

Abstract
Context: Nurses are the primary hospital caregivers. Increasing the efficiency and effectiveness of nursing care is essential to hospital function and the delivery of safe patient care.
Objective: We undertook a time and motion study to document how nurses spend their time. The goal was to identify drivers of inefficiency in nursing work processes and nursing unit design.
Design: Nurses from 36 medical-surgical units were invited to participate in research protocols designed to assess how nurses spend their time, nurse location and movement, and nurse physiologic response.
Main Outcome Measures: Nurses' time was divided into categories of activities (nursing practice, unit-related functions, nonclinical activities, and waste) and locations (patient room, nurse station, on-unit, off-unit). Total distance traveled and energy expenditure were assessed. Distance traveled was evaluated across types of unit design.
Results: A total of 767 nurses participated. More than three-quarters of all reported time was devoted to nursing practice. Three subcategories accounted for most of nursing practice time: documentation (35.3%; 147.5 minutes), medication administration (17.2%; 72 minutes), and care coordination (20.6%; 86 minutes). Patient care activities accounted for 19.3% (81 minutes) of nursing practice time, and only 7.2% (31 minutes) of nursing practice time was considered to be used for patient assessment and reading of vital signs.
Conclusion: The time and motion study identified three main targets for improving the efficiency of nursing care: documentation, medication administration, and care coordination. Changes in technology, work processes, and unit organization and design may allow for substantial improvements in the use of nurses' time and the safe delivery of care.
Introduction
The US hospital system is in a state of transition. Hospitals face daunting challenges, such as evolving technologies and reimbursement policies, demographic trends, competing fiscal demands, and a worsening workforce shortage. This point in time also affords a unique opportunity, as the US is in the midst of one of the largest hospital-building and -renovation booms in history.1 A reconsideration of hospital design and work processes holds the potential to affect the efficiency and effectiveness of care delivery for the foreseeable future. Bold changes in the hospital work environment are imperative to ensure the sustainability and affordability of the hospital as part of the American health care delivery system.
Nurses are the linchpin of hospital care delivery. These frontline caregivers represent a critical and costly resource; maximizing the efficiency and effectiveness of nurses is essential to the integrity of hospital function and the promotion of safe patient care. A growing evidence base links more nursing time per patient-day with better patient outcomes.2–5 However, increased nurse workload and the growing nursing workforce shortage6 reduce the amount of nursing time available for patient care activities.
How medical-surgical nurses spend their time is a key driver of bold changes in the hospital work environment.7–9 Current research suggests that two interrelated elements—nurse work process and the physical hospital environment—contribute to the efficiency and safety of patient care.10–12 An understanding of how nurses spend their time will target opportunities for nursing care effectiveness through improvements in management, workforce, work processes, and organizational culture.13
We undertook a time and motion study to provide an evidence-based understanding of how medical-surgical nurses spend their time and of the influence of unit architectural layout on nurses' use of time and distance traveled. Documenting the drivers of inefficiency in nursing practice will allow for targeted changes to the work environment to positively influence patient safety and quality of care.
The primary objectives of the study were to identify how nurses spend their time during their shift and to pinpoint environmental variables in the acute-care nursing workplace that can be altered to positively affect the efficiency of nursing care and, ultimately, patient safety.
Specifically, the study aimed to determine:
the amount of time nurses spend on specific activities: nursing practice, unit-related functions, nonclinical activities, and waste
the distance traveled by the aver-age nurse during a typical shift, and whether this movement is efficient
the physiologic impact of the work environment on nurses.
This study was also designed to provide baseline data regarding documentation activities prior to the installation of electronic health record (EHR) technology in specific units. These findings are not included in this article because of complications in the analysis of the data collected.
Methods
The time and motion study was conducted at 36 hospital medical-surgical units within 17 health care systems and 15 states. Together, these geographically diverse health care systems operate a total of 274 hospitals with more than 63,000 beds. Each participating study health system and hospital's institutional review board approved the study protocol.
Study Units and Participants
From a list of all eligible medical-surgical units at each of the participating hospitals, one unit per hospital was randomly selected for inclusion in the study. An eligible medical-surgical unit was defined as a unit in which patients who require less care than that which is available in intensive care units, step-down units, or specialty care units, and receive 24-hour inpatient general medical services, postsurgery services, or both general medical and postsurgery services. These units may include mixed patient populations with diverse diagnoses and of diverse age groups who require care appropriate to a medical-surgical unit.
Nurses at each participating unit meeting the eligibility criteria were invited to join the study; participation was voluntary. To be eligible, nurses were required to be licensed (RN, LPN, or LVN) and to provide direct nursing care for patients on the study unit. In-house pool nurses were eligible if they worked on the study unit for more than eight weeks. Ineligible nurses included: float and agency nurses; nurse preceptors and preceptees; and nursing supervisors, charge nurses, or other nurse specialists, unless they provided direct nursing care with the same acuity and patient load as other participants.
