

Abstract
Purpose
Pressure algometry is widely used to obtain measures of mechanical pain sensitivity in adults, both in experimental and clinical pain conditions. Only very few studies describe the use of pressure algometry in children. The purpose of this study was to produce reference values of pressure pain thresholds and to determine the intra- and interrater agreement, in order to introduce pressure algometry as a standardized method for the assessment of pain thresholds in children with orthopedic disorders.
Methods
Pressure pain thresholds were determined at the leg and at the thenar in 50 children aged 4–12 years. All were scheduled for physical examination at the outpatient Orthopedic Clinic at Aarhus University Hospital, Denmark, because of various orthopedic disorders such as clubfoot and Baker’s cyst. Pressure pain thresholds were determined by two different raters: 20 children were examined twice by rater 1 (intrarater agreement), and another 20 children were examined by both rater 1 and rater 2 (interrater agreement). An additional ten children were examined once by rater 1 to increase the number of children used to determine the reference values.
Results
The pressure pain threshold was 183.1 kPa (mean, SD: 90.7) at the leg and 179.1 kPa (mean, SD: 97.4 kPa) at the thenar (n = 50). Pressure pain thresholds were similar in boys (n = 27) and girls (n = 23). Also, pressure pain thresholds were not affected by age. Bland–Altman plots showed excellent intrarater agreement and satisfactory interrater agreement.
Conclusion
Pressure algometry has excellent intrarater agreement and satisfactory interrater agreement. Pressure algometry was well-tolerated even by very young children. The method deserves more widespread use both in clinical and experimental settings.
Keywords: Pressure algometry, Pressure pain thresholds, Reliability, Children
Introduction
Pressure algometry has proven to be an important psychophysical examination tool to obtain measures of mechanical pain sensitivity from deep tissue. It has been widely used in adults, both in experimental and clinical pain conditions [1]. In, for example, osteoarthritis, fibromyalgia, temporomandibular disorders, and whiplash syndrome, reduced pressure pain thresholds to mechanical pressure have been shown, indicating the presence of hyperexcitability [2–5].
However, only a few studies of pressure algometry have been conducted in children [6–11]. Haskes et al. [6] found that 44 children aged 4–12 years with growing pains had lower pain thresholds at several predefined points than 46 control children without growing pains. The same population of children was examined after 5 years. Pressure pain thresholds were still significantly lower in children with continuing growing pains than in controls and children with resolved growing pains [7]. Furthermore, pressure pain thresholds were significantly lower over the trigeminal and nontrigeminal nerves in children with tension-type headache than in healthy controls [8]. Hogeweg et al. [9] studied the effect of site of stimulation and age and gender on pain thresholds in 69 children aged 6 to 17 years. Pressure pain thresholds were slightly lower paraspinally than at the extremities. Pressure pain thresholds measured paraspinally increased with age, but thresholds measured at the extremities did not increase with age. Pressure pain thresholds were not affected by gender.
Numerous studies in adults have documented intra- and interrater agreement of pressure pain thresholds [12–15]. However, intra- and interrater agreement of pressure pain thresholds in children has only been examined by Chaves et al. [10]. Pain thresholds were measured in 30 children aged 7–12 years by two trained examiners. Fourteen children had orofacial pain and 16 were free of symptoms. Intra- and interrater agreement was found to be moderate or excellent for most of the masticatory structures examined.
Orthopedic pain conditions are frequent in children. We therefore wanted to produce reference values for pressure pain thresholds in children with orthopedic disorders and to determine the intra- and interrater agreement, in order to introduce pressure algometry as a standardized method for the assessment of pain thresholds in both clinical and experimental settings.
