

Abstract
Errors arise when an action is intended but not performed; errors that arise from poor planning or inadequate knowledge are characterized as mistakes; those that arise from imperfect execution of well-formulated plans are called slips when an erroneous act is committed and lapses when a correct act is omitted.
Some tasks are intrinsically prone to error. Examples are tasks that are unfamiliar to the operator or performed under pressure. Tasks that require the calculation of a dosage or dilution are especially susceptible to error.
The tasks of prescribing, preparation, and administration of medicines are complex, and are carried out within a complex system; errors can occur at each of many steps and the error rate for the overall process is therefore high.
The error rate increases when health-care professionals are inexperienced, inattentive, rushed, distracted, fatigued, or depressed; orthopaedic surgeons and nurses may be more likely than other health-care professionals to make medication errors.
Medication error rates in hospital are higher in paediatric departments and intensive care units than elsewhere.
Rates of medication errors may be higher in very young or very old patients.
Intravenous antibiotics are the drugs most commonly involved in medication errors in hospital; antiplatelet agents, diuretics, and non-steroidal anti-inflammatory drugs are most likely to account for ‘preventable admissions’.
Computers effectively reduce the rates of easily counted errors. It is not clear whether they can save lives lost through rare but dangerous errors in the medication process.
Keywords: iatrogenic disease, lapses, medication errors, mistakes, psychology, slips
Error –‘something incorrectly done through ignorance or inadvertence’[1]– is a fact of the human condition. We dial wrong numbers, take wrong turnings, and make slips of the tongue. Psychologists have pointed out the inevitability of error in human actions [2]. As Mach stated, ‘Knowledge and error flow from the same mental sources, only success can tell the one from the other’[3]. A conscious human action can be performed correctly and reach its intended goal. Errors arise when an action is intended but not performed. The ‘human factors approach’ is now widely adopted in understanding medical error and in seeking ways to reduce harm from errors [4, 5]. In this review we consider how errors can occur and what factors alter the risk of error. Other models have been proposed and are reviewed elsewhere [6].
Forms of error
An error is a disorder of an intentional act. The act can be considered in two parts: formulating the plan for action; and executing it (Figure 1).
Figure 1.
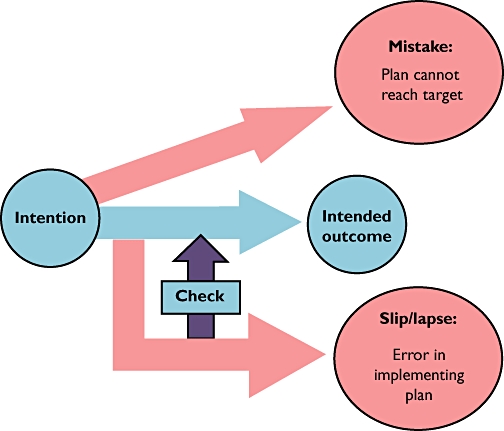
Diagram of the ‘routes of error.’ An action is initiated with the intention of reaching a specific outcome. When all goes well, there is no error, and the intended outcome is achieved. Sometimes the plan will be wrong, or the information used in formulating the action is wrong, so that it is impossible to reach the intended outcome. Errors of this sort are labelled mistakes. If the plan is correct, and based on correct information, but there is distraction on the route from intention to outcome, then a slip or lapse results. Slips are errors of commission, whereas lapses are errors of omission. Checking during execution can intercept errors (slips, lapses, or mistakes)
An error in formulating the plan is a mistake. Mistakes occur when people undertake non-routine tasks that require conscious (supervisory) attention, i.e. they require problem-solving, judgement, diagnosis, or theoretical knowledge, or are outside the previous experience of the person undertaking them [7]. Even if a task is routine, cognitive error is still possible, if it is ambiguous or poorly understood or if, for example, the staff are not adequately trained, so that they have to think out explicit solutions to the problems posed by the task. Mistakes can arise from a lack of knowledge, resulting in a poor plan, or from good plans applied in the wrong circumstances. An example of the former would be to begin warfarin treatment by giving three doses of 10 mg on successive days (‘10–10–10’) before monitoring coagulation. Such a plan inevitably leads to over-treatment of many patients [8]. A mistake of the second type occurs when cardiopulmonary resuscitation is instituted on a patient whose cardiac monitor shows a flat-line trace, not because the patient has had a cardiac arrest, but because the leads have fallen off.
An error in executing a plan can occur either because one or more step in the plan is executed incorrectly – a slip; or because one or more steps is omitted – a lapse. Picking penicillamine from a computer list of drug names when intending to prescribe penicillin V is a slip. Intending to write a prescription for penicillin V, but forgetting to do so, constitutes a lapse. Errors occur when the execution is in ‘automatic mode’, i.e. it follows a well-worn path (the ‘schema’) until there is a distraction or failure of attention [9, 10].
Actions do not take place in isolation, but as part of a system, a group of interacting entities of which the person performing the action is one. Hospital medication systems are very complex, and the entities involved include, at the very least, a medicine, a patient, one or several healthcare professionals, pharmacy and pharmacy staff, and ultimately the manufacturers and suppliers of the medicines.
The psychologist James Reason called attention to latent errors, i.e. errors that arise because of systems that have the potential to be unsafe – errors ‘waiting to happen’. This is one reason why observed errors that do not result in harm are nevertheless important to analyse. If they reveal latent errors with the potential for harm, they can suggest how to alter a system in order to make it safer.
