

Abstract
Florida red tides are naturally occurring blooms of the marine dinoflagellate, Karenia brevis. K. brevis produces natural toxins called brevetoxins. Brevetoxins become part of the marine aerosol as the fragile, unarmored cells are broken up by wave action. Inhalation of the aerosolized toxin results in upper and lower airway irritation. Symptoms of brevetoxin inhalation include: eye, nose, and throat irritation, coughing, wheezing, chest tightness, and shortness of breath. Asthmatics appear to be more sensitive to the effects of inhaled brevetoxin. This study examined data from 97 asthmatics exposed at the beach for 1 hour during K. brevis blooms, and on separate occasions when no bloom was present. In conjunction with extensive environmental monitoring, participants were evaluated utilizing questionnaires and pulmonary function testing before and after a 1-hour beach walk. A modified Likert scale was incorporated into the questionnaire to create respiratory symptom intensity scores for each individual pre- and post-beach walk. Exposure to Florida red tide significantly increased the reported intensity of respiratory symptoms; no significant changes were seen during an unexposed period. This is the first study to examine the intensity of reported respiratory symptoms in asthmatics after a 1-hour exposure to Florida red tide.
Keywords: asthma, symptom score, brevetoxins, red tide, Harmful Algal Blooms (HABs), Karenia brevis
Introduction
Harmful algal blooms (HAB) occur annually along the west coast of Florida. In recent years, these blooms appear to be increasing in incidence, duration, and geographic spread, drawing greater attention from scientists and the general public (1). Karenia brevis, a marine dinoflagellate, is the organism responsible for Florida red tides (2). K. brevis produces a group of potent natural neurotoxins called brevetoxins which are tasteless, odorless, and very stable (3). The toxins are lipid-soluble, cyclic polyethers that are sodium channel activators (4–6).
Exposures to these toxins occur via ingestion of contaminated shellfish, or inhalation of affected marine aerosols (3). Although ingestion is associated with more severe effects because of larger doses, inhalation of aerosolized Florida red tide toxins is significantly more widespread. The toxic aerosol is created when the unarmored dinoflagellate is broken apart by wave action, releasing the toxins into the water column, and through bubble-mediated transport, subsequently incorporates the toxins into the airborne salt spray produced by the wind and waves (7). Air samples taken up to a mile inland have been found to contain brevetoxins (8).
Inhaling these aerosols leads to upper respiratory track discomfort and decreased forced expiratory volume in one second (FeV1), both of which are quickly reversible after leaving the beach and entering an air-conditioned area (3, 9). Asthmatics seem to be particularly susceptible to the respiratory effects of Florida red tide (10, 11). In addition, Abraham et al. (12, 13) have shown that K. brevis aerosols are potent airway constrictors in allergic sheep, and that asthma medication can reduce and prevent the respiratory effects of brevetoxins. Fleming et al. (11) and Backer et al. (14) discovered that healthy individuals showed no significant changes in their airflow after exposure to relatively low levels of aerosolized red tide toxins, while there were small but statistically significant changes in the airflow parameters of asthmatics after a 1-hour exposure; both healthy and asthmatic individuals reported significantly increased respiratory symptoms after exposure to aerosolized Florida red tide toxins.
The objective of this study was to examine the intensity of these self-reported symptoms in a cohort of 97 asthmatics. Previous studies (11, 14, 15) only examined the report of a respiratory symptom if the participant reported no symptoms prior to exposure to Florida red tide and then reported symptoms after exposure; furthermore, there was no utilization of symptom intensity information. In addition to examining reported degrees of intensity of respiratory symptoms, investigators also examined whether or not living close to the beach and whether pre-treatment with asthma medications affected a reported respiratory symptom intensity score with and without exposure to aerosolized brevetoxins.
Materials and Methods
Study Protocol
This study was approved by the Human Subjects Committees of the University of Miami (Miami, Florida) and the Florida Department of Health (Tallahassee, Florida).
Study Site and Dates
The study was conducted on the public beach access to Siesta Key Beach, Sarasota, Florida. Data were collected from 4 different 3-day events and one 4-day event (15).
