

Abstract
Background
In our efforts to develop novel effective treatment regimens for multiple myeloma we evaluated the potential benefits of combining the immunomodulatory drug lenalidomide with daratumumab. Daratumumab is a novel human CD38 monoclonal antibody which kills CD38+ multiple myeloma cells via antibody-dependent cell-mediated cytotoxicity, complement-dependent cytotoxicity and apoptosis.
Design and Methods
To explore the effect of lenalidomide combined with daratumumab, we first carried out standard antibody-dependent cell-mediated cytotoxicity and complement-dependent cytotoxicity assays in which the CD38+ multiple myeloma cell line UM-9 and primary multiple myeloma cells isolated from patients were used as target cells. We also tested the effect of lenalidomide on daratumumab-dependent cell-mediated-cytotoxicity and complement-dependent cytotoxicity of multiple myeloma cells directly in the bone marrow mononuclear cells of multiple myeloma patients. Finally, we determined the daratumumab-dependent cell-mediated cytotoxicity using peripheral blood mononuclear cells of multiple myeloma patients receiving lenalidomide treatment.
Results
Daratumumab-dependent cell-mediated cytotoxicity of purified primary multiple myeloma cells, as well as of the UM-9 cell line, was significantly augmented by lenalidomide pre-treatment of the effector cells derived from peripheral blood mononuclear cells from healthy individuals. More importantly, we demonstrated a clear synergy between lenalidomide and daratumumab-induced antibody-dependent cell-mediated cytotoxicity directly in the bone marrow mononuclear cells of multiple myeloma patients, indicating that lenalidomide can also potentiate the daratumumab-dependent lysis of myeloma cells by activating the autologous effector cells within the natural environment of malignant cells. Finally, daratumumab-dependent cell-mediated cytotoxicity was significantly up-regulated in peripheral blood mononuclear cells derived from 3 multiple myeloma patients during lenalidomide treatment.
Conclusions
Our results indicate that powerful and complementary effects may be achieved by combining lenalidomide and daratumumab in the clinical management of multiple myeloma.
Keywords: multiple myeloma, lenalidomide, daratumumab
Introduction
Over the past years, experimental and clinical studies have indicated that the use of chemotherapeutic agents with strong immune stimulatory properties can offer promising perspectives for multiple myeloma (MM) patients.1,2 Perhaps the best example of such an agent is lenalidomide (LEN),3–5 a structural analog of thalidomide with similar but more potent immunomodulatory activities.6–8 Since its approval by the FDA, lenalidomide has demonstrated impressive results in patients with newly-diagnosed and relapsed multiple myeloma9,10 and also improved graft versus multiple myeloma effects after allogeneic stem cell transplantation.11 In several initial studies, lenalidomide has been frequently used alone or in combination with other chemotherapeutical agents.12–15 Nonetheless, such strategies are possibly not exploiting the full immunomodulatory capacities of lenalidomide. In particular, its Natural Killer cell stimulatory properties suggest that lenalidomide could be highly effective in combination with therapeutic antibodies capable of inducing antibody-dependent cell-mediated cytotoxicity (ADCC).12–14 Supporting this idea, a number of earlier studies showed that both thalidomide and lenalidomide can enhance rituximab-mediated antibody-dependent cell-mediated cytotoxicity.15–17 Furthermore, multiple myeloma cell lysis was significantly improved when lenalidomide was combined with a humanized CD40 antibody.13,14 Indeed, promising results are being reported from a number of recently started clinical trials combining lenalidomide with rituximab or CD40 antibodies for the treatment of chronic lymphoid leukemia, lymphoma and multiple myeloma.16–18
A highly interesting target for antibody therapy in multiple myeloma is the CD38 molecule, a 46 kDa type II trans-membrane glycoprotein with a short N-terminal cytoplasmic tail (20 amino acids) and a long extracellular domain (256 amino acids).19,20 CD38 is expressed at low or moderate levels on various hematopoietic cells and in some solid tissues; but the extremely bright and uniform expression of CD38 on all multiple myeloma cells suggests that this molecule is an optimal therapeutic target for antibody therapy.21,22 Recently we have developed a new human CD38 antibody, daratumumab (DARA), and we have shown that it induces killing of tumor cells via anti-Fc-mediated effector functions, e.g. complement-dependent cytotoxicity, Natural Killer cell-mediated antibody-dependent cell-mediated cytotoxicity and apoptosis upon secondary cross-linking. Therefore, we now investigated the possibility that combining lenalidomide with daratumumab would significantly enhance the killing of multiple myeloma tumor cells. In a series of experiments using a CD38+ multiple myeloma cell line, purified multiple myeloma cells and full bone marrow mononuclear cells (BM-MNC) of multiple myeloma patients containing 2–50% malignant plasma cells, we demonstrate that lenalidomide significantly improves daratumumab-dependent lysis of multiple myeloma cells, mainly by activating the effector cells of antibody-dependent cell-mediated cytotoxicity. Furthermore, peripheral blood mononuclear cells (PBMC) isolated from patients during or just after lenalidomide treatment show an increased capacity of mediating daratumumab-dependent antibody-dependent cell-mediated cytotoxicity against multiple myeloma cells, emphasizing the potential clinical benefits that can be obtained by combination of daratumumab with lenalidomide in the clinical setting.