Since errors are unintentional, there is support for the view, first expressed 70 years ago, that ‘the ordinarily careful and conscientious nurse who makes a mistake has had, in the realization of her act, all the punishment and discipline and suffering which are desirable. What is done beyond that must be of a constructive nature or it had better be left undone’[11].
Violations, actions that deliberately disregard formal instructions, are distinct from errors, which are unintentional deviations from the intended action. Violations, such as the use of proprietary names on drug charts that specify the use of non-proprietary names, are common in medication practice. Systems that tolerate common violations can be criticized either because the formal instructions are unsatisfactory and the violations are understandable; or because the instructions are well formulated but the system fails to ensure that they are complied with.
Medication errors
The difficulties of defining and categorizing medication errors have been reviewed elsewhere in this issue [12]. Here a medication error is taken to be ‘a failure in the treatment process that leads to, or has the potential to lead to, harm to the patient’[13]. The treatment process includes the prescribing, transcribing, manufacturing or compounding, dispensing, and administration of a drug, and monitoring therapy. Each of these separate activities has many components. For example, a single prescription on our hospital drugs chart requires the prescriber to include 21 separate pieces of information, such as the patient's date of birth and the time of administration of the prescribed drug. Each entails an action with the potential for error.
The process of administration of intravenous injections, which is particularly likely to result in harm to the patient, has been examined in some detail [14, 15]. At least a dozen separate steps, and many sub-steps, are required to perform this task; some are trivial but others have the potential for serious error. The probability of undertaking a multistep task without error is the product of the probabilities of carrying out each step without error.† The corollary of this is that a small risk at each step leads to a high probability of error overall. For example, if there are 21 steps, each of which is preformed without error 99% of the time, the overall process will be correct only 80% of the time.
The probability of error
The risk of an error in performing the steps in a complex task is not, in practice, the same for each step. Experiments to determine the rates of error in elementary tasks have given some insight into this. For example, Kirwan set out nominal rates of human unreliability for a series of tasks (Table 1) [16].
Table 1.
Nominal rates of human unreliability for generic tasks (after Kirwan [16])
| Task | Nominal error rate | 95% CI |
|---|---|---|
| Completely familiar, well-designed, highly practised routine task | 0.0004 | 0.00008, 0.009 |
| Routine, highly practised, rapid task requiring little skill | 0.02 | 0.007, 0.045 |
| Fairly simple task performed rapidly or given scant attention | 0.09 | 0.06, 0.13 |
| Complex task requiring high level of comprehension and skill | 0.16 | 0.12, 0.28 |
| Totally unfamiliar task, performed at speed, with no real idea of likely consequences | 0.55 | 0.35, 0.97 |
Berwick and Nolan provided estimates of the error rates in healthcare, based on similar data (Table 2) [17].
Table 2.
Nominal error rates of activities in healthcare (after Berwick and Nolan [17])
| Task | Nominal error rate |
|---|---|
| Error of commission, e.g. misreading label | 0.003 |
| Simple arithmetic errors with self checking | 0.03 |
| Error of omission without reminders | 0.01 |
| Inspector fails to recognize an error | 0.1 |
| Error rate under very high stress when dangerous activities are occurring rapidly | 0.25 |
Leape et al. examined the records from patients admitted to hospital over a 6-month period [18]. Most of the errors occurred at the physician ordering stage (39%), and they were mostly due to lack of knowledge of the drug or lack of information about the patient. Poor dissemination of drug knowledge – lack of information on drug dosage and routes, interactions, and contraindications – was the most common systems failure, followed by dose and identity checking.
Experimental determination of the risks of medication errors
In a systematic analysis of error rates at different stages in the administration of intravenous medicines, reported rates varied widely [15]. Experimental studies would allow the fractional error rates for each step in the complex process to be estimated. That would help to identify the areas of highest risk. However, there are relatively few identifiable simulation studies of medication errors.
One particular cognitive challenge in prescribing and giving medicines is dosage calculation. Lesar et al. reported that more than one in six prescribing errors involved miscalculation of dose, wrong decimal point placement, incorrect expression of unit of measurement, or an incorrect medication administration rate [19]. Calculation errors were more likely to occur in paediatric settings.
In an early study, paediatric staff were asked to calculate doses. In 8% of calculations, nurses made a 10-fold error; paediatricians did so 4% of the time [20, 21]. Experienced nurses made as many errors as inexperienced nurses, but were more confident of their abilities [22]. When teams of paediatric staff were observed undertaking simulated resuscitation tasks, there were 10-fold errors in dosing on 3% of occasions [23]. The rate of 10-fold errors was higher in a separate study of paediatric resident doctors [24].
Physicians, nurses, pharmacists, and pharmacy technicians all had difficulty in calculating drug doses in a non-clinical environment, with an error rate of 5% [95% confidence interval (CI) 3.7, 6.2][25]. Risks were associated with the number of infusions prepared in the previous week, number of years' professional experience, and profession. When healthcare professionals were asked to prepare intravenous infusions for use in neonates, 161/464 infusions (35%, 95% CI 30, 39) were made up in the wrong concentration.
During a simulated resuscitation task, the concentration of injectate differed from the expected concentration by >50% in 7% of cases [23].
Garnerin et al.[26] measured the error rates in (i) the arithmetical calculations required to prepare an injection; and (ii) the manual task of preparation. The measured rates of error in the arithmetic task were 24% for nurses and 9% for anaesthetists. For preparation, they were 3% for nurses and 7% for anaesthetists.
Pharmacists and students, asked to identify newly coined drug names, misclassified one in eight, and the misclassification rate was highest for those names that most closely resembled existing drug names [27].
