

Abstract
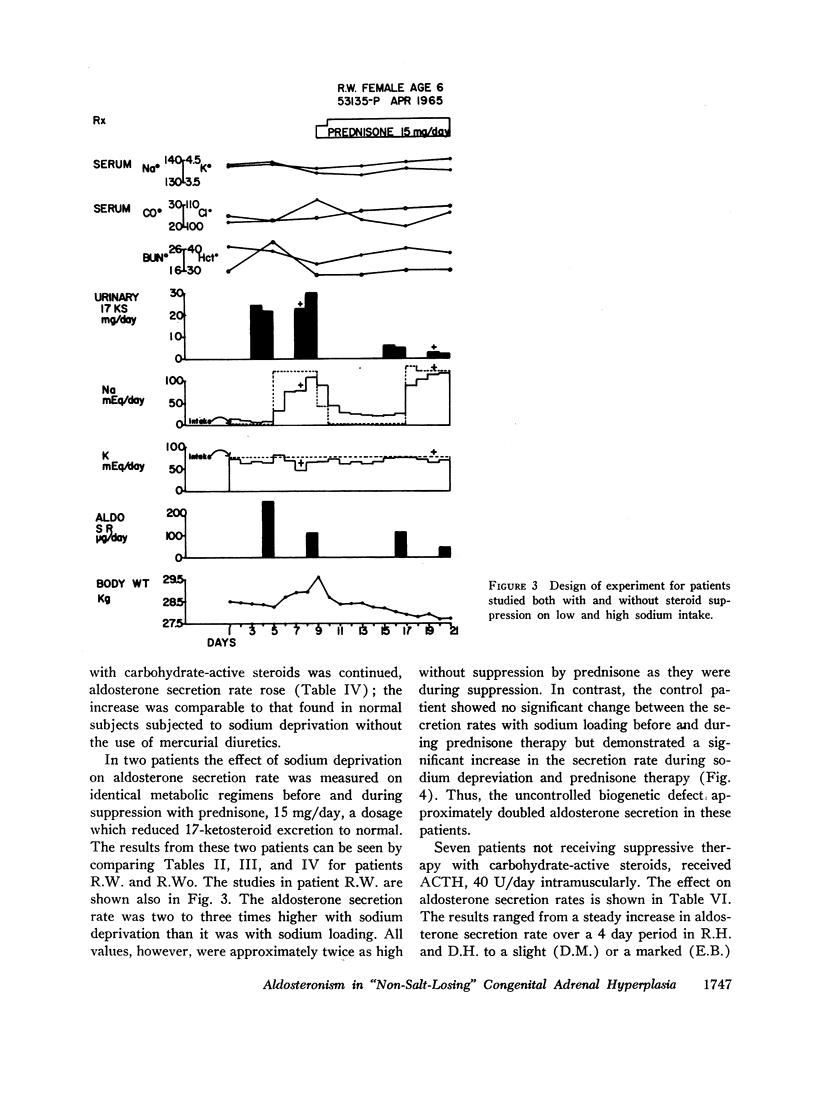
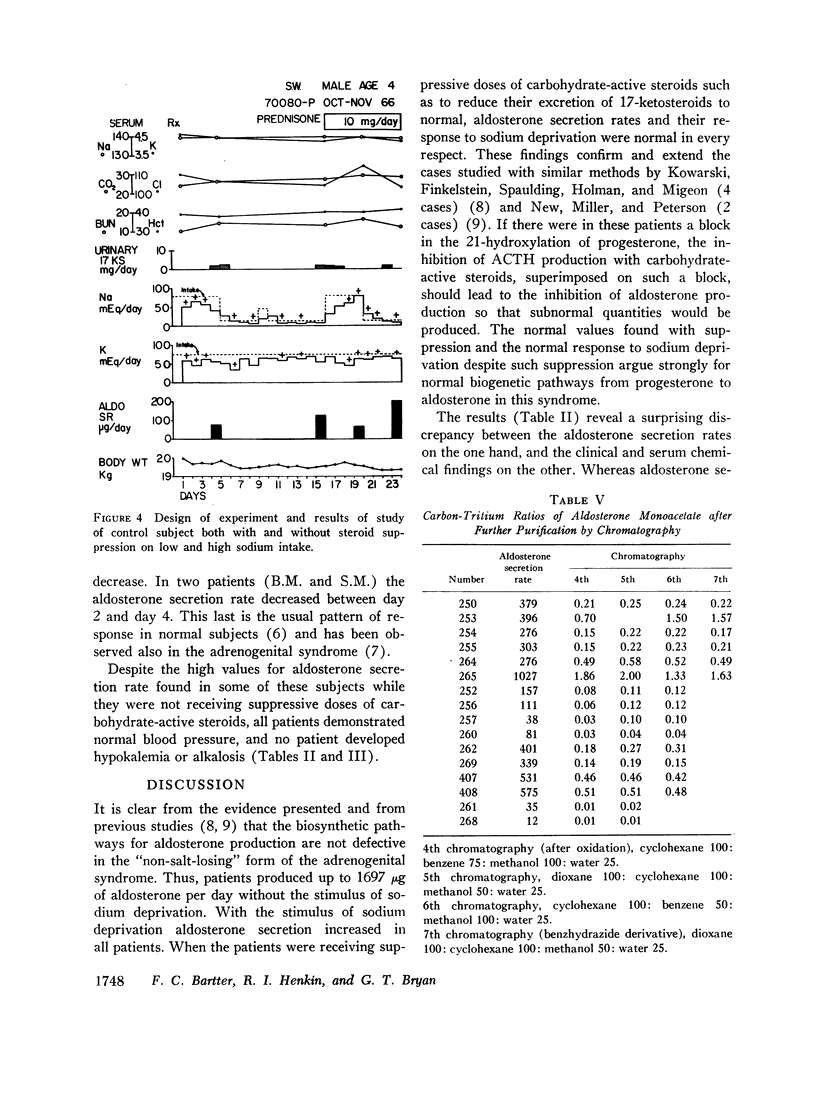
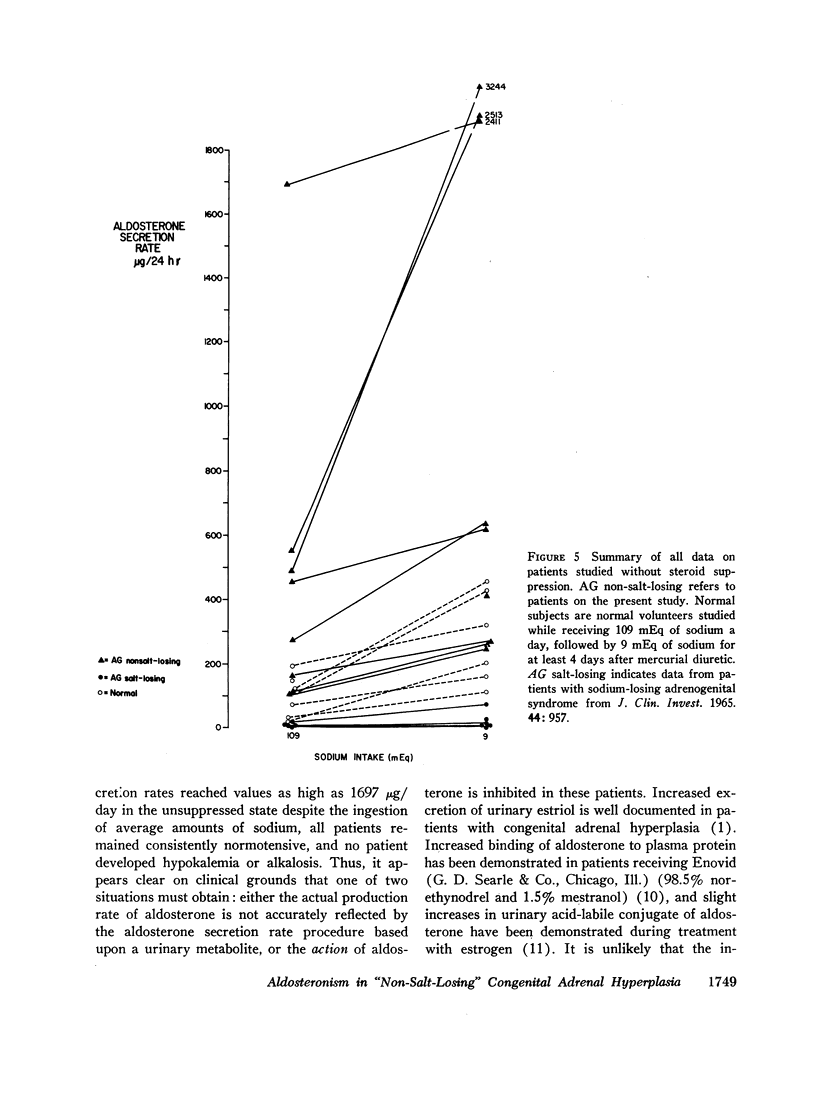
Patients with the “non-salt-losing” form of the adrenogenital syndrome were studied before and after suppression of adrenal cortical activity with carbohydrate-active steroids. The response of aldosterone secretion to sodium deprivation was measured; in some patients response to adrenocorticotropic hormone (ACTH) was measured as well.