Design and Methods
Primary multiple myeloma cells and multiple myeloma cell lines
After obtaining written informed consent, primary CD138+ multiple myeloma cells were isolated from bone marrow of multiple myeloma patients using anti-CD138 (Becton Dickinson) coated rabbit-anti-mouse microbeads (Miltenyi Biotech, Bergisch Gladbach, Germany) according to the manufacturer’s protocol. Isolated primary multiple myeloma cells were immediately used in experiments after determining CD138 and CD38 expression. The CD38+ multiple myeloma cell line UM9 was generated and maintained as previously described.23,24
Peripheral blood mononuclear cells from healthy donors and multiple myeloma patients
All procedures involving material from healthy donors and multiple myeloma patients were approved by the institutional medical ethical committee. After obtaining written informed consent peripheral blood was obtained from healthy volunteers and from multiple myeloma patients. Peripheral blood mononuclear cells were isolated by Ficoll-Hypaque density-gradient centrifugation.11 Freshly isolated peripheral blood mononuclear cells from healthy individuals were used either immediately or after culturing with lenalidomide (Cellgene, 3μmol/L) for three days as effector cells in antibody-dependent cell-mediated cytotoxicity assays. Peripheral blood mononuclear cells from multiple myeloma patients were frozen prior to use as effector cells in antibody-dependent cell-mediated cytotoxicity assays.
Bone marrow mononuclear cells from multiple myeloma patients
All procedures involving bone marrow material were approved by the institutional medical ethical committee. Mononuclear cells from bone marrow were isolated by Ficoll-Hypaque density-gradient centrifugation11 and contained 2–50% malignant plasma cells. Freshly isolated bone marrow mononuclear cells from patients were treated immediately with lenalidomide (3μmol/L) and/or daratumumab (Genmab, 10 microg/ml) for 48 h and used in FACS-based bone marrow antibody-dependent cell-mediated cytotoxicity assays.
Immunophenotyping
Peripheral blood mononuclear cells, multiple myeloma cells and bone marrow mononuclear cells were labeled with the indicated fluorescein conjugated antibodies. The cells were washed and analyzed by flow cytometry using a FACScalibur device (Becton Dickinson). Data were analyzed using Cellquest Pro data acquisition software.
Antibody-dependent cell-mediated cytotoxicity against purified multiple myeloma cells
Antibody-dependent cell-mediated cytotoxicity was measured by standard 4 h chromium-51 (51Cr) release assays using 2,500 cells/well (51Cr labeled) and a 100-fold of effector cells in the presence or absence of antibodies (0.01–1 μg/mLl). Percentage specific lysis was calculated as follows: % specific lysis = (mean experimental release – mean spontaneous release)/(mean maximum release – mean spontaneous release) x100.
FACS-based antibody-dependent cell-mediated cytotoxicity against CD38+ cells in healthy peripheral blood mononuclear cells
Peripheral blood mononuclear cells were isolated by Ficoll-Hypaque density-gradient from blood from healthy volunteers and incubated with or without 10 μg/mL antibody and 3 μM lenalidomide. After 48 h, monocytes and Natural Killer cells were stained with CD14, CD16 FITC mAbs (BD), Topro and a CD38 PE antibody provided by Genmab, which recognizes a different epitope to daratumumab. Percentage of surviving cells was measured as described above. Daratumumab alone or daratumumab+lenalidomide treatment of healthy peripheral blood mononuclear cells did not significantly influence the survival of CD38+ monocytes or Natural Killer cells (Online Supplementary Figure S1).