Patients were likely to misinterpret labelled instructions on medicines; the rates of misunderstanding the instruction ‘Take one tablet by mouth twice daily for seven days’ were 27% for patients with good literacy skills and 48% for patients with poor literacy skills [28].
An analysis of the potential flaws in the administration of intravenous infusions in an intensive care unit led to the introduction of a simple infusion dosage calculator and a substantial reduction in the predicted error rate. There was, however, no direct demonstration that the calculated error rates corresponded to those occurring in practice [29].
Factors that alter the risk of errors
The data on risk quoted in Tables 1 and 2 suggest that tasks are associated with some intrinsic risk. Routine and well-specified tasks are less likely to be risky than novel or poorly specified tasks. Tasks that carry a high cognitive burden, for example, are susceptible to mistakes. On the other hand, when two tasks that are largely automatic have similar schemata, there is a risk that inattention will allow a slip from one schema to the other [9]. Driving home (‘on auto-pilot’) rather than driving to the supermarket would be an everyday example.
The overall safety of a system depends heavily on checking for errors during the process, but an analysis of three healthcare incidents concluded that routine collaborative cross-checking had not been effective [30].
The intrinsic risk can be modified by other factors. In the context of medication errors, these include: factors relating to the person performing the action; the possibility that other people will supervise or intervene; the circumstances in which the action is performed; the state of the patient; and particular characteristics of the medicine.
The person performing the action
Some people are more likely to err than others for constitutive (‘canonical’) reasons, such as their intrinsic thoroughness, hesitancy, or perfectionism [31]. Overlaid on this ‘differential accident involvement’ are other factors that can increase or reduce the likelihood of error. In a large prospective Australian study of anaesthetists, one or more of the following factors was thought to be present when medication errors occurred: inattention (37% of medication errors); haste (39%); distraction (27%); and fatigue (11%) [32].
An analysis of 1305 errors made by nursing students, reported to the American MEDMARX Patient Safety programme, identified inexperience (78%) and distractions (20%) as the principal factors contributing to the errors [33]. In a paediatric emergency department, errors were more likely to be committed by junior doctors [odds ratio (OR) 1.64; 95% CI 1.06, 2.52] and in seriously ill patients (OR 1.55; 95% CI 1.06, 2.26), even after controlling for patient age, waiting time, and other factors [34].
In a prospective study of prescribing errors in an eye hospital, drug-related errors were identified in 15/1808, all made by junior doctors and none by senior doctors. Conversely, senior doctors made just as many errors as junior doctors in writing prescriptions [35].
In a Dutch hospital study, the OR for an error by prescribers in orthopaedics was 3.36 (95% CI 2.08, 5.41), and for nursing staff 2.53 (95% CI 1.77, 3.62) compared with the average rate for staff in a large hospital [36].
The mental state of the prescriber might influence susceptibility to error. In a questionnaire study of 123 paediatric residents, the 17 who were depressed were six times as likely to describe making a medication error as those who were not, whereas the 77 described as ‘burnt out’ had average error rates [37].
Training
Training can reduce error rates, for example in resuscitation drills. Up to now there has been little direct evidence that training before qualification reduces medication error rates after qualification. There is some evidence that students cope better with Objective Structured Clinical Examinations of prescribing skills over time [38].
Site
The risk of harm from medications in hospital depends on the type of ward. Rates, expressed as adverse events per 1000 patient-days per drug used, were twice as high on medical intensive care units as on surgical ones [39]. Several other studies have shown high rates of medication errors in intensive care units [40–42]. Part of the explanation may lie in the higher rate of prescribing errors in critical care units, where the prescriber may not have immediate access to critical information such as drug allergies, drug–drug interactions, or concomitant medical conditions [43].
Drug use on neonatal units entails especially high risks of medication error, partly because the doses used in treating babies weighing 1 or 2 kg are very small compared with doses used in older children and adults, but the size of a drug vial is geared to adults. Almost one-third of intravenous drug prescriptions observed on one paediatric unit were for less than a tenth of the contents of a single vial [44].
In a 6-month prospective analysis of medication order errors in a large Israeli hospital, the surgical ward had the highest number of errors, followed by internal medicine [45]. Prescribing errors in outpatients seem less common (7.6% in one study) [46].
Time
Wright et al. examined a surgical database of 130 912 operating room cases over a 4-year period [47]. Operating cases that began in the late afternoon were significantly more likely to experience adverse events than cases begun at other times. The authors suggested that this may have been a result of several factors such as patient characteristics, fatigue, and case workload.
Working conditions
Taxis et al. identified several error-producing conditions associated with intravenous medication errors [48]. Lack of knowledge of the preparation procedure and inadequate use of technology were the most common failures. The authors also highlighted the role of the technology – poorly designed equipment or unsuitable preparation procedures – in producing errors, and lack of appropriate training and failure to involve pharmacists as important latent errors.
In Dean's prospective analysis of prescribing errors in hospital [49], the following were all identified as error-producing: working conditions (insufficient staffing levels, heavy workload); the team (lack of communication); the individual (fatigue, hunger, lack of skills or knowledge); and task factors.
Nichols et al. carried out face-to-face interviews with 26 medical staff members who had been involved in a medication error [50]. There were 21 slips or lapses, and eight knowledge-based mistakes. All administration and dispensing errors were caused by errors in attention or lapses in memory. The healthcare professionals responded that slips or lapses were more likely to occur when they were busy, tired, or distracted.
In a large direct-observation study of drug administration errors in a paediatric teaching hospital over 1 year, 27% of administrations contained an error [51]. Nurses who worked full-time in the unit were less likely to make a medicine administration error. The authors suggested that the high error rate might have been due to the lack of training and the limited familiarity of nursing students or temporary staff with paediatric dosage forms.