Study Protocols
The study consisted of four protocols: A, B, C, and D (Table 1). Nurses who consented to participate were randomized to either protocol A or protocol B. All nurses were asked to participate in protocol C, and any nurse who volunteered to do so took part in protocol D. For each protocol, study staff collected data for seven consecutive days, 24 hours a day, except for protocol D, for which data were collected for 23 hours a day.
Table 1.
Description of study protocols
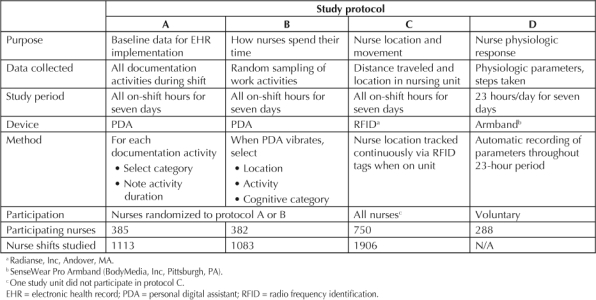
Protocol A: Baseline Data for EHR Implementation
Nurses participating in protocol A were supplied with personal digital assistants (PDAs) to record all documentation-related activities during their shifts. With these PDAs, unit nurses documentation categories from the following options:
Admission paperwork
Assessment
Transcribe orders
Writing care plan
Medications paperwork
Teaching
Discharge paperwork
Other.
For each documentation activity, nurses selected “start” on their PDA, then the documentation category. When they completed the activity, nurses pressed “stop.” Protocol A sought to measure the amount of time spent on nursing work processes before the installation of EHRs. Pre- versus postinstallation results will be reported elsewhere.
Protocol B: How Nurses Spend Their Time
Nurses in research protocol B carried PDAs that vibrated at random times during their work shift to remind them to stop what they were doing and record the activity in which they were engaged. Each PDA was programmed to vibrate 25 times per 13-hour shift (in case of overtime), with a minimum interval of ten minutes between alarms. If the nurse did not respond immediately, the PDA continued to vibrate every 15 seconds until the nurse responded. When the PDA vibrated, the nurse was asked to select from categoric data sets describing where they were (patient room, nurse station, on unit, or off unit) and what they were doing (Table 2). For this report, the term patient room refers to any patient room that the nurse visited, not a single patient room.
Table 2.
Categories and subcategories of nursing time for protocol B
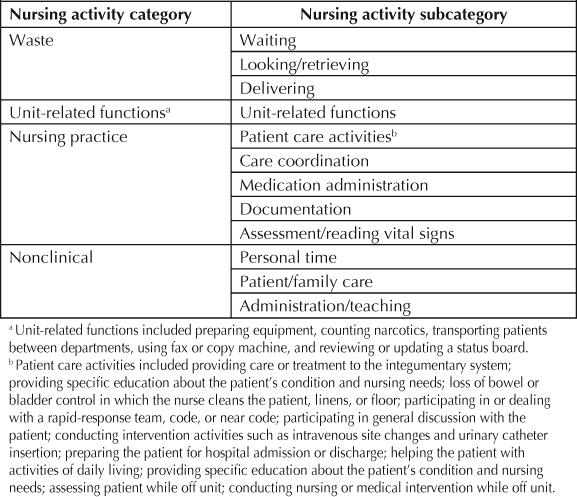
The nurses' activities were clustered into categories and subcategories of how much time nurses spend on activities considered to be nursing practice, nonclinical, unit-related, or waste. These categories and subcategories (Table 2) were selected to cluster sufficient increments of time to make strong comparisons and to identify important targets for change. The goals were to reveal drivers of inefficiency in how nurses spend their time and to identify opportunities to improve efficiency through changes to unit design and/or organization.
The subcategory of patient care activities does not represent a comprehensive accounting of all activities related to patient care. Other care-related subcategories, such as medication administration, care coordination, and documentation were separated from patient care activities to help identify what activities consume nurses' time. These categories, therefore, are intended to be utilitarian rather than absolute.
To assess the physical impact of workload and stress on the nurses, volunteers … had their physiologic response monitored by specialized armbands …
Protocol C: Nurse Location and Movement
To monitor nurse location and movement, nurses in research protocol C wore radiofrequency identification (RFID) tags (Radianse, Inc, Andover, MA) that continually monitored where they were, how far they traveled, and the duration of activity in any one spot. Signals from each RFID tag were transmitted to an indoor positioning system installed on each unit for the study week. The RFID tags measured the distance traveled in relation to the physical layout of the nursing unit. As nurses spent only 20 to 30 seconds in any one spot, each nurse was fitted with four tags to ensure that grouping signals would not be missed.
