

Abstract
In addition to the inherent qualities of a digital image, the qualities of the monitor and graphics control card as well as the viewing conditions will affect the perceived quality of an image that is displayed on a soft copy display (SD) system. With the implementation of picture archiving and communication systems (PACS), many diagnoses are being made based on images displayed on SD devices, and consequently SD quality may affect the accuracy of diagnosis. Unlike the traditional film-on-lightbox display, optimal SD system parameters are not well defined, and many issues remain unsettled. In this article, the human observer performance, as measured by contrast sensitivity, for several SD devices including an active matrix liquid crystal flat panel monitor is reported. Contrast sensitivities were measured with various display system configurations. Experimental results showed that contrast sensitivity depends on many factors such as the type of monitor, the monitor brightness, and the gamma settings of the graphics card in a complex manner. However, there is a clear correlation between the measured contrast thresholds and the gradient of the display device’s luminance response curve. Based on this correlation, it is proposed to use the gradient of luminance response curve as a quality-index or metric for SD devices.
Keywords: Soft copy display, contrast sensitivity, gradient of luminance response curve, display quality index, human observer performance
A DISPLAY SYSTEM is the final link between the acquired image data and the eye–brain system of the human observer. Obviously the quality of a soft copy display (SD) system has a direct impact on the perceived image quality, and various components of an SD system can affect the performance of the human observer.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15 An SD system typically includes a monitor (either CRT or LCD flat-panel) and a graphics control card. An SD system is more complex than a conventional film/lightbox (the hard copy) display system, and it has many varieties. In radiology, the increasing number of picture archiving and communication system (PACS) implementations worldwide has led to an increasing number of diagnostic decisions being made based on images that are displayed on computer monitors. However, the quality of SD systems varies and there is no common, easy-to-use quality index to determine and to compare the quality of a display or to predict a user’s performance. Furthermore, image processing and manipulation may partially compensate for an SD system’s contrast and spatial resolution deficiency.7,16,17 For instance, zooming in on an image on an SD work station can compensate for the spatial resolution limitations of the monitor. Also, it is possible to adjust image contrast by “windowing and leveling” of an image. However, these adjustments decrease a user’s performance efficiency. Thus, it is important to ensure the optimization of the entire SD system so that unnecessary adjustments are minimized.
To display a digital image on an SD system involves multiple steps. It can be briefly described as follows. Once the image acquisition modalities (e.g., CR, DR, CT, and MR) acquire the images, they are stored as digital data on a computer. A digital image is represented in a computer by a two-dimensional matrix of data. Each data point of the matrix is called a pixel. Pixels are normally represented by integer values ranging from 0 to 4096 (12 bits). On a computer, the pixel matrix can be processed or manipulated to enhance certain features in an image. Modern imaging software offers a variety of image-processing algorithms. One example of these algorithms is the familiar “widowing and leveling,” where pixel values within some data range are re-scaled to match the full output range of the display in order to enhance the contrast. A graphics card on the computer produces the analog signals required for image display monitors. On the graphics card, pixel values are scaled into digital driving levels (DDLs) matched to the acceptance range of the card’s digital-to-analog converter (DAC). Normal ranges are 8 bits for desktop computers, and 10 bits for some specialized medical display devices. The DDL scaling process utilizes a conversion table, which is often referred to as the “look-up table” (LUT) on the graphics card and can be adjusted on some cards. The analog output of the graphics card drives the display monitor. The electronics in a monitor amplifies the analog signals to modulate the intensity of the electron beam for the CRT monitors or the driving voltage for LCD monitors. Through fast scanning, the monitor generates a visible pattern of luminance distribution, i.e., the “image.” Signal amplification in the CRT monitor’s electronics is linear by design. However, the CRT cathode follows a power-law response, thus the CRT monitors’ electronics inclusive of the cathode response is nonlinear. This adds another level of conversion in the image displaying process.
Therefore, at least three steps of conversion have been performed before an image data matrix is displayed on a monitor. The first step is the computerized image processing and enhancement performed on the data, which is independent of the display device. The second conversion occurs when the post-processed pixel data is scaled to DDLs on the graphics card. The third happens when the output analog video voltage from the graphics card is converted to a luminance pattern (i.e., the visible image) on the monitor. Each of these conversions will affect the final appearance of an image. To explain the differences in image appearance between SD systems, these multiple conversions must all be taken into account. In this article, however, the focus is on the last two conversions, both of which happen within the display system. The combination of the second and the third conversion steps is referred as the luminance response curve throughout this article. The luminance response curve relates the pixel value of a digital matrix to the measured monitor luminance output for that pixel value. An SD system’s luminance response curve will be affected by the characteristics of monitor, graphics card, and viewing conditions.
