

Abstract
Key questions remain unresolved regarding the advantages and limitations of colloids for fluid resuscitation despite extensive investigation. Elucidation of these questions has been slowed, in part, by uncertainty as to the optimal endpoints that should be monitored in assessing patient response to administered fluid. Colloids and crystalloids do not appear to differ notably in their effects on preload recruitable stroke volume or oxygen delivery. Limited evidence nevertheless suggests that colloids might promote greater oxygen consumption than crystalloids. It remains unclear, in any case, to what extent such physiological parameters might be related to clinically relevant outcomes such as morbidity and mortality. Recent randomized controlled trial results indicate that, at least in certain forms of fluid imbalance, albumin is effective in significantly reducing morbidity and mortality. Much further investigation is needed, however, to determine the effects of colloid administration on clinically relevant outcomes in a broad range of critically ill patients. The ability of administered colloids to increase colloid osmotic pressure (COP) constitutes one mechanism by which colloids might reduce interstitial oedema and promote favourable patient outcomes. However, the applicability of this mechanism may be limited, due to the operation of compensatory mechanisms such as increased lymphatic drainage. Attempts to increase COP might also be less useful in states of increased vascular permeability such as acute respiratory distress syndrome, although this issue has by no means been settled by empirical data. Colloids are clearly more efficient than crystalloids in attaining resuscitation endpoints as judged by the need for administration of far smaller fluid volumes. Among the colloids, albumin offers several advantages compared with artificial colloids, including less restrictive dose limitations, lower risk of impaired haemostasis, absence of tissue deposition leading to severe prolonged pruritus, reduced incidence of anaphylactoid reactions, and ease of monitoring to prevent fluid overload. The cost of albumin, nevertheless, limits its usage. Crystalloids currently serve as the first-line fluids in hypovolaemic patients. Colloids can be considered in patients with severe or acute shock or hypovolaemia resulting from sudden plasma loss. Colloids may be combined with crystalloids to obviate administration of large crystalloid volumes. Further clinical trials are needed to define the optimal role for colloids in critically ill patients.
Keywords: colloids, critical care, osmotic pressure, serum albumin, shock
Introduction
The long-standing controversy regarding the optimal role of colloids in fluid resuscitation shows little sign of abating. Indeed, two recent meta-analyses have reintensified the debate [1,2]. Although investigations related to this issue have spanned four decades, many questions remain unresolved. Yet this area of clinical investigation remains highly active, and some of the most recent data on potential advantages of colloid administration have provided important new insight [3].
Given the continuing accumulation of relevant clinical data, it is pertinent to ask what conclusions can now be drawn regarding the appropriate role of both natural and artificial colloids. What are the most useful endpoints for evaluating the effects of administered fluids? From the clinical standpoint, how important is COP? How similar are natural and artificial colloids in their properties? Is there conclusive evidence of differences in patient outcomes with colloids versus crystalloids? In what clinical situations might colloids offer advantages over crystalloids? These are the primary issues that this review is intended to address.
Fluid resuscitation endpoints
Hypovolaemia is very difficult to detect at the bedside [4]. Neither hypotension nor severe tachycardia may be apparent. Stroke volume may be declining; however, this decline may go undetected unless measurements are made of this parameter. What, then, is the optimal set of fluid resuscitation endpoints that should be monitored to promote favourable patient outcomes? The definitive answer is not yet at hand. Oliguria, generally regarded as an adverse finding, might in one scenario prompt the administration of fluid. As a result, increases might be achieved in blood pressure, oxygen delivery to the tissues and, perhaps, associated oxygen consumption. These changes may be associated with increased preload recruitable stroke work, resulting in decreased lactate levels. The tonometric PCO2 gradient could also provide a useful measure of regional perfusion adequacy. It is nevertheless unclear whether this would be the optimal parameter to monitor, either alone or in conjunction with other measurements. The type of fluid that would be of greatest utility in rectifying the patient's oliguria is also unclear.
In a randomized controlled trial (RCT) of 26 patients with hypovolaemic and septic shock, the left ventricular stroke work index (LVSWI) was found to rise with increasing pulmonary artery wedge pressure (PAWP) following fluid challenge [5]. This finding provides evidence for the existence of preload recruitable stroke work in hypovolaemia. The volume of crystalloid needed to maintain the target PAWP level was two- to four-fold greater than that of colloid. Increased LVSWI is associated with rising PAWP up to approximately 12 mmHg whereas, at PAWP>12 mmHg, little or no further rise is observed in LVSWI [6]. Colloids and crystalloids have not been found to differ notably in promoting a preload recruitable stroke work response.