Protocol D: Nurse Physiologic Responses
To assess the physical impact of workload and stress on the nurses, volunteers from any study group had their physiologic response monitored by specialized armbands (SenseWear Pro Armband, BodyMedia, Inc, Pittsburgh, PA) to measure the physiologic metrics both on and off shift for 23 hours a day for a seven-day period (nurses removed armbands for one hour per day). The armbands simultaneously measured skin temperature, near body temperature, galvanic skin response, heat flux, and motion via a two-axis accelerometer. From these data, estimates were made for total energy expenditure (calories burned), distance traveled, speed, active energy expenditure, sleep, and categories of physical activity.
Site Implementation
Before study startup, the optimal placement of IPS receivers were mapped on computerized architectural drawings (CADs) of the study unit. Two days before the data-collection period, the temporary wireless access points were installed and tested to ensure proper functioning. At each study unit, the necessary hardware was installed, and staff and management members were oriented regarding the purpose of the study and the use of devices before data collection. The hospital study coordinator managed the data-collection process with the unit manager and nurse executive.
The study was conducted at each site during a period of seven consecutive days. Data for all units were collected between June 2005 and June 2006.
Unit-Assessment Data-Collection Tool
A standardized unit-assessment data-collection tool was completed by each study unit's nursing manager to collect more than 200 hospital unit demographic, technologic, and architectural variables. These variables were used to interpret unit and nurse variation, as well as cluster relationships that correlated or explained the difference in efficiency and nursing time spent with patients.
Data Management and Statistical Analysis
The statistical and technical methods used in this study will be reported in detail in a separate publication. In brief, each hospital unit transmitted raw data to computer scientists at Purdue University who then stored the data in an Oracle database. Data was transferred from the Oracle database to an R system for graphics database. A new framework was used for data display in which a “visualization database” exhibited all cleaned data as well as summary statistics. This deep visualization allowed for the development of valid statistical models and the performance of appropriate data analyses.
Cross-Validation Between Protocols
Data collected from the different protocols allowed for cross-validation of certain findings. Distance traveled on the unit, for example, was evaluated in both protocol C (through RFID tracking) and protocol D (through armband accelerometer). Nurse location could be validated between protocol B (PDA selection of location) and protocol C (RFID-determined location). Before the study was begun, location data for protocol C was validated by tracking “walks in the units.” RFID-tracked location was compared with audio recordings from unit walk-through.
Results
Profile of Participating Hospitals and Nurses
Of the participating medical-surgical units, 33 were in urban facilities (3 rural) and 17 were part of teaching/academic institutions. The average length of stay for the study units ranged from 2.62 to 8.67 days (average, 4.37 days). Unit sizes ranged from 11 to 20 beds to 81 to 90 beds (median, 31–40 beds).
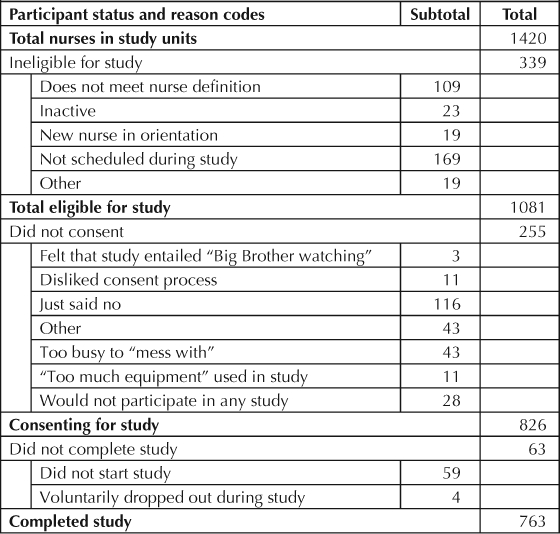
A total of 1420 nurses were identified at the 36 study units. Of this total, 339 were deemed ineligible by study criteria; 826 of the eligible nurses consented to participate, and 763 completed the study (Table 3). No participants were removed from the study because of noncompliance. The majority of participants were RNs (783), and the remainder were LPN/LVN (43). Nurses' educational background was as follows: 57%, AD or nursing diploma; 41%, BSN; 2%, MSN.
Table 3.
Nurses eligible, consenting, and completing study
The study population of 767 nurses were randomized, 385 to protocol A and 382 to protocol B (Table 1). All nurses were included in protocol C, with the exception of nurses at one study unit, leaving a total of 750 participants. For protocol D, 288 nurses volunteered. In all, data were collected for 2201 nursing shifts (2065 RNs; 136 LVNs/LPNs) and 21,882 total hours (20,573 RNs; 1309 LVNs/LPNs). Average shift length was 9.94 hours.
Nurses randomized to protocol B responded on average 17 times per shift. Figure 1 illustrates the average time spent by nurses in each location category (patient room, on the unit, off the unit, nurse station); an additional 45 minutes per average 10-hour shift (7.5% of a ten-hour shift) were not accounted for by participants (no response, no location chosen, undefined, or pushed wrong response). Percentages reported below and in Figures 1 through 5 do not include undocumented time.