An SD system’s brightness, spatial resolution, number of distinct shades of gray, contrast ratio, LUT, and viewing conditions are all members of the long list of factors affecting image perception and the performance of a human observer. In radiology, these factors usually affect human performance by influencing the visibility of structures or abnormalities with respect to the background. Thus there is a direct effect on the sensitivity and specificity of clinical diagnoses.1,2,3,4,7,9 Furthermore these factors may affect the time taken to perform a task as well as the observer’s level of fatigue. However, the two most important aspects of any image-display device are the spatial and contrast resolution. The higher the spatial resolution, the better the display quality is. For SD systems, the spatial resolution is limited by monitor technology, and a compromise is usually struck between spatial resolution, brightness, contrast ratio, and cost. Contrast resolution is more complex and can be adjusted in an SD system. The contrast resolution of an SD system may be different at different pixel levels (or different luminance levels) depending on the configurations of the monitor and the graphics card. It is partially constrained by the monitor brightness range and the bit depth of the graphics card.18,19,20 Therefore, the quality of two identical SD devices may differ because of differences in configuration. In addition, image processing and manipulation can also modify image contrast. This is independent of the SD system but is often confused with the contrast modification done by the display. Ideally an SD system should be adjusted to ensure the optimal performance of a human observer. In this article we report the contrast sensitivity measurements of several monitors designed for medical applications and several desktop computer monitors.
In the past several years, the active matrix liquid crystal display (AMLCD) based monitors have been introduced to the radiology community for primary diagnostic usage in PACS by several vendors and have gained broader clinical acceptance. However, the understanding of their characteristics, especially the contrast sensitivity, is not widely known. As of today, the predominant component for the flat panels is the IBM 3 megapixel core. The performance attributes of the AMLCD core form a common backdrop for the various electronic configurations of row/column driver, internal calibration LUT (if present), and graphics card performance. The metrics that have served the industry for decades with CRT-based displays must now be redefined to encompass attributes such as off-axis viewing, latent image retention, and discontinuities in response inherent in the AMLCD. It is up to the vendors to address the response characteristics so that they are transparent to the end user, providing a display system that achieves digital imaging and communication in medicine (DICOM) compliance.
The responsiveness of the AMLCD to small luminance signal changes has been a primary weakness of the technology. In this study, we measured the contrast sensitivity of an AMLCD monitor and compared it to that of the conventional CRT-based monitors.
METHODS
An interactive computer program was developed to measure the observer’s contrast sensitivity for the SD devices evaluated. During the experiments, a human observer was presented with a series of test images. In each of the test images, there was a single circular object randomly located on a uniform background. If the observer pointed and clicked the mouse at the correct location of the object, then another object with decreased object contrast but the same size appeared at another random location. The tests continued until the observer could no longer correctly locate the object. The last visible contrast level was recorded automatically as the contrast threshold for that particular object size and that particular background level. More test images with another object size were then presented to the observer. This continued until the contrast thresholds for a pre-defined range of object sizes and background levels were obtained. Details about this interactive program and the data acquisition can be found in a previous publication.21 The computer program can be obtained for evaluation and research purposes by contacting the authors directly.
Contrast thresholds were measured at various background luminance levels for a range of object sizes, from small (2 mm diameter) to large (10 mm diameter). To simulate the clinical use of these monitors, observers were instructed to perform the testing from a comfortable viewing distance (normally around 40-50 cm). No restrictions were applied to their viewing distance or viewing angle.
Contrast threshold was defined as the pixel value difference of the object from that of its background. It was calculated by subtracting the pixel value for the background from that of the object. A lower contrast threshold means that the observer can see an object with lower contrast, and thus the display system has higher contrast sensitivity (or better user performance). The test images were all 8-bit gray-scale images. In other words, the maximum brightness corresponded to a pixel value of 255 and the minimum brightness corresponded to a pixel of zero.
To study the effect of room lighting on detection performance, the contrast thresholds were also measured with and without the fluorescent room light on. This resulted in a measured value of 170 lux with the lights on 2 lux with the lights off.
Several monitors were evaluated in the experiments, which included a Clinton Electronics DL3000 AMLCD flat-panel monochrome monitor, a Clinton Electronics DMA373 CRT monochrome monitor, an Image Systems M21HBMax CRT monochrome monitor, an Image System M21Max CRT monochrome monitor, and several color CRT monitors (ViewSonic GA771, NEC MultiSync XVI7, and KDS XF9c). All monochrome monitors were designed for medical imaging use. A computer running Microsoft NT was used to generate digital test images used in this study. The computer system had its own internal graphics adapter that allowed the user to set the display matrix size and gamma. The graphics adapter supported a 256 step gray-scale (8-bit). The matrix size of the graphics adapter was set to 1280 × 1024 for all displays except the AMLCD flat-panel monitor. For the flat-panel monitor, a computer equipped with a Matrox Med 3MP graphics card was used.
The monitor’s luminance outputs for a range of pixel values were measured for each display with a calibrated Minolta LS110 luminance meter (Minolta Corporation, Ramsey, NJ). The measurement set-up followed the protocol recommended by AAPM TG18.27 The measurements give the luminance response curve of each display system. No additional conversion was applied at the software level. The gradient of luminance response curve is defined as the slope of the log (luminance) versus pixel value plots. Thus the unit for the gradient of luminance response curve is log (cd/m2)/(pixel value).
A total of 10 observers (age range: 25 years to 58 years) participated in the studies, although not all observers participated in all experiments. Their contrast threshold measurements were repeated three times for intra- and inter-observer repeatability assessment of contrast threshold measurement.
