

Abstract
Successful cardiac surgery requires highly skilled individuals to interact effectively in a variety of complex situations. Although cardiac surgery requires individuals to have the requisite medical knowledge and skills, interpersonal competencies are vital to any successful cardiac surgery. Surgeons, anesthesiologists, perfusionists, nurses and residents must communicate effectively in order to ensure a successful patient outcome. Breakdowns in communication, decision-making or leadership could lead to adverse patient outcomes. Realizing that human error is responsible for many adverse patient outcomes, we attempted to understand the team processes involved in cardiac surgery. An adaptation of the Operating Room Management Attitudes Questionnaire was used to gather a variety of responses related to group decision-making and communication. The results indicate inherent group differences based on factors such as seniority and occupational group membership. The implications of the research findings and suggestions for future research are discussed in detail.
Abstract
Pour assurer le succès d'une chirurgie cardiaque, des personnes hautement qualifiées doivent interagir efficacement dans diverses situations complexes. Même si la chirurgie cardiaque exige des intervenants qu'ils et elles possèdent les connaissances et les compétences médicales nécessaires, leur compétence interpersonnelle jouent un rôle vital dans la réussite de toute chirurgie cardiaque. Chirurgiens, anesthésistes, perfusionnistes, infirmières et résidents doivent communiquer efficacement afin de garantir un résultat heureux pour le patient. Les ruptures des communications, de la prise de décision et du leadership peuvent entraîner des résultats indésirables pour le patient. Sachant que l'erreur humaine est la cause de nombreux résultats indésirables pour les patients, nous avons cherché à comprendre les mécanismes d'équipe qui interviennent dans la chirurgie cardiaque. Nous avons utilisé une version adaptée du questionnaire sur les attitudes de gestion en salle d'opération pour réunir diverses réponses reliées à la prise de décision et à la communication en groupe. Les résultats indiquent des différences inhérentes aux groupes fondées sur des facteurs comme l'ancienneté et l'appartenance à un groupe professionnel. On discute en détail des répercussions des résultats de la recherche et on suggère des recherches futures.
The effectiveness of the Canadian health service is largely dependant upon the behaviour of medical staff. Advances in medical science have increased life expectancy through the development of new treatments and medical procedures for previously incurable diseases. It would seem reasonable to expect that these advances would increase the status of the medical profession, yet health care providers still receive criticism for a variety of reasons, including public concern over medical error. For example, the public inquiry into the case of 12 children in Manitoba who died during or after open-heart surgery concluded that the children did not receive the level of care their parents rightly expected.1 The public inquiry into the Manitoba deaths concluded that we must accept that medical staff do make errors and that specific methods are required to help prevent error from occurring. Further, given that error does occur, strategies to mitigate the consequences of errors are also a necessity.2 In Canada, it is estimated that the adverse event rate is about 7.5 per 100 hospital admissions. More specifically, the Canadian Adverse Events Study suggests that annually 185 000 hospital visits are associated with an adverse event or outcome.3 An adverse event, according to the Canadian Patient Safety Dictionary, is considered „an incident that occurs during the process of providing health care and results in patient injury or death.”4 Of these 185 000 events, 70 000 are considered „potentially preventable.”3 These results have been used to estimate the number of deaths that occur in Canada due to preventable adverse events. On the basis of these extrapolations, it is estimated that preventable adverse events contribute to between 9000 and 23 000 preventable deaths annually.3 Preventable adverse events contribute to 4%–10% of all deaths, making them the fourth most frequent cause of death in Canada. Although this number may seem astonishing to some, it is important to note that the Canadian figures are similar to those in other developed countries.
Research in the United States,5 Australia6 and the United Kingdom7 has estimated the impact of medical error on patient health. Two major studies in the US, one conducted in New York8 and the other in Colorado and Utah,5 reviewed patient records to identify the number of patient injuries that occurred due to medical error. These studies estimate that 3.7%8 and 2.9%5 of individuals admitted to hospital experienced an injury caused by medical error. The error rates estimated by the studies conducted in the US are lower than those estimated in Canadian and other national studies. For example, the Australian study found a 13% adverse incident rate6 using a similar methodology. In the UK, Vincent and colleagues7 estimated that 10.8% of patients admitted to hospital experienced an adverse event. It is not clear whether these differences in rates reflect true differences in the incidence of adverse events or if they were due to subtle differences in methodology. Further research is clearly required.