Figure 1.
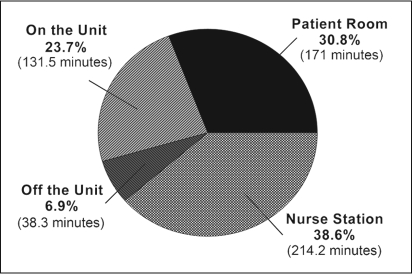
Reported nurse time by location.
In protocol B, location was selected by the nurse from four categories: patient room, nurse station, on the unit, and off the unit. Data were normalized to a 10-hour shift (600 minutes). Of this total, 45 minutes (7.5% of total) were not accounted for by participants (data not shown). Data in chart are percentages of all reported time (555 minutes).
Figure 5.
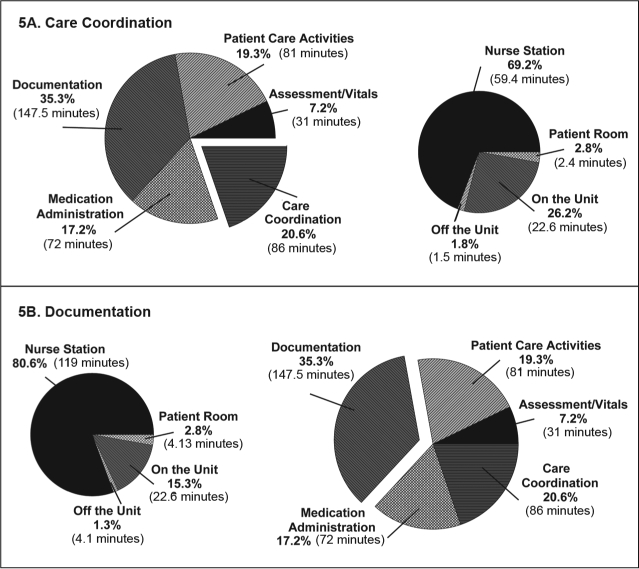
Care coordination and documentation subcategories by location.
Analysis of nursing practice subcategories by location found that care coordination was performed primarily at the nurse station (69.2%) and documentation was also performed primarily at the nurse station (80.6%).
Figure 2 illustrates how nurses spent their time by activity category. More than three-quarters of nurses' time was devoted to nursing practice (417 minutes, 77.7% reported time per shift). Activities considered to be waste consumed 36.3 minutes, or 6.6%, of reported time per 10-hour shift. Nurses' time was further analyzed according to activity by location, and by subcategory. Figure 3 illustrates the amount of time per activity category in each of the four locations. Nursing practice accounted for the majority of time in all locations except off the unit. Waste and nonclinical activities accounted for larger proportions of time spent by nurses on the unit (excluding patient room and nurse station) or off the unit, compared to the patient room and nurse station. Time devoted to nonclinical activities was approximately equivalent for nurse station (20.6 minutes), on the unit (17.8 minutes), and off the unit (18.2 minutes); nonclinical activities accounted for only 11.3 minutes of time spent in the patient room.
Figure 2.
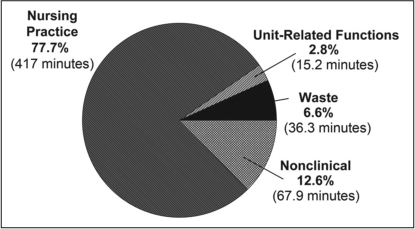
Reported nurse time spent by care category.
In protocol B, activity category was selected by the nurse from the following: nursing practice, nonclinical, unit-related functions, or waste. Data were normalized to 10-hour shift (600 minutes). Of this total, 63.5 minutes (10.6% of total) were not accounted for by participants (data not shown). Data in chart are percentages of all reported time (536.4 minutes). Nursing practice accounts for over three-quarters of all nursing time.
Figure 3.
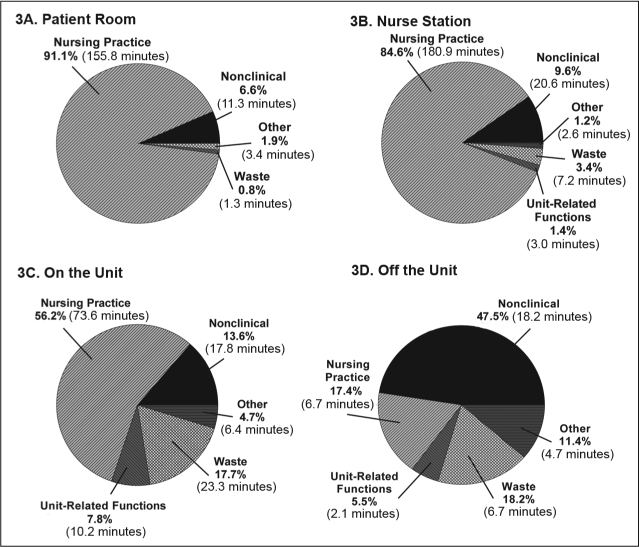
Reported nurse time in each activity category by location.