Environmental Monitoring
Environmental monitoring protocols for these field studies have been reported in detail by Cheng et al. (16). Portable, solar powered, weather stations were used to measure temperature, humidity, and average wind speed and wind direction. Six high volume air samplers (TE-5000; Tisch Environmental, Inc.) were placed on the beach in the same area where study participants walked for 1 hour. Samplers collected aerosols for brevetoxin concentration in air, as well as for particle size. Filters from samplers were changed twice daily with each capturing a 4-hour period. Near shore water samples were collected 3 times per day in 1 L bottles, and evaluated for cell counts (number of K. brevis cells/L) and brevetoxin concentrations. Finally, every participant was outfitted with a personal air sampler during their 1-hour beach walk to determine an individualized aerosol dose. Brevetoxin analyses for all environmental monitoring were performed by High Performance Liquid Chromatography (HPLC) and by a brevetoxin Enzyme-Linked ImmunoSorbent Assay (ELISA) (17).
Participants
To be enrolled in the study, participants had to meet the following criteria: asthma diagnosed by a physician, 12 years of age or older, smoking for less then 10 years, able to walk continuously on the beach for 30 minutes, and a resident of Florida for at least 6 months of the year. A total of 97 asthmatics participated in at least one study period of exposure to Florida red tide and one non-exposure period. Information concerning asthma severity and proximity to the beach from the primary residency was collected at study enrollment, as well as before and after each beach walk.
Respiratory symptoms (i.e., eye and/or throat irritation; nasal congestion; cough; wheeze; chest tightness; and shortness of breath) and other symptoms designed to identify people who over-report symptoms (i.e., headache; itchy skin and/or diarrhea), as well as the use of asthma medications, were elicited before and after each 1-hour beach walk. If the participant reported any symptom, they were asked to describe it as “mild, moderate, or severe” and a respiratory symptom intensity score was devised. The respiratory symptom intensity score was the sum of intensities of each reported respiratory symptom, where mild = 1, moderate = 2, and severe = 3. A measure of asthma control was created using the data on medication use. Compared with participants who reported that they did not use asthma medications within 12 hours before doing study activities, participants who reported taking asthma medications within 12 hours of performing study activities were considered to have less-controlled asthma. The data were examined by exposure to brevetoxins (exposed or unexposed), by geographic area of residence (i.e., “coastal” ≤ 1 mile from the coast and “inland” > 1 mile from the coast), and by asthma control based on recent medication use.
Participants also underwent nasal swabbing (for inflammatory markers and brevetoxin concentration by ELISA), and spirometry (by individuals certified using the National Institute for Occupational Safety and Health approved training program) before and after beach walk. The results of these tests have been reported elsewhere (11, 14, 15).
Statistical Analysis
All questionnaire data were entered at the time of interview into a Microsoft Access database. Statistical analysis was performed for this study using SPSS statistical software. For each individual, their pre-beach walk value was compared to their post-beach walk value using a two-tailed paired t-test at the 0.05 level of significance.
Results
During the non-exposure study periods, the K. brevis cell counts in this area of the Gulf of Mexico were between <1000 and 6000 cells/L, and the concentrations of brevetoxins in the water ranged from <0.01 to 0.20 μm/L. The concentrations of brevetoxins in the aerosol did not exceed 0.2 ng/m3, but were often much lower. During exposure study periods, there were K. brevis cell counts between 14,000 and 200,000 cells/L in the water; the concentrations of brevetoxins in the water ranged from 0.50 to 29.20 μm/L; and, the concentrations of brevetoxins in the aerosol from 0.02 to 76.6 ng/m3 (with higher levels during direct onshore winds).
Ninety-seven asthmatics participated in at least one evaluation during an active K. brevis bloom (exposure period) and one evaluation during a non-exposure period. Their mean (± Standard Deviation) age was 38.2 ± 18.6 years (range 12.0–69.0 years). They were predominantly female (58%), and white non-Hispanics (97%). At the time of the baseline interview, participants had been diagnosed with asthma a mean of 21.8 ± 19.4 years prior to study enrollment. Forty-two participants (43%) reported regularly using asthma medications and 16 (16.5%) reported being hospitalized at least once for respiratory illness in the past year. Only 9 (9.3%) were current smokers, and 71 (73%) reported having experienced respiratory symptoms with exposure to Florida red tide blooms prior to participating in the study (15).