Not surprisingly, however, such studies have sparked much debate about the accuracy and the meaning of the injury rates. For example, McDonald and colleagues9 point out that many of these patients were critically ill and may have died anyway. Nonetheless, there is general agreement that the current level of medical error is unacceptably high.10
The recognition of the need to reduce the frequency of adverse events has resulted in substantial research into medical error.11 12 13 Recent medical error studies have drawn upon the large body of research into human error within high-reliability industries such as aviation, chemical processing and nuclear power.14 15 16 At a superficial level, medical teams appear to be very different from commercial aviation flight crews, nuclear control room operators and other high-reliability teams, but closer examination reveals that they face very similar challenges. For example, medical teams often have to work in situations where they are faced with time pressure, competing goals, poorly defined problems and significant consequences of error.
Research suggests that technological solutions alone are unlikely to be effective and that a broader systemic approach including organizational and interpersonal aspects of performance is required. This is also referred to as the „systems approach” to human error,17 which views human error as a consequence of system failure rather than a cause of an incident. This is in stark contrast to the person approach that has been traditionally used within the medical domain. The person approach views human error as being due to inadequacies (mental, physical or motivational) of the individual. Therefore, actions taken to prevent a reoccurrence focus solely on the individual and include discipline, litigation and retraining. Although the person approach is emotionally satisfying, particularly if you have suffered as a result of the error, it presents a major barrier to the development of safer health care organizations.17
There is increasing recognition of the need to pay more attention to the psychological and human factors aspects of medical performance.18 Chopra and colleagues19 concluded that 80% of medical errors are caused by failures to check, poor communication, or haste and fatigue. Increasing numbers of human factors researchers have started working within the medical domain in order to test the extent to which theoretical frameworks developed in other high-reliability industries, such as the petrochemical industry,20 aviation11 and offshore oil,12 apply within the medical domain.
To date, anesthesiology is the medical discipline that has been most receptive to adopting human factors techniques to investigate and reduce error. It is estimated that in 20% of all surgeries an anesthesia problem will occur. Of these problems, 1 of every 4 will lead to an adverse outcome for the patient.21 Most studies designed to explore methods to reduce error have focused on increasing situational awareness of these professionals. In most cases, improvements to equipment displays were suggested as a method to improve reaction times.22 In one study, detection time was improved by 63% after the introduction of a new 3- dimensional display.22 These findings offer additional support for the view that human error can be reduced through methods other than technical training.
Adverse incident analysis studies have been conducted examining adverse drug events,23 intensive care incidents24 and transfusion errors.25 These studies have been successful at identifying human factors causes that contributed to adverse incidents. Additional studies have also identified human error as a cause of adverse patient outcomes in intensive care units.26 Thirty-seven percent of 554 cases of human error (identified over a 4-month period) were attributed to communication breakdowns. These numbers suggest that the potential for error is not simply the result of inadequacies in health care professionals' knowledge or skills. The authors concluded that an increased emphasis on communication and/or leadership skills may have prevented some of the errors they identified.26
In cardiac surgery, de Leval and colleagues27 have observed operations and coded errors they identified using a human factors framework. These studies have documented a wide range of system factors that contributed to negative patient outcomes. Although these studies provide important information about system failures that lead to adverse outcomes, they provide little information about system factors that ensure positive outcomes. There is a need to conduct a more comprehensive prospective analysis of medical performance and to identify the processes that underlie successful recovery from error.27
An alternative research approach to investigating medical team performance is to examine team members' attitudes to identify those associated with successful performance. Medical teams' attitudes are important because there is substantial evidence that attitudes reflect subsequent behaviour.28 Therefore, it is important to identify attitudes that reflect behaviours that influence patient outcomes. Sexton and colleagues11 modified the Flight Management Attitudes Questionnaire (FMAQ), which is widely used in the aviation industry, to develop the Operating Room Management Attitudes Questionnaire (ORMAQ) and surveyed medical staff. Their comparison of medical staff with flight crews indicates that medical staff responses differ from flight crews' responses on a number of critical dimensions. Medical staff members are more likely than flight crews to deny the impact that stress and fatigue may have on performance, and there is long-standing research evidence that links stress and fatigue with error.29
Successful cardiac surgery requires highly skilled individuals to work effectively as a team. Although surgery requires team members to have the requisite medical knowledge and skills, interpersonal skills are vital to successful cardiac surgery. Surgeons, anesthesiologists, perfusionists, nurses and residents must communicate effectively in order to ensure successful patient outcomes. Breakdowns in communication, decision-making or leadership could prove disastrous for the patient and, in consequence, for the reputation of the hospital and medical staff.