FACS-based antibody-dependent cell-mediated cytotoxicity and complement-dependent cytotoxicity assays in bone marrow mononuclear cells
These assays were executed as described previously25 with slight modifications. Briefly, bone marrow mononuclear cells were isolated by Ficoll-Hypaque density-gradient from full bone marrow aspirates and incubated with or without 10 μg/mL antibody and 3 μM lenalidomide. After 24 – 48 h bone marrow mononuclear cells were stained with CD138 PE mAbs (BD) for antibody-dependent cell-mediated cytotoxicity. For complement-dependent cytotoxicity assays, bone marrow mononuclear cells were treated with lenalidomide for 24 h and 10 μg/mL antibody and complement were added 45 min prior to FACS measurements in which absolute numbers of cells were determined by using flow cytometric count beads as a constant. The percentage of multiple myeloma cell lysis was determined relative to controls with the following formula: % lysis cells = (1- (absolute number of surviving cells in treated wells/absolute number of surviving cells in control wells) x 100%. To determine the overall lysis percentages, the wells treated with control antibody were used as control values.
Statistics
Differences between treatment groups were tested for significance in repeated measure ANOVA, using Tukey’s post hoc multiple comparison tests and in paired Student’s tests with two-tailed 95% confidence intervals. P values below 0.05 were considered significant.
Where appropriate, we tested whether the effect of daratumumab and lenalidomide is proportional (the product of the effects of the individual treatments) or results in an extra effect. To this end, the ratios between cell counts with daratumumab relative to medium and the combination of lenalidomide+daratumumab relative to lenalidomide were calculated and the log-transformed ratios were fitted by a mixed model, with fixed effect lenalidomide (yes, no) and a random effect for patient sample.
Results
Lenalidomide significantly improves daratumumab-dependent antibody-dependent cell-mediated-cytotoxicity by activating effector cells
Since antibody-dependent cell-mediated cytotoxicity via Natural Killer cells is an important mechanism of action for daratumumab, and lenalidomide is known to increase the activity of Natural Killer cells, we first investigated the possible improvement of daratumumab-dependent antibody-dependent cell-mediated cytotoxicity by lenalidomide. Here, we first used standard 4-h antibody-dependent cell-mediated cytotoxicity assays, in which peripheral blood mononuclear cells from different healthy individuals (n=10), untreated or treated with lenalidomide for 72 h, were used as effector cells against the multiple myeloma cell line UM-9 (n=5) or against primary multiple myeloma cells (n=6) freshly isolated from patients’ bone marrow (Figure 1). Untreated peripheral blood mononuclear cells from 5 different healthy individuals mediated significant daratumumab-induced antibody-dependent cell-mediated cytotoxicity against UM9 cells (Figure 1A). A representative dose-response curve is shown in Figure 1B. Antibody-dependent cell-mediated cytotoxicity against UM-9 was significantly enhanced by pre-treatment of peripheral blood mononuclear cells with lenalidomide (P<0.001). Likewise, lenalidomide pre-treatment of peripheral blood mononuclear cells resulted in significant enhancement of antibody-dependent cell-mediated cytotoxicity against primary multiple myeloma cells (P<0.05) (Figure 1C), indicating that lenalidomide can improve the effects of daratumumab through activation of effector cells mediating antibody-dependent cell-mediated cytotoxicity which resided in the CD3 negative cell subset (Online Supplementary Figure S2).
Figure 1.

Enhancement of DARA induced ADCC by preincubation of effector PBMC with LEN. PBMC from healthy individuals were incubated with LEN (3 μM) for 72 h prior to ADCC assays in which UM9 (A, B) and purified MM cells (C) were used after addition of DARA (0.1 μg/mL) or a control antibody against KLH (1 μg/mL). A representative DARA dose-response curve is shown in (B). Error bars represent the SEM of triplicate measurements. P values are calculated by the Tukey’s post hoc analysis of a repeated measures ANOVA.
Next to its immunomodulatory properties, lenalidomide can directly induce apoptosis in multiple myeloma cells. Lenalidomide was also shown to sensitize multiple myeloma cells to CD40–induced cell death. We, therefore, also evaluated whether lenalidomide could sensitize multiple myeloma cells for daratumumab-induced antibody-dependent cell-mediated cytotoxicity. To test this, we treated primary multiple myeloma cells or the UM9 cells with lenalidomide for 24 h prior to antibody-dependent cell-mediated cytotoxicity assays in which peripheral blood mononuclear cells from healthy donors were used as effector cells. Pre-treatment of multiple myeloma cells did not change the expression of CD38. Also the expression of MHC class I and LFA-1, surface molecules that can influence Natural Killer cell mediated lysis, remained unchanged (data not shown). Pre-treatment of multiple myeloma cells with lenalidomide did not result in a significant improvement of antibody-dependent cell-mediated cytotoxicity (Figure 2) indicating that lenalidomide does not sensitize multiple myeloma cells for daratumumab-mediated antibody-dependent cell-mediated cytotoxicity.
Figure 2.
