

Abstract
Objectives
To examine trends in mortality among babies registered solely by their mother (lone mothers) and to compare these with trends in infant mortality for couple registrations overall and couple registrations subdivided by social class of father.
Design
Analysis of trends in infant death rates from 1975 to 1996 for the three groups. The data source was the national linked infant mortality file, containing all records of infant death in England and Wales linked to the respective birth records.
Setting
England and Wales.
Participants
All live births (n=14.3 million) from 1975 to 1996; all deaths of infants from birth to 12 months of age over the same period (n=135 800).
Main outcome measures
Death rates in the perinatal, neonatal, and postneonatal periods and for infancy overall.
Results
For the babies of lone mothers infant mortality has fallen to less than a third of the 1975 level, with a clear reduction in the gap between the mortality in these babies compared with all couple registrations: the excess mortality in solely registered births was 79% in 1975 reducing to 33% in 1996. Most of the narrowing of the sole-couple differential was associated with the neonatal period, for which there is now no appreciable gap. For couple registrations analysed by social class of father, infant death rates have more than halved in each social class from 1975 to 1996. The reductions in mortality were greater in the late 1970s and early 1990s. Infant death rates in classes IV-V remained between 50% and 65% higher than in classes I-II. Differentials between social classes were largest in the postneonatal period and smallest in the perinatal and neonatal periods. The gap in perinatal and neonatal mortality between the babies of lone mothers and couple parents in social classes IV-V has disappeared.
Conclusions
The differential in infant mortality between social classes still exists, whereas the differential between sole and couple registrations has decreased, showing positive progress in the reduction of inequalities. As the reduction in the differential was confined to the neonatal period these improvements may be more a reflection of healthcare factors than of factors associated with lone mothers’ social and economic circumstances.
Key messages
Social inequalities in infant mortality are widely regarded as unacceptable and as a spur to action
Babies of lone mothers and those born to couple parents in manual social classes continue to be at higher risk of infant mortality
From 1975 to 1996 the differential in infant mortality between social classes for babies of couple parents showed little tendency to narrow, whereas there was a clear improvement in the mortality differential between the babies of lone and couple parents
The pattern of reduction in the lone-couple differential—confined to the neonatal period—suggests that healthcare factors may have made a major contribution to the observed improvement
In contrast, the lack of improvement of the differentials in postneonatal mortality add to the concern that insufficient progress is being made in this critical period of babies’ lives with the groups at greatest risk
Introduction
Infant mortality has long been accepted as an important indicator of a population’s health, with evidence of any social differentials in this indicator regarded as particularly unacceptable and a spur to action. The traditional way of analysing social trends in infant mortality, often limited to births inside marriage by social class of father, has, however, become increasingly problematic as growing numbers of infants are excluded from such an analysis, not least the babies of lone mothers.
Over the past 20 years there has been a clear reduction in the proportion of births registered within marriage in England and Wales,1 and this trend has been accentuated in manual social classes. Table 1 shows that while 90% or more of live births in each of the six social classes occurred within marriage in the mid-1970s, by 1996 only 89% of registrations in social class I were within marriage in 1996, reducing to 51% of births in social class V. Furthermore, inspection of mortality data from the Office for National Statistics shows that in every year since 1990 there have been more deaths in social class V babies born outside than inside marriage.2
Table 1.
Proportions (percentages) of live births within marriage by social class of father, England and Wales, 1975 to 1996*
| Year | Social class
|
|||||
|---|---|---|---|---|---|---|
| I | II | IIIN | IIIM | IV | V | |
| 1975-7 | 98 | 97 | 97 | 94 | 93 | 90 |
| 1985-7 | 96 | 91 | 90 | 82 | 80 | 68 |
| 1994-6 | 89 | 82 | 79 | 65 | 63 | 51 |
Source: Office for National Statistics birth statistics, various years. Note: percentages may not add up because of rounding.
A second distinct group commonly excluded from the traditional analyses of social trends in mortality consists of babies registered outside marriage solely by their mothers. Table 2 shows that the size of this group has increased from 5% of births in 1975 to 8% in 1996. The social class of the father is not available from these records, and it has not been possible to assign a social class on the basis of the mother’s occupation to most births until the last few years as occupation of the mother has only been recorded at registration since 1986 and then only on a voluntary basis, with slow take up of this option in the early years. We believe, however, that this category consists largely of the babies born outside marriage to lone mothers and that they form a potentially vulnerable group in society. In Britain, a high proportion of lone mothers live in poverty,3,4 and their children not only face socioeconomic disadvantage but are known to have higher risks of health problems such as accidents and infections.5,6 It is therefore important to include this previously excluded group in any consideration of socioeconomic trends in infant mortality in this country.