Activity category data from protocol B were examined by each of the four nurse locations: patient room (3A), nurse station (3B), on the unit (3C), and off the unit (3D). Unreported time is categorized as “other.” Nursing practice accounted for most time in the patient room and at the nurse station and a majority of time on the unit. Time off the unit was fragmented into multiple categories.
Nursing Practice: Locations and Subcategories
Nursing practice time was concentrated in the patient room (155.7 minutes) and nurse station (180.6 minutes) (Figure 4A). Within nursing practice, the greatest proportion of time was devoted to documentation (147.5 minutes, 35.3%, Figure 4B). Care coordination—communication with team members or other departments—accounted for 86 minutes (20.6% of nursing practice). Patient care activities accounted for less than one-fifth of total nursing practice time (81 minutes, 19.3%); time spent on assessment and obtaining vital signs was least among subcategories of nursing practice (30.9 minutes, 7.2%).
Figure 4.
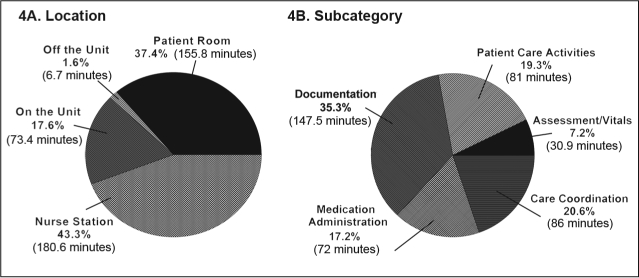
Nursing practice by location and by subcategory.
Analysis of nursing practice time by location revealed that the largest proportion of nursing practice was done at the nurse station (4A). Three subcategories of nursing practice (4B) consumed most nursing practice time not accounted for by patient care activities: documentation, medication administration, and care coordination.
The subcategories care coordination and documentation were further analyzed by dividing each according to nurses' location (Figure 5A/B). Both were performed predominantly at the nurse station (documentation: 119 minutes, 80.6% documentation time; care coordination: 59.4 minutes, 69.2% care coordination time). Only a minority of care coordination (2.4 minutes, 2.8%) and documentation (4.13 minutes, 2.8%) took place in the patient room.
Unit Architecture
Three different unit architectural types were included in the study: “racetrack,” “corridor,” and “radial.” Of 36 study units, 19 had a racetrack design; 12, corridor; and 5, radial. The effects of these three design types and design subtypes on nurses' activities were evaluated. No consistent, statistically significant relationship was found between the various architectural types and nursing time spent with patients.
Distance Traveled
Individual nurses across all study units traveled between 1 and 5 miles per 10-hour daytime shift. During daytime shifts, average distance traveled ranged between 2.4 and 3.4 miles per 10 hours (median, 3.0 miles).
Nurses traveled less distance during nighttime shifts when most activities and patient tasks change (patients are less mobile, pain often increases). On night shifts, average distance traveled ranged between 1.3 and 3.3 miles per 10 hours. The median distance was 2.2 miles, a reduction of 0.8 miles per 10 hours from daytime shifts.
Nurses spent considerably less time moving when they were not at work. While they were off shift during the daytime, distance traveled varied from 1.2 miles to 3.5 miles. The median was 2.1 miles, or 0.9 miles fewer per 10 hours compared with daytime work shifts.
Variation Between Shifts
Distance traveled varied widely by shift. Distance per shift varied by a factor of four or more, even within the same unit (data not shown). Time spent on various activities (including documentation) also varied considerably between shifts. Of interest, the variability between individual nurses on the same unit was often greater than the variance across different hospital units.
Physiologic Impact
The normalized metabolic equivalents (nME), defined as energy expenditure during activity normalized to energy expenditure during sleeping time (ie, nME = 1 during sleep), were calculated for nurses in protocol D. The median nME for nurses on daytime shifts was 1.71. Nurses working on night shifts had a reduced nME, with a median of 1.52, an 11% reduction. While they were off shift, nME dropped to a median of 1.5, a 12% reduction from the daytime shift.
Discussion
This study is the first hospital environmental study to quantify how nurses spend their time, in real-time and in real work contexts. The findings demonstrate that nurses spent more than three-quarters of their time on nursing practice-related activities—but less than one-fifth of all nursing practice time on activities defined as patient care activities. Three other activities accounted for the majority of nursing practice time: documentation, care coordination, and medication administration. Only 7.2% (31 minutes) of nursing practice time was dedicated to patient assessment and recording of vital signs.
