

Abstract
Background and Purpose
Limited research suggests that an effect of whole body vibration (WBV) on the central nervous system (CNS) is suppression. An indirect measure used to assess CNS level of activation is the Soleus H-reflex. If true suppression does occur, other factors such as range of motion may be impacted. The purpose of this study was to examine the impact of WBV on H-reflex amplitude and passive ankle dorsiflexion.
Subjects and Methods
Twenty-seven healthy volunteers between the ages of 21-41 participated. Subjects were randomly assigned to a control group (n=13) or WBV group (n=14). H-reflex and ankle dorsiflexion measures were assessed before and after a three minute WBV perturbation (40 μHz, amplitude 2-4 mm). These measurements were repeated every five minutes up to twenty minutes following the intervention.
Results
The H-reflex amplitude showed a significant decrease (p<.05) between pre-test and initial post-test for both groups. The H-reflex returned to baseline within five minutes following the intervention. The dorsiflexion range of motion showed significant interaction (p<.05). All changes were less than 5 degrees; therefore, no clear clinical impact was evident.
Conclusions
The observed decrease in H-reflex amplitude immediately following WBV agreed with previous research indicating a lower level of CNS activation. However, since the control group also showed this change, WBV does not appear to be a key cause of suppression. Range of motion was not clinically significant for either group.
Keywords: Whole body vibration, H-reflex, Soleus muscle
INTRODUCTION
Enhancing athletic performance, at both the elite and recreational levels, requires the coordinated efforts of athletes, coaches, scientists, health care professionals, and exercise specialists. One of the primary trends in the sports industry today is analyzing the anatomical and physiological needs of athletes in their respective sports in order to locate possible methods or tools for sports performance improvement. Similarly, in a time where athletes are under great scrutiny, it is imperative to identify means to augment sport-specific skills without the use of ergogenic aids. One such aid that has recently been in the forefront of research is whole body vibration (WBV). Research regarding tools to enhance athletic performance is pertinent and crucial for not only for assessing athletes′ current physical capacities or locating deficits in performance, but also decisions whether to apply interventions in order to improve the athletes′ performance. Ultimately, athletes seek interventions that provide the most effective and efficient improvements that are achieved safely and noninvasively.
WBV is a neuromuscular training method that has sparked new research interest as an intervention useful for many populations in the field of physical therapy. In this form of training, the entire body is exposed to oscillating motions through the use of a vibrating platform upon which exercises can be performed.1 WBV has the potential to create short term gains in both flexibility and power that most athletes desire as described in a meta-analysis by Cardinale and Bosco as well as by Armstrong et al2,3 Research on the effects of WBV has been predominantly focused on muscle power and strength, body composition, electromyography, and balance and functional mobility in all age distributions.4 Results of current research indicate that WBV acts as a positive feedback mechanism serving to increase the contractile force of the muscle. Delecluse et al determined that a 12-week WBV protocol produced significant strength gains in the knee extensors in addition to increases in power.5 Results from a study by Bosco et al demonstrated that an increase in neural activity during vibration played an important role in muscle performance, specifically power, gains after WBV on an explosive power training regimen.6 An understanding of how WBV may affect performance is important in order to optimally apply this technique in clinical and athletic practices. To date, however,there is little research focusing on the effects of vibration on a single muscle group from a single exposure. Results of studies support that there is an increase in range of motion following exposure to WBV, but do not describe a hypothesis to explain how this occurs.1 The decrease in motor neuron pool excitability at the level of the spinal cord after using WBV is one possible hypothesis.3 A decrease in motor neuron pool excitability provides concurrent suppression of the central nervous system, which may allow for short-term gains in ROM.