We are not aware of any published literature available on the attitudes of cardiac surgery team members toward teamwork and safety. Although there have been attempts to investigate other variables such as processes and structures within cardiac surgery,30 these studies did not explore team communication, leadership or error management. This paper reports the findings of what we believe to be the first Canadian study to use the ORMAQ to survey cardiac surgery team members' attitudes toward teamwork and safety.
Methods
Cardiac team members' attitudes were measured via the ORMAQ. This questionnaire, based on the FMAQ, is designed to measure factors associated with effective team performance. The FMAQ was developed through extensive research in the aviation industry and has been used as a key indicator of flight safety. One drawback of the ORMAQ is concern about the reliability of the factors measured by the questionnaire. Helmreich and Davis31 report internal consistencies between 0.55 and 0.85 for the ORMAQ. We obtained an internal consistency of 0.53 on the 60-item attitudes scale, which is somewhat low. Nonetheless, the ORMAQ is the standard measure used to assess attitudes in medical teams.20 The final format of the questionnaire included 4 sections: (1) attitude statements, (2) ratings of team members, (3) observed error and (4) a section for comments and background information.
Operating room management attitudes
This portion of the questionnaire was made up of 60 items. Responses (on a 5-point scale) ranged from 1 („disagree strongly”) to 5 („agree strongly”) with 3 („neutral”) as the midpoint. Examples of items found in this section are „Doctors who encourage suggestions from operating theatre team members are weak leaders” or „I am encouraged by my leaders and coworkers to report any incidents I may observe.” These 60 items address a total of 8 topics including leadership structure, confidence assertion, information sharing, stress and fatigue, teamwork, work values, error/procedural compliance and organizational climate.11
Evaluation of team members
This 9-item section measures individual members' perceptions of the level of teamwork, cooperation and communication with each group of members of the cardiac team (e.g., surgeons, perfusionists, nurses). Responses ranged on a 5-point scale from „very low” to „very high” with „adequate” as the midpoint.
Error in medicine
This section measured respondents' attitudes toward medical error, the causes of error and their perception of potential actions to prevent error. The section included Likert-style response options (a 5-point scale from „disagree strongly” to „agree strongly” with „neutral” as the midpoint). Examples of items in this section included „Errors committed during patient management are not important, as long as the patient improves” or „Medical errors are discussed to prevent recurrence.” In addition, there was an open-ended portion that included 2 questions: „What are the 3 most frequently occurring errors in the theatre (that you have observed)?” and „In your experience, what strategies have you seen to be effective for managing error in the operating theatre?”
Comments and demographic information
This section captured comments and background information such as position within the cardiac team.
Participants
The questionnaire was distributed to members of the cardiac surgery team, which included anesthesiologists, cardiac surgeons, perfusionists, anesthesia residents, surgical residents and operating room nurses. Participants were invited to take part in the study during rounds or special meetings. The authors gave a presentation outlining the purpose of the project, how the responses would be used and the anonymity of respondents. Following the presentation, the authors answered any questions. Those who were interested were given an informed consent form to read and sign. The questionnaires were then distributed, and participants were encouraged to complete them at that time. If time constraints did not permit completion of the questionnaire on site, participants had the option to respond via a stamped, addressed envelope. Team members who were unable to attend the departmental meetings were sent questionnaire packs through internal mail.
Statistical analysis
Once all data were screened, a series of nonparametric tests was conducted to determine whether any significant differences between the occupational groups were evident. The Kruskal–Wallis k-sample test for independent samples was selected, because the assumptions for a 1-way analysis of variance could not be met. The primary concern in this study was the violation of homogeneity of variance between groups. The results must be treated with caution because there is potential for type I error(s), since there is a risk of capitalizing on chance by conducting 60 individual Kruskal–Wallis tests. To reduce the risk of type I error(s), only differences significant at p < 0.01 are presented. All post hoc tests were completed using the Mann–Whitney U indicator. The U statistic represents a comparison or contrast between groups. The M statistic denotes mean responses within a group. Significance for the Mann–Whitney test was set at p < 0.05.
Results
A total of 53 completed questionnaires were returned, which is a response rate of 76%. The 53 respondents included 13 theatre nurses, 12 anesthesia residents, 9 anesthesiologists, 6 cardiac surgeons, 6 perfusionists, 5 surgical residents and 1 clinical clerk. One subject did not complete the job category field. Table 1 indicates the percentage of respondents who agreed, responded neutrally or disagreed with the 60 items on the first portion of the ORMAQ. For ease of presentation, the 5-item response scale was collapsed by merging the response categories. „Disagree strongly” and „disagree slightly” are labelled „disagree,” and „agree strongly” and „agree slightly „were merged into the single category of „agree.” The midpoint remained „neutral.”