Of all reported time, 6.6% (36.3 minutes) was categorized as waste. Activities within this category—many of which were “hunting and gathering” behaviors—are clearly targets for improving efficiency. The much larger proportions of time devoted to care coordination, medication administration, and, in particular, documentation may also represent opportunities for process improvement. Documentation accounted for the largest proportion of nursing time; in fact, this category by itself accounts for 27.5% of all reported time, more than unit-related functions, nonclinical activities, and waste combined.
Among locations, the nurse station featured prominently. Nurses spent the largest proportion of their time—38.6% (214.2 minutes)—at the nurse station, compared with less than one-third (171 minutes) in the patient room. It is also the primary location for activities related to documentation and care coordination. Whereas time spent in the patient room and at the nurse station was almost entirely devoted to nursing practice (Figure 3), nurses' time at other locations on the unit and off the unit was fragmented between nursing practice, nonclinical activities, unit-related functions, and waste.
A picture emerges of the professional nurse who is constantly moving from patient room to room, nurse station to supply closet and back to room, spending a minority of time on patient care activities …
A picture emerges of the professional nurse who is constantly moving from patient room to room, nurse station to supply closet and back to room, spending a minority of time on patient care activities and a greater amount of time on documentation, coordination of care, medication administration, and movement around the unit. The motion findings of the study support this picture. Nurses walked significant distances while at work and walked farther while on shift (median, 3.0 miles) than when not at work (median, 2.1 miles). In previous studies, walking has been identified as a major time consumer for nurses, and evidence suggests that time saved walking translates into more time spent on patient-care activities.1
Previous research has shown that a primary reason for nurse attrition is the workloads traditionally inherent in this profession.14 Our findings regarding the physical activity required in nursing—long distances traveled and increased metabolic expenditure—corroborate the physical and workload demands nurses endure on a regular basis.
Documentation
Documentation is an essential part of nursing practice and accounts for a major portion of the nurses' time. The documentation process in many hospitals is also rife with inefficiencies. For example, nurses and other care providers often must transfer information between data collection systems, consuming nursing time and contributing to transcription errors. Documentation is often duplicated between departments and disciplines because of the lack of a single patient problem list for all providers. The result is fragmentation of care, duplication of data sets, and the inability to quantify the outcome of the care provided. Evolving regulatory and public policy requirements for documentation (such as “present on admission”) may exacerbate these problems.15
The efficiency of documentation is a multifactorial problem, and solutions remain varied and controversial. Health care systems will need robust processes driven by caregivers to improve efficiency and reduce time dedicated to documentation. There is hope that EHRs will improve efficiency, but whether they can has not yet been documented.
Medication Administration
Like documentation, medication administration is an essential component of nursing practice. Because nurses devote considerable time to this category of care, opportunities may exist to improve efficiency. Approximately two-thirds of all time spent on medication administration in this study was related to drug delivery to the patient (46.7 minutes). The other third (24.9 minutes) was spent preparing drugs for administration. Process improvements could reduce the time required for this step. Furthermore, medication administration has been identified by other researchers as a leading source of operational failures.10
Hospital medication processes may be affected by the fragmentation of the informatics infrastructure. In an ideal patient care nursing unit, medications would be administered as part of a seamless closed-loop system that provides accurate and timely information about the patient, including patient identification, order verification, allergies, laboratory values, potential reactions, and preferences. Operational failures within this process demand the nurse's attention and time and may be a source of additional distance traveled.
Proposed improvements to this process include advanced automated dispensing systems, the use of small medication cabinets within the patient room, and the use of case carts to provide most medications predicted on that basis of patient condition. Creating closed-loop medication administration systems will require an interdisciplinary effort, including supply chain, informatics, work process, and vendor platform integration.
Care Coordination
Care coordination (communication regarding the patient) accounts for approximately one-fifth of nursing practice time. The benefits of timely and efficient communication between team members have been documented by other investigators.16–19 However, inefficiencies in communication may consume nurses' time and put patients at risk. Failure to rescue—death following the occurrence of an adverse event—is a nurse-sensitive outcome that has been correlated with nurse–patient ratios, communication, and patient surveillance, among other factors.2 Indeed, many failure-to-rescue situations can be traced back to communication delays or omissions.
The efficient flow of patient information and status updates could reduce wasted time and the potential for errors. Proposed technology solutions include wireless networks, handheld and ear devices for the delivery of patient information, and intelligent systems that automatically track the physical location of a medical provider.
Most care coordination time is spent at the nurse station. Indeed, the nurse station itself may represent an opportunity for design and process improvement. The location of terminals and/or wireless devices for data entry, for example, could reduce the need for and time spent at the nurse station. Such changes could reduce walking time between patient rooms and the nurse station, and increase the amount of time available in the patient room.