A summary of the respiratory symptom intensity score data analysis is displayed in Table 1. Inhalation of Florida red tide toxin aerosols during exposure events resulted in statistically significant increases in the respiratory symptom intensity scores (p = 0.001). The initial pre-beach walk mean symptom score value was 1.91, while the post-beach walk mean respiratory symptom intensity score value was 3.01. During non-exposure studies, there was non-significant decrease in respiratory symptom intensity score (p = 0.62), dropping from 1.98 before the beach walk to 1.84 after the beach walk. As seen in Figure 1, there was a significant difference between the exposure to brevetoxin and non-exposure mean respiratory intensity symptom scores post-beach walk (p = 0.003). Of note, non-respiratory symptoms (e.g., diarrhea) were not reported during either the exposed, nor the non-exposed, study periods (data not shown) (15).
Table 1.
Respiratory symptom intensity scores pre/post 1-hour beach walk.
| n | Pre-exposure ± standard deviation | Post-exposure ± standard deviation | Difference | p Value* | |
|---|---|---|---|---|---|
| All Participants | |||||
| Exposure | 97 | 1.91 ± 2.02 | 3.01 ± 3.02 | 1.10 | 0.001 |
| Non-Exposure | 97 | 1.98 ± 2.49 | 1.84 ± 2.29 | −0.14 | 0.62 |
| Between exposed and non-exposed | 0.003 | ||||
| Place of Residence | |||||
| Exposure coastal | 30 | 1.93 ± 1.87 | 3.77 ± 3.69 | 1.84 | 0.02 |
| Exposure inland | 67 | 1.90 ± 2.10 | 2.67 ± 2.63 | 0.77 | 0.02 |
| Non-exposure coastal | 30 | 1.67 ± 2.40 | 1.30 ± 1.90 | −0.37 | 0.55 |
| Non-exposure inland | 67 | 2.12 ± 2.53 | 2.07 ± 2.43 | −0.05 | 0.89 |
| Pre-treatmentmedication | |||||
| Exposure meds | 51 | 2.37 ± 2.15 | 3.04 ± 2.66 | 0.67 | 0.07 |
| Exposure no meds | 46 | 1.39 ± 1.74 | 2.98 ± 3.41 | 1.59 | 0.006 |
| Non-exposure meds | 51 | 2.45 ± 2.59 | 2.35 ± 2.70 | −0.10 | 0.81 |
| Non-exposure no meds | 46 | 1.46 ± 2.29 | 1.26 ± 1.57 | −0.20 | 0.64 |
two-tailed t-test.
Figure 1.
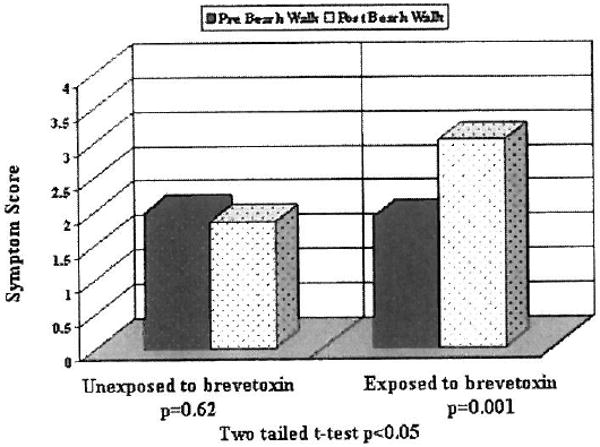
Respiratory symptom intensity score pre- and post-beach walk: All participants.
Figures 2 and 3 explored the possibility that where the study participant lived (i.e., “coastal” ≤ 1 mile from coast and “inland” > 1 mile from the coast) could affect the exposure and response of asthmatics to Florida red tide aerosols. Both subgroups arrived at the beach with similar respiratory symptom intensity scores during the exposure events as follows: 1.93 for the coastal group and 1.90 for the inland group. The mean respiratory symptom intensity score for people living near the coast increased 1.84 points to 3.77 (p = 0.02), and the mean respiratory symptom intensity score for people living inland increased 0.77 points to 2.67 (p = 0.02). During the non-exposure studies there were no significant changes in reported respiratory symptom intensity scores for either the coastal (1.67 pre, 1.3 post; p = 0.55) or for the inland (2.12 pre, 2.07 post; p = 0.89) study participants.
Figure 2.