Table 1
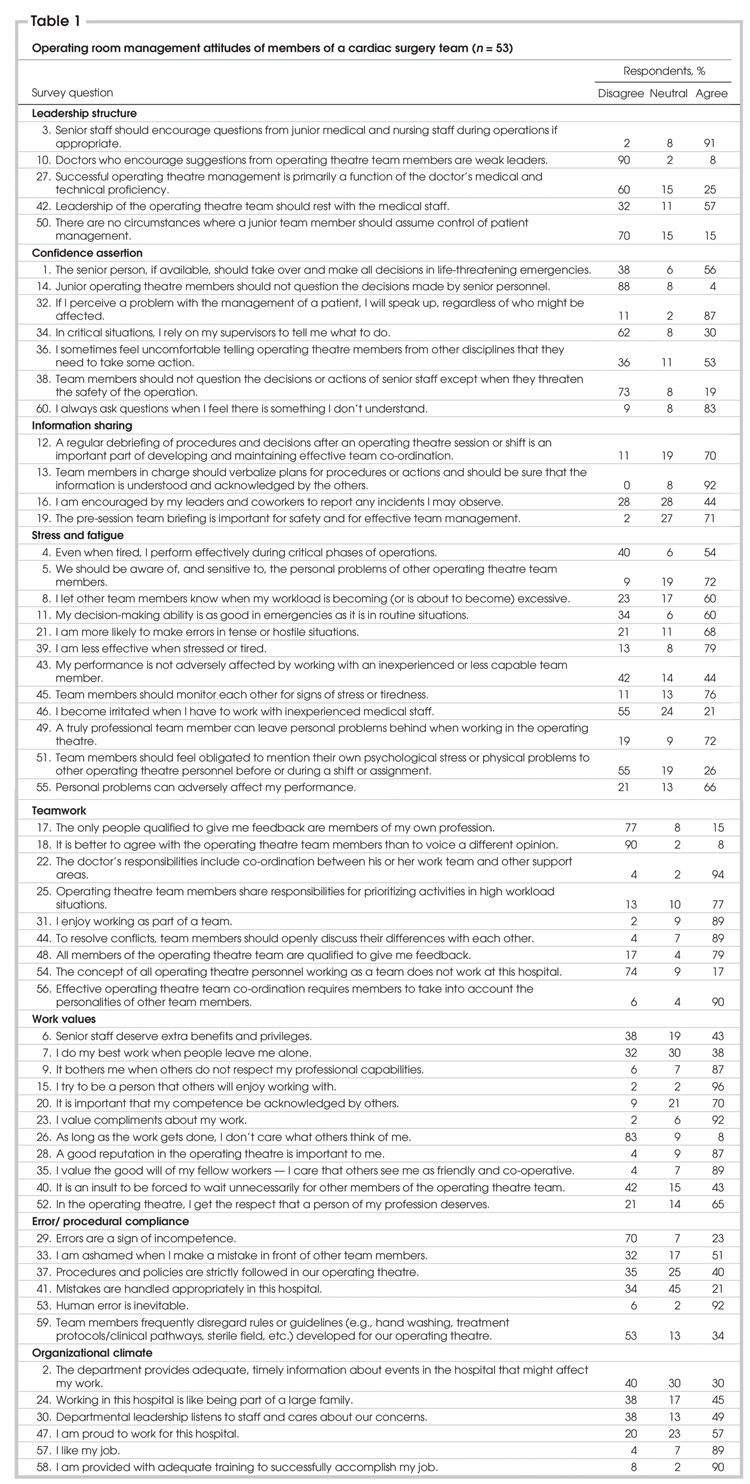
Operating room management attitudes
Occupations were divided into 4 groups: surgeons and surgical residents, anesthesiologists and anesthesia residents, nurses and perfusionists. Significant differences for the ORMAQ items are reported in (Figure 1.
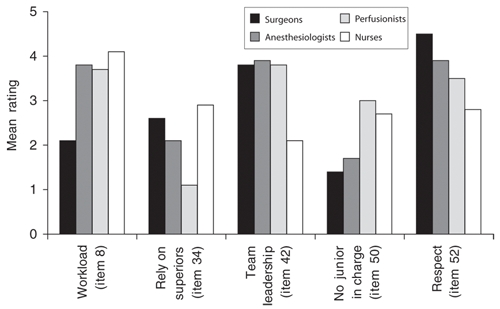
FIG. 1. Attitudes of members of a cardiac surgery team grouped according to occupation (see Results section). Ratings on a 5-point scale ranged from 1 = „disagree strongly” to 5 = „agree strongly.” ORMAQ items are displayed in parentheses. ORMAQ = Operating Room Management Attitudes Questionnaire.