Table 2.
Proportions (percentages) of live births by type of registration category, England and Wales, 1975 to 1996*
| Year | Solely by mother | Inside marriage | Jointly registered outside marriage | Average No of live births per year |
|---|---|---|---|---|
| 1975-7 | 5 | 91 | 5 | 585 700 |
| 1985-7 | 7 | 79 | 14 | 666 300 |
| 1994-6 | 8 | 66 | 27 | 654 100 |
Source Office for National Statistics birth statistics, various years. Note: percentages may not add up because of rounding.
We analysed trends in mortality in babies of lone mothers and compared these with mortality trends in babies of couple parents from different social classes, including all births registered by both parents, whether married or not.
Methods
Tabulations of the numbers of live births, stillbirths, and early neonatal, late neonatal, and postneonatal deaths for each year from 1975 to 1996 were obtained from the Office for National Statistics for babies born inside marriage, babies born outside marriage but jointly registered by both parents, and babies born outside marriage registered solely by the mother.
Since 1975 registrations of infant deaths in England and Wales have been linked to birth records; a high linkage rate of over 98% has been achieved in each year.2 This linkage means that the more detailed information collected at birth on a range of sociodemographic factors can be used in the analyses of deaths.
For births inside marriage and those outside marriage jointly registered by both parents the Office for National Statistics assigns a social class to a 10% sample of records (about 58 000 records each year) on the basis of the occupation of the father stated on the birth record.7 Even births to fathers who were currently unemployed could be assigned a social class if the father gave details of his last main occupation. All the social class analyses are based on this 10% sample of coded records.
In each year only about 5% of the sample of records could not be coded to a social class in this way, and this proportion remained fairly constant over the 21 year period. Records relating to these births were placed in a residual category labelled “other,” consisting of live births whose fathers who were in the armed forces, full time students, unemployed with no previous occupation stated, permanently sick, and unoccupied and those who were employed but gave insufficient details about their current occupation to allow coding to a social class.
Data relating to births outside marriage registered solely by the mother were placed in a separate category, which we believe consists largely of the babies of lone mothers and is the best proxy available from the readily published national statistics (see box).
Sole registrations: are they the babies of lone mothers?
We assumed that the category containing births outside marriage registered solely by the mother consists largely of the babies of lone mothers on the basis of knowledge of registration procedures and data processing by the Office for National Statistics.
Registration of births is a legal requirement. A baby born to a married couple may be registered by either parent, with both the baby’s father and mother entered into the record. For births outside marriage, there are provisions for fathers who wish to register their child jointly with the mother, provided the mother is a party to the registration. Special arrangements can be made by the mother for joint registration outside marriage if the father is absent at the time of registration. These provisions are widely taken up: in 1995, 78% of births outside marriage were registered by both parents, and nearly three quarters of these births were registered by parents living at the same address, presumed to be cohabiting.8
For the quarter of joint registrations outside marriage in which the parents were living at different addresses a proportion probably relate to the babies of lone mothers, not cohabiting with a partner, but we have no way of differentiating these births. On the other hand, because the option of joint registration is widely available and used it is unlikely that the sole registration category contains more than a small proportion of couple parents who wished but failed to make a joint registration.
