

Abstract
This case report describes removal of a knotted, subclavian, pulmonary artery catheter using a tracheostomy dilator. With this simple method an invasive procedure might be averted.
Keywords: knotting, pulmonary artery catheter, tracheostomy dilator
Introduction
Pulmonary artery catheterization is a well established technique in the management of the critically ill. This technique is not entirely without complications, however. Serious complications occur in only 3-4.4% [1,2], and include pneumothorax, haemothorax, pulmonary artery rupture, valve damage, dysrhythmias and rarely knotting of the catheter. In case of a knotted catheter, its subsequent withdrawal may lead to damage of the tricuspid valve, or rupture of the papillary muscle or vessel wall [3]. In the present case, a subclavian Swan Ganz (pulmonary artery) catheter, after formation of a knot, became firmly stuck between the clavicle and the second rib, and its subsequent method of removal is described.
Case report
A 69-year-old male with a history of silicosis was admitted to our hospital with a splenic abscess, for which computed tomography-guided percutaneous drainage was performed. Subsequently, he developed septic shock and respiratory failure, necessitating mechanical ventilation. A pulmonary artery catheter was uneventfully introduced via the right subclavian vein to manage fluid resuscitation and administration of inotropic agents. Initially, the patient recovered, and the Swan Ganz catheter was removed after 4 days. The abscess persisted, however, with ensuing haemodynamic instability. A splenectomy was performed, and postoperatively, in yet another uneventful procedure, a new pulmonary artery catheter (Criti Cath Thermodilution, 7F, SP 5107 H) was inserted through the left subclavian vein. Chest radiography showed a knot in the catheter at a distance of 16 cm from the tip, however (Fig 1).
Figure 1.
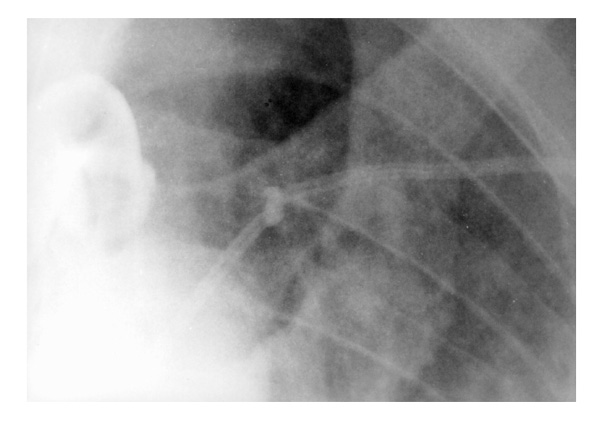
Chest radiography showing a knot in the pulmonary artery catheter at a position between the clavicle and the second rib.
An attempt was made to remove the catheter. On gentle pulling the knot appeared to be firmly stuck between the left clavicle and the second rib, even after careful manipulation of shoulder and arm. Attempts to untie the knot using a guidewire or to tighten the knot using traction at the introducer sheath were unsuccesful. We felt reluctant to pull out the catheter with sheath without reducing the size of the knot, because of the danger of laceration of the subclavian vein. After application of a local anaesthetic and thorough antiseptic treatment of the catheter, the distal end of the catheter was cut off and the flexible introducer sheath was removed. Then a 12 F tracheostomy dilator (Cook, Ciaglia percutaneous tracheostomy introducer set, C-PTS-100; William Cook Europe AIS, Bjaeverskov, Denmark) was inserted over the remaining part of the catheter whithout encountering any resistance. The catheter was carefully withdrawn until the knot reached the end of the dilator. There the knot was pulled tighter, but could not be retracted into the dilator. The knot had approximately the same circumference as the middle part of the dilator, however, and together they were removed without the occurrence of any further complications (Fig 2).
Figure 2.
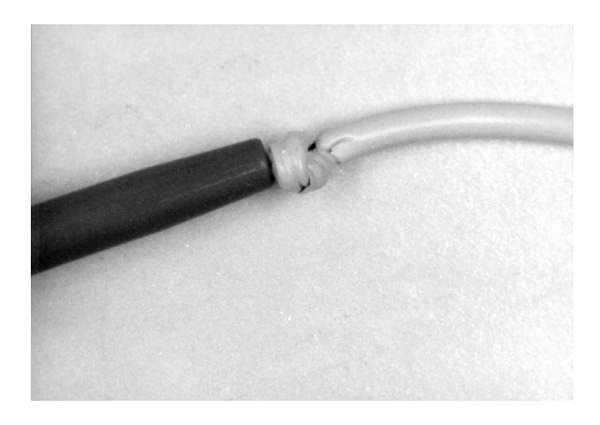
Tracheostomy dilator and pulmonary artery catheter after removal.