The results indicate that surgeons are less likely than other team members to inform others when their workload is becoming excessive (χ23 = 19.25, p < 0.001). A post hoc analysis revealed that surgeons were less likely than anesthesiologists (U = 27.5, p < 0.001), perfusionists (U = 11, p < 0.05) and nurses (U = 13, p < 0.001) to inform others of workload issues. This finding was not surprising, because it supports previous studies that suggest that professional cultures (e.g., physicians, pilots) may have unrealistic attitudes regarding their personal capabilities.32 Perfusionists reported being less likely to rely on their superior for guidance during critical situations (χ 2 3 = 8.66, p < 0.05). This is probably because their supervisor is typically not present in the operating room. Nurses were less satisfied (M = 2.07) with team leadership than other occupational groups (M = 3.86), (χ 2 3 = 13.4, p < 0.05). A significant difference was identified on the item „there are no circumstances where a junior team member should take charge” (χ 2 3 = 11.5, p = 0.05), such that perfusionists (M = 3.0) and nurses (M = 2.76) were more likely than others (M = 1.56) to agree with the statement.
Respondents were also classified on the basis of occupational status within the operating room, such that responses of surgeons and anesthesiologists were combined as the group with greater authority in the operating room. Responses of perfusionists, residents and nurses were combined as the group more likely to have less authority in the operating room hierarchy. (Figure 2 highlights the differences between these 2 groups. Subordinate team members (M = 2.24) were more likely to report that there were no circumstances when a junior member of the team should take charge (U = 177, p < 0.05). Interestingly, surgeons and anesthesiologists were less likely to agree with the above statement (M = 1.53), suggesting that they trust the capabilities of subordinate staff to a greater extent than the rest of the team (including their residents). Consistent with this finding, surgeons and anesthesiologists (M = 1.26) were less likely to agree with the statement that junior team members should not question their decisions (U = 181, p < 0.05) than the rest of the team (M = 1.66). Therefore senior staff reported being more open to being questioned than subordinate staff perceive them to be. In contrast with this finding, surgeons and anesthesiologists (M = 3.00) were more likely to report being intolerant of working with inexperienced staff (M = 2.16) (U = 155.5, p < 0.001) than other team members.
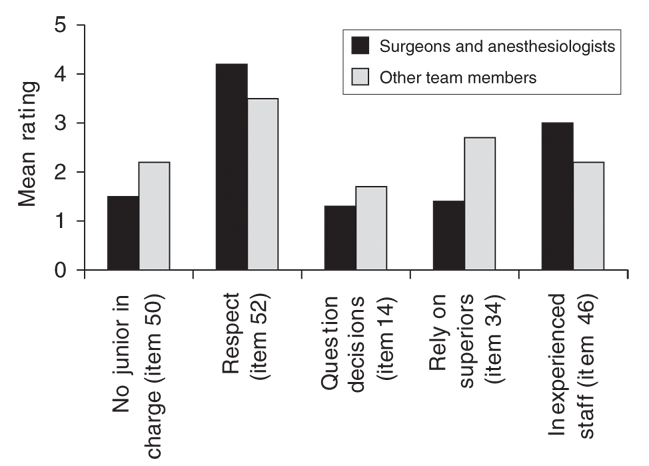
FIG. 2. Attitudes of members of a cardiac surgery team grouped according to occupational status (see Results section). Ratings on a 5-point scale ranged from 1 = „disagree strongly” to 5 = „agree strongly.” ORMAQ items are displayed in parentheses. ORMAQ = Operating Room Management Attitudes Questionnaire.
Team members in positions of authority reported higher levels of perceived professional respect (M = 4.2) than the subordinate team members (M = 3.5) (U = 174.5, p = 0.05). In addition, senior staff were less likely to report that they relied on their superiors (M = 1.40) (U = 235.5, p < 0.001) than the rest of the team (M = 2.70), which is not surprising given that they typically do not have a supervisor in the operating room.
Evaluation of team members
Respondents also evaluated each occupational group (e.g., surgeons) on the basis of their ability to work as part of a team on a 5-point scale from „very low” to „very high.” (Figure 3 presents how each occupational group views themselves and how others view them. Most occupational groups' ratings of their colleagues are the same as others' rating of their own group. The anesthesia residents and surgical residents are the notable exceptions, because they rated their colleagues more positively than other groups rated them. This may be the result of a lack of awareness regarding their skills at working as part of a team, or it may indicate that they work effectively together but are less effective at working with other occupational groups.