Mortality for various ages within infancy was calculated from 1975 to 1996 for the babies registered solely by the mother and for each social class (see box below). Data for births inside marriage were combined with those outside marriage jointly registered by both parents—the combination referred to here as “couple registrations” or “couple parents.” Data for social class I (registrar general’s system) were combined with class II and those for class IV with class V to increase the numbers in the analysis and thereby the robustness of the calculated rates. Three year moving averages were calculated for the same reason. Confidence intervals around the mortalities were calculated by the methods of Breslow and Day.9
Stages of infancy used in calculation of infant mortality
Perinatal: deaths under 7 days and stillbirths per 1000 total births (that is, including live births and stillbirths)
Neonatal: deaths under 28 days per 1000 live births
Postneonatal: deaths 28 days and over but under 1 year per 1000 live births
Infant: deaths under 1 year per 1000 live births
Results
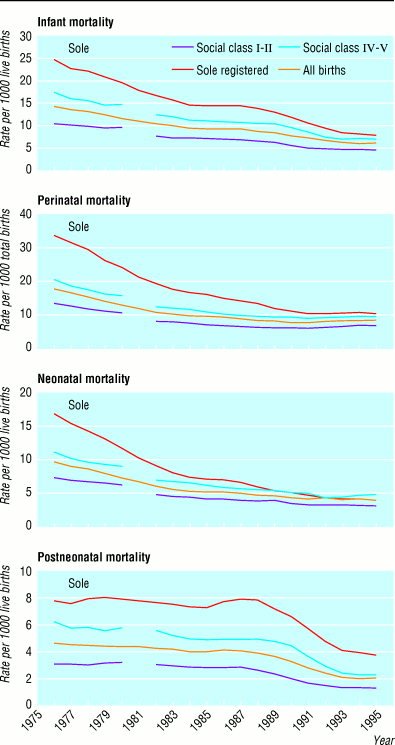
The figure shows that the trends varied for each stage of infancy and by social grouping. At the beginning of the period mortality was highest for the babies of lone mothers followed by a gradient from classes IV-V down to classes I-II with the lowest mortality. The most obvious changes occurred in relation to babies of lone mothers compared with those of couple parents. Infant mortality fell steadily for the sole registration category until 1984 and remained stable until 1989, when the decline resumed. During that time there was a distinct narrowing of the differential between the sole and couple registrations. In the mid-1970s infant mortality was 79% higher in the sole registrations compared with the couple registrations, and by 1996 this had reduced to a 33% excess (table 3). The confidence intervals show that the decreases in mortality over time in the various stages of infancy were all significant for both sole and couple registrations. It should be noted that there was a significant rise in perinatal mortality in couple registrations from 1989-91 to 1994-6.
Table 3.
Trends in infant mortality (95% confidence interval) for sole and couple registrations, England and Wales, 1975 to 1996
| Year | Sole registrations | Couple registrations | Excess mortality sole/couple (%) |
|---|---|---|---|
| Perinatal mortality/1000 total births | |||
| 1975-7 | 34.2 (33.0 to 35.5) | 17.2 (17.0 to 17.3) | 100 |
| 1982-4 | 17.8 (17.1 to 18.6) | 10.1 (9.9 to 10.2) | 77 |
| 1989-91 | 11.5 (11.0 to 12.0) | 7.8 (7.7 to 7.9) | 47 |
| 1994-6 | 10.6 (10.1 to 11.1) | 8.6 (8.4 to 8.7) | 24 |
| Neonatal mortality/1000 live births | |||
| 1975-7 | 17.1 (16.2 to 18.0) | 9.5 (9.3 to 9.6) | 81 |
| 1982-4 | 8.2 (7.6 to 8.7) | 5.7 (5.6 to 5.8) | 43 |
| 1989-91 | 5.3 (4.9 to 5.6) | 4.4 (4.3 to 4.5) | 19 |
| 1994-6 | 4.2 (3.8 to 4.5) | 4.1 (4.0 to 4.1) | 2 |
| Postneonatal mortality/1000 live births | |||
| 1975-7 | 7.6 (7.1 to 8.3) | 4.4 (4.3 to 4.5) | 74 |
| 1982-4 | 7.5 (7.0 to 8.0) | 3.9 (3.8 to 4.0) | 91 |
| 1989-91 | 6.6 (6.2 to 7.0) | 3.0 (2.9 to 3.0) | 123 |
| 1994-6 | 3.7 (3.4 to 4.0) | 1.8 (1.7 to 1.9) | 103 |
| Overall infant mortality/1000 live births | |||
| 1975-7 | 24.7 (23.7 to 25.9) | 13.9 (13.7 to 14.0) | 79 |
| 1982-4 | 15.7 (14.9 to 16.4) | 9.6 (9.5 to 9.7) | 63 |
| 1989-91 | 11.9 (11.3 to 12.4) | 7.4 (7.3 to 7.5) | 61 |
| 1994-6 | 7.8 (7.4 to 8.3) | 5.9 (5.8 to 6.0) | 33 |
Most of the narrowing resulted from greater improvements in mortality of solely registered births in the perinatal and neonatal periods from the mid-1970s and throughout the 1980s. By 1994-6 the difference between mortality in sole registered and couple registered babies in the neonatal period was no longer significant (table 3). This contrasted with the pattern of postneonatal mortality seen in the figure, for which there was little improvement in mortality for the couple registrations from 1975 to 1989 and a rise in mortality for sole registrations from 1985 to 1989. The postneonatal mortality differential between sole and couple registrations has been large and has shown no tendency to narrow; if anything it has widened over the 21 year period (table 3).