Materials and methods
Subjects
Fifty children aged 4–12 years were consecutively included in the study. All children underwent physical examination at the outpatient Orthopedic Clinic at Aarhus University Hospital, Denmark, because of orthopedic disorders, e.g., club foot, flat foot, knock knee, short Achilles tendon, and Baker’s cyst. Children with cerebral palsy, other severe systemic disease, or pain at rest were excluded from participation. Information about the study was sent to the parents of eligible children before the visit to the Orthopedic Clinic, and informed written consent was obtained before inclusion. Clinical data including age, sex, ethnicity, weight, height, and orthopedic disease were collected. The study was approved by the local ethics committee (2007-21171) and the Danish Data Protection Agency.
Pressure algometry
Pressure pain thresholds were determined using a hand-held electronic pressure algometer with a 1 cm2 probe area and an application rate of 20 kPa/s (Algometer®, Somedic Sales, Hörby, Sweden). The pressure algometer consists of a ‘pistol’ handle and a rod with a pressure-sensitive gauge strain at the tip (Fig. 1). The children were instructed to say “stop” as soon as the sensation of a pressure changed to a sensation of pain. The applied pressure could be read on a digital display. Three values were obtained at each of the two sites. The pain threshold was determined as an average of the last two values, as this procedure has been found to be reliable in both children and adults [10, 16].
Fig. 1.

A hand-held pressure algometer. (Algometer®, Somedic Sales, Hörby, Sweden). The pressure algometer consists of a ‘pistol’ handle and a rod with a pressure-sensitive gauge strain at the tip. The applied pressure can be read on a digital display
Procedure
Pressure algometry was performed on the same day as the physical examination under quiet and non-stressful conditions. The children were examined in a relaxed sitting position, and carefully introduced to the procedure. For the youngest children, a teddy bear was used for demonstration. To determine the intrarater agreement, 20 children were examined twice by rater 1 (ADK). To determine the interrater agreement, another 20 children were examined by both rater 1 and rater 2 (LN) in a randomized order (in ten children the first examination was done by rater 1, and in another ten children the first examination was done by rater 2). An additional ten children were examined once by rater 1 to increase the number of children used to determine the reference values from 40 to 50 children.
The time elapsed between the first and second examination ranged from 15 to 30 min. Rater 1 and rater 2 were both trained users of pressure algometry. Two sites were chosen for evaluation, and examined in the following order: (1) the lateral aspect of the calf on the affected side above the gastrocnemius muscle and approximately where the upper 1/3 of the lower leg meets the lower 2/3 of the lower leg (if both legs were affected, the leg ipsilateral to the dominant hand was examined), and (2) the thenar of the dominant hand.
Statistics
Descriptive statistics was used for demographic data. An analysis described by Bland and Altman [17] was performed, in which intra- and interrater differences between two measurements were plotted against the corresponding mean. The differences were tested for normal distribution using probability plots and histograms. A paired t-test was used to test intra- and interrater differences in pressure pain thresholds. An unpaired t-test was used to test if sex, age, or site of stimulation affected pressure pain thresholds. Results are presented as mean (SD). The Number Cruncher Statistical System (NCSS) (2004) statistical software package was used.
Results
Seventy-seven children were asked to participate, and 27 refused. Pressure algometry was well-tolerated by all 50 included children, and none withdrew during the examination. The baseline characteristics can be seen in Table 1. The pressure pain threshold was 183.1 (90.7) kPa at the leg and 179.1 (97.4) kPa at the thenar (n = 50, all examinations done by rater 1). Pressure pain thresholds were similar in younger (4–7 years, n = 18) and older children (8–12 years, n = 32) [leg: 156.5 (87.1) kPa vs 191.8 (101.9) kPa, P = 0.22; thenar: 180.6 (89.5) kPa vs 184.5 (92.8) kPa, P = 0.89](Fig. 2). Pressure pain thresholds were similar in boys (n = 27) and girls (n = 23) [leg: 195.5 (114.2) kPa vs 159.8 (70.7) kPa, P = 0.18; thenar: 197.9 (92.6) kPa vs 165.6 (87.3) kPa, P = 0.21]. Bland–Altman plots showed excellent intrarater agreement (Figs. 3a, b) and satisfactory interrater agreement between the two raters (Figs. 4a, b). Pressure pain thresholds were statistically significantly higher both at the leg [difference: 41.4 (57.5) kPa, P < 0.01] and at the thenar [difference: 29.4 (42.7) kPa, P < 0.01] for thresholds obtained by rater 1 compared with thresholds obtained by rater 2.