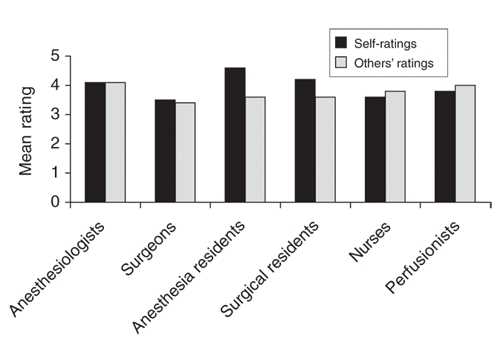
FIG. 3. Ratings of ability to work as part of a team for each occupation by self and by other occupational groups (see Results section). Ratings on a 5-point scale ranged from 1 = „very low” to 5 = „very high.”
Error in medicine
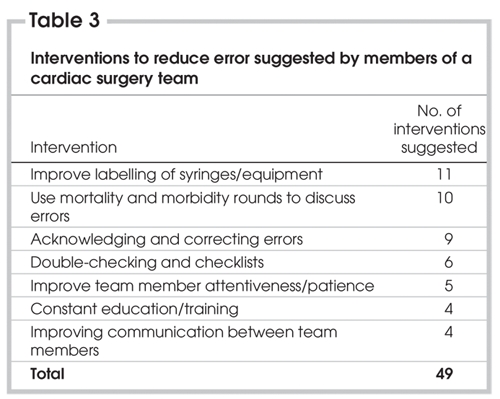
Respondents reported the most frequent errors they observed cardiac surgery team members committing. Table 2 presents a summary of the errors reported grouped into similar categories. The most frequent error types included miscommunication, not performing actions at the correct time and not following established procedures. Respondents also proposed interventions to reduce error. Table 3 categorizes the various team members' suggestions into common themes. Common suggestions were to improve the labelling of equipment and drugs and to make better use of mortality and morbidity rounds to discuss error and identify solutions. In addition, cardiac surgery team members suggested the use of interventions to increase patience and reduce haste when performing various functions in the operating room.
Table 2
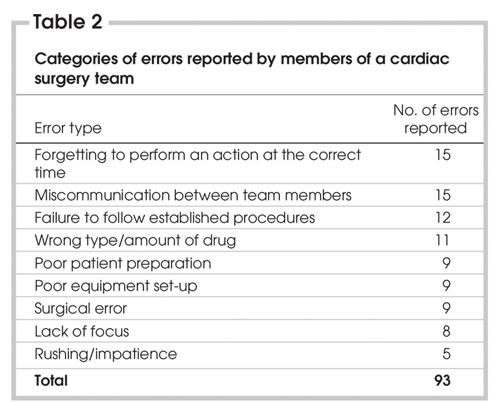
Table 3
Discussion
This pilot study is the first attempt that we are aware of to measure Canadian cardiac surgery team attitudes to teamwork and error using the ORMAQ. Although the sample was small (n = 53), the response rate of 76% was good. The high response rate supports the approach of organizing specific meetings to distribute the questionnaires to participants. These sessions informed participants about the research and gave them dedicated time to complete and return the questionnaire.
In general, the responses are positive, indicating that team members are willing to speak up if they have a concern or ask questions. For example, 90% of respondents disagreed with the statement „It is better to agree with the operating theatre team members than to voice a different opinion;” 83% agreed with the statement „I always ask questions when I feel there is something I don't understand;” 87% agreed with the statement „If I perceive a problem with the management of a patient, I will speak up, regardless of who might be affected;” and 88% disagreed with the statement „Junior operating theatre members should not question the decisions made by senior personal.” In addition, respondents indicated that they were aware of the effects of fatigue and stress on performance as 79% agreed with the statement „I am less effective when stressed or tired.”
Although responses were generally positive, the results suggest that team performance could be improved by addressing compliance with procedures and encouraging team members to report adverse events. For example, 35% disagreed with the statement „Procedures and policies are strictly followed in our operating theatre;” 34% agreed with the statement „Team members frequently disregard rules or guidelines (e.g., hand washing);” and only 43% agreed with the statement „I am encouraged by my leaders and co-workers to report any incidents I may observe.” This suggests that further investigation of compliance with rules and procedures is worthwhile, in order to establish the extent of the problem and to identify the factors that influence compliance. In addition, the results indicate that safety could be improved by senior surgical team members increasing the level of encouragement they give team members to report adverse events, as these reports are an important source of information.