Nursing Unit Design
One of our study objectives was to describe the variation in distance traveled, time spent by category, and workload between units with different physical layouts. No statistically significant correlation was found between type of unit design and time spent with patients. In fact, there was more variation in miles traveled and patient time between nurses on the same unit than between units. One likely explanation for these findings is that nurses' ability to organize their work and staffing assignments has greater impact on these measures than does physical space by itself. For example, a nurse with geographically contiguous patient assignments traveled less than a nurse with an assignment based on the level of acuity of illness in which patients were placed in noncontiguous rooms. This finding suggests that process and policy, as well as relatively minor physical changes within a unit (such as distribution points of supplies or medications), can have a major impact on nurse workload.
Nurses' adaptability may allow them to compensate for limitations imposed by the physical design of the unit. This adaptation may mask potential effects of unit layout on distance traveled and time spent per activity. Additional statistical analyses of time and motion data are currently underway to detect interactions between unit architecture and nurse time and movement.
It may be that for unit layout to make a difference in nursing time spent on patient care activities, other contextual factors must also change. Such factors include the interoperability of technology, staff work assignments, and work processes. Previous research provides compelling evidence that poorly organized practice environments can negate the benefits of excellent staffing and positive patient outcomes.20,21 A holistic approach is needed whereby people, process, and technology come together harmoniously in a physical space to produce the maximum medical-surgical unit efficiency.
Study Limitations
The challenge study nurses faced in continuing their jobs without interference from the time and motion study (both with respect to patient needs and ensuring study validity) might have led to problems in the data collected. For example, some nurses in protocol A forgot to turn off their PDAs after completing their respective activity, leading to outlier times in the database. In protocol B, nurses occasionally selected no category or pressed incorrect buttons. These are limitations of the self-report methodology.
The study design required identification of all activities of a nursing shift and grouping these activities into cogent, useful, and appropriate categories. The rationale for these activities and groupings could be sensibly debated. The category of patient care activities, for example, does not include activities, such as medication administration, that have obvious and direct impact on patient safety and outcomes. The categories were selected with the intention of grouping activities that comprise sufficient nursing time to provide useful data while avoiding more vague terms such as direct and indirect care.
Conclusions
Nurses are the primary hospital caregivers, and the efficient use of their time and energy is critical to the future of American hospitals. Our study evaluated the time that nurses spent and the distance that they traveled across 36 geographically diverse medical-surgical units. The results demonstrate that nurses devote large proportions of their time to documentation, medication administration, and care coordination and somewhat less time to patient care activities. Nurses also travel significantly larger distances and exert more energy during daytime shifts than when away from work.
A holistic approach is needed whereby people, process, and technology come together harmoniously in a physical space to produce the maximum medical-surgical unit efficiency.
These findings illustrate the complex and demanding hospital work environment and suggest opportunities to improve the efficiency of nursing work. Changes to the process and technology of documentation, communication, and medication handling, as well as the physical design of units, could benefit nursing efficiency and the safe delivery of care.
Truly transforming the hospital–patient care environment to improve the delivery of safe, high-quality, patient-centered care would be a paradigm shift. The task now is to test solutions to create a more effective work environment that seamlessly supports clinicians in the direct care of patients.
Disclosure Statement
The author(s) have no conflicts of interest to disclose.



Acknowledgments
This study was funded by grants from the Robert Wood Johnson Foundation and the Gordon and Betty Moore Foundation.
We thank the following health systems: Ascension Health, Aurora Health Care, Carolinas HealthCare System, Christiana Care Health System, Duke University Health System, Henry Ford Health System, Intermountain Healthcare, Inova Health System, Kaiser Permanente, Legacy Health System, Moses Cone Health System, New York–Presbyterian (the University Hospital of Columbia and Cornell), North Shore-Long Island Jewish Health System, Saint Barnabas Health Care System, Sisters of Mercy Health System, Trinity Health, and Vanderbilt University.
We are indebted to Wendy S Goshert, National Study Coordinator, Health Evolutions, Inc; the Purdue University–based time and motion study research team led by William S Cleveland, PhD, Department of Statistics, and Christopher W Clifton, PhD, Department of Computer Science; James Serack, PhD, Chief Technology Officer, CSC; and the Ascension Health and Kaiser Permanente project managers with special recognition to Sylvia Speck and Curtis Dikes.
Joshua Kilbridge of Kilbridge Associates provided writing assistance.
Katharine O'Moore-Klopf of KOK Edit provided editorial assistance.