The aldosterone secretion was normal and responded normally to sodium deprivation in all patients studied during suppression with carbohydrate-active steroids. This finding suggests that 21-hydroxylation of progesterone is normal in this syndrome.
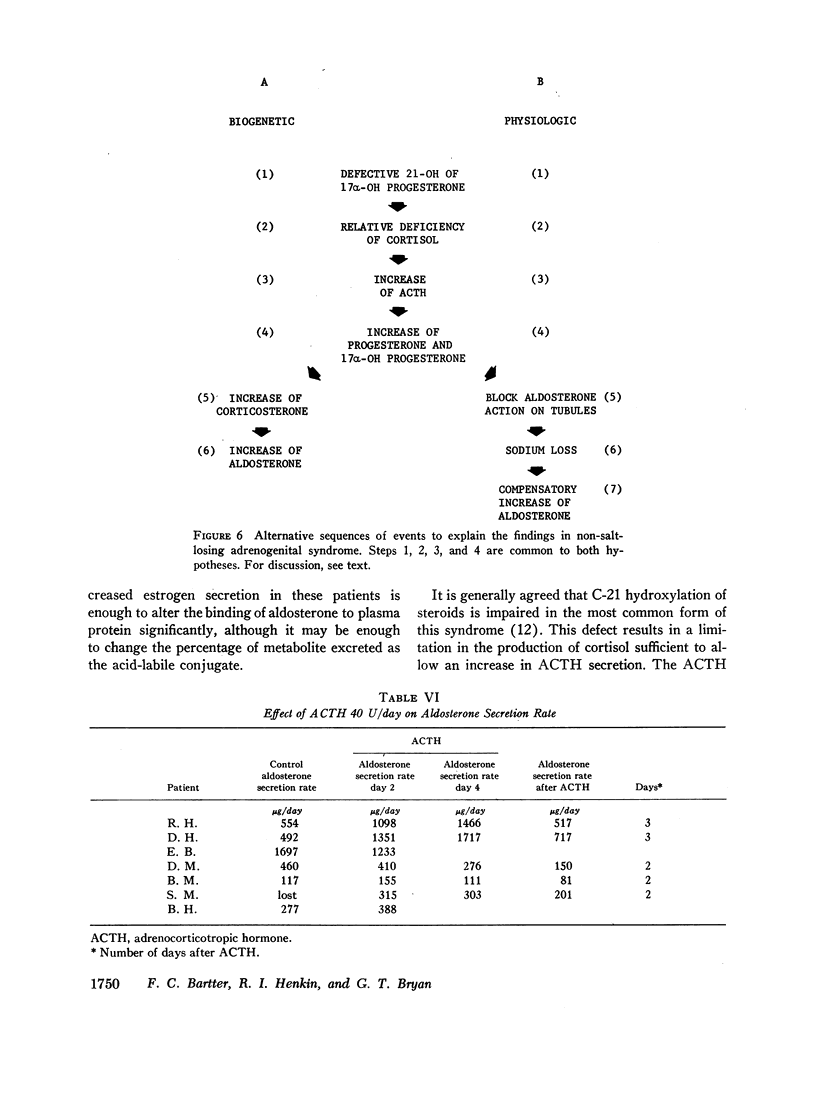
The sole abnormality in the production of aldosterone in these patients was found to be excessive secretion of aldosterone while they were not receiving suppressive doses of carbohydrate-active steroids. This finding strongly supports the view that the biogenetic pathways through which aldosterone is produced from progesterone are intact in this syndrome.
No patient showed hypertension or hypokalemic alkalosis despite very high aldosterone secretion rates. This observation suggests that the hyper-aldosteronism is secondary to a tendency to sodium loss in the patient whose ACTH production is not suppressed.