In general, the occupational groups and the respondents with different levels of authority reported similar attitudes and there were relatively few statistically significant differences. Interestingly, the surgeons reported being less willing to inform other team members when their workload was becoming excessive. This may provide an opportunity for improvement by training surgeons to make better use of the resources available in times of peak workload. Making use of all the resources available is one of the core aims of Crew Resource Management, which has been used successfully in the aviation industry. Leadership is another area where there are differences between the occupational groups. Junior team members are less satisfied with their leadership: they are uncertain about taking charge of a situation and are not confident about questioning the decisions of more senior staff. These differences suggest that surgeons and anesthesiologists could demonstrate more effective leadership by encouraging junior team members to speak up if they have any concerns, and they could give guidance about situations when it would be appropriate for junior team members to take charge of a situation.
Most respondents identified errors associated with interpersonal competencies, such as miscommunication or not complying with procedures, although surgical error was listed by 9 of the respondents. Miscommunication in this context only considers miscommunication between operating room personnel. These common error types provide opportunities for improving patient safety, by identifying strategies to reduce the likelihood of these errors. For example, the introduction of checklists may reduce the likelihood of forgetting to perform an action at the correct time and to ensure correct equipment set-up. In fact, the perfusion department use checklists for their equipment set-up. Communication could be improved by providing communication skills training and the introduction of closed-loop communication (repeating important messages to confirm understanding) practices. In addition, further research into other areas of cardiac medicine such as preoperative and postoperative care is advised to determine potential weaknesses in communications throughout the various stages of patient care. Clearly, further investigation is required to identify suitable interventions to reduce the frequency of these errors.
Participants also identified a number of interventions that could reduce the frequency of error. These interventions are similar to strategies being proposed by other patient safety bodies. Participants also highlighted the importance of open reporting and discussion of errors. As mentioned above, patient safety could be improved by senior surgical team members encouraging others to report errors by modelling this behaviour for other team members.
Limitations and future research
Although this pilot study produced some interesting findings, the results must be treated with caution because they are based on the responses of only one team and because the study involved a small sample. Because it is not possible to be confident that the results can be generalized to other Canadian cardiac teams, we plan to conduct further research by expanding the sample to include a larger number of cardiac teams. Although there is evidence supporting the relation between responses on the FMAQ and outcomes in the aviation industry, the relation between responses on the ORMAQ and patient outcomes has not been demonstrated. Therefore, it is not possible to be confident that participant responses are related to patient outcomes. By surveying more cardiac teams, it may be possible to examine the relation between questionnaire responses and outcomes, through examining differences between teams.
Concerns about the reliability of the factor structure of the ORMAQ is another limitation of the study, because it necessitated comparing groups on questionnaire items rather than factors. This item comparison is unsatisfactory, because it increases the possibility that the differences between groups are only due to chance rather than true differences.
Acknowledgments
The authors would like to thank Janet Slaunwhite and all the members of the cardiac team for their participation in this study. We would also like to thank Dr. Robert Helmreich for use of the ORMAQ as an assessment tool.
This research was funded through Nova Scotia Health Research Fund Development Grants awarded to the first and second authors and a Saint Mary's University Faculty of Graduate Studies and Research grant awarded to the first author.
Competing interests: None declared.
Correspondence to: Dr. Mark Fleming, Department of Psychology, Saint Mary's University, Halifax NS B3H 3C3; tel 902 420-5273; fax 902 496-8287; mark.fleming@smu.ca
References
- 1.Sinclair CM. The report of the Manitoba Pediatric Cardiac Surgery Inquest: an inquiry into twelve deaths at the Winnipeg Health Sciences Centre in 1994. Winnipeg: Provincial Court of Manitoba; 2000. Available: www.pediatriccardiacinquest.mb.ca (accessed 2005 Nov 28).
- 2.Davies J. Painful inquiries: lessons from Winnipeg. CMAJ 2001;165:1503-5. [PMC free article] [PubMed]
- 3.Baker GR, Norton P, Flintoft V, et al. The Canadian Adverse Events Study: the incidence of adverse events among hospital patients in Canada. CMAJ 2004;170:1678-86. [DOI] [PMC free article] [PubMed]
- 4.Royal College of Physicians and Surgeons of Canada. The Canadian patient safety dictionary. Ottawa: the College; 2003.