Results
The AMLCD Flat-Panel Monitor
Figure 1a shows the luminance response curve of the Clinton Electronics DL3000 AMLCD flat-panel monitor measured at 90 degrees (perpendicular to) and 45 degrees to the monitor surface. The x-axis represents the input pixel values, and the y-axis represents the corresponding luminance levels in cd/m2 (log scale). Note that there is a slight luminance decrease at the 45-degree angle, which is expected because of the intrinsic angular-dependence of LCD luminance output. In addition, a close-up view of the luminance response curve (Fig 1b) reveals “step-like” features on the luminance response curve at some pixel values. Note that at these pixel values, an increase in pixel value does not result in increase in output luminance level, and some even have decreased luminance level. Figure 1c is a plot of the gradient of the luminance response curve in Figure 1a. The gradient of the luminance response curve is defined as the slope of the luminance response curve in Figure 1a and has a unit of cd/m2 per pixel value (in log scale). Note the spikes and troughs on the luminance response curve (Fig 1c), which are the results of the step-like features from the luminance response curve. This step-like feature in the luminance response curve is a problem unique to the present AMLCD technology, and it is a result of the intrinsic response of the liquid crystal material to applied voltage. The liquid crystals’ response to the two least significant bits of AMLCD is also problematic, and often techniques such as “dithering” are used to force a response that would otherwise not occur. For comparison, Figure 2 shows an example of the luminance response curve for one of the CRT monitors evaluated in the study. Note the absence of the step-like features in the luminance response curve. Unlike the AMLCD flat-panel monitor, all CRT monitors evaluated in this study have relatively smooth luminance response curves. The discontinuities in the AMLCD monitor’s luminance response curve result in troughs and spikes in the gradient of luminance response curve. At the pixel values where some of the troughs occur, the contrast threshold increases (contrast sensitivity decreases), as depicted in Figure 3a and 3b.
Figure 1.
a. The luminance response curves of the Clinton Electronics D13000 AMLCD flat panel monitor measured at 90 and 45 degrees to the surface of the monitor. b. The close-up view of the luminance response curves in Figure 1a. Note the “steps” on the curves. c. The gradient of luminance response curves for the flat panel monitor. Note the spikes and troughs in the gradient of luminance response curves.
Figure 2.
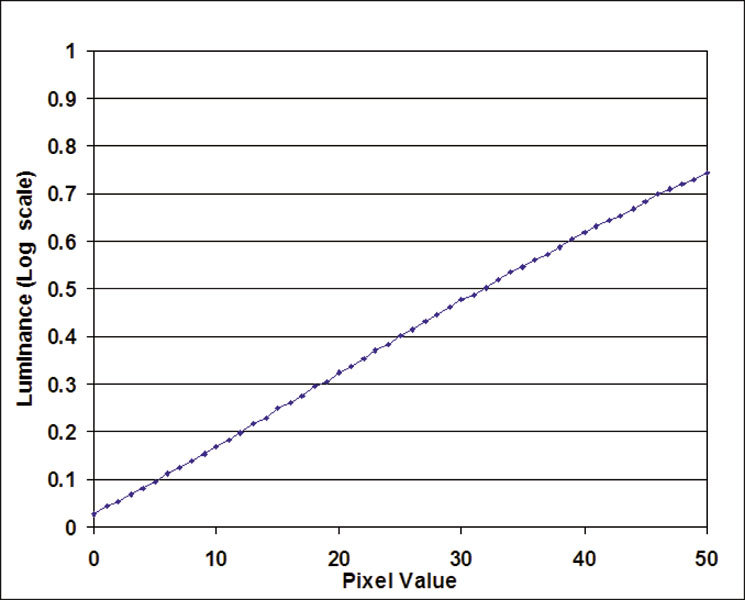
The luminance response curve for one of the CRT monitors evaluated in the study. Note the absence of the “step-like” features in Figure 1a and 1b.
Figure 3.
a. The contrast threshold and gradient of luminance response curve for the AMLCD flat panel monitor. b. Close-up view of Figure 3a. Note that every time the gradient is less than 0.01, the contrast threshold is larger than the minimum, 1 pixel level.
In Figure 3a, the contrast thresholds of one observer using the AMLCD monitor and the gradient of luminance response curve is shown for the entire 8-bit pixel values (from 0 to 255). The gradient is re-scaled (multiplied by 100) in order to over-plot the contrast threshold on the same graph. Figure 3b shows the close-up view of figure 3a (for pixel value range from 1 to 50). It clearly shows that contrast thresholds of this flat-panel monitor are correlated to the gradient of the luminance response curve. When the value of the gradient decreases to below 0.01 at some pixel values, the contrast threshold increases (i.e., contrast sensitivity decreases) to above 1 pixel value. In other words, at these particular pixel values where the gradient decreases below 0.01, a low-contrast structure with only 1 pixel value contrast difference from its background may be invisible to the observer; potentially resulting in missed subtle objects and structures in clinical images.
The CRT Monitors
For all the CRT monitors evaluated in this study, contrast thresholds showed a complex dependency on target object size, background luminance level, and graphics card gamma setting. Figure 4 shows an example of such complexity. Figure 4a-e shows the contrast thresholds as a function of object size for one monochrome CRT monitor (Image System M21Max CRT monitor) at various background luminance levels and graphics card gamma settings. The five frames of Figure 4 are often referred as the “contrast-detail curves.” In general the contrast threshold decreases as the object size increases, which means that a larger object is easier to detect. The contrast threshold reaches a minimum once the object reaches a certain size where the contrast threshold becomes almost independent of object size.
Figure 4.