Subsequently, there is an explicit demand for a method by which to objectify the effects of WBV. The Hoffman Reflex (H-reflex) is an important electrophysiological measure that enables better understanding of muscular activation patterns through assessment of spinal reflexes of key muscles. Specifically, it is a monosynaptic reflex that is elicited by stimulating a nerve and is analogous to a spinal stretch reflex. The H-reflex allows researchers to compare muscle activity of individuals using latency and amplitude measurements of the electrical activity associated with a muscle contraction. In adults, the “H-reflex is an estimate of alpha motor neuron excitability when presynaptic inhibition and intrinsic excitability of the alpha motor neurons remain constant. This measurement can be used to assess the response of the nervous system to various neurologic conditions, musculoskeletal injuries, application of therapeutic modalities, pain, exercise training and performance of motor tasks (p 268).”7 Armstrong et al used the H-reflex as a measure of motor neuron excitability in the soleus muscle.3 “It is a measure of the efficacy of synaptic transmission as the stimulus travels in the afferent (1a sensory) fibers through the motor-neuron pool of the corresponding muscle to the efferent (motor) fibers (p 268)”.7 To elicit the H-reflex in the soleus muscle, an electrical pulse is applied to the tibial nerve in the popliteal fossa. If the motor neuron excitability is decreased and the muscle remains relaxed, it is reasonable to assume that range of motion (ROM), both passive and active, could increase due to less resistance to stretch. Specifically, the inhibition of the tibial nerve excitability may allow an increase in the passive movement of dorsiflexion, which may influence motor control relative to gait patterns, functional activities and athletic performance.
Two proposed mechanisms exist that attempt to describe how WBV may cause muscle adaptation. Researchers have theorized that one such mechanism is a tonic vibration reflex, which may be the physiological response that is mediated by muscle through the utilization of interventions that use vibration.3,7,8,9 In addition, the tonic vibration reflex may cause repeated elongation of activated muscles which in turn elicits Ia afferent activity, leading to reflexive muscle contractions. Another suggested mechanism describes how an increased load applied to muscles during vibration facilitates a neuromuscular response. During the sinusoidal displacements provided by the WBV platform high accelerations, up to 15 g delivered at the equivalent of 147 m/s2 are generated.10 Ultimately, WBV seems to have a direct impact on both elicitation and consequent suppression of H-reflex activity, making the H-reflex a sound, objective method for exploration of the physiological effects of WBV.
While manual stretching is a typical method used to promote functional gains in muscle and tendon length, it requires consistent active effort from the individual or an outside source (i.e., a physical therapist). As noted in the stressstrain curve (Figure 1) there is a necessary and crucial threshold that must be attained and maintained in order to achieve permanent deformation and gains in extensibility of the musculotendinous unit.
Figure 1.

Stress-Strain Curve.
In order to achieve success in athletic performance, individuals may stretch muscle groups regularly, but perhaps there is a means by which functional gains in ranges of motion can be promoted and maintained by other interventions. Suppression of antagonistic muscle activity that would otherwise be inhibiting passive range of motion could be such an intervention. “The stretch reflex is a pathway with one central nervous synapse, relaying information about length changes to the alpha motoneuron. Within this pathway the Ia-afferent nerve fibers have a predominant effect on large motor units containing predominantly fast twitch muscle fibres. After demanding exercise the reflex amplitude is typically decreased (p 82).”11 It would seem that a stretch reflex, such as the H-reflex, may be inhibited by exercise, and therefore the effects of WBV would potentially suffice to fatigue muscle in the same fashion that other types of exercise otherwise would. Rittweger et al found in 2003, “…vibration frequency below 20Hz induces muscular relaxation whereas there are reports that at frequencies above 50 Hz severe muscle soreness and even hematoma may emerge in untrained subjects (p 82).”11 Additionally, mechanical vibration, administered to ten-dons or muscles, at frequencies between 10-200 Hz can cause a reflex response or contraction of the muscle belly.12
Armstrong et al suggested that whole body vibration may suppress the central nervous system which is observed as a decreased or inhibited H-reflex.3 The WBV induced inhibition of the monosynaptic reflex pathway of the plan-tarflexors may provide an increase in range of motion into dorsiflexion at the ankle joint. Armstrong et al studied the effects of WBV on 19 subjects implementing a one minute whole body vibration period followed by measurements of the H-reflex every 30 seconds up to 30 minutes following the intervention. All subjects “displayed a significant suppression of the H-reflex during the first minute post-WBV.”3 Jacobs and Burns demonstrated a significant increase in range of motion of knee extension between subjects who had utilized the WBV compared to those who had used a cycle ergometer.1 Therefore, it is possible that CNS suppression as reflected by H-reflex amplitude measured after WBV interventions coincides with concurrent gains in ROM. The purpose of this study was to examine the impact of WBV on H-reflex amplitude and passive ankle dorsiflexion range of motion.