These studies provide additional evidence in support of the hypothesis that the salt-losing and “non-salt-losing” forms of adrenogenital syndrome are genetically and biochemically distinct.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BARTTER F. C., ALBRIGHT F., FORBES A. P., LEAF A., DEMPSEY E., CARROLL E. The effects of adrenocorticotropic hormone and cortisone in the adrenogenital syndrome associated with congenital adrenal hyperplasia: an attempt to explain and correct its disordered hormonal pattern. J Clin Invest. 1951 Mar;30(3):237–251. doi: 10.1172/JCI102438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BONGIOVANNI A. M. Adrenogenital syndrome: uncomplicated and hypertensive forms. Pediatrics. 1958 Apr;21(4):661–667. [PubMed] [Google Scholar]
- BONGIOVANNI A. M. In vitro hydroxylation of steroids by whole adrenal homogenates of beef, normal man, and patients with the adrenogenital syndrome. J Clin Invest. 1958 Oct;37(10):1342–1347. doi: 10.1172/JCI103723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BONGIOVANNI A. M., ROOT A. W. The adrenogenital syndrome. N Engl J Med. 1963 Jun 6;268:1283–contd. doi: 10.1056/NEJM196306062682308. [DOI] [PubMed] [Google Scholar]
- BRYAN G. T., KLIMAN B., BARTTER F. C. IMPAIRED ALDOSTERONE PRODUCTION IN "SALT-LOSING" CONGENITAL ADRENAL HYPERPLASIA. J Clin Invest. 1965 Jun;44:957–965. doi: 10.1172/JCI105213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CHILDS B., GRUMBACH M. M., VAN WYK J. J. Virilizing adrenal hyperplasia; a genetic and hormonal study. J Clin Invest. 1956 Feb;35(2):213–222. doi: 10.1172/JCI103266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DEGENHART H. J., VISSER H. K., WILMINK R., CROUGHS W. ALDOSTERONE- AND CORTISOL SECRETION RATES IN INFANTS AND CHILDREN WITH CONGENITAL ADRENAL HYPERPLASIA SUGGESTING DIFFERENT 21-HYDROXYLATION DEFECTS IN "SALT-LOSERS" AND "NON SALT-LOSERS". Acta Endocrinol (Copenh) 1965 Apr;48:587–601. doi: 10.1530/acta.0.0480587. [DOI] [PubMed] [Google Scholar]
- GEORGE J. M., SAUCIER G., BARTTER F. C. IS THERE A POTENT NATURALLY OCCURRING SODIUM-LOSING STEROID HORMONE? J Clin Endocrinol Metab. 1965 May;25:621–627. doi: 10.1210/jcem-25-5-621. [DOI] [PubMed] [Google Scholar]
- JACOBS D. R., VAN DER POLL J., GABRILOVE J. L., SOFFER L. J. 17alpha-Hydroxyprogesterone--a salt-losing steroid: relation to congenital adrenal hyperplasia. J Clin Endocrinol Metab. 1961 Aug;21:909–922. doi: 10.1210/jcem-21-8-909. [DOI] [PubMed] [Google Scholar]
- KENNY F. M., MALVAUX P., MIGEON C. J. Cortisol production rate in newborn babies, older infants, and children. Pediatrics. 1963 Mar;31:360–373. [PubMed] [Google Scholar]
- KOWARSKI A., FINKELSTEIN J. W., SPAULDING J. S., HOLMAN G. H., MIGEON C. J. ALDOSTERONE SECRETION RATE IN CONGENITAL ADRENAL HYPERPLASIA. A DISCUSSION OF THE THEORIES ON THE PATHOGENESIS OF THE SALT-LOSING FORM OF THE SYNDROME. J Clin Invest. 1965 Sep;44:1505–1513. doi: 10.1172/JCI105257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LAIDLAW J. C., RUSE J. L., GORNALL A. G. The influence of estrogen and progesterone on aldosterone excretion. J Clin Endocrinol Metab. 1962 Feb;22:161–171. doi: 10.1210/jcem-22-2-161. [DOI] [PubMed] [Google Scholar]
- LANDAU R. L., LUGIBIHL K. Inhibition of the sodium-retaining influence of aldosterone by progesterone. J Clin Endocrinol Metab. 1958 Nov;18(11):1237–1245. doi: 10.1210/jcem-18-11-1237. [DOI] [PubMed] [Google Scholar]
- MEYER C. J., LAYNE D. S., TAIT J. F., PINCUS G. The binding of aldosterone to plasma proteins in normal, pregnant, and steroid-treated women. J Clin Invest. 1961 Sep;40:1663–1671. doi: 10.1172/JCI104389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- New M. I., Miller B., Peterson R. E. Aldosterone excretion in normal children and in children with adrenal hyperplasia. J Clin Invest. 1966 Mar;45(3):412–428. doi: 10.1172/JCI105356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenbloom A. L., Smith D. W. Varying expression for salt losing in related patients with congenital adrenal hyperplasia. Pediatrics. 1966 Aug;38(2):215–219. [PubMed] [Google Scholar]