Landrigan et al. examined the effect of an intervention schedule that eliminated extended work shifts and reduced the number of hours worked per week [52]. Interns made significantly fewer serious medical errors during the intervention schedule than in the traditional schedule (100 compared with 136 errors per 1000 patient-days).
In a study in two Dutch intensive care units, at least one administration error was associated with 33% of medications administered (when time errors were excluded) [53]. There were more errors with gastrointestinal drugs and more errors on Mondays.
In a large observational study of a cardiovascular thoracic surgery unit and a geriatric unit, medication administration errors were associated with a high nurse workload and incomplete or illegible prescriptions [54].
Several studies have reported an increased incidence in errors due to stress [55, 56], fatigue [56–59], and heavy workload [49, 60].
In a review of potential adverse events in 132 Japanese long-term psychiatric care units the registered nurse ratio – the ratio of registered nurses to assistant nurses – was a significant predictor of potential wrong drug administration events [61].
Qualitative interviews with nurses who had made a drug administration error over the course of a 12-month study identified specific factors that the nurses felt contributed to the error, including: work load; poor skill mix; interruptions; loss of concentration; lack of knowledge; and tiredness or sickness [62].
Psychiatric nurses identified specific factors believed to have contributed to medication administration errors, including: busy, noisy wards; staff shortages; failures in communication; confusion over similar-sounding drug names; and problems with the physical layout of the drug administration area [63].
The patient
A meta-analysis showed that the proportion of admissions to hospital with adverse drug reactions that were preventable was much higher in elderly than in younger adults [64].
In a review of medical records from hospitals in two American states there was a significantly higher incidence of preventable drug-related adverse events in patients aged >64 than in patients aged 16–64 years (5% compared with 3%) [65].
Errors are also significantly more likely in children. An inpatient study using a prospective chart review showed that the rate of ‘near-miss’ errors in children was three times the rate in adult patients [66].
Raju et al. undertook a prospective analysis of incident reports over 4 years from a paediatric and neonatal intensive care unit [67]. During the study period 2147 patients were admitted and 315 medication error incident reports were submitted. Wrong time was the commonest type of error. Errors were most frequent during the day shift, although this was most probably due to the large number of prescriptions issued during the day.
Haw et al. undertook a retrospective analysis of medication administration errors reported in a UK psychiatric hospital. The majority of errors (53%) were reported by the adolescent division, compared with only 3% among elderly patients [63].
The medicine
In a retrospective review of medication errors reported over a 4-year period in a large paediatric hospital, antibiotics were the commonest drugs and the intravenous route was the commonest (56%) route involved [68].
In a large 9-year study of prescribing errors in a teaching hospital, antimicrobials (34%), cardiovascular agents (16%) and gastrointestinal agents (7%) were identified as the three drug classes most commonly involved in prescription errors [69].
In a systematic review, three drug classes most commonly associated with preventable drug-related hospital admissions were identified: antiplatelet drugs (including aspirin when used as an antiplatelet drug), diuretics, and non-steroidal anti-inflammatory drugs [70]. According to another review, errors were more likely with medications used in the eyes (OR 11; 95% CI 4.3, 29) or for inhalation (OR 4; 95% CI 2.6, 6.6) [36]. In a prospective study, anti-infective drugs accounted for most errors (39%) [46].
Han et al. undertook a prospective study of intravenous fluid administration errors in a surgical ward over a 4-week period. The lack of permanent staff and the presence of peripheral lines contributed to administration errors. The level of nurse experience, the time of drug administration, and the patient's sex were not associated with an increased risk of errors [71].
The risk of harm from over-sedation in children increased substantially when more than two drugs were used: with three drugs 13/15 episodes resulted in death or permanent neurological damage compared with 24/45 when only one drug was used [72].
Computer assistance
Potts et al. studied the impact of computer physician order entry on medication errors in a paediatric critical care unit [73]. The rate of medication prescribing errors fell significantly from 30 per 100 orders to 0.2 per 100 errors. The rates of potential adverse drug events and rule violations also fell significantly.
In a prospective study in three units, of which two used paper-based prescribing and one computer-based prescribing, minor medication prescribing errors were significantly lower in the computer-based unit (0.7 per 100 orders) than in the paper-based unit (18 per 100 orders) [74]. Serious prescribing errors were also significantly less common in the computer-based unit. However, the authors reported that the computer system introduced two new types of errors: double prescriptions and insufficient drug monitoring information.
When a computerized system offers ‘decision support’, i.e. provides the user with knowledge and warning, the information is often ignored. In one hospital study, 80% of allergy warnings were overridden. In general practice >90% of alerts were over-ridden [75]. While ‘the over-rides were deemed clinically justifiable’, 6% of patients may have experienced an adverse reaction as a result [76].
In a residential care setting many alerts were disregarded and the number of appropriate prescribing decisions was only slightly increased compared with a control setting in which alerts were not displayed [77]. Overall, a systematic review found that 50–90% of all alerts were overridden [78]. Since alerts are perceived as criticism, it has been suggested that effective systems might be more readily espoused if they also provided congratulations – positive feedback [79].
Garg et al. systematically reviewed 97 studies of computerized decision support and concluded that many systems improved practitioner performance. ‘To date, the effects on patient outcomes remain understudied, and, when studied, inconsistent’[80].