Methodology
Approval was granted from Belmont University's Institutional Review Board for the study. Flyers were posted to attract a sample of convenience from the Belmont University School of Physical Therapy. To be included in the study a participant had to be a healthy individual over the age of twenty-one without any of the following: having participated in strenuous activity in the past four hours, recent (in the past 5 years) lower extremity or spinal surgery, presence of leg, ankle, or foot pathology, pregnancy, or any other disorders that could potentially affect sensation or musculoskeletal performance. Prior to data collection, the purpose and procedures of the study were explained to the subjects, and each subject signed aninformed consent form. Each subject then completed a medical history form, followed by a noninvasive lower quarter screen of leg strength, range of motion, and sensation to ensure each subject's eligibility to participate in the study. If the subject met the study eligibility criteria, the dominant leg of the subject was determined by kicking a gym ball. They were then randomly assigned to one of two groups, whole body vibration plate intervention or control.
Each participant was positioned prone over a pillow with the knee of the dominant leg slightly flexed over a pillow. The back of the knee and lower leg was cleaned with alcohol swabs. The tibial nerve was marked in the popliteal fossa indicating where the stimulating electrode was to be placed. A measurement was taken on the medial aspect of the leg from the marker in the popliteal fossa to the medial malleolus. This distance was divided in half, and a marker was placed at this location. The recording electrode was placed at this halfway marker with the reference electrode placed 2 cm distally. The ground electrode was placed on the lateral aspect of the calf. Two alligator clips were used to connect the two adhesive electrodes to the EMG unit. A gel medium was placed on the tip of the stimulating and dispersive electrodes. The stimulating bar electrode was placed on the marked location in the popliteal fossa with the dispersive electrode distal and the reference electrode proximal. The bar electrode was taped to the skin, the wrapped with a Nylatex band to create a constant pressure and prevent movement of the electrode (Figure 2). Normalization procedures as well as subject positioning is “crucial during H-Reflex testing because factors such as eye closure, head position, joint position and angle, and muscles length affect the H-reflex amplitude. (p 271)”7 Therefore, participants wore acoustic noise cancelling headphones to decrease perceived noise in the room that may otherwise stimulate or excited them, possibly affecting the elicited H-reflex amplitude and not allowing measurement of a true baseline H-reflex.7 To attain the pre-exercise values, all participants had his/her tibial H-reflex amplitudes measured using the Cadwell® Wave® EMG unit. The amplitude was increased to stimulate a supramaximal M wave. This created a baseline measurement for the participant. Once a supramaximal M wave was recorded, the amplitude was decreased to 30 percent of the amplitude used to obtain the appropriate H reflex wave. The H reflex was elicited at this amplitude 5 times consecutively, and recorded to be averaged for later data entry.
Figure 2.
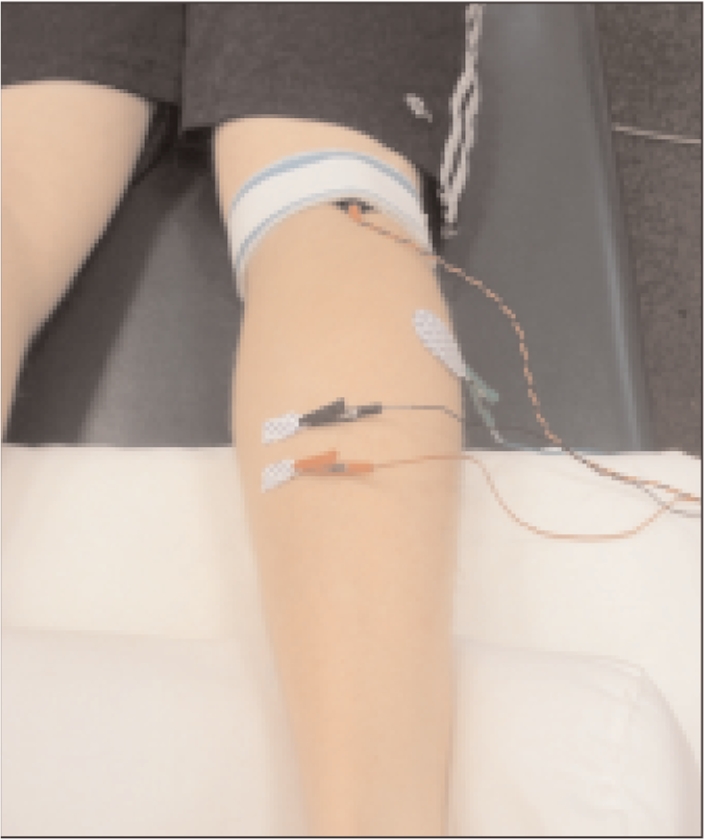
H-Reflex electrode placement.