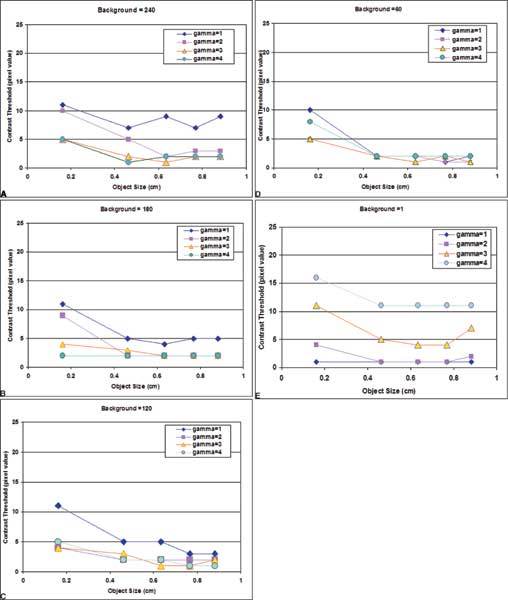
The contrast-detail curves (a-e) of the Image System M21Max CRT monitor at various background luminance levels and effect of gamma settings.
Changing the gamma settings on the graphics card will change the shape of the luminance response curve, consequently resulting in changes in contrast sensitivity. Historically the gamma is defined for the monitor, which relates the input analog video voltage to the output luminance. Nowadays there are high-quality CRT-based displays for primary reading that also provide gamma correction from the factory. In our experiments, however, the gamma setting on the graphics card can be modified. Changing the gamma settings changes the shape of the LUT on the graphics card. To study the effect of various gamma settings on contrast sensitivity, we measured the contrast threshold at several gamma values.
In Figure 5, the contrast thresholds of a small object (0.46 cm in diameter) for different graphics card gamma settings are shown for the Image Systems M21HBMax monochrome CRT monitor. Note that changing gamma affects the contrast threshold differently at different background levels. Larger gamma settings tend to result in lower contrast threshold at higher pixel values, whereas lower gamma settings tend to result in lower contrast threshold at lower pixel values. In Figure 5, a gamma setting of 2 gives a lower contrast threshold for a broader range of background pixel values.
Figure 5.
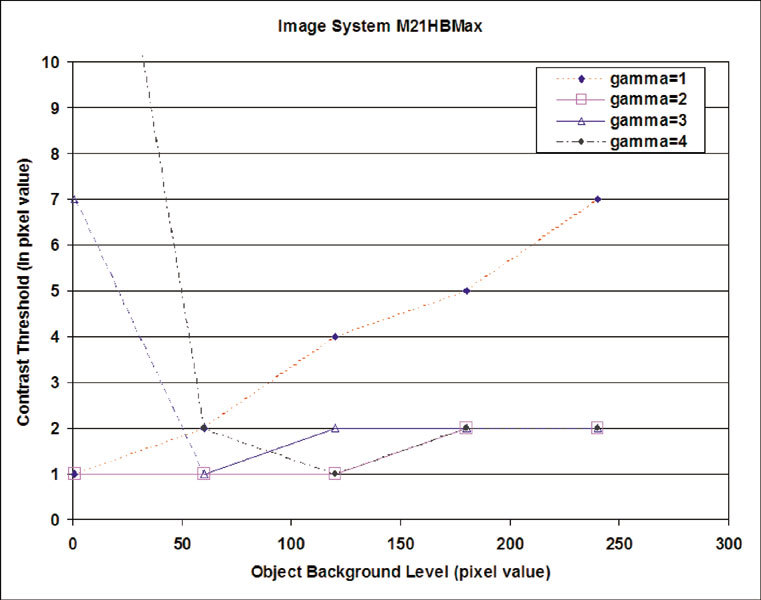
The effect of changing gamma card settings on the measured contrast threshold.
Figure 6 shows the contrast thresholds of one observer over the entire luminance range on a CRT monitor (ViewSonic GA771) with three different graphics card settings. The solid line represents the gradient of luminance response curve, and the dots indicate the measured contrast thresholds. Figure 6a-c clearly shows that when the gradient of the luminance response curve decreases the contrast sensitivity also decreases (i.e., the contrast threshold increases). It is also apparent from Figure 6 that a larger gamma on the graphics card, with a higher gradient at higher luminance values, results in a contrast sensitivity shifted toward higher luminance.
Figure 6.
The contrast threshold plots as a function of the luminance level for a graphics card gamma setting of 1.50 (a) and 2.20 (b) and 3.0 (c). Over-plotted is the gradient of the corresponding luminance response curve.
Intra- and Inter-Observer Variance of the Contrast Threshold Measurement
To find the intra- and inter-observer variance of the contrast threshold measurements, contrast threshold was measured three times by a group of seven observers. It was found that the intra-observer repeatability in measured contrast threshold at various luminance levels and object sizes was within 1 pixel value. Inter-observer repeatability measured by the standard deviation of the averaged contrast threshold at various luminance levels and object sizes was found to be within 0.5.
The Correlation between the Contrast Threshold and the Gradient of Luminance Response Curve
Contrast thresholds measured at various background levels are plotted versus the corresponding gradient values in Figure 7a and 7b. In Figure 7a, the contrast thresholds of a CRT monitor (ViewSonic GA771) for one observer are shown with three different graphics card gamma settings. There are 250 data points on the graph for each gamma setting, so that there are total of 750 data points on Figure 7a. Figure 7b shows the contrast thresholds of two observers for the Clinton DL3000 AMLCD flat-panel monitor with identical graphics card settings, and there are 250 data points for each observer on the graph. Note that when the gradient value is larger than a cutoff value (approximately 0.035 in Figure 7a and b), all the measured contrast thresholds become 1 pixel value. Because of the digital nature of SD systems, the best achievable contrast threshold is 1 pixel value. In other words, if the contrast threshold is 1 pixel value at all input digital values for an SD system, then this display system is capable of displaying all the inherent contrast information. Figure 7 also implies that, fully display the inherent contrast information in a digital image, the gradient of the luminance response curve must be high enough to ensure that it exceeds the cut-off value at all input pixel values.
