Memorial Hospital, Atlanta, Ga., during a 6-month period were analyzed to determine the time required for a blood culture to become positive, the time at which a culture could safely be considered negative, and the spectrum of isolated organisms. During the study period, 1,248 samples were submitted from all nurseries and processed by an automated detection instrument (BACTEC NR660). Of the 1,248 samples, 98 (7.8%) were positive by the end of a 7-day processing period; 29 of the 98 were classified as definite bacterial pathogens, 52 were classified as possible bacterial pathogens, 9 were classified as yeasts, and 8 were classified as contaminants. Virtually all organisms (28 of 29) categorized as definite pathogens were identified by day 2 of processing, and all were identified by day 4. All isolates of group B streptococcus, Escherichia coli, Klebsiella species, and Staphylococcus aureus were identified by day 2. Of all positive blood cultures, 79% were identified by day 2, 88% were identified by day 3, and 94% were identified by day 4. Of the 21 isolates identified after day 2, the only definite pathogen was from a sick baby in the intensive care unit. From among the 870 term low-risk newborns cultured because of maternal risk factors, only four possible pathogens were identified after day 2. The positive and negative predictive values of blood culture at days 2 and 4 were 92 and 99%, respectively.We conclude that, in our institution, (i) a 2-day processing period is sufficient to detect positive blood cultures in the asymptomatic term infant, (ii) a 4-day processing period will detect virtually all clinically important infections, and (iii) clinical yield from continuing blood culture processing beyond 4 days does not justify the time and cost involved.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aronson M. D., Bor D. H. Blood cultures. Ann Intern Med. 1987 Feb;106(2):246–253. doi: 10.7326/0003-4819-106-2-246. [DOI] [PubMed] [Google Scholar]
- Donowitz L. G., Haley C. E., Gregory W. W., Wenzel R. P. Neonatal intensive care unit bacteremia: emergence of gram-positive bacteria as major pathogens. Am J Infect Control. 1987 Aug;15(4):141–147. doi: 10.1016/0196-6553(87)90137-4. [DOI] [PubMed] [Google Scholar]
- Freeman J., Platt R., Sidebottom D. G., Leclair J. M., Epstein M. F., Goldmann D. A. Coagulase-negative staphylococcal bacteremia in the changing neonatal intensive care unit population. Is there an epidemic? JAMA. 1987 Nov 13;258(18):2548–2552. [PubMed] [Google Scholar]
- Masterson K. C., McGowan J. E., Jr Detection of positive blood cultures by the Bactec NR660. The clinical importance of five versus seven days of testing. Am J Clin Pathol. 1988 Jul;90(1):91–94. doi: 10.1093/ajcp/90.1.91. [DOI] [PubMed] [Google Scholar]
- Pichichero M. E., Todd J. K. Detection of neonatal bacteremia. J Pediatr. 1979 Jun;94(6):958–960. doi: 10.1016/s0022-3476(79)80233-4. [DOI] [PubMed] [Google Scholar]
- Rowley A. H., Wald E. R. Incubation period necessary to detect bacteremia in neonates. Pediatr Infect Dis. 1986 Sep-Oct;5(5):590–591. doi: 10.1097/00006454-198609000-00022. [DOI] [PubMed] [Google Scholar]
- Rowley A. H., Wald E. R. The incubation period necessary for detection of bacteremia in immunocompetent children with fever. Implications for the clinician. Clin Pediatr (Phila) 1986 Oct;25(10):485–489. doi: 10.1177/000992288602501001. [DOI] [PubMed] [Google Scholar]
- Schmidt B. K., Kirpalani H. M., Corey M., Low D. E., Philip A. G., Ford-Jones E. L. Coagulase-negative staphylococci as true pathogens in newborn infants: a cohort study. Pediatr Infect Dis J. 1987 Nov;6(11):1026–1031. [PubMed] [Google Scholar]
- Townsend T. R., Wenzel R. P. Nosocomial bloodstream infections in a newborn intensive care unit: a case-matched control study of morbidity, mortality and risk. Am J Epidemiol. 1981 Jul;114(1):73–80. doi: 10.1093/oxfordjournals.aje.a113176. [DOI] [PubMed] [Google Scholar]
- Weinstein M. P., Reller L. B., Murphy J. R., Lichtenstein K. A. The clinical significance of positive blood cultures: a comprehensive analysis of 500 episodes of bacteremia and fungemia in adults. I. Laboratory and epidemiologic observations. Rev Infect Dis. 1983 Jan-Feb;5(1):35–53. doi: 10.1093/clinids/5.1.35. [DOI] [PubMed] [Google Scholar]