Table 1.
Baseline characteristics of 50 children with orthopedic disorders
| Gender (n, %) | |
| Male | 27 (54) |
| Female | 23 (46) |
| Age, years, mean ± SD | |
| Male | 8.0 ± 2.4 |
| Female | 8.5 ± 2.3 |
| Ethnicity (n, %) | |
| Caucasian | 47 (94) |
| Other | 3 (6) |
| Height, cm, mean ± SD | |
| Male | 134.8 ± 14.6 |
| Female | 134.8 ± 15.2 |
| Weight, kg, mean ± SD | |
| Male | 29.9 ± 8.5 |
| Female | 30.6 ± 8.1 |
| Dominant hand (n, %) | |
| Right | 46 (92) |
| Left | 4 (8) |
| Orthopedic disorder (n, %) | |
| Bones | 18 (36) |
| Joints | 3 (6) |
| Connective tissue | 22 (44) |
| Unspecific | 7 (14) |
| Purpose of visit (n, %) | |
| Follow-up after surgery | 16 (32) |
| Planned surgery | 10 (20) |
| Consultation | 24 (48) |
Fig. 2.
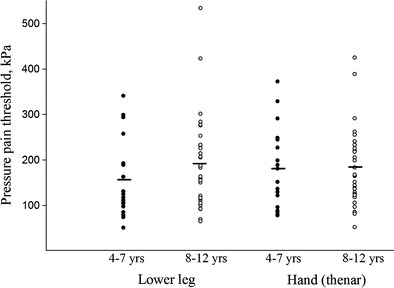
Pressure pain thresholds. Each dot represents a child. Pressure pain thresholds were similar in younger (4–7 years, n = 18) and older children (8–12 years, n = 32) [leg: 156.5 (87.1) kPa vs 191.8 (101.9) kPa, P = 0.22; thenar: 180.6 (89.5) kPa vs 184.5 (92.8) kPa, P = 0.89] [mean, (SD)]
Fig. 3.
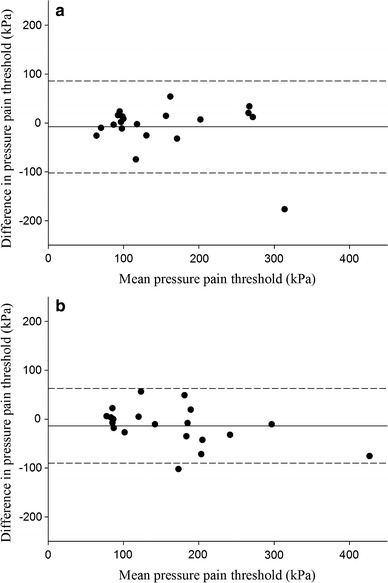
Intrarater agreement for pressure pain threshold at the lower leg and at the thenar in 20 children. Bland–Altman plot. Each dot represents the difference between two measurements plotted against the mean of the two measurements. Both measurements were obtained in the same child by rater 1. a Lower leg. The horizontal line (−7.85 kPa) represents the mean value of the difference for 20 children, and the upper (86.4 kPa) and lower (−102.1) limits of agreements are shown as dotted lines; SD: 48.1 ± 1.96. b Thenar. The horizontal line (−13.9 kPa) represents the mean value of the difference for 20 children, and the upper (63.1 kPa) and lower (−90.9 kPa) limits of agreements are shown as dotted lines; SD: 39.3 ± 1.96
Fig. 4.