Figure 7.
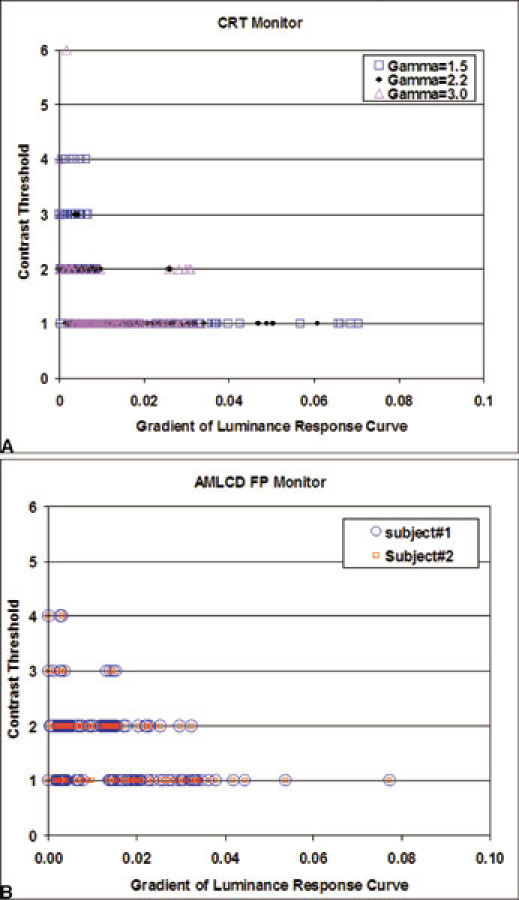
Contrast threshold versus gradient plot for a CRT monitor (Figure 3) and for an AMLCD monitor (Fig 6). Both a and b show that as the gradient increases, the contrast threshold decreases. Also note that when the value of the gradient is larger than 0.03 almost all the measured contrast thresholds become 1 pixel value, which is the best achievable. In other words, the observer can resolve a low-contrast object with minimum contrast (1 pixel value) in a uniform background.
Effect of Viewing Conditions on the Gradient of Luminance Response Curve
It is well known that room light affects the displayed image quality in SD system, especially for the darker areas on a radiographic image. Figure 8 shows the effect of room light on the gradient of luminance response curve, and it clearly demonstrates the reduction of gradient at the lower pixel values while the reduction at higher pixel values are minimal. This reduction in gradient of luminance response curve at lower pixel values explains the reduction of contrast sensitivity at the darker regions on a radiographic image under poor viewing conditions.
Figure 8.
Effect of room light on the gradient of luminance response curve.
DISCUSSION
The experimental results have shown that contrast sensitivity for an SD system is a complex function of multiple variables including monitor characteristics, the configurations of the graphics card, and the viewing conditions. At first glance, it seemed almost impossible to compare monitors’ overall quality because some monitors have better performance at lower luminance levels and others may have better performance at higher luminance levels. In addition, monitor brightness also affects the contrast sensitivity in a complex manner. However, further analysis of the contrast threshold data showed a general correlation between the contrast sensitivity and the measured gradient of luminance response curve. Because of this correlation between the gradient of luminance response curve and the human observer’s contrast sensitivity, and because of the fact that the gradient of luminance response curve of the SD systems is very similar to the H&D curve for the film-screen, or the hardcopy display system, it seems natural and logical to use the gradient of luminance response curve as a quality-index to compare the contrast sensitivity of SD systems. To further illustrate the similarity and differences, Figure 9 and Figure 10 depict schematically the processes from image acquisition to image display in a film-screen system and a digital imaging system.
Figure 9.
The process from image acquisition to display for a film-screen (hard copy display) system.
Figure 10.
The process from image acquisition to image display in a digital system.
Although there are similarities and differences between the hard copy (film/lightbox) display system and the SD system, fundamentally, both display systems present a distribution of luminance pattern, i.e. the image, to a human observer, although the steps involved in achieving that goal differ. In hard copy display the image acquisition and display devices are the same medium, i.e., the film. In the hard copy system, the x-ray exposure (usually measured in relative log scale) is converted to shade of darkness on a film following the H&D curve in a nonlinear fashion (Fig. 9). When the film is displayed on a lightbox, the shades of darkness on the film block the light from the lightbox, and forms a distribution of luminance, i.e., an image. The higher the x-ray exposure, the darker the film gets, and the less light passes through the film. Once the film is exposed and processed, there is little one can do to change the relative distribution of shades of darkness on it. The only thing one can change is the lightbox luminance level, which will change the absolute luminance levels reaching the eyes, but not the relative distribution of luminance intensity. To separate the effect of the lightbox luminance level from that of the “image” itself on the film, optical density (OD) was defined as the log of the ratio of the amount of light transmitted through the film. To obtain the luminance distribution of an image on a lightbox, one can calculate the transmitted luminance level from the optical density distribution on the film and the luminance level of the lightbox (assuming the lightbox has a uniform luminance distribution). As depicted in Figure 9, to obtain luminance distribution of an image on a film, one can calculate I1 by using the equation, D1 =log (IB/I1), where D1 is the optical density and IB is the luminance level of the lightbox. Following the same formula, one can calculate the contrast between the object (I0) and its background (I1).