The figure also shows a different pattern for mortality in social classes I-II to IV-V. Although infant mortality declined in each social class, there has been a little narrowing of the differential between IV-V and I-II. In 1975-7 infant mortality was 64% higher in classes IV-V, since when it has fluctuated, but was still 52% higher in 1996 (table 4). What is striking, however, is the clear reduction in the differential to a negligible level between the infant mortality of the solely registered group and that of classes IV-V (tables 3 and 4).
Table 4.
Trends in infant mortality rates (95% confidence interval) for couple registrations by father’s social class, England and Wales, 1975 to 1996
| Year | Class I-II | Class IV-V | Excess mortality classes IV-V over I-II (%) |
|---|---|---|---|
| Perinatal mortality/1000 total births | |||
| 1975-7 | 13.8 (13.4 to 14.1) | 20.6 (20.1 to 21.0) | 50 |
| 1982-4 | 8.2 (8.0 to 8.5) | 12.4 (12.1 to 12.8) | 51 |
| 1989-91 | 6.5 (6.3 to 6.7) | 9.5 (9.2 to 9.8) | 47 |
| 1994-6 | 7.2 (7.0 to 7.4) | 10.2 (9.9 to 10.5) | 41 |
| Neonatal mortality/1000 live births | |||
| 1975-7 | 7.6 (7.4 to 7.9) | 11.3 (11.0 to 11.7) | 48 |
| 1982-4 | 4.7 (4.5 to 4.8) | 7.0 (6.7 to 7.3) | 50 |
| 1989-91 | 3.7 (3.6 to 3.9) | 5.2 (5.0 to 5.5) | 40 |
| 1994-6 | 3.4 (3.2 to 3.5) | 4.8 (4.6 to 5.0) | 42 |
| Postneonatal mortality/1000 live births | |||
| 1975-7 | 3.0 (2.8 to 3.2) | 6.1 (5.9 to 6.4) | 105 |
| 1982-4 | 2.9 (2.8 to 3.1) | 5.2 (5.0 to 5.4) | 78 |
| 1989-91 | 2.0 (1.9 to 2.1) | 4.3 (4.1 to 4.6) | 118 |
| 1994-6 | 1.3 (1.2 to 1.4) | 2.2 (2.1 to 2.4) | 78 |
| Overall infant mortality/1000 live births | |||
| 1975-7 | 10.6 (10.3 to 10.9) | 17.5 (17.0 to 17.9) | 64 |
| 1982-4 | 7.6 (7.3 to 7.8) | 12.2 (11.8 to 12.5) | 61 |
| 1989-91 | 5.7 (5.5 to 5.9) | 9.6 (9.3 to 9.9) | 67 |
| 1994-6 | 4.6 (4.4 to 4.8) | 7.0 (6.8 to 7.3) | 52 |
It can be seen in the figure that the differential between social classes is larger in the postneonatal period than in the perinatal period (an excess in classes IV-V over I-II of 78% and 41%, respectively, table 4).
Infant mortality in the “other” category (couple registrations unclassified by social class) followed a similar pattern, with the rate more than halving from 1975 to 1996, decreasing from 26 per 1000 to 10 per 1000. The rate for this category still remains higher than for any of the social classes or for the solely registered (data not shown).
Discussion
This analysis shows an improvement in mortality in babies registered solely by their mothers. In absolute terms, infant mortality for this group has declined to a third of its 1975 level. In addition, the mortality of babies in this group relative to other groups has fallen. Although infant mortality is still 33% higher than for couple registrations, the gap has reduced from an excess of 79%. Furthermore, there is now little difference between the death rates of solely registered babies and those of classes IV-V, in contrast with the findings of studies in the 1970s10 and the 1980s.11 It is noteworthy that much of this improvement for the solely registered babies up until 1990 was in relation to the perinatal and neonatal periods rather than for postneonatal mortality.
For each social class infant mortality has more than halved since 1975, but the gap between the top and bottom of the social scale has shown little narrowing. As with sole registrations the differential between classes IV-V and I-II is smallest in the neonatal and largest in the postneonatal period.
Limitations
We have not been able to identify all the babies of lone mothers. Although we are confident that the solely registered births are predominantly those to lone mothers, some babies of lone mothers may also be included in the joint registration category, and these cannot be identified separately from published sources. There is no reason to believe, however, that this form of misclassification has changed over the study period in a way which would affect the interpretation of trends. Secondly, the status of the baby at death may be different to that at birth—for example, if the lone mother has since married. This is unlikely to be an issue for most deaths that take place in the relatively short neonatal period (within 1 month of birth).