- 5.Thomas EJ, Studdert DM, Burstin HR, et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care 2000;38:261-71. [DOI] [PubMed]
- 6.Wilson RMcL, Runciman WB, Gibberd RW, et al. The Quality in Australian Health Care Study. Med J Aust 1995;163:458-71. [DOI] [PubMed]
- 7.Vincent C, Neale G, Woloshynowych M. Adverse events in British hospitals: preliminary retrospective record review. BMJ 2001;322:517-9. [DOI] [PMC free article] [PubMed]
- 8.Brennan T, Leape L, Laird N, et al. Incidence of adverse events and negligence in hospitalized patients. N Engl J Med 1991;324:370-6. [DOI] [PubMed]
- 9.McDonald CJ, Weiner M, Hui SL. Deaths due to medical errors are exaggerated in Institute of Medicine report. JAMA 2000;284:93-4. [DOI] [PubMed]
- 10.Hayward R, Hofer T. Estimating hospital deaths due to medical error. JAMA 2001;286:415-20. [DOI] [PubMed]
- 11.Sexton J, Helmreich RL, Thomas E. Error, stress and teamwork in medicine and aviation: cross sectional surveys. BMJ 2000;320:745-50. [DOI] [PMC free article] [PubMed]
- 12.Carthey J, de Laval MR, Reason JT. The human factor in cardiac surgery: errors and near misses in a high technology medical domain. Ann Thorac Surg 2001;72:300-5. [DOI] [PubMed]
- 13.Laffel G, Nemeskal R, Peterson LA, et al. Systems analysis of adverse drug events. JAMA 1995;274:35-43. [PubMed]
- 14.Perrow C. Normal accidents. New York: Basic Books; 1984.
- 15.Reason J. Human error. Cambridge: Cambridge University Press; 1990.
- 16.Reason J. Managing the risk of organization accidents. Brookfield: Ashgate; 1997.
- 17.Reason J. Human error: models and management. BMJ 2000;320:768-70. [DOI] [PMC free article] [PubMed]
- 18.Leape LL. Error in medicine. JAMA 1994;272:1851-7. [PubMed]
- 19.Chopra V, Bovill JG, Spierdijk J, et al. Reported significant observations during anaesthesia: a prospective analysis over an 18-month period. Br J Anaesth 1992;68:13-7. [DOI] [PubMed]
- 20.Flin R, Fletcher G, McGeorge P, et al. Anaesthestists' attitudes to teamwork safety. Anaesthesia 2003;58:233-42. [DOI] [PubMed]
- 21.Gaba D, Maxwell M, DeAnda A. Anaesthetic mishaps: breaking the chain of accident evolution. Anesthesiology 1987;66:670-6. [PubMed]
- 22.Zhang Y, Drews FA, Westenskow DR, et al. Effects of integrated graphical displays on situational awareness in anesthesiology. Cogn Technol Work 2002;4:82-90.
- 23.Anderson BJ, Ellis JF. Common errors of drug administration in infants: causes and avoidance. Paediatr Drugs 1999;1:93-107. [DOI] [PubMed]
- 24.Zimmerman JE, Shortell SM, Knaus WA, et al. Value and cost of teaching hospitals: a prospective, multicenter, inception cohort study. Crit Care Med 1993;21:1432-42. [DOI] [PubMed]
- 25.Kaplan HS, Battles JB, Van der Schaaf TW, et al. Identification and classification of the causes of events in transfusion medicine. Transfusion 1998;38:1071-81. [DOI] [PubMed]
- 26.Donchin Y, Gopher D, Olin M, et al. A look into the nature and causes of human errors in the intensive care unit. Crit Care Med 1995;23:294-300. [DOI] [PubMed]
- 27.De Leval MR, Carthey J, Wright DJ, et al. Human factors and cardiac surgery: a multicenter study. J Thorac Cardiovasc Surg 2000;119:661-72. [DOI] [PubMed]
- 28.Eagly AH, Chaiken S. The psychology of attitudes. Fort Worth (TX): Harcourt Brace Janovich; 1993.
- 29.Wickens C, Hollands J. Engineering psychology and human performance. Upper Saddle River (NJ): Prentice Hall; 2000.
- 30.Shroyer AL, London MJ, Villanueva CB, et al. The processes, structures, and outcomes of care in cardiac surgery study protocol. Med Care 1995;33(10 Suppl):OS17-25. [DOI] [PubMed]
- 31.Helmreich R, Davies J. Human factors in the operating room: interpersonal determinants of safety, efficiency and morale. In: Aikenhead A, editor. Balliere's clinical anaesthesiology. London: Balliere Tindall; 1996. p. 277-95.
- 32.Helmreich R, Merritt A. Culture at work in aviation and medicine: national, organizational and professional influences. Aldershot (UK): Ashgate; 1998.