A better film-screen system is the one that gives relatively larger luminance difference for the same amount of exposure difference over a broader range of x-ray exposures, i.e., a film-screen system that has higher value in Δ(log(luminance))/Δ(exposure) will be a better system. Since log(luminance) is proportional to the optical density, therefore the gradient of H&D curve, Δ(OD)/Δ(exposure) can be used as a quality-index for the film-screen system. It has been used to compare the overall film-screen system quality and as a guide to the proper radiation exposure level for good quality radiographic images. To compare the quality of screen-film systems, one can simply compare the gradient curves. A system with higher gradient values over the desired optical density range will offer optimal contrast and thus is a better system. The gradient curve has been used as the quality index for the “hard copy displays” for many years.
In digital imaging, however, image acquisition and image displaying processes are separated, and this has provided the opportunities for better image quality and tremendous flexibilities in the image display. Figure 10 depicts the entire process of digital imaging, from image acquisition to image display. In digital imaging, the x-ray exposure is converted to pixel values (P1 and P0 in Figure 10), which are represented by integers in an image matrix. These pixel values can be (and usually are) processed according to the specific needs of contrast and spatial enhancement of the image (P1′and P0′ in Figure 10). Then these processed pixels are re-scaled to digital driving levels, which are converted into various levels of output video voltages on the graphics card (V1 and V0). Finally, on the monitor, these video voltages are converted into various luminance levels (I1 and I0), which form a pattern of luminance distribution, the image which human observers can see.
Although the flexibilities introduced by digital data processing can enhance the contrast and the spatial resolution in digital image data, image displaying is still a critical part of the entire process. For instance, one can have a superb image-processing algorithm, but if the display system cannot fully display the inherent image contrasts, then all the processing will have little effect on the image quality “perceived” by the observer. More importantly, because of the nonlinear nature of the monitor luminance output to its video voltage input, it is necessary to consider the SD as a whole system and to ensure that the display system itself does not suppress any inherent contrasts one wants to enhance. In general, a better SD system should have relatively higher contrast in luminance at a broader range of input pixel value, given the same difference contrast in pixel value (P1′ and P0′). In other words, given the same input pixel value difference in a digital image, a better SD system should give relatively larger differences in luminance levels (I1 and I0) for a broader range of input pixel values. Naturally, Δ(log(luminance))/Δ(P′) can be used as a measure of the quality of a display system. An SD system with higher value in Δ(log(luminance))/Δ(P′) over a broader range of input pixel values is a better display system. Since log(luminance) versus P′ plot is defined as the luminance response curve, Δ(log(luminance))/Δ(P′) is simply the gradient of the luminance response curve of an SD system.
Therefore, this proposed quality-index, the gradient of luminance response curve, is similar to the gradient of H&D curve for the film-screen system. The only difference is that in digital imaging there is the added layer of digitization process, which converts x-ray exposure to digital pixel values. For most digital radiographic systems, the relationship between the log of x-ray exposure levels to the pixel values (P1 and P0 in Figure 10) is actually linear. Because of this linearity, in the digital data processing step (from P1 and P0 to P1′ and P0′ in Figure 10) a non-linear conversion is applied in order to give a familiar “film-look” to the observers.
By studying the gradient of the luminance response curve for an SD system, one can compare and predict the contrast sensitivity performance of an average observer using this SD. For instance in Figure 8, the luminance response curves with room lights on and off were measured using a telescopic luminance meter which took into account the combined effects of room lights and reflection off the surface of the monitor. The reduction in the gradient of luminance response curve at the lower luminance range indicates an expected decrease in contrast sensitivity in darker image regions under poor viewing conditions (room light on) while the decrease in the brighter region of image will be minimal. The reduction in luminance response curve gradient is effectively caused by reflection of room light from the monitor’s glass surface, which results in decreased contrast sensitivity. Ideally, to take into account the effects of actual viewing conditions, gradient of luminance response curves should be measured with a telescopic luminance meter in the actual ambient environment of an SD system’s usage to assess the “effective luminance response curve.” On the other hand, the inherent contrast resolution characteristic of an SD system should be measured with a near-focus (a shaded luminance meter with a suction cup) right on the surface of the monitor.
Unlike the film-screen systems, digital imaging enables the separation of image acquisition and image display. Thus, radiographic images can be preprocessed optimally according to the exam type and body part being imaged. For instance, the optimal processing algorithms for the digital radiograph of AP chest and of extremities are different. Furthermore, because of the adjustability of contrast by the SD system, object contrast can be modified on the fly as needed during image viewing. However, the SD system should also be optimized such that it does not suppress any of the inherent contrast information of the postprocessed images. In other words, ideally there should be no loss of information in the image displaying process. One simple way to ensure that the SD system does not suppress any inherent contrast information in a digital image is to ensure that an average user can resolve an object in a uniform background. But this requirement may be over-stringent because, for clinical images, because of the human eye’s dynamic adaptation to the luminance variations and complex background in clinical images, the contrast sensitivity of the human visual system will be much lower than that measured from the images with uniform background. Unfortunately, contrast sensitivity data for clinical images are difficult to obtain. More research using clinical images is needed.