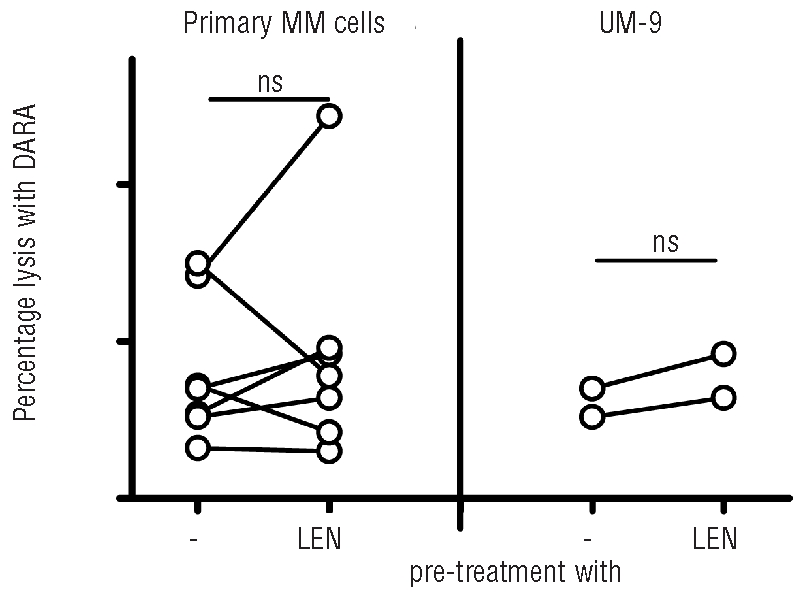
Absence of sensitization of MM cells by LEN for DARA-induced ADCC. Primary MM cells (N=7, left) or UM9 (n=2, right) where pre-treated for 24 h with LEN (3 mM). A standard ADCC was performed with DARA (0.1 mg/mL) and PBMC from healthy donors. Percentage lysis is calculated as indicated in the Design and Methods section. P values are calculated by a paired t-test.
Lenalidomide improves daratumumab-induced antibody-dependent cell-mediated cytotoxicity of multiple myeloma cells by whole bone marrow mononuclear cells
To evaluate the outcome of the combination therapy in a more physiological manner, we conducted a new series of antibody-dependent cell-mediated cytotoxicity assays without isolating multiple myeloma cells from their natural environment. Thus, bone marrow mononuclear cells of multiple myeloma patients containing stromal cells and 2–50% malignant plasma cells (n=14) were treated with lenalidomide, daratumumab or with the combination for 48 h. The survival of multiple myeloma cells in the bone marrow was then determined by enumeration of CD138+ cells by FACS staining. In these assays, 0–5% multiple myeloma cell lysis was observed in the presence of the control anti-KLH antibody. As illustrated in Figure 3A, lenalidomide alone induced poor to moderate levels of multiple myeloma cell lysis. In contrast, daratumumab induced substantial multiple myeloma cell lysis, which was significantly increased when it was combined with lenalidomide. Interestingly, a mixed model analysis revealed that lenalidomide and daratumumab acted in a synergistic fashion to generate 20% extra effect as compared to expected additive effects of the agents (Figure 3B).
Figure 3.

Improvement of DARA-induced ADCC by LEN in BM-MNC of MM patients. (A) BM-MNC of MM patients (n=14) were incubated for 48 h with LEN (3 μM) and DARA (0.1 μg/mL). Surviving MM cells were enumerated by FACS analysis of CD138+ cells. Percentage lysis of MM cells in LEN, DARA and LEN+ DARA treated patients were calculated using the MM survival in wells treated with the control anti-KLH antibody alone, which was indistinguishable from the medium control (thus 100% survival or no lysis). P values are calculated by the Tukey’s post hoc analysis of repeated measures ANOVA. (B) The observed effect (% lysis) of the combination treatment was compared to the expected proportional effect of the combined treatments. Mixed model analysis (see Design and Methods section) supports the conclusion that the combination treatment is synergistic.
Lenalidomide does not interfere with daratumumab-induced complement-dependent cytotoxicity
Daratumumab has documented strong complement-dependent cytotoxicity effects on primary multiple myeloma cells.26 Here, we determined the impact of lenalidomide on daratumumab-mediated complement-dependent cytotoxicity in our whole bone marrow mononuclear cell system. We treated freshly isolated bone marrow mononuclear cells of multiple myeloma patients (n=16) with lenalidomide for 24 h, added daratumumab in the last 45 min in the absence or presence of active complement (heat inactivated or inactivated human serum) and determined the lysis of multiple myeloma cells by FACS (Figure 4). Lenalidomide alone induced little or no lysis of multiple myeloma cells in the absence or in the presence of complement. Daratumumab mediated moderate lysis of multiple myeloma cells in the absence of complement, but as expected the lysis was significantly up-regulated by the addition of complement. The combination of lenalidomide and daratumumab did not further increase cell death via complement-dependent cytotoxicity as compared to cell death achieved with daratumumab alone (Figure 4).