References
- Ulrich R, Quan X, Zimring C, Joseph A, Choudhary R.The role of the physical environment in the hospital of the 21st century: a once-in-a-lifetime opportunity [monograph on the Internet, about 69 pages] Concord, CA: The Center for Health Design; 2004. [cited 2008 Apr 21]. Available from: www.healthdesign.org/research/reports/pdfs/role_physical_env.pdf. [Google Scholar]
- Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002 Oct 23;288(16):1987–93. doi: 10.1001/jama.288.16.1987. [DOI] [PubMed] [Google Scholar]
- Kovner C, Jones C, Zhan C, Gergen PJ, Basu J. Nurse staffing and post-surgical adverse events: an analysis of administrative data from a sample of US hospitals, 1990–1996. Health Serv Res. 2002 Jun;37(3):611–29. doi: 10.1111/1475-6773.00040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Needleman J, Buerhaus P, Mattke S, Stewart M, Zelevinsky K. Nurse-staffing levels and the quality of care in hospitals. N Engl J Med. 2002 May 30;346(22):1715–22. doi: 10.1056/NEJMsa012247. [DOI] [PubMed] [Google Scholar]
- Anderson S.Deadly consequences: the hidden impact of America's nursing shortage [monograph on the Internet] Arlington, VA: National Foundation for American Policy; 2007 Sep. [cited 2008 Apr 21]. Available from: www.nfap.com/pdf/0709deadlyconsequences.pdf. [Google Scholar]
- O'Neil E.Healthcare workforce in the US economy. San Francisco: Health Workforce Solutions LLC; 2007. [Google Scholar]
- Lundgren S, Segesten K. Nurses' use of time in a medical-surgical ward with all-RN staffing. J Nurs Manag. 2001 Jan;9(1):13–20. doi: 10.1046/j.1365-2834.2001.00192.x. [DOI] [PubMed] [Google Scholar]
- Hendrickson G, Doddato TM, Kovner CT. How do nurses use their time? J Nurs Adm. 1990 Mar;20(3):31–7. doi: 10.1097/00005110-199003000-00008. [DOI] [PubMed] [Google Scholar]
- Quist BD. Work sampling nursing units. Nurs Manage. 1992 Sep;23(9):50–1. [PubMed] [Google Scholar]
- Tucker AL, Spear SJ. Operational failures and interruptions in hospital nursing. Health Serv Res. 2006 Jun;41(3 Pt 1):643–62. doi: 10.1111/j.1475-6773.2006.00502.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tucker AL. The impact of operational failures on hospital nurses and their patients. Journal of Operations Management. 2004 Apr;22(2):151–69. [Google Scholar]
- Hendrich A, Fay J, Sorrells A. Courage to heal: comprehensive cardiac critical care. Healthcare Design. 2002 Sep:11–13. [Google Scholar]
- Institute of Medicine. Keeping patients safe: transforming the work environment of nurses. Washington, DC: National Academy Press; 2004. [Google Scholar]
- Shindul-Rothschild J, Berry D, Long-Middleton E. Where have all the nurses gone? Final results of our Patient Care Survey. Am J Nurs. 1996 Nov;96(11):25–39. doi: 10.1097/00000446-199611000-00034. [DOI] [PubMed] [Google Scholar]
- Centers for Medicare & Medic-aid Services. Eliminating serious, preventable, and costly medical errors—never events [press release on the Internet] Baltimore, MD: US Department of Health and Human Services; 2006 May 18. [cited 2008 Apr 21]. Available from: www.cms.hhs.gov/apps/media/press/release.asp?Counter=1863. [Google Scholar]
- Sexton JB, Holzmueller CG, Pronovost PJ, et al. Variation in caregiver perceptions of teamwork climate in labor and delivery units. J Perinatol. 2006 Aug;26(8):463–70. doi: 10.1038/sj.jp.7211556. [DOI] [PubMed] [Google Scholar]
- Sexton JB, Thomas EJ, Helmreich RL. Error, stress, and teamwork in medicine and aviation: cross sectional surveys. BMJ. 2000 Mar 18;320(7237):745–9. doi: 10.1136/bmj.320.7237.745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCauley K, Irwin RS. Changing the work environment in ICUs to achieve patient-focused care: the time has come. Chest. 2006 Nov;130(5):1571–8. doi: 10.1378/chest.130.5.1571. [DOI] [PubMed] [Google Scholar]
- Pronovost PJ, Wu AW, Sexton JB. Acute decompensation after removing a central line: practical approaches to increasing safety in the intensive care unit. Ann Intern Med. 2004 Jun 15;140(12):1025–33. doi: 10.7326/0003-4819-140-12-200406150-00013. [DOI] [PubMed] [Google Scholar]
- Aiken LH, Smith HL, Lake ET. Lower Medicare mortality among a set of hospitals known for good nursing care. Med Care. 1994 Aug;32(8):771–87. doi: 10.1097/00005650-199408000-00002. [DOI] [PubMed] [Google Scholar]
- Aiken LH, Patrician PA. Measuring organizational traits of hospitals: the Revised Nursing Work Index. Nurs Res. 2000 May–Jun;49(3):146–53. doi: 10.1097/00006199-200005000-00006. [DOI] [PubMed] [Google Scholar]