The general relationship between the contrast sensitivity of human observer and the gradient of luminance response curve demonstrated in this study may also have further implications such as in the calculation of the minimum requirement for the luminance contrast ratio of an SD system. Contrast threshold data show that when the gradient of luminance response curve is greater than a cut-off value, the average human observer can resolve an object that only has one pixel value contrast difference from its uniform background. One implication is that, to fully display all the inherent contrast information in a digital image, the gradient should be sufficient to ensure that the luminance difference between adjacent pixel values exceeds the contrast threshold of an average observer. Based on such an assumption, one can estimate the required monitor luminance ratio (Lmax/Lmin) to fully display all the inherent contrast of a digital image simultaneously. However, we also realize that clinical images are quite different from a simple circular object in a uniform background, and the critical value in contrast threshold for clinical images may be different.22,23 In fact, studies have suggested that if the gradient of luminance response is too high, contouring artifacts may occur.22,23 Therefore, there may be an optimal value for the gradient of the luminance response curve for the SD system. Further studies using clinical images are needed to find the contrast sensitivity requirements for an SD system.
Monitor performance deteriorates over time and graphics card settings may change.25,26,27 Therefore quality assurance and quality control of an SD system should be a vital part of the clinical operation in PACS.27,28,29,30,31,32,33,34,35,36 Committees of ACR/NEMA Spell out ACR/NEMA DICOM have been trying to address the display quality standard issues since DICOM’s inception. It has established a standard luminance response curve, based on previous psychophysical research results.24 To provide guidance and to standardize the technique for routine quality assurance and quality assessment of an SD system, the American Association of Physicists in Medicine has established a task group (TG18). It has published a report, which specifically addresses the quality control and quality assurance issues for medical image displays.27 The report discusses the important factors in SD systems such as the luminance level, the spatial and contrast resolution, the uniformity, and the monitor glare, among other features. The report also includes several test patterns, which can be used to quickly assess the overall quality of a display device. Detailed descriptions of the methods and tools to access the particular characteristics of an SD device are also presented.
CONCLUSIONS
The AMLCD flat-panel monitor based on current technology still has some problems and issues that need to be resolved, such as the discontinuity in luminance response curve. The contrast sensitivity of an SD system is a complex function of monitor characteristics and graphics card configuration as well as viewing conditions. It can be measured with good repeatability and accuracy. The contrast sensitivity of the human observer correlates well with the gradient of the luminance response curve. Thus the overall quality of an SD system can be assessed using the gradient curve of the luminance response curve. Gradient of luminance response curve can be used as a quality-index for SD systems. The luminance response curve should be measured under real viewing conditions, and at the actual location of the SD system usage so that the effects of viewing condition on SD quality can also be taken into account.
Acknowledgements
The authors thank Drs. Jon Anderson, Tim Blackburn, and Gary Arbique for their insightful comments and suggestions in preparing this manuscript, and Ms. J Xu for her help in part of the experiment.
References
- 1.Wang J, Langer S. A brief review of human perception factors in Digital Display for PACS. J Digit Imaging. 1997;10:158–168. doi: 10.1007/BF03168838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Krupinski EA, Roehrig H. Influence of monitor luminance and tone scale on observers’ search and dwell patterns. Proc SPIE. 1999;3663:151–156. doi: 10.1117/12.349636. [DOI] [Google Scholar]
- 3.Carrino JA. “Image Quality: a clinical perspective” In: Siegel E, Reiner BI, and Carrino J, editors. SCAR University Primer 3: Quality Assurance in the Digital Medical Enterprise. Society for Computer Applications in Radiology; 2002.
- 4.Carrino JA. “Image Quality: a clinical perspective” In: Siegel E, Reiner BI, and Carrino J, editors. SCAR University Primer 3: Quality Assurance in the Digital Medical Enterprise. Society for Computer Applications in Radiology; 2002.