Figure 4.

MM cell lysis in the BM of MM patients by the combination of DARA+LEN in the absence or presence of complement. BM-MNCs from MM patients (n=16) were subsequently incubated for 24 h with LEN and for 45 min with or without complement in the absence or presence of DARA. P values are calculated by the Tukey’s post hoc analysis of a one-way repeated measure ANOVA.
Peripheral blood mononuclear cells from lenalidomide treated patients show significant antibody-dependent cell-mediated cytotoxicity in the presence of daratumumab
Since lenalidomide appeared to improve the daratumumab-mediated effects primarily through activation of effector cells, we questioned whether the effector cells of multiple myeloma patients who received lenalidomide treatment would also show increased antibody-dependent cell-mediated cytotoxicity when treated with daratumumab ex vivo. To this end, we used peripheral blood mononuclear cells from multiple myeloma patients who were under treatment with lenalidomide as effector cells to mediate antibody-dependent cell-mediated cytotoxicity against UM-9 cells. The effector peripheral blood mononuclear cells were isolated from multiple myeloma patients before, during and one week after their first treatment cycle with lenalidomide and were stored in liquid N2 until use. As shown in Figure 5, peripheral blood mononuclear cells isolated from patients during or just after lenalidomide treatment showed a significantly increased capacity to mediate daratumumab-dependent antibody-dependent cell-mediated cytotoxicity against UM-9 cells. Thus, also in this ex vivo clinical setting, we show that the daratumumab-mediated killing of multiple myeloma tumor cells is significantly augmented by stimulating effector cells.
Figure 5.

Significant DARA-dependent ADCC in PBMC from patients treated with LEN. Frozen PBMC obtained from 3 patients (Pt 1–3) 0–7 days before (Pre), during (During) or one month after (Post) the first cycle of LEN treatment (25mg/daily) was tested in ADCC assays after addition of DARA and control antibody KLH. Control antibody against KLH did not induce any ADCC (data not shown) Error bars represent the SEM of the duplicate conditions. P values are calculated using a Student’s t-test.
Discussion
The survival of multiple myeloma patients has improved over the last decade as a result of the introduction of novel immunomodulatory agents such as lenalidomide and bortezomib with remarkable efficacy in relapsed and refractory myeloma.27 Nonetheless, multiple myeloma still remains an incurable disease and almost all patients will eventually relapse. In an attempt to develop an effective therapy for multiple myeloma, we evaluated the potential benefits of combining lenalidomide with a novel human antibody daratumumab, which targets the CD38 molecule which is highly expressed on multiple myeloma cells. In a series of experiments using purified multiple myeloma cells, multiple myeloma cell lines, full bone marrow mononuclear cell suspensions derived from multiple myeloma patients and peripheral blood mononuclear cells isolated from lenalidomide-treated patients, we show that the combination of lenalidomide and daratumumab significantly increases the lysis of multiple myeloma cells as compared to either of the single agents.
Obviously, the increased lysis of multiple myeloma cells by the combination of lenalidomide and daratumumab is to a certain extent due to the separate actions of these agents. For instance, daratumumab is known to induce its effects against multiple myeloma predominantly via complement-dependent cytotoxicity and antibody-dependent cell-mediated cytotoxicity, while lenalidomide induces multiple myeloma cell apoptosis via a mechanism involving increase in p21WAF-1 expression and cell arrest in the G0-G1 phase.28–30 Obviously, targeting multiple myeloma cells via various mechanisms is a primary goal of combination strategies to diminish the chance of developing resistance. A combination therapy becomes, however, more powerful if the agents work synergistically to improve each others’ actions. From this point of view, the lenalidomide-daratumumab combination appears to be a highly interesting choice since our results demonstrate that lenalidomide significantly synergises with daratumumab to improve the multiple myeloma cell lysis. Our assays demonstrate that the most important mechanism of this synergism is the ability of lenalidomide to activate the effector cells of antibody-dependent cell-mediated cytotoxicity, since lenalidomide appeared not to interfere with complement-dependent cytotoxicity and improved antibody-dependent cell-mediated cytotoxicity, predominantly after pre-incubation of peripheral blood mononuclear cells but not of multiple myeloma cells.