In the UK, where hospital prescribing is usually paper based, introduction of a computer-based prescribing system halved prescribing errors in a small before-and-after study on a surgical ward [81]. In a separate study, based on an intensive care unit, error rates fell from 6.5 to 4.8%, mainly because of the reduction in errors of omission, although the computer system was responsible for at least one important error related to a drop-down menu: that is to say, when the operator had to perform cognitive tasks [82]. An analysis of a dosing error that led to a dangerous overdose of potassium solution found errors ‘in several converging aspects of the drug ordering process: confusing on-screen laboratory results review, system usability difficulties, user training problems, and suboptimal clinical system safeguards’[83].
Conclusion
Medication errors are no different in their genesis from other human errors: some result from poor knowledge or defective plans, and some from the unavoidable slips and lapses that are inevitable dangers in routine acts. Checking should intercept errors, but what little evidence is available suggests that routine checking is sometimes little more than ritual. While computers can effectively reduce the rates of easily counted errors, there is much less evidence that they can save lives lost through rare but dangerous errors in the medication process.
Footnotes
If there are n steps and the probability of correct execution of step i is Pi, the probability of the whole process being faultless is: 
Competing interests
None to declare.
S.E.M. was supported by the Antidote Trust Fund of Sandwell and West Birmingham Hospitals NHS Trust.
REFERENCES
- 1.Simpson J, Weiner E. Oxford English dictionary. Online]. Available at http://dictionary.oed.com/ (last accessed 21 January 2009.
- 2.Reason JT. Human Error. Cambridge: Cambridge University Press; 1990. [Google Scholar]
- 3.Mach E. Knowledge and error. In: McGuinness B, editor. Knowledge and error: sketches on the psychology of enquiry. Dordrecht: D. Reidel Publishing Company; 1975. p. 79.p. 91. [Google Scholar]
- 4.Vincent C, Ennis M, Audley RJ. Medical Accidents. Oxford: Oxford University Press; 1993. [Google Scholar]
- 5.Leape LL. A systems analysis approach to medical error. In: Cohen MR, editor. Medication Errors. Washington, DC: American Pharmaceutical Association; 1999. pp. 2.1–2.14. [Google Scholar]
- 6.Kirwan B. A Guide to Practical Human Reliability Assessment. London: Taylor & Francis; 1994. [Google Scholar]
- 7.Kirwan B. Human-error analysis. In: Kirwan B, editor. A Guide to Practical Human Reliability Assessment. London: Taylor & Francis; 1994. p. 79.p. 182. [Google Scholar]
- 8.Fennerty A, Dolben J, Thomas P, Backhouse G, Bentley DP, Campbell IA, Routledge PA. Flexible induction dose regimen for warfarin and predication of maintenance dose. BMJ. 1984;288:1268–70. doi: 10.1136/bmj.288.6426.1268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Norman DA. Categorization of action slips. Psychol Rev. 1981;88:1–15. [Google Scholar]
- 10.Shallice T. Specific impairments of planning. Philos Trans R Soc Lond B. 1982;298:199–209. doi: 10.1098/rstb.1982.0082. [DOI] [PubMed] [Google Scholar]
- 11.Faddis MO. Eliminating errors in medication. Am J Nurs. 1939;39:1217–23. [Google Scholar]
- 12.Ferner RE. The epidemiology of medication errors: the methodological difficulties. Br J Clin Pharmacol. 2009;67:614–20. doi: 10.1111/j.1365-2125.2009.03417.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ferner RE, Aronson JK. Clarification of terminology in medication errors: definitions and classification. Drug Saf. 2006;29:1011–22. doi: 10.2165/00002018-200629110-00001. [DOI] [PubMed] [Google Scholar]
- 14.Lane R, Stanton NA, Harrison D. Applying hierarchical task analysis to medication administration errors. Appl Ergon. 2006;37:669–79. doi: 10.1016/j.apergo.2005.08.001. [DOI] [PubMed] [Google Scholar]
- 15.McDowell SE, Mt-Isa S, Ashby D, Ferner RE. Where errors occur in the preparation and administration of intravenous medicines: a systematic review and Bayesian analysis. Qual Saf Health Care; in press. [DOI] [PubMed]
- 16.Kirwan B. The validation of three human reliability quantification techniques – THERP, HEART and JHEDI: part 1 – technique descriptions and validation issues. Appl Ergon. 1996;27:359–73. doi: 10.1016/s0003-6870(96)00044-0. [DOI] [PubMed] [Google Scholar]
- 17.Berwick D, Nolan T. High reliability health care. Presented at the Institute for Healthcare Improvement's 15th Annual National Forum on Quality Improvement in Health Care in New Orleans, Louisiana, USA. December 2003.