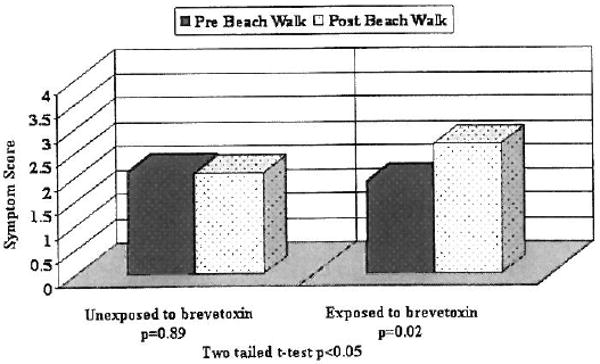
Respiratory symptom intensity score pre- and post-beach walk: Inland participants.
Figure 3.
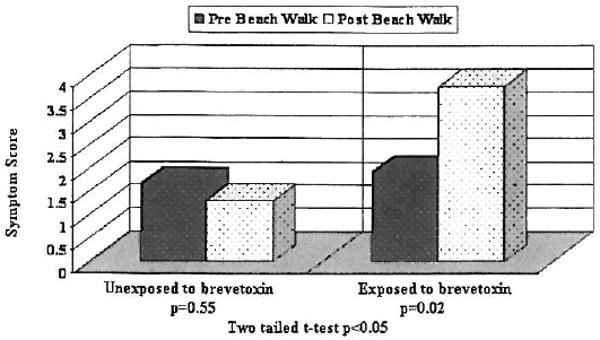
Respiratory symptom intensity score pre- and post-beach walk: Coastal participants.
The results for the medicated participants (i.e., people with less well-controlled asthma) vs. non-medicated asthmatics (i.e., people with well-controlled asthma) are shown in Figure 4. Respiratory symptom intensity scores of the participants who took medication within 12 hours prior to exposure to Florida red tide aerosols did not increase significantly (2.37 pre, 3.04 post; p = 0.07). However, non-medicated participants reported a significant increase in the mean respiratory symptom intensity scores from 1.39 to 2.98 (p = 0.006). For the periods when there were no Florida red tide, there were no significant changes in respiratory symptom intensity scores after the beach walk compared to before the beach walk for either the medicated or the non-medicated subgroups (Table 1).
Figure 4.
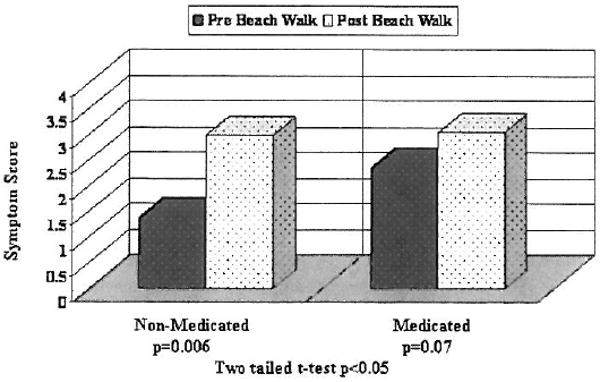
Respiratory symptom intensity score and medication use: During a Florida Red Tide exposure period.
Discussion
Abraham et al. (13) demonstrated that brevetoxins are potent airway constrictors in allergic sheep. Consistent with those observations, we have reported that asthmatics experience significant increases in the report of upper and lower airway symptoms during a Florida red tide event, and small but significant decreases in pulmonary function (11, 15). This study provided additional evidence that in asthmatics respiratory symptom intensity increased during a 1-hour exposure to Florida red tide, while respiratory symptom intensity did not change significantly after a 1-hour beach walk when unexposed to Florida red tide. This study also suggested that the location of residence does not necessarily predispose those who lived in either coastal or inland communities to be more vulnerable to the aerosolized brevetoxins, as both coastal and inland residents both reacted significantly; of note, similar objective pulmonary function changes were seen in both the inland and coastal subpopulations by Fleming et al. (15).
This study found that medicated asthmatics reported fewer changes in respiratory symptom intensity compared with non-medicated asthmatics when exposed to aerosolized brevetoxins. These results are consistent with the allergic sheep model (13), which demonstrated that pre-treatment with albuterol lessens the bronchoconstrictive effects of brevetoxin aerosols. Furthermore, it is possible that the participants whose asthma was apparently better controlled reported greater changes in symptoms possibly because they were not accustomed to being symptomatic, while the participants whose asthma was not well controlled had blunted symptom perception (18). Chen et al. (19) evaluated the perception of severity of reported symptoms among asthmatics. Their study concluded that appropriate perception is grounded in prior experience and learning. This implies that participants experiencing the same amount of respiratory discomfort could have potentially reported those symptoms differently depending on previous experiences. Since our study was based on self-reported symptom data, it is also possible that this finding may actually reflect differences in the perception of symptom severity, particularly since the participants with less controlled asthma appeared to have the greater objective decreases in pulmonary function (11, 15).