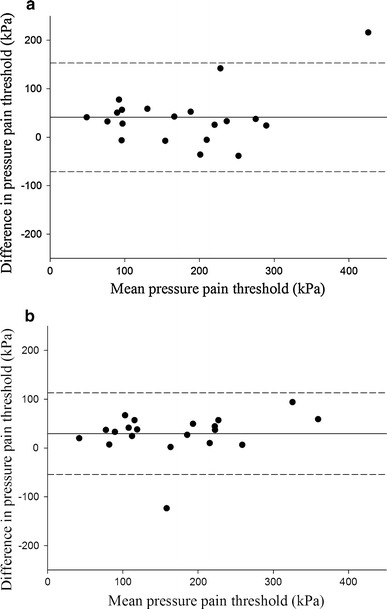
Interrater agreement for pressure pain threshold at the lower leg and at the thenar in 20 children. Bland–Altman plot. Each dot represents the difference between two measurements plotted against the mean of the two measurements. Both measurements were obtained in the same child by two different raters (rater 1 and rater 2). a Lower leg. The horizontal line (41.2 kPa) represents the mean value of the difference for 20 children, and the upper (153.9 kPa) and lower (−71.5 kPa) limits of agreements are shown as dotted lines; SD: 57.5 ± 1.96. b Thenar. The horizontal line (29.4 kPa) represents the mean value of the difference for 20 children, and the upper (113.1 kPa) and lower (−54.3 kPa) limits of agreements are shown as dotted lines; SD: 42.7 ± 1.96
Discussion
In this study, we found excellent intrarater agreement and satisfactory interrater agreement for pressure pain thresholds obtained at the leg and at the thenar in children aged 4–12 years with orthopedic disorders.
The Bland–Altman plot was used for presentation and analysis of data. Some authors have used the Intraclass Correlation Coefficient (ICC) to show if there is an agreement between raters. However, this method is liable to systemic error, and does not reveal clearly the variation between each pair of repeated measures.
Pressure pain thresholds obtained by rater 1 were statistically significant higher than thresholds obtained by rater 2. This difference may have several explanations. Both raters were trained users of the pressure algometer, and the children were carefully instructed in how and when to respond to the applied pressure. However, a mean interrater difference of 41.2 kPa at the leg and 29.4 kPa at the hand is rather low compared with differences found in other reliability studies using the pressure algometer. Chesterton et al. [15] studied the interrater agreement of pressure pain thresholds obtained at the hand in healthy adults, and accepted an interrater difference of 173.9 kPa before it was categorized as a true difference. Person et al. [18] found interrater differences of 44–71 kPa when examining pressure pain thresholds in shoulder muscles of healthy women. In the study of intra- and interrater agreement in 30 children with and without orofacial pain, the interrater difference in pressure pain thresholds obtained at the thenar in children with pain was 28.2 kPa and these children were older (7–12 years of age) [10]. Although studies on interrater agreement involve trained users of pressure algometry, it is possible that different raters might place the pressure pain algometer in a slightly different area, with a slightly different angle to the skin and with a slightly different application rate.
Rater 1 was a male nurse and rater 2 was a female medical doctor. Studies in adults have shown that experimenter gender and professional status may influence thresholds to pain stimuli [19, 20]. In the study by Kállai et al. [19], 160 healthy volunteers were asked to immerse their hand as long as possible in cold water (−1°C). The volunteers tolerated pain longer when examined by a faculty member compared to when examined by a student. Also, the volunteers expressed higher pain intensity when examined by a female experimenter. We cannot exclude the possibility that gender and educational level may have influenced pressure pain thresholds in the present study. In the study by Chaves et al. [10], no information was provided about gender and educational level of the raters. More studies on how these factors may influence pressure pain thresholds in children are warranted.
The children's sex and age did not significantly affect pressure pain thresholds. Thus, our findings are in accordance with the findings by Hogeweg et al. [9]. A few studies in children suggest that pressure pain thresholds may be affected by site of stimulation [6, 9]. In adults, pressure pain thresholds decrease with age [21], and women exhibit lower thresholds than men [22]. It has been shown that other factors, e.g., the children`s level of anxiety, anticipation and parental catastrophizing, may affect response to pressure pain induced by a pressure algometer [23].