- 18.Leape LL, Bates DW, Cullen DJ, Cooper J, Dermonaco HJ, Gallivan T, Hallisey R, Ives J, Laird N, Laffel G. Systems analysis of adverse drug events. JAMA. 1995;274:35–43. [PubMed] [Google Scholar]
- 19.Lesar TS, Briceland L, Stein DS. Factors related to errors in medication prescribing. JAMA. 1997;277:312–7. [PubMed] [Google Scholar]
- 20.Perlstein PH, Callison C, White M, Barnes B, Edwards NK. Errors in drug computations during newborn intensive care. Am J Dis Child. 1979;133:376–9. doi: 10.1001/archpedi.1979.02130040030006. [DOI] [PubMed] [Google Scholar]
- 21.Koren G, Barzilay Z, Modan M. Errors in computing drug doses. Can Med Assoc J. 1983;129:721–3. [PMC free article] [PubMed] [Google Scholar]
- 22.Perlstein PH, Callison C, White M, Barnes B, Edwards NK. Errors in drug computations during newborn intensive care. Am J Dis Child. 1979;133:376–9. doi: 10.1001/archpedi.1979.02130040030006. [DOI] [PubMed] [Google Scholar]
- 23.Kozer E, Seto W, Verjee Z, Parshuram C, Khattak S, Koren G, Jarvis DA. Prospective observational study on the incidence of medication errors during simulated resuscitation in a paediatric emergency department. BMJ. 2004;329:1321. doi: 10.1136/bmj.38244.607083.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rowe C, Koren T, Koren G. Errors by paediatric residents in calculating drug doses. Arch Dis Child. 1998;79:56–8. doi: 10.1136/adc.79.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Parshuram CS, To T, Seto W, Trope A, Koren G, Laupacis A. Systematic evaluation of errors occurring during the preparation of intravenous medication. CMAJ. 2008;178:42–8. doi: 10.1503/cmaj.061743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Garnerin P, Pellet-Meier B, Chopard P, Perneger T, Bonnabry P. Measuring human-error probabilities in drug preparation: a pilot simulation study. Eur J Clin Pharmacol. 2007;63:769–76. doi: 10.1007/s00228-007-0319-z. [DOI] [PubMed] [Google Scholar]
- 27.Lambert BL, Chang KY, Lin SJ. Effect of orthographic and phonological similarity on false recognition of drug names. Soc Sci Med. 2001;52:1843–57. doi: 10.1016/s0277-9536(00)00301-4. [DOI] [PubMed] [Google Scholar]
- 28.Davis TC, Wolf MS, Bass PF, 3rd, Thompson JA, Tilson HH, Neuberger M, Parker RM. Literacy and misunderstanding prescription drug labels. Ann Intern Med. 2006;145:887–94. doi: 10.7326/0003-4819-145-12-200612190-00144. [DOI] [PubMed] [Google Scholar]
- 29.Apkon M, Leonard J, Probst L, DeLizio L, Vitale R. Design of a safer approach to intravenous drug infusions: failure mode effects analysis. Qual Saf Health Care. 2004;13:265–71. doi: 10.1136/qshc.2003.007443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Patterson ES, Woods DD, Cook RI, Render ML. Collaborative cross-checking to enhance resilience. Cogn Tech Work. 2007;9:155–62. [Google Scholar]
- 31.McManus C, Vincent C. Selecting and educating safer doctors. In: Vincent C, Ennis M, Audley RJ, editors. Medical Accidents. Oxford: Oxford University Press; 1993. pp. 80–105. [Google Scholar]
- 32.Abeysekera A, Bergman IJ, Kluger MT, Short TG. Drug error in anaesthetic practice: a review of 896 reports from the Australian incident monitoring study database. Anaesthesia. 2005;60:220–7. doi: 10.1111/j.1365-2044.2005.04123.x. [DOI] [PubMed] [Google Scholar]
- 33.Wolf ZR, Hicks R, Serembus JF. Characteristics of medication errors made by students during the administrative phase: a descriptive study. J Prof Nurs. 2006;22:39–51. doi: 10.1016/j.profnurs.2005.12.008. [DOI] [PubMed] [Google Scholar]
- 34.Kozer E, Scolnik D, Macpherson A, Keays T, Shi K, Luk T, Koren G. Variables associated with medication errors in pediatric emergency medicine. Pediatrics. 2002;110:737–42. doi: 10.1542/peds.110.4.737. [DOI] [PubMed] [Google Scholar]
- 35.Mandal K, Fraser SG. The incidence of prescribing errors in an eye hospital. BMC Ophthalmol. 2005;5:4. doi: 10.1186/1471-2415-5-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Fijn R, van den Bemt PM, Chow M, De Blaey CJ, De Jong-Van den Berg LT, Brouwers JR. Hospital prescribing errors: epidemiological assessment of predictors. Br J Clin Pharmacol. 2002;53:326–31. doi: 10.1046/j.0306-5251.2001.bjcp1558.doc.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Fahrenkopf AM, Sectish TC, Barger LK, Sharek PJ, Lewin D, Chiang VW, Edwards S, Wiedermann BL, Landrigan CP. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336:488–91. doi: 10.1136/bmj.39469.763218.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Langford NJ, Martin U, Kendall MJ, Ferner RE. Medical errors. Medical schools can teach safe drug prescribing and administration. BMJ. 2001;322:1424. [PubMed] [Google Scholar]
- 39.Bates DW, Cullen DJ, Laird N, Petersen LA, Small SD, Servi D, Laffel G, Sweitzer BJ, Shea BF, Hallisey R. Incidence of adverse drug events and potential adverse drug events: implications for prevention. JAMA. 1995;274:29–34. [PubMed] [Google Scholar]
- 40.Schneider MP, Cotting J, Pannatier A. Evaluation of nurses' errors associated in the preparation and administration of medication in a pediatric intensive care unit. Pharm World Sci. 1998;20:178–82. doi: 10.1023/a:1012087727393. [DOI] [PubMed] [Google Scholar]