A narrowing gap
The findings of this study raise two major issues. First, they show a positive reduction in social inequalities in health because of a greater improvement in infant mortality in solely registered births compared with other groups. This is in clear contrast with the trends for adults. For instance, over the period from 1970 to 1993 in England and Wales there was a widening of social class inequalities in mortality for men and women of working ages and in life expectancy at birth, age 15, and age 65 between classes IV-V and I-II.12,13 Studies that compared rich and poor areas in the United Kingdom have also concluded that there was an increase in differentials in adult mortality during the 1980s14,15 and in life expectancy between affluent and deprived local authorities in England.16 The finding that there can be improvements, or at least a standstill, in the differential at the youngest ages may provide important new clues about tackling health inequalities. There is a need to look more closely at what the underlying determinants of the observed improvements are.
We tested the possibility that shifts in the demographic characteristics of lone mothers, such as their age distribution,17,18 could account for the improvement by plotting trends in age distribution of lone and couple mothers and carrying out the test for linearity (sole r=0.99, couple r=0.97).19 We then performed the test for difference between slopes of the linear regression lines (sole slope 0.18, couple slope 0.13; no significant difference at any level).19 Thus we concluded that there were similar shifts in the age distribution of the two groups, with the average age of motherhood increasing for both sole and couple mothers over the period but at the same rate.
The role of health care
Secondly, and linked to the first issue, the timing of the improvements—largely confined to the perinatal and neonatal stages of infancy—focuses attention on the part played by maternal and neonatal health care in reducing these specific differentials. Mortality in these early stages of infancy is especially sensitive to the quality of care given to the mother and baby.20 The predominant causes of death in the neonatal period are conditions related to immaturity, congenital anomalies, and asphyxia, anoxia, or trauma.21 The confidential inquiry into stillbirths and deaths in infancy (CESDI) found that the main contribution to the overall decline in neonatal mortality over the past 10 years has been a 50% reduction in deaths from congenital malformation. The inquiry concluded that this was probably related to improved prenatal diagnosis with a combination of preregistration abortion and improved survival after treatment.22 Our results raise the possibility that these improvements in diagnosis and treatment have been particularly beneficial for the babies of lone mothers or that their access to the relevant services has improved, or both.
Socioeconomic circumstances
Conversely, postneonatal mortality is thought to be influenced to a much greater extent by parents’ socioeconomic circumstances, reflected in the causes of death.23,24 The main causes of death in this period are the sudden infant death syndrome, congenital anomalies, infections, and injury and poisoning.21 For the population overall, trends from 1986 to 1995 in the postneonatal period show that deaths from congenital malformation have continued to decline and deaths from infection have nearly halved, but there has been little change in other specific conditions. Overall death rates from the sudden infant death syndrome remained stable until 1988, when they started to decline. Of the fall in the number of postneonatal deaths since 1988, 68% was because of the reduction in sudden infant death.21 The inquiry found that this is more common in babies of younger mothers and that the previously recognised association between sudden infant death and socioeconomic deprivation had become more obvious by the mid-1990s. In particular, there was a striking excess of sudden infant death in families in which neither partner was employed.25
Our findings of a lack of improvement in the differentials in postneonatal mortality between lone mothers and couple parents and between more and less disadvantaged social classes add to the concern that insufficient progress is being made with the groups at greatest risk. The lack of improvement is also in line with the trends we have found elsewhere4 in the material disadvantage of lone mothers and less skilled social classes, for many of whom conditions deteriorated during the 1980s and 1990s. The research highlights the need for lone and unsupported mothers to be given every possible assistance after the birth of their babies, not just in the neonatal period, but on a sustained basis.
Supplementary Material
Figure.

Infant mortality, England and Wales, 1975-96 (3 year moving averages). Registrar general’s social class I-II: professional, managerial, and technical occupations; IV-V: partly skilled and unskilled occupations; sole registered: babies whose birth is registered solely by the mother; all births: all births, regardless of type of registration. Data for social class for 1981 are not available because of industrial action by registrars in that year
Acknowledgments
We thank Jeremy Schuman, Office for National Statistics, for help in extracting the deaths data.
Editorial by Delamothe et al
Footnotes
Funding: None.
Competing interests: None declared.