Choice of fluid, however, may affect oxygen delivery and associated oxygen consumption, although relevant data are scanty. Infusion of Ringer's lactate in hypovolaemic surgical patients resulted in modest oxygen delivery increases due to greater preload recruitable stroke work, but concomitant augmentation of oxygen consumption was not observed [7]. In patients receiving 25% albumin, by contrast, the magnitude of increase in oxygen delivery was significantly greater than that of Ringer's lactate recipients, and albumin infusion was also associated with rising oxygen consumption. The precise mechanisms and consequences of these phenomena have yet to be delineated. It is plausible that Ringer's lactate may increase tissue oedema as compared with hyperoncotic albumin. The expected effect of such oedema would be to retard oxygen uptake by increasing distances from the blood vessels to the mitochondria. In this regard, natural colloid may exert more favourable effects on tissue oxygenation than a crystalloid. The extent to which such fluid-associated differences in oxygenation might translate into morbidity or mortality differences remains to be defined. Further studies are needed to confirm the relationship between fluid type and oxygenation, and to characterize this relationship in terms of clinically relevant outcomes.
One recently reported RCT of patients with cirrhosis and spontaneous bacterial peritonitis has demonstrated superior outcomes in terms of both morbidity and mortality in patients receiving albumin [3]. Such patients experience circulatory dysfunction characterized by vasodilatation, hypotension, elevated cardiac output, diminished effective blood volume, activation of the renin-angiotensin and sympathetic nervous systems, and increased circulating arginine vasopressin and endothelin. Volume expansion with albumin might avert this circulatory dysfunction by maintaining effective blood volume and prevent subsequent renal impairment. The frequency of renal impairment, as shown in Figure 1, was significantly lower in albumin recipients than in the control group, and mortality was significantly reduced both during hospitalization and at 3 months after discharge.
Figure 1.
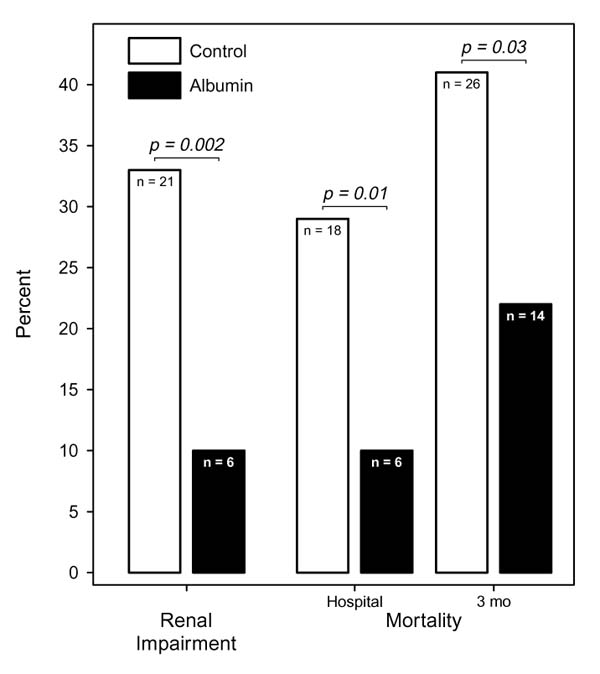
Percent incidence of kidney impairment and death in albumin recipients and control patients with cirrhosis and spontaneous bacterial peritonitis. Based on the data of Sort et al [3].
Colloid osmotic pressure
Based upon Starling's equation, COP should theoretically be important for maintaining fluid balance in patients by virtue of its influence on fluid flux between the intravascular and extravascular compartments. Depressed COP during hypovolaemia could contribute to interstitial fluid overload and oedema formation. Impaired blood flow, oxygen transport, and hepatic and renal function might result. Oedema in the lungs would lead to deterioration in gas exchange.
The role played by COP may nevertheless not be major. Low plasma COP, for example, may not result in tissue oedema under normal circumstances due to compensatory mechanisms such as increased lymphatic drainage. Attempts in increased permeability states to increase COP by administration of colloids could also fail to ameliorate interstitial oedema. The normal transcapillary escape rate of albumin, mediated in major part by the liver, is 5%/h. Fluid filtration, surface area and permeability are the primary factors affecting transcapillary escape rate, and clinical conditions associated with an elevation of this rate are summarized in Table 1.
Table 1.
Clinical conditions associated with increased albumin transvascular escape rate
| Hypertension |
| Congestive heart failure |
| Exercise |
| Catecholamines |