While our standard antibody-dependent cell-mediated cytotoxicity and complement-dependent cytotoxicity assays using purified multiple myeloma cells or multiple myeloma cell lines were suitable and sufficient to reveal the basic lytic mechanisms of the lenalidomide and daratumumab combination, in this study we also aimed to assess the influence of the micro environment on such therapy. This is of particular interest because the interaction of multiple myeloma cells with bone marrow stromal cells is crucial for their survival31–32 and may even induce a certain level of resistance against immune mediated lysis mechanisms. Therefore, in this study we used a new assay to measure antibody-dependent cell-mediated cytotoxicity and complement-dependent cytotoxicity assays without isolating multiple myeloma cells from their natural environment. Thus we incubated lenalidomide and daratumumab directly with mononuclear cells isolated from full bone marrow, which contains not only multiple myeloma cells but also stromal cells. Setting up the assays in this way provided not only a more physiological platform but also allowed us to measure antibody-dependent cell-mediated cytotoxicity without being forced to determine the effector to target cell ratios arbitrarily. Also the results of these assays clearly demonstrated a synergistic improvement of daratumumab mediated antibody-dependent cell-mediated cytotoxicity by lenalidomide, thus strongly substantiating the idea that significant anti-multiple myeloma effects can be expected from the daratumumab-lenalidomide combination even in the presence of stromal cells that support multiple myeloma cell growth. Interestingly, in these full bone marrow assays we observed 20% extra effect of lenalidomide-daratumumab combination above the expected additive effects of separate agents, which could translate into a substantial improvement in the clinical setting.
We argue that a final and strong indication for the clinical relevance of the daratumumab-lenalidomide combination therapy is the significant induction/augmentation of daratumumab-dependent antibody-dependent cell-mediated cytotoxicity in peripheral blood mononuclear cells isolated from 3 multiple myeloma patients during or just after oral treatment with lenalidomide. The results obtained from these patients are remarkable and strongly suggest that oral administration of lenalidomide also stimulates the effector cells of multiple myeloma patients to enhance daratumumab-dependent lysis of multiple myeloma cells. Taken together, our results demonstrate the potential benefits of combining lenalidomide with the novel CD38 antibody daratumumab in the treatment of multiple myeloma.
There are currently a growing number of studies addressing the efficacy of therapies based on the combination of lenalidomide with antibodies that can successfully target tumor cells. While in several CD20+ B-cell malignancies, such as lymphoma or chronic lymphocytic leukemia, the rutiximab-lenalidomide combination is tested, in the multiple myeloma setting promising antibodies are considered to target CD40, CS-1 and FGFR3, surface molecules highly expressed on multiple myeloma cells. Our results now indicate that daratumumab, which effectively targets CD38 and is capable of inducing antibody-dependent cell-mediated cytotoxicity as well as complement-dependent cytotoxicity, is a highly interesting additional candidate to combine with lenalidomide to exploit its full immunomodulating power. We believe that our results merit further evaluation of the lenalidomide-daratumumab combination in clinical trials, and a phase I/II clinical trial based on a dose-escalation principle will be the choice of strategy to evaluate the feasibility, safety and efficacy of this novel approach in the management of multiple myeloma.
Acknowledgments
The authors would like to thank UMC Utrecht and Genmab bioscience for providing researching funding.
Footnotes
Funding: this work was supported by research grants from UMC Utrecht and Genmab B.V provided to TM and HL.
The online version of this article has a supplementary Appendix.
Authorship and Disclosures
The information provided by the authors about contributions from persons listed as authors and in acknowledgments is available with the full text of this paper at www.haematologica.org.
Financial and other disclosures provided by the authors using the ICMJE (www.icmje.org) Uniform Format for Disclosure of Competing Interests are also available at www.haematologica.org.