In summary, pressure algometry has excellent intrarater agreement and satisfactory interrater agreement. Pressure algometry was well-tolerated even by very young children. The method deserves more widespread use both in clinical and experimental settings.
Acknowledgments
This work was supported in part by a grant from Agustinus Fonden.
References
- 1.Rolke R, Baron R, Maier C, Tolle TR, Treede RD, Beyer A, Binder A, Birbaumer N, Birklein F, Botefur IC, Braune S, Flor H, Huge V, Klug R, Landwehrmeyer GB, Magerl W, Maihofner C, Rolko C, Schaub C, Scherens A, Sprenger T, Valet M, Wasserka B. Quantitative sensory testing in the German research network on neuropathic pain (DFNS): standardized protocol and reference values. Pain. 2006;123:231–243. doi: 10.1016/j.pain.2006.01.041. [DOI] [PubMed] [Google Scholar]
- 2.Arendt-Nielsen L, Nie H, Laursen MB, Laursen BS, Madeleine P, Simonsen OH, Graven-Nielsen T. Sensitization in patients with painful knee osteoarthritis. Pain. 2010;149:573–581. doi: 10.1016/j.pain.2010.04.003. [DOI] [PubMed] [Google Scholar]
- 3.Kosek E, Ekholm J, Hansson P. Sensory dysfunction in fibromyalgia patients with implications for pathogenic mechanisms. Pain. 1996;68:375–383. doi: 10.1016/S0304-3959(96)03188-0. [DOI] [PubMed] [Google Scholar]
- 4.Baad-Hansen L, Leijon G, Svensson P, List T. Comparison of clinical findings and psychosocial factors in patients with atypical odontalgia and temporomandibular disorders. J Orofac Pain. 2008;22:7–14. [PubMed] [Google Scholar]
- 5.Kasch H, Qerama E, Kongsted A, Bach FW, Bendix T, Jensen TS. Deep muscle pain, tender points and recovery in acute whiplash patients: a 1-year follow-up study. Pain. 2008;140:65–73. doi: 10.1016/j.pain.2008.07.008. [DOI] [PubMed] [Google Scholar]
- 6.Hashkes PJ, Friedland O, Jaber L, Cohen HA, Wolach B, Uziel Y. Decreased pain threshold in children with growing pains. J Rheumatol. 2004;31:610–613. [PubMed] [Google Scholar]
- 7.Uziel Y, Chapnick G, Jaber L, Nemet D, Hashkes PJ. Five-year outcome of children with “growing pains”: correlations with pain threshold. J Pediatr. 2010;156:838–840. doi: 10.1016/j.jpeds.2009.11.078. [DOI] [PubMed] [Google Scholar]
- 8.Fernandez-Mayoralas DM, Fernandez-de-las-Penas C, Ortega-Santiago R, Ambite-Quesada S, Jimenez-Garcia R, Fernandez-Jaen A. Generalized mechanical nerve pain hypersensitivity in children with episodic tension-type headache. Pediatrics. 2010;126:187–194. doi: 10.1542/peds.2010-0012. [DOI] [PubMed] [Google Scholar]
- 9.Hogeweg JA, Kuis W, Oostendorp RA, Helders PJ. The influence of site of stimulation, age, and gender on pain threshold in healthy children. Phys Ther. 1996;76:1331–1339. doi: 10.1093/ptj/76.12.1331. [DOI] [PubMed] [Google Scholar]
- 10.Chaves TC, Nagamine HM, de Sousa LM, de Oliveira AS, Grossi DB. Intra- and interrater agreement of pressure pain threshold for masticatory structures in children reporting orofacial pain related to temporomandibular disorders and symptom-free children. J Orofac Pain. 2007;21:133–142. [PubMed] [Google Scholar]