The participant remained prone with the knee slightly flexed for measurement of passive dorsiflexion of the ankle. The foot on the dominant leg was off the edge of the plinth while 30 pounds of force was applied at the metatarsal heads through the Lafayette Instrument® Manual Muscle Test System digital hand dynamometer to determine a consistent, standardized force. A Baseline® Digital Absolute + Axis® Goniometer was used to measure ankle dorsiflexion simultaneously (Figure 3).
Figure 3.
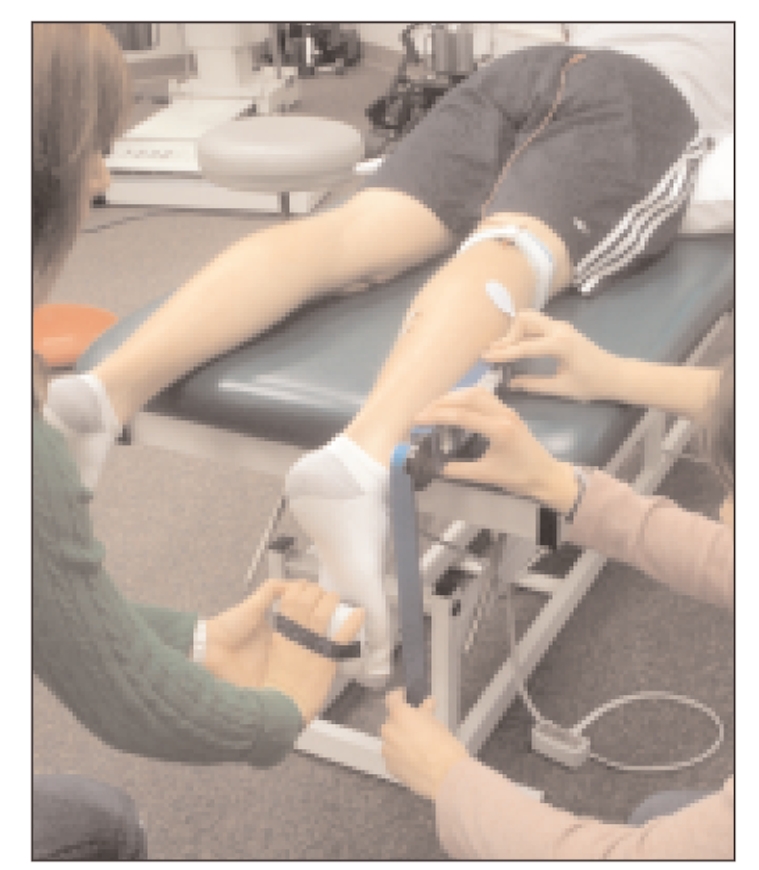
Testing position for ankle range of motion with standardized force application.
After the data was collected, the alligator clips were removed from the electrodes on the calf, allowing the participant to walk to the vibration platform. The participants of both groups stood on the Pneumex Vibration Plate® for the three minute intervention, in the standardized position of feet shoulder-width apart and knees slightly flexed, with the vibration plate turned on (intervention) or off (control). (Figure 4) The vibration plate was set to 40 μHz with amplitude of 2-4 mm as seen previously in the Armstrong et al research.3 All participants returned to the prone position on the table immediately following the WBV intervention or sham intervention in order to collect post-intervention H reflex and dorsiflexion PROM measures using the same methods as pre-intervention data collection. H reflex and dorsiflexion PROM measures were subsequently collected at 5, 10, 15, and 20 minutes post intervention.
Figure 4.

Standardized placement on the WBV device.
Results
The research study had thirteen control subjects and fourteen whole body vibration subjects. The average age of the control group was 23.92 years, and the average age of the WBV group was 25.93 years. The percentage of females in the control and WBV groups, respectively, were 76.92% and 64.29%. All subjects were right leg dominant except for one control group subject.
Data were analyzed using two mixed 2-way ANOVA's, utilizing SPSS version 16.0. A pre-determined alpha level of p<2 0.05 was utilized to determine if statistically significant differences existed between groups or conditions. One analysis compared the Hreflex amplitude over time of the between the control group and the vibration group. (Figure 5) There was no significant interaction between Hreflex amplitude and group (p=0.876). There was a significant difference in H-reflex amplitude over time (p= 0.001) for all subjects.