References
- 1.Andersen MH, Sorensen RB, Schrama D, Svane IM, Becker JC, Rhor SP. Cancer treatment: the combination of vaccination with other therapies. Cancer Immunol Immunother. 2008;57(11):1735–43. doi: 10.1007/s00262-008-0480-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dougan M, Dranoff G. Immune therapy for cancer. Annu Rev Immunol. 2009;27:83–117. doi: 10.1146/annurev.immunol.021908.132544. [DOI] [PubMed] [Google Scholar]
- 3.Bartlett JB, Tozer A, Stirling D, Zeldis JB. Recent clinical studies of the immunomodulatory drug (IMiD) lenalidomide. Br J Cancer. 2005;93(6):613–9. doi: 10.1038/sj.bjc.6602774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kale V, List AF. Immunomodulatory drugs (IMiDs): a new treatment option for myelodysplastic syndromes. Curr Pharm Biotechnol. 2006;7(5):339–42. doi: 10.2174/138920106778521587. [DOI] [PubMed] [Google Scholar]
- 5.Knight R. IMiDs: a novel class of immunomodulators. Semin Oncol. 2005;32 (4 Suppl 5):S24–S30. doi: 10.1053/j.seminoncol.2005.06.018. [DOI] [PubMed] [Google Scholar]
- 6.Anderson KC. The role of immunomodulatory drugs in multiple myeloma. Semin Hematol. 2003;40(4 Suppl 4):23–32. doi: 10.1053/j.seminhematol.2003.09.010. [DOI] [PubMed] [Google Scholar]
- 7.Galustian C, Labarthe MC, Bartlett JB, Dalgleish AG. Thalidomide-derived immunomodulatory drugs as therapeutic agents. Expert Opin Biol Ther. 2004;4 (12):1963–70. doi: 10.1517/14712598.4.12.1963. [DOI] [PubMed] [Google Scholar]
- 8.Singhal S, Mehta J. Novel therapies in multiple myeloma. Int J Hematol. 2003;77(3):226–31. doi: 10.1007/BF02983778. [DOI] [PubMed] [Google Scholar]
- 9.Armoiry X, Aulagner G, Facon T. Lenalidomide in the treatment of multiple myeloma: a review. J Clin Pharm Ther. 2008;33(3):219–26. doi: 10.1111/j.1365-2710.2008.00920.x. [DOI] [PubMed] [Google Scholar]
- 10.Ocio EM, Mateos MV, Maiso P, Pandiella A, San-Miguel JF. New drugs in multiple myeloma: mechanisms of action and phase I/II clinical findings. Lancet Oncol. 2008;9(12):1157–65. doi: 10.1016/S1470-2045(08)70304-8. [DOI] [PubMed] [Google Scholar]
- 11.Minnema MC, van der Veer MS, Aarts T, Emmelot M, Mutis T, Lokhorst HM. Lenalidomide alone or in combination with dexamethasone is highly effective in patients with relapsed multiple myeloma following allogeneic stem cell transplantation and increases the frequency of CD4+Foxp3+ T cells. Leukemia. 2009;23 (3):605–7. doi: 10.1038/leu.2008.247. [DOI] [PubMed] [Google Scholar]
- 12.Hideshima T, Bergsagel PL, Kuehl WM, Anderson KC. Advances in biology of multiple myeloma: clinical applications. Blood. 2004;104(3):607–18. doi: 10.1182/blood-2004-01-0037. [DOI] [PubMed] [Google Scholar]
- 13.Tai YT, Catley LP, Mitsiades CS, Burger R, Podar K, Shringpaure R, et al. Mechanisms by which SGN-40, a humanized anti-CD40 antibody, induces cytotoxicity in human multiple myeloma cells: clinical implications. Cancer Res. 2004;64(8):2846–52. doi: 10.1158/0008-5472.can-03-3630. [DOI] [PubMed] [Google Scholar]
- 14.Tai YT, Li XF, Catley L, Coffey R, Breitkreutz I, Bae J, et al. Immunomodulatory drug lenalidomide (CC-5013, IMiD3) augments anti-CD40 SGN-40-induced cytotoxicity in human multiple myeloma: clinical implications. Cancer Res. 2005;65(24):11712–20. doi: 10.1158/0008-5472.CAN-05-1657. [DOI] [PubMed] [Google Scholar]
- 15.Tai YT, Dillon M, Song W, Leiba M, Li XF, Burger P, et al. Anti-CS1 humanized mono-clonal antibody HuLuc63 inhibits myeloma cell adhesion and induces antibody-dependent cellular cytotoxicity in the bone marrow milieu. Blood. 2008;112(4):1329–37. doi: 10.1182/blood-2007-08-107292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Byrd JC, Lin TS, Grever MR. Treatment of relapsed chronic lymphocytic leukemia: old and new therapies. Semin Oncol. 2006;33 (2):210–9. doi: 10.1053/j.seminoncol.2006.01.012. [DOI] [PubMed] [Google Scholar]