References
- 1.Babb P, Bethune A. Trends in births outside marriage. Popul Trends. 1995;81:17–22. [PubMed] [Google Scholar]
- 2.Office for National Statistics. Mortality statistics: childhood, infant and perinatal, England and Wales, 1996. London: Stationery Office; 1998. (Series DH3 No 29.) [Google Scholar]
- 3.Bradshaw J. International comparisons of support for lone parents. In: Ford R, Millar J, editors. Private lives and public responses: lone motherhood and future policy in the UK. London: Policy Studies Institute; 1998. [Google Scholar]
- 4.Shouls S, Whitehead M, Burström B, Diderichsen F. Trends in the health and socio-economic circumstances of British lone mothers over the last two decades. Popul Trends. 1999;95:5–10. . (16 March.) [PubMed] [Google Scholar]
- 5.Roberts I, Pless B. Social policy as a cause of childhood accidents: the children of lone mothers. BMJ. 1995;311:925–928. doi: 10.1136/bmj.311.7010.925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wadsworth J, Burnell I, Taylor B, Butler N. Family type and accidents in preschool children. J Epidemiol Community Health. 1983;37:100–104. doi: 10.1136/jech.37.2.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Office of Population Censuses and Surveys. Standard occupational classification. Vol. 3. London: HMSO; 1991. [Google Scholar]
- 8.Office for National Statistics. Birth statistics 1995. London: Stationery Office; 1997. (FMI Series No 27.) [Google Scholar]
- 9.Breslow N, Day N. The standard mortality ratio. In: Sen P, editor. . Biostatistics: statistics in biomedical public health and environmental science. New York: Elsevier; 1985. [Google Scholar]
- 10.Macfarlane A, Mugford M. Birth counts: statistics of pregnancy and childbirth. London: HMSO; 1980. [Google Scholar]
- 11.Leon DA, Vågerö D, Olausson OP. Social class differences in infant mortality in Sweden: a comparison with England and Wales. BMJ. 1992;305:687–691. doi: 10.1136/bmj.305.6855.687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Drever F, Whitehead M, Roden M. Current patterns and trends in male mortality by social class (based on occupation) Popul Trends. 1996;86:163–168. [PubMed] [Google Scholar]
- 13.Hattersley L. Expectation of life by social class. In: Drever F, Whitehead M, editors. . Health inequalities—decennial supplement. London: Stationery Office; 1997. (DS Series No 15.) [Google Scholar]
- 14.Phillimore P, Beattie A, Townsend P. Widening inequality of health in northern England, 1981-91. BMJ. 1994;308:1125–1128. doi: 10.1136/bmj.308.6937.1125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McLoone P, Boddy A. Deprivation and mortality in Scotland, 1981-91. BMJ. 1994;309:1465–1470. doi: 10.1136/bmj.309.6967.1465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Raleigh V, Kiri V. Life expectancy in England: variations and trends by gender, health authority, and level of deprivation. J Epidemiol Community Health. 1997;51:649–658. doi: 10.1136/jech.51.6.649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Office of Population Censuses and Surveys. Birth statistics. Historical 1837-1983. London: HMSO; 1987. (FM1 Series No 13.) [Google Scholar]
- 18.Office for National Statistics. Birth statistics 1996. London: Stationery Office; 1998. (FM1 Series No 25.) [Google Scholar]
- 19.Howell D. Statistical methods for psychology. 2nd ed. Boston: Duxbury Press; 1982. [Google Scholar]
- 20.Spencer N. Poverty and child health. Oxford: Radcliffe Medical Press; 1996. [Google Scholar]
- 21.Schuman J. Childhood, infant and perinatal mortality, 1996. Social and biological factors in deaths of children under 3. Popul Trends. 1998;92:5–14. [PubMed] [Google Scholar]
- 22.4th Annual Report, 1 January-31 December 1995. London: Department of Health; 1997. Confidential Enquiry into Stillbirths and Deaths in Infancy (CESDI) [Google Scholar]
- 23.Pharoah POD, Macfarlane A. Studies in sudden infant deaths. London: HMSO; 1982. Recent trends in postneonatal mortality. (Studies in medical and population subjects No 45.) [Google Scholar]
- 24.Pharoah POD, Alberman E. Annual statistical review. Arch Dis Child. 1990;65:147–151. doi: 10.1136/adc.65.1.147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.3rd Annual Report 1 January-31 December 1994. London: Department of Health; 1996. Confidential Enquiry into Stillbirths and Deaths in Infancy (CESDI) [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
{kind=link}