- 41.Tissot E, Cornette C, Demoly P, Jacquet M, Barale F, Capellier G. Medication errors at the administration stage in an intensive care unit. Intensive Care Med. 1999;25:353–9. doi: 10.1007/s001340050857. [DOI] [PubMed] [Google Scholar]
- 42.Calabrese AD, Erstad BL, Brandl K, Barletta JF, Kane SL, Sherman DS. Medication administration errors in adult patients in the ICU. Intensive Care Med. 2001;27:1592–8. doi: 10.1007/s001340101065. [DOI] [PubMed] [Google Scholar]
- 43.Ridley SA, Booth SA, Thompson CM. Prescription errors in UK critical care units. Anaesthesia. 2004;59:1193–200. doi: 10.1111/j.1365-2044.2004.03969.x. [DOI] [PubMed] [Google Scholar]
- 44.Chappell K, Newman C. Potential tenfold drug overdoses on a neonatal unit. Arch Dis Child Fetal Neonatal Ed. 2004;89:F483, 4. doi: 10.1136/adc.2003.041608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lustig A. Medication error prevention by pharmacists – an Israeli solution. Pharm World Sci. 2000;22:21–5. doi: 10.1023/a:1008774206261. [DOI] [PubMed] [Google Scholar]
- 46.Gandhi TK, Weingart SN, Seger AC, Borus J, Burdick E, Poon EG, Leape LL, Bates DW. Outpatient prescribing errors and the impact of computerized prescribing. J Gen Intern Med. 2005;20:837–41. doi: 10.1111/j.1525-1497.2005.0194.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wright MC, Phillips-Bute B, Mark JB, Stafford-Smith M, Grichnik KP, Andregg BC, Taekman JM. Time of day effects on the incidence of anaesthetic adverse events. Qual Saf Health Care. 2006;15:258–63. doi: 10.1136/qshc.2005.017566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Taxis K, Barber N. Causes of intravenous medication errors: an ethnographic study. Qual Saf Health Care. 2003;12:343–8. doi: 10.1136/qhc.12.5.343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Dean B, Schachter M, Vincent C, Barber N. Causes of prescribing errors in hospital inpatients: a prospective study. Lancet. 2002;359:1373–8. doi: 10.1016/S0140-6736(02)08350-2. [DOI] [PubMed] [Google Scholar]
- 50.Nichols P, Copeland TS, Craib IA, Hopkins P, Bruce DG. Learning from error: identifying contributory causes of medication errors in an Australian hospital. Med J Aust. 2008;188:276–9. doi: 10.5694/j.1326-5377.2008.tb01619.x. [DOI] [PubMed] [Google Scholar]
- 51.Prot S, Fontan JE, Alberti C, Bourdon O, Farnoux C, Macher MA, Foureau A, Faye A, Beaufils F, Gottot S, Brion F. Drug administration errors and their determinants in pediatric in-patients. Int J Qual Health Care. 2005;17:381–9. doi: 10.1093/intqhc/mzi066. [DOI] [PubMed] [Google Scholar]
- 52.Landrigan CP, Rothschild JM, Cronin JW, Kaushal R, Burdick E, Katz JT, Lilly CM, Stone PH, Lockley SW, Bates DW, Czeisler CA. Effect of reducing interns' work hours on serious medical errors in intensive care units. N Engl J Med. 2004;351:1838–48. doi: 10.1056/NEJMoa041406. [DOI] [PubMed] [Google Scholar]
- 53.van den Bemt PM, Fijn R, van der Voort PH, Gossen AA, Egberts TC, Brouwers JR. Frequency and determinants of drug administration errors in the intensive care unit. Crit Care Med. 2002;30:846–50. doi: 10.1097/00003246-200204000-00022. [DOI] [PubMed] [Google Scholar]
- 54.Tissot E, Cornette C, Limat S, Mourand JL, Becker M, Etievent JP, Dupond JL, Jacquet M, Woronoff-Lemsi MC. Observational study of potential risk factors of medication administration errors. Pharm World Sci. 2003;25:264–8. doi: 10.1023/b:phar.0000006519.44483.a0. [DOI] [PubMed] [Google Scholar]
- 55.Reilley S, Grasha AF, Schafer J. Workload, error detection, and experienced stress in a simulated pharmacy verification task. Percept Mot Skills. 2002;95:27–46. doi: 10.2466/pms.2002.95.1.27. [DOI] [PubMed] [Google Scholar]
- 56.Sexton JB, Thomas EJ, Helmreich RL. Error, stress, and teamwork in medicine and aviation: cross sectional surveys. BMJ. 2000;320:745–9. doi: 10.1136/bmj.320.7237.745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Gander PH, Merry A, Miller MM, Weller J. Hours of work and fatigue-related error: a survey of New Zealand anaesthetists. Anaesth Intensive Care. 2000;28:178–83. doi: 10.1177/0310057X0002800209. [DOI] [PubMed] [Google Scholar]
- 58.Gaba DM. Human error in anaesthetic mishaps. Int Anesthesiol Clin. 1989;27:137–47. doi: 10.1097/00004311-198902730-00002. [DOI] [PubMed] [Google Scholar]
- 59.Gravenstein JS, Cooper JB, Orkin FK. Work and rest cycles in anesthesia practice. Anesthesiology. 1990;72:737–42. doi: 10.1097/00000542-199004000-00024. [DOI] [PubMed] [Google Scholar]
- 60.Seki Y, Yamazaki Y. Effects of working conditions on intravenous medication errors in a Japanese hospital. J Nurs Manag. 2006;14:128–39. doi: 10.1111/j.1365-2934.2006.00597.x. [DOI] [PubMed] [Google Scholar]
- 61.Ito H, Yamazumi S. Common types of medication errors on long-term psychiatric care units. Int J Qual Health Care. 2003;15:207–12. doi: 10.1093/intqhc/mzg038. [DOI] [PubMed] [Google Scholar]
- 62.Gladstone J. Drug administration errors: a study into the factors underlying the occurrence and reporting of drug errors in a district general hospital. J Adv Nurs. 1995;22:628–37. doi: 10.1046/j.1365-2648.1995.22040628.x. [DOI] [PubMed] [Google Scholar]