- 17.Friedberg JW. Treatment of follicular non-Hodgkin's lymphoma: the old and the new. Semin Hematol. 2008;45(3 Suppl 2):S2–S6. doi: 10.1053/j.seminhematol.2008.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hussein M, Berenson JR, Niesvizky R, Munshi N, Matous J, Sobecks R, et al. A phase 1 multidose study of dacetuzumab (SGN-40; humanized anti-CD40 mAb) in patients with multiple myeloma. Haematologica. 2010;95(5):845–8. doi: 10.3324/haematol.2009.008003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bergsagel PL, Smith AM, Szczepek A, Mant MJ, Belch AR, Pilarski LM. In multiple myeloma, clonotypic B lymphocytes are detectable among CD19+ peripheral blood cells expressing CD38, CD56, and monotypic Ig light chain. Blood. 1995;85(2):436–47. [PubMed] [Google Scholar]
- 20.Vooijs WC, Schuurman HJ, Bast EJ, de Gast GC. Evaluation of CD38 as target for immunotherapy in multiple myeloma. Blood. 1995;85(8):2282–4. [PubMed] [Google Scholar]
- 21.Malavasi F, Funaro A, Alessio M, DeMonte LB, Ausiello CM, Dianzani U, et al. CD38: a multi-lineage cell activation molecule with a split personality. Int J Clin Lab Res. 1992;22(2):73–80. doi: 10.1007/BF02591400. [DOI] [PubMed] [Google Scholar]
- 22.Mehta K, Shahid U, Malavasi F. Human CD38, a cell-surface protein with multiple functions. FASEB J. 1996;10(12):1408–17. doi: 10.1096/fasebj.10.12.8903511. [DOI] [PubMed] [Google Scholar]
- 23.Spaapen RM, Lokhorst HM, van den Oudenalder K, Otterud BE, Dolstra H, Leppert MF, et al. Toward targeting B cell cancers with CD4+ CTLs: identification of a CD19-encoded minor histocompatibility antigen using a novel genome-wide analysis. J Exp Med. 2008;205(12):2863–72. doi: 10.1084/jem.20080713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.van der Spek E, Bloem AC, Lokhorst HM, van Kessel B, Bogers-Boer L, van de Donk NW. Inhibition of the mevalonate pathway potentiates the effects of lenalidomide in myeloma. Leuk Res. 2009;33(1):100–8. doi: 10.1016/j.leukres.2008.06.001. [DOI] [PubMed] [Google Scholar]
- 25.Spaapen R, van den Oudenalder K, Ivanov R, Bloem A, Lokhorst H, Mutis T. Rebuilding human leukocyte antigen class II-restricted minor histocompatibility antigen specificity in recall antigen-specific T cells by adoptive T cell receptor transfer: implications for adoptive immunotherapy. Clin Cancer Res. 2007;13(13):4009–15. doi: 10.1158/1078-0432.CCR-07-0286. [DOI] [PubMed] [Google Scholar]
- 26.de Weers M, Tai YT, van der Veer MS, Bakker JM, Vink T, Jacobs DC, et al. Daratumumab, a Novel Therapeutic Human CD38 Monoclonal Antibody, Induces Killing of Multiple Myeloma and Other Hematological Tumors. J Immunol. 2010 Dec 27; doi: 10.4049/jimmunol.1003032. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 27.Kumar SK, Rajkumar SV, Dispenzieri A, Lacy MQ, Hayman SR, Buadi FK, et al. Improved survival in multiple myeloma and the impact of novel therapies. Blood. 2008;111(5):2516–20. doi: 10.1182/blood-2007-10-116129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gandhi AK, Kang J, Naziruddin S, Parton A, Schafer PH, Stirling DI. Lenalidomide inhibits proliferation of Namalwa CSN.70 cells and interferes with Gab1 phosphorylation and adaptor protein complex assembly. Leuk Res. 2006;30(7):849–58. doi: 10.1016/j.leukres.2006.01.010. [DOI] [PubMed] [Google Scholar]
- 29.Lu L, Payvandi F, Wu L, Zhang LH, Hariri RJ, Man HW, et al. The anti-cancer drug lenalidomide inhibits angiogenesis and metastasis via multiple inhibitory effects on endothelial cell function in normoxic and hypoxic conditions. Microvasc Res. 2009;77(2):78–86. doi: 10.1016/j.mvr.2008.08.003. [DOI] [PubMed] [Google Scholar]
- 30.Vallet S, Palumbo A, Raje N, Boccadoro M, Anderson KC. Thalidomide and lenalidomide: Mechanism-based potential drug combinations. Leuk Lymphoma. 2008;49 (7):1238–45. doi: 10.1080/10428190802005191. [DOI] [PubMed] [Google Scholar]
- 31.De Raeve HR, Vanderkerken K. The role of the bone marrow microenvironment in multiple myeloma. Histol Histopathol. 2005;20(4):1227–50. doi: 10.14670/HH-20.1227. [DOI] [PubMed] [Google Scholar]
- 32.Thomas X, Anglaret B, Magaud JP, Epstein J, Archimbaud E. Interdependence between cytokines and cell adhesion molecules to induce interleukin-6 production by stromal cells in myeloma. Leuk Lymphoma. 1998;32(1–2):107–19. doi: 10.3109/10428199809059251. [DOI] [PubMed] [Google Scholar]
- 33.Drach J, Kaufmann H, Urbauer E, Schreiber S, Ackermann J, Huber H. The biology of multiple myeloma. J Cancer Res Clin Oncol. 2000;126(8):441–7. [PubMed] [Google Scholar]