One possible limitation to our study was the use of self-reported symptoms. However, in addition to objectively-documented spirometry changes and the lack of over-reporting of the non-respiratory symptoms (11, 15), the respiratory symptoms accounted for nearly 75% of the change when all reported symptoms were evaluated (data not shown). Thus, these study results are unlikely to reflect over-reporting bias on the part of the subjects. One important strength of our study was the comparison of each individual to themselves, decreasing the possible effects of confounders such as smoking, obesity and work environment.
Conclusions and Future Directions
This study documented the intensifying of respiratory symptoms after only one hour of exposure to the Florida red tide aerosols in asthmatics. Kirkpatrick et al. (20) demonstrated increased emergency room admissions for pneumonia, bronchitis, asthma and upper airway disease (particularly for coastal residents) during years with active Florida red tides compared to non-exposure years. Given the recent apparent increase in incidence, duration and geographic spread of Florida red tide blooms (1), the health effects in asthmatics and other persons with underlying chronic lung disease from chronic occupational and/or environmental exposure, as well as exposures to high concentrations of aerosolized Florida red tides, need to be explored.
Acknowledgments
This study could not have been performed without the help of numerous volunteer investigators. In addition, the investigators thank Mote Marine Laboratory; the Siesta Beach administration; the Tropical Breeze and Holiday Inn hotels; and all of our study participants and their families in Sarasota, Florida.
This research was supported by the National Science Foundation under The Research Experience for Undergraduate Program, grant number 0453955 and the P01 ES 10594, DHHS NIH of the National Institute of Environmental Health Sciences, as well as by the Centers for Disease Control and Prevention and the Florida Department of Health (Cooperative Agreement: U50/CCU423360-02).
References
- 1.Van Dolah FM. Marine Algal Toxins: origins, health effects, and their increased occurrence. Environ Health Perspect. 2000;108(1):133–141. doi: 10.1289/ehp.00108s1133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.MacLean HL. Indo Pacific red tides. Toxic dinoflagellate blooms. Proceedings of the second International Conference on Toxic Dinoflagellate Blooms; Key Biscayne, FL. North Holland: Elsevier; 1979. pp. 173–178. [Google Scholar]
- 3.Kirkpatrick B, Fleming LE, Squicciarini D, Backer LC, Clark R, Abraham W, Benson J, Cheng YS, Johnson D, Pierce R, Zaias J, Bossart GD, Baden DG. Literature review of Florida red tide: Implications for human health effects. Harmful Algae. 2004;3(2):99–115. doi: 10.1016/j.hal.2003.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Baden DG. Brevetoxins: unique polyether dinoflagellate toxins. FASEB J. 1989;3:1807–1817. doi: 10.1096/fasebj.3.7.2565840. [DOI] [PubMed] [Google Scholar]
- 5.Baden DG. Marine food-borne dinoflagellate toxins. Int Rev Cytol. 1983;82:99–150. doi: 10.1016/s0074-7696(08)60824-4. [DOI] [PubMed] [Google Scholar]
- 6.Purkerson SL, Baden DG, Fieber LA. Brevetoxin modulates neuronal sodium channels in two cell lines derived from rat brain. Neurotoxicology. 1999;20(6):909–920. [PubMed] [Google Scholar]
- 7.Pierce R, Henry M, Boggess S, Rule A. Marine toxins in bubble generated aerosol. In: Monahan E, Van Patton P, editors. The climate and health implications of bubble-mediated Sea-Air exchange. Groton, CT: Connecticut Sea Grant Publications; 1989. pp. 27–42. CT SG 89-06. [Google Scholar]