Haemoblobin levels remained stable, and chest radiography showed no signs of haemothorax. Unfortunately, the patient died 9 days later because of therapy-resistant sepsis.
Discussion
Knotting of a pulmonary artery catheter is a rare complication, to which several factors may contribute. Dilatation of the right ventricle; the insertion of a pulmonary artery catheter for more than 50 cm without achieving a pulmonary capillary wedge pressure curve; and the introduction of an incompletely inflated balloon all entail a high risk of coiling and subsequent knotting [3,4].
Various different methods for removal of knotted catheters have been reported. One approach is to pull the catheter against the introducer sheath, thereby reducing the size of the knot, followed by removing both catheter and sheath [5]. In catheters inserted via the subclavian route, a potential danger is venous laceration and subsequent haemothorax.
Another method is to attempt to unwire the knot. This may be achieved by inserting a guidewire in the pulmonary artery catheter itself [6], or through the femoral vein or antecubital vein and manipulate it to untie the knot [7]. Tan et al [8] achieved this by introducing a balloon catheter through the femoral vein, pushing it through the knot and inflating it, thereby unwiring it. Alternatively, a Dotter basket can be inserted through the femoral vein to snare the pulmonary artery catheter and remove it in two pieces [9]. Furthermore, surgical removal can be used, either by venous cut down or open surgery (ie thoracotomy).
In the present case attempts to unwire the knot were unsuccesfull. Because of the flexibility of the introducer sheath it was not possible to tighten the knot further without the risk of damaging the sheath and thereby inducing venous tearing. We therefore removed the introducer sheath and replaced it with a firm tracheostomy dilator with a diameter close to that of the knot. After that the knot could be tightened further and the catheter effortlessly removed. This procedure is similar to that used by Dach et al [10] with a biliary stent catheter. Although there still remains a chance of venous laceration and subsequent haemothorax, we believe this procedure reduces the risk of bleeding of the subclavian vein.
The preferred technique to remove a knotted Swan Ganz catheter is to untie the knot, but in some cases this can not be achieved. In those cases, removal of a tightened knot resting behind an unflexible sheath or tracheostomy dilator with a comparable diameter could be a simple, elegant and noninvasive solution.
References
- Colbert S, O'Hanlon DM, Quill DS, Keane P. Swan Ganz catheter-all in a knot. Eur J Anaesthesiology. 1997;14:518–520. doi: 10.1046/j.1365-2346.1997.00201.x. [DOI] [PubMed] [Google Scholar]
- Boyd KD, Thomas SJ, Gold J, Boyd AD. A prospective study of complications of pulmonary artery cathetrization in 500 consecutive patients. Chest. 1983;84:245–249. doi: 10.1378/chest.84.3.245. [DOI] [PubMed] [Google Scholar]
- Kranz A, Mundigler G, Bankier A, et al. Knotting of two central venous catheters: a rare complication of pulmonary artery catheterization. Wien Klin Wochenschr. 1996;18:404–406. [PubMed] [Google Scholar]
- Fibuch EE, Tuohy GF. Intracardiac knotting of a flow-directed balloon-tipped catheter. Anesth Analg. 1980;59:217–219. [PubMed] [Google Scholar]
- Castellá M, Riambau V, Palacin J, Font C, Mulet J. True knot in a Swan Ganz catheter on a central venous catheter: a simple trick for percutaneous removal. Intens Care Med. 1996;22:830–831. doi: 10.1007/BF01709529. [DOI] [PubMed] [Google Scholar]
- Böttiger BW, Schmidt H, Böhrer H, Martin E. Mistakes and dangers:non-surgical removal of a knotted Swan-Ganz-Catheter [in German]. . Anaesthesist. 1991;40:682–686. [PubMed] [Google Scholar]
- Agarwal NN, Giesswein P, Leverett L, Gracey J, Hess D. An unusual case of pulmonary artery catheter knotting during withdrawal. Crit Care Med. 1989;17:1081–1082. doi: 10.1097/00003246-198910000-00027. [DOI] [PubMed] [Google Scholar]
- Tan C, Bristow PJ, Segal P, Bell RJ. A technique to remove knotted pulmonary artery catheters. Anaesth Intens Care. 1997;25:160–162. doi: 10.1177/0310057X9702500211. [DOI] [PubMed] [Google Scholar]
- Bellamy CM, Ramsdale DR. Removal of a knotted Swan-Ganz balloon catheter using a Dotter basket. Postgrad Med J. 1988;64:475–476. doi: 10.1136/pgmj.64.752.475-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dach JL, Galbut DL, LePage JR. The knotted Swan-Ganz catheter: new solution to a vexing problem. Am J Roentgenol. 1981;137:1274–1275. doi: 10.2214/ajr.137.6.1274. [DOI] [PubMed] [Google Scholar]