- 63.Haw CM, Dickens G, Stubbs J. A review of medication administration errors reported in a large psychiatric hospital in the United Kingdom. Psychiatr Serv. 2005;56:1610–3. doi: 10.1176/appi.ps.56.12.1610. [DOI] [PubMed] [Google Scholar]
- 64.Beijer HJ, de Blaey CJ. Hospitalisations caused by adverse drug reactions (ADR): a meta-analysis of observational studies. Pharm World Sci. 2002;24:46–54. doi: 10.1023/a:1015570104121. [DOI] [PubMed] [Google Scholar]
- 65.Thomas EJ, Brennan TA. Incidence and types of preventable adverse events in elderly patients: population based review of medical records. BMJ. 2000;320:741–4. doi: 10.1136/bmj.320.7237.741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Kaushal R, Bates DW, Landrigan C, McKenna KJ, Clapp MD, Federico F, Goldmann DA. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285:2114–20. doi: 10.1001/jama.285.16.2114. [DOI] [PubMed] [Google Scholar]
- 67.Raju TN, Kecskes S, Thornton JP, Perry M, Feldman S. Medication errors in neonatal and paediatric intensive-care units. Lancet. 1989;2:374–6. doi: 10.1016/s0140-6736(89)90548-5. [DOI] [PubMed] [Google Scholar]
- 68.Ross LM, Wallace J, Paton JY. Medication errors in a paediatric teaching hospital in the UK: five years operational experience. Arch Dis Child. 2000;83:492–7. doi: 10.1136/adc.83.6.492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Lesar TS, Lomaestro BM, Pohl H. Medication-prescribing errors in a teaching hospital: a 9-year experience. Arch Intern Med. 1997;157:1569–76. [PubMed] [Google Scholar]
- 70.Howard RL, Avery AJ, Slavenburg S, Royal S, Pipe G, Lucassen P, Pirmohamed M. Which drugs cause preventable admissions to hospital? A systematic review. Br J Clin Pharmacol. 2006;63:136–47. doi: 10.1111/j.1365-2125.2006.02698.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Han PY, Coombes ID, Green G. Factors predictive of intravenous fluid administration errors in Australian surgical care wards. Qual Saf Health Care. 2005;14:179–84. doi: 10.1136/qshc.2004.010728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Coté CJ, Karl HW, Notterman DA, Weinberg JA, McCloskey C. Adverse sedation events in pediatrics: analysis of medications used for sedation. Pediatrics. 2000;106:633–44. doi: 10.1542/peds.106.4.633. [DOI] [PubMed] [Google Scholar]
- 73.Potts AL, Barr FE, Gregory DR, Wright L, Patel NR. Computerized physician order entry and medication errors in a pediatric critical care unit. Pediatrics. 2004;113:59–63. doi: 10.1542/peds.113.1.59. [DOI] [PubMed] [Google Scholar]
- 74.Colpaert K, Claus B, Somers A, Vandewoude K, Robays HD. Impact of computerized physician order entry on medication prescription errors in the intensive care unit: a controlled cross-sectional trial. Crit Care. 2006;10:R21. doi: 10.1186/cc3983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Weingart SN, Toth M, Sands DZ, Aronson MD, Davis RB, Phillips RS. Physicians' decisions to override computerized drug alerts in primary care. Arch Intern Med. 2003;163:2625–31. doi: 10.1001/archinte.163.21.2625. [DOI] [PubMed] [Google Scholar]
- 76.Hsieh TC, Kuperman GJ, Jaggi T, Hojnowski-Diaz P, Fiskio J, Williams DH, Bates DW, Gandhi TK. Characteristics and consequences of drug allergy alert overrides in a computerized physician order entry system. J Am Med Inform Assoc. 2004;11:482–91. doi: 10.1197/jamia.M1556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Judge J, Field TS, DeFlorio M, Laprino J, Auger J, Rochon P, Bates DW, Gurwitz JH. Prescribers' responses to alerts during medication ordering in the long term care setting. J Am Med Inform Assoc. 2006;13:385–90. doi: 10.1197/jamia.M1945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.van der Sijs H, Aarts J, Vulto A, Berg M. Overriding of drug safety alerts in computerized physician order entry. J Am Med Inform Assoc. 2006;13:138–47. doi: 10.1197/jamia.M1809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Sittig DF, Krall M, Kaalaas-Sittig J, Ash JS. Emotional aspects of computer-based provider order entry: a qualitative study. J Am Med Inform Assoc. 2005;12:561–7. doi: 10.1197/jamia.M1711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Garg AX, Adhikari NK, McDonald H, Rosas-Arellano MP, Devereaux PJ, Beyene J, Sam J, Haynes RB. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review. JAMA. 2005;293:1223–38. doi: 10.1001/jama.293.10.1223. [DOI] [PubMed] [Google Scholar]
- 81.Donyai P, O'Grady K, Jacklin A, Barber N, Dean Franklin B. The effects of electronic prescribing on the quality of prescribing. Br J Clin Pharmacol. 2007;65:230–7. doi: 10.1111/j.1365-2125.2007.02995.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Shulman R, Singer M, Goldstone J, Bellingan J. Medication errors: a prospective cohort study of hand-written and computerised physician order entry in the intensive care unit. Crit Care. 2005;9:R516, 21. doi: 10.1186/cc3793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Horsky J, Kuperman GJ, Patel VL. Comprehensive analysis of a medication dosing error related to CPOE. J Am Med Inform Assoc. 2005;12:377–82. doi: 10.1197/jamia.M1740. [DOI] [PMC free article] [PubMed] [Google Scholar]