Figure 5.

Standardized placement on the WBV
A post hoc analysis using a paired t-test with a Bonferroni correction was necessary (p<2 0.0033). The post-test amplitude was significantly different (p< 0.0033) when compared to pretest and 5, 10, 15 and 20 minute intervals. After the decreased post-test amplitudes were collected, a trend became evident across all times with a return to similar pre-test values. (Figure 6)
Figure 6.

Paired T-tests comparing post-test H-reflex amplitudes across time
No significant differences in range of motion existed across the repeated trials (p=0.934) for all subjects. Additionally, no significant interaction (p= 0.077) between dorsiflexion range of motion and group was demonstrated. (Figure 7)
Figure 7.

Dorsiflexion ROM vs. time.
Discussion
This investigation has several key findings that need to be discussed. First, the post-test H-reflex values significantly decreased from pre-test values, in both groups. This finding suggests that WBV is not the primary reason for the decrease in H-reflex amplitude. The researchers theorize that there was something inherent to the protocol that created this suppression in the immediate post-test time. Plausible factors for the change in H reflex include anything that occurred during the time that the participant stood up from the table to the time that he/she took to return to the prone position. These factors include the transitions between prone and standing, ambulation to and from the vibration platform, removal of headphones upon standing, or prolonged static positioning used during the intervention or sham intervention. Despite the fact that the H reflex amplitude of both groups decreased in the posttest time, the results of the WBV group were consistent with similar studies such as Armstrong et al who demonstrated “all subjects displayed a significant suppression of the H-reflex during the first minute post-WBV.”3 Notably, this study employed a sample size and achieved power values consistent with previous studies of the same nature. Unique to the current study was the inclusion of a control group which provides additional information to the previous studies that did not have a control group. Therefore, it is not that the WBV group results are different from results of similar studies but the implications of the results vary due to the inclusion of a control group, which was previously unused.
Another point of interest is that H-reflex amplitudes are highly variable within the general population.7 H-reflex amplitudes have been documented to vary due to “variations in skin resistance, different amounts of subcutaneous fat and locations of the nerve relative to the stimulus” (p 271).7 Even with a wide range of variability of H-reflex amplitudes among subjects, the results of the current study are unable to demonstrate that WBV as an intervention is a significant source of CNS suppression and increase in ankle ROM. Other researchers such as Sands et al and Jacobs and Burns, have found range of motion gains in the hamstrings and low-back/hamstrings using WBV respectively.1,13 However these researchers used elite athletes who also performed ballistic stretching on the vibration plate. They also employed different vibration techniques to the muscle bellies. Sands et al “did not use the general WBV platform axial loading strategy; instead, they use an experimental apparatus to apply an oscillatory stimulus oblique to muscle fibers elongated without the mechanical loading associated with upright stance, thus without the respective level of muscle tension” (p 55).1 Therefore, it is inappropriate to directly compare the results of the current study to their findings as protocols and subjects were drastically different.
In order to look at the relevance of the findings of the current study, limitations need to be addressed. Notably, an initial dorsiflexion range to qualify or exclude the participants was not specified. Since most participants had PROM dorsiflexion values near 20 degrees, which is considered normal according to the AAOS and AMA, it is possible that there was limited room for improvement of ROM or a ceiling effect for range of motion.14 An anatomical bony block should have occurred between the talus and the distal tibia and fibula, which would have prevented additional gains in ROM. The ankle joint and its surrounding musculature may not be optimal to examine the effects of WBV on ROM because of its anatomical design. Research examining WBV effects on a joint or muscular region may be better studied in a joint or muscle with a greater ROM or with a different anatomical design (i.e. the knee and the hamstrings).