- 11.Chaves TC, Nagamine HM, de Sousa LM, de Oliveira AS, Grossi DB. Comparison between the reliability levels of manual palpation and pressure pain threshold in children who reported orofacial pain. Manual therapy. 2010;15:508–512. doi: 10.1016/j.math.2010.03.010. [DOI] [PubMed] [Google Scholar]
- 12.Ohrbach R, Gale EN. Pressure pain thresholds, clinical assessment, and differential diagnosis: reliability and validity in patients with myogenic pain. Pain. 1989;39:157–169. doi: 10.1016/0304-3959(89)90003-1. [DOI] [PubMed] [Google Scholar]
- 13.Chung SC, Kim JH, Kim HS. Reliability and validity of the pressure pain thresholds (PPT) in the TMJ capsules by electronic algometer. Cranio. 1993;11:171–176. doi: 10.1080/08869634.1993.11677961. [DOI] [PubMed] [Google Scholar]
- 14.Antonaci F, Sand T, Lucas GA. Pressure algometry in healthy subjects: inter-examiner variability. Scand J Rehabil Med. 1998;30:3–8. doi: 10.1080/003655098444255. [DOI] [PubMed] [Google Scholar]
- 15.Chesterton LS, Sim J, Wright CC, Foster NE, Chesterton LS, Barlas P, Foster NE, Baxter GD, Wright CC. Interrater reliability of algometry in measuring pressure pain thresholds in healthy humans, using multiple raters. Clin J Pain. 2007;23:760–766. doi: 10.1097/AJP.0b013e318154b6ae. [DOI] [PubMed] [Google Scholar]
- 16.Meeus M, Roussel NA, Truijen S, et al. Reduced pressure pain threshold in response to exercise in chronic fatigue syndrome but not in chronic low back pain: An experimental study. J Rehabil Med. 2010;42:884–890. doi: 10.2340/16501977-0595. [DOI] [PubMed] [Google Scholar]
- 17.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–310. doi: 10.1016/S0140-6736(86)90837-8. [DOI] [PubMed] [Google Scholar]
- 18.Persson AL, Brogardh C, Sjolund BH. Tender or not tender: test–retest repeatability of pressure pain thresholds in the trapezius and deltoid muscles of healthy women. J Rehabil Med. 2004;36:17–27. doi: 10.1080/16501970310015218. [DOI] [PubMed] [Google Scholar]
- 19.Kallai I, Barke A, Voss U. The effects of experimenter characteristics on pain reports in women and men. Pain. 2004;112:142–147. doi: 10.1016/j.pain.2004.08.008. [DOI] [PubMed] [Google Scholar]
- 20.Aslaksen PM, Myrbakk IN, Hoifodt RS, Flaten MA. The effect of experimenter gender on autonomic and subjective responses to pain stimuli. Pain. 2007;129:260–268. doi: 10.1016/j.pain.2006.10.011. [DOI] [PubMed] [Google Scholar]
- 21.Lautenbacher S, Kunz M, Strate P, Nielsen J, Arendt-Nielsen L. Age effects on pain thresholds, temporal summation and spatial summation of heat and pressure pain. Pain. 2005;115:410–418. doi: 10.1016/j.pain.2005.03.025. [DOI] [PubMed] [Google Scholar]
- 22.Chesterton LS, Barlas P, Foster NE, Baxter GD, Wright CC. Gender differences in pressure pain threshold in healthy humans. Pain. 2003;101:259–266. doi: 10.1016/S0304-3959(02)00330-5. [DOI] [PubMed] [Google Scholar]
- 23.Goubert L, Vervoort T, Cano A, Crombez G. Catastrophizing about their children`s pain is related to higher parent–child congruency in pain ratings: an experimental investigation. Eur J Pain. 2009;13:196–201. doi: 10.1016/j.ejpain.2008.03.009. [DOI] [PubMed] [Google Scholar]