- 8.Kirkpatrick B, Pierce R, Henry M, Blum P, Osborne S, Nierenberg K, Fleming LE, Cheng YS, Reich A, Baden DG, Backer LC. Inland Transport of Aerosolized Florida Red Tides. doi: 10.1016/j.hal.2009.09.003. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fleming LE, Backer LC, Baden DG. Overview of aerosolized Florida red tide toxins: exposures and effects. Environ Health Perspect. 2005;113(5):618–620. doi: 10.1289/ehp.7501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Asai S, Krzanowski JJ, Anderson WH. Effects of the toxin of red tide, Ptychodiscus brevis, on canine tracheal smooth muscle: a possible new asthma triggering mechanism. J Allergy Clin Immunol. 1982;69:418–428. doi: 10.1016/0091-6749(82)90116-6. [DOI] [PubMed] [Google Scholar]
- 11.Fleming LE, Kirkpatrick B, Backer LC, Bean JA, Wanner A, Dalpra D, Tamer R, Zaias J, Cheng YS, Pierce R, Naar J, Abraham W, Clark R, Zhou Y, Henry MS, Johnson D, Bogarl G, Bossart GD, Harrington M. Initial evaluation of the effects of aerosolized floridared tide toxins (brevetoxins) in persons with asthma. Environ Health Perspect. 2005;113(5):650–657. doi: 10.1289/ehp.7500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Abraham WM, Ahmed A, Bourdelais AJ, Baden DG. Effects of novel antagonists of polyether brevetoxin (PbTx)-induced bronchoconstriction in allergic sheep. In: Steidinger KA, Landsberg JH, Tomas CR, Vargo GA, editors. Harmful Algae 2002. Florida Fish and Wildlife Conservation Commission, Florida Institute of Oceanography, and Intergovernmental Oceanographic Commission of UNESCO. St. Petersburg, FL: Litho Services Inc; 2004. pp. 496–498. [Google Scholar]
- 13.Abraham WM, Bourdelais AJ, Ahmed A, Serebriakov I, Baden DG. Effects of Inhaled Brevetoxins in Allergic Airways: Toxin-Allergen Interactions and Pharmacologic Intervention. Environ Health Perspect. 2005;113(5):632–637. doi: 10.1289/ehp.7498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Backer LC, Kirkpatrick B, Fleming LE, Cheng YS, Pierce R, Bean JA, Clark R, Johnson D, Wanner A, Tamer R, Zhou Y, Baden D. Occupational exposure to aerosolized brevetoxins during Florida red tide events: Effects on a healthy worker population. Environ Health Perspect. 2005;113(5):644–649. doi: 10.1289/ehp.7502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fleming LE, Kirkpatrick B, Backer LC, Bean JA, Wanner A, Reich A, Dalpra D, Zaias J, Cheng YS, Pierce R, Naar J, Abraham WM, Baden DG. Aerosolized Red-Tide Toxins (Brevetoxins) and Asthma. Chest. 2007;131(1):187–194. doi: 10.1378/chest.06-1830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cheng YS, Zhou Y, Irvin M, Pierce R, Naar J, Backer LC, Fleming LE, Kirkpatrick BA, Baden DG. Characterization of Marine Aerosol for Assessment of Human Exposure to Brevetoxins. Environ Health Perspect. 2005;113(5):638–643. doi: 10.1289/ehp.7496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pierce RH, Henry MS, Blum PC, Lyons J, Cheng YS, Yazzle D, Zhou Y. Brevetoxin concentrations in marine aerosol: human exposure levels during a K. brevis harmful algal bloom. Bull Environ Contam Toxicol. 2003;70(1):161–165. doi: 10.1007/s00128-002-0170-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Martinez-Moragon E, Perpina M, Belloch A. Does experience influence perception of dyspnea? Arch Bronconeumol. 2006;42(4):171–174. doi: 10.1016/s1579-2129(06)60438-2. [DOI] [PubMed] [Google Scholar]
- 19.Chen E, Herman C, Rogers D, Oliver-Welker T, Strunk RC. Symptom perception in childhood asthma: the role of anxiety and asthma severity. Health Psychol. 2006;25(3):389–395. doi: 10.1037/0278-6133.25.3.389. [DOI] [PubMed] [Google Scholar]
- 20.Kirkpatrick B, Fleming LE, Backer LC, Bean JA, Tamer R, Kirkpatrick G, Kane T, Wanner A, Dalpra D, Reich A, Baden DG. Environmental exposures to Florida red tides: effects on emergency room diagnoses admissions. Harmful Algae. 2006;5:526–533. doi: 10.1016/j.hal.2005.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]