Conclusion
Since a decrease in H-reflex occurred in both the control and WBV groups, new hypotheses need to be generated to determine the cause of this change. Additional studies should use participants with limited dorsiflexion ROM in order to provide a greater window for possible range of motion improvement. In examining a population with limited range in dorsiflexion, the researchers should investigate trends in response to whole body vibration interventions as based on two factors: 1) the pathology or cause of the dorsiflexion limitation (e.g., do participants with limited dorsiflexion secondary to tight heel cords respond better to WBV interventions than do participants with limited dorsiflexion secondary to Cerebral Palsy), and 2) how long the source of limited dorsiflexion, be it pathology or other impairment, has been present in the participants.Although the WBV parameters used in the current study were gleaned from similar previous studies, no consistent parameters for this intervention were present in those previous investigations. A standard WBV protocol for intervention would allow for more consistency in studies regarding the efficacy and mechanism of action of this intervention. In conclusion, the current study does not support the hypothesis that WBV creates a suppression of the CNS, as measured by H reflex. Ankle PROM was not significantly affected by WBV. Further investigation is needed to identify the cause of the decreased H-reflex that occurred post WBV in both groups. Finally, additional research is needed to standardize a WBV intervention protocol.
REFERENCES
- 1.Jacobs PL, Burns P. Acute Enhancement of lower-extremity dynamic strength and flexibility with whole-body vibration. J Strength Cond Res. 2009; 231: 51–57 [DOI] [PubMed] [Google Scholar]
- 2.Cardinale M, Bosco C. The use of vibration as an exercise intervention. Exercise and Sport Sciences Review. 2003; 311: 3–7 [DOI] [PubMed] [Google Scholar]
- 3.Armstrong WJ, Nestle HN, Grinnell DC, Cole LD, Van Gilder EL, Warren GS, Capizzi EA. The acute effect of whole-body vibration on the Hoffmann reflex. J Strength Cond Res. 2008; 222: 471–476 [DOI] [PubMed] [Google Scholar]
- 4.Merriman H, Jackson K. The effects of whole-body vibration training in aging adults: A systemic review. Journal of Geriatric Physical Therapy. 2009; 32: 134–145 [DOI] [PubMed] [Google Scholar]
- 5.Delecluse C, Roelants M, Verschueren S. Strength increase after whole-body vibration compared with resistance training. Journal of the American College of Sports Medicine. 2003; 356: 1033–1041 Retrieved February 7, 2006, from http://gateway.ut.ovid.com.proxy.library.vanderbilt.edu/gw1/ovidweb.cgi Ovid [DOI] [PubMed] [Google Scholar]
- 6.Bosco C, Cardinale M, Tsarpela O. Influence of vibration on mechanical power and electromyogram activity in human arm flexor muscles. European Journal of Applied Physiology. 1999; 79: 306–311 [DOI] [PubMed] [Google Scholar]
- 7.Palmieri RM, Ingersoll CD, Hoffmann MA. The Hoffmann reflex: Methodologic considerations and applications for use in sports medicine and athletic training research. Journal of Athletic Training. 2004; 393: 268–277 [PMC free article] [PubMed] [Google Scholar]
- 8.Cormie P, Russell DS, Triplett NT, McBride JM. Acute effects of whole-body vibration on muscle activity, strength, and power. J Strength Cond Res. 2006; 202: 257–261 [DOI] [PubMed] [Google Scholar]
- 9.Issurin VB, Tenenbaum G. Acute and residual effects of vibratory stimulation on explosive strength in elite and amateur athletes. Journal of Sports Sciences. 1999; 17: 177–182 [DOI] [PubMed] [Google Scholar]
- 10.Savelburg H, Keizer HA, Meijer K. Whole-body vibration induced adaptation in knee extensors; Consequences of initial strength, vibration frequency, and joint angle. J Strength Cond Res.. 2007; 212: 589–593 [DOI] [PubMed] [Google Scholar]
- 11.Rittweger J, Mutschelknauss M, Felsenberg D. Acute changes in neuromuscular excitability after exhaustive whole body vibration exercise as compared to exhaustion by squatting exercise. Clinical Physiology and Functional Imaging. 2003; 232: 81–86 [DOI] [PubMed] [Google Scholar]
- 12.Hagbarth K, Eklund G. Motor effects of vibration stimuli. In Granit R. (ed) Muscular Afferents and Motor Control. Proceedings of the First Symposium. Almqvist and Wiksell; 1965 [Google Scholar]
- 13.Sands WA, McNeal JR, Stone MH, Russell EM, Monem J. Flexibility enhancement with vibration: Acute and long-term. Med Sci Sports Exerc. 2006; 38: 720–725 [DOI] [PubMed] [Google Scholar]
- 14.Norkin D. Joyce White Cynthia C. “Appendix A.” Measurement of Joint Motion: A Guide to Goniometry: 3rd edition. Philadelphia: F.A. Davis, 2003; 378 [Google Scholar]