- 5.Roehrig H, Blume H, Ji TL, et al. Performance tests and quality control of cathode ray tube displays. J Digit Imaging. 1990;3:134–45. doi: 10.1007/BF03167599. [DOI] [PubMed] [Google Scholar]
- 6.Blume H, Roehrig H, Brown M, et al. Comparison of the physical performance of high resolution CRT displays and films recorded by laser image printers and displayed on light-boxes and the need for a display standard. Proc SPIE. 1990;1232:97–114. [Google Scholar]
- 7.Horii SC. Quality assurance for picture archiving and communication systems (PACS) and PACS technology applications in radiology. J Digit Imaging. 1995;8:1–2. doi: 10.1007/BF03168049. [DOI] [PubMed] [Google Scholar]
- 8.Roehrig H, Krupinski E. Image quality of CRT displays and the effect of brightness on diagnosis of mammograms. J Digit Imaging. 1998;11(Suppl 1):187–188. doi: 10.1007/BF03168300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Arenson RL, Chakraborty D, Seshadri SB, et al. The digital imaging workstation. Radiology. 1990;176:303–315. doi: 10.1148/radiology.176.2.2367643. [DOI] [PubMed] [Google Scholar]
- 10.Dwyer SJ, Stewart BK, Sayre JW, et al. Performance characteristics and image fidelity of gray-scale monitors. Radiographics. 1992;12:765–772. doi: 10.1148/radiographics.12.4.1636038. [DOI] [PubMed] [Google Scholar]
- 11.Roehrig H, Willis CE, Damento MA. Characterization of monochrome CRT display systems in the field. J Digit Imaging. 1999;12:152–165. doi: 10.1007/BF03168851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Blume H, Hemminger BM. Image presentation in digital radiology: perspectives on the emerging DICOM display function standard and its application. Radiographics. 1997;17:769–777. doi: 10.1148/radiographics.17.3.9153711. [DOI] [PubMed] [Google Scholar]
- 13.Muka E, Mertelmeier T, Slone R, et al. Impact of phosphor luminance noise on the specification of high-resolution CRT displays for medical imaging. Proc SPIE. 1997;3031:210–221. [Google Scholar]
- 14.Pilgram TK, Slone RM, Muka E, et al. Perceived fidelity of compressed and reconstructed radiological images: a preliminary exploration of compression, luminance, and viewing distance. J Digit Imaging. 1998;11:168–175. doi: 10.1007/BF03178079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Langer S, Wang J. User and system interface issues in the purchase of imaging and information systems. J Digit Imaging. 1996;9:113. doi: 10.1007/BF03168605. [DOI] [PubMed] [Google Scholar]
- 16.Dwyer S: Soft copy displays and digitizers. In Frey G Sprawls P (eds) Proceedings of 1997 AAPM Summer School on Expanding Role of Medical Physics in Diagnostic Imaging AAPM 1997, Medical Physics Publishing, Madison, WI, 381
- 17.Cook LT, Cox GG, Insana MF, et al. Comparison of a cathode-ray-tube and film for display of computed radiographic images. Med Phys. 1998;25(7 Pt1):1132–1138. doi: 10.1118/1.598304. [DOI] [PubMed] [Google Scholar]
- 18.Wang J, Stetson C: Characteristic evaluations of medical image displays using contrast-detail curve measurements. Society for Information Display International Symposium, SID Digest 172-175, 2000
- 19.Wang J, Anderson J, Lane L, et al. Contrast-detail characteristic evaluations of several displays devices. J Digit Imaging. 2000;13(Suppl l):. doi: 10.1007/BF03167651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Langer S, Wang J. An evaluation of ten digital image review workstations. J Digit Imaging. 1997;10:65. doi: 10.1007/BF03168558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wang J, Peng Q. An interactive method of assessing the characteristics of softcopy display using observer performance tests. Proc SPIE. 2002;4686:189–197. doi: 10.1117/12.462677. [DOI] [PubMed] [Google Scholar]
- 22.Muka E, Whiting BR. On the human visual system intrascene luminance dynamic range. Proc SPIE. 2002;4686:169. doi: 10.1117/12.462676. [DOI] [Google Scholar]
- 23.Muka E, Reiker G. Reconsidering bit depth for radiological images—is eight enough? Proc SPIE. 2002;4686:177. doi: 10.1117/12.462675. [DOI] [Google Scholar]
- 24.Hemminger BM, Johnston RE, Rolland JP, et al. Introduction to perceptual linearization of video display systems for medical image presentation. J Digit Imaging. 1995;8:21–34. doi: 10.1007/BF03168052. [DOI] [PubMed] [Google Scholar]
- 25.Flynn MJ, Badano A. Image quality degradation by light scattering in display devices. J Digit Imaging. 1999;12:50–59. doi: 10.1007/BF03168843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Badano A, Flynn MJ. Image degradation by glare in radiologic display devices. Proc SPIE: Int Soc Optical Eng. 1997;3031:222–231. [Google Scholar]
- 27.Samei E, Badano A, Chakraborty D, et al: Assessment of Display Performance for Medical Imaging Systems. Draft Report of the American Association of Physicists in Medicine (AAPM) Task Group 18, Version 9.0, October 2002
- 28.Wang J: Computer monitor QC issues. Categorical Course at SCAR annual conference, 2001
- 29.Weibrecht M, Spekowius G, Quadflieg P, et al. Image quality assessment of monochrome monitors for medical soft copy display. Proc SPIE. 1997;3031:232–244. [Google Scholar]
- 30.Roehrig H. Image quality assurance for CRT display systems. J Digit Imaging. 1999;12:1–2. doi: 10.1007/BF03168620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Roehrig H. Image quality assurance for CRT display systems—Part II. J Digit Imaging. 1999;12:49. doi: 10.1007/BF03168842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hangiandreou NJ, Fetterly KA, Bernatz SN, et al. Quantitative evaluation of overall electronic display quality. J Digit Imaging. 1998;11(Suppl 1):180–186. doi: 10.1007/BF03168299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Weiser JC, Drummond KT, Evans BD, et al. Quality assurance for digital imaging. J Digit Imaging. 1997;10:7–8. doi: 10.1007/BF03168639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hangiandreou NJ, Fetterly KA, Felmlee JP. Optimization of a contrast-detail-based method for electronic image display quality evaluation. J Digit Imaging. 1999;12:60–67. doi: 10.1007/BF03168844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Reiker GG, Gohel N, Muka E, et al. Quality monitoring of soft-copy displays for medical radiography. J Digit Imaging. 1992;5:161–167. doi: 10.1007/BF03167765. [DOI] [PubMed] [Google Scholar]
- 36.Wang J. A Quality Index for the quality of softcopy display in PACS. Med Phys. 2002;29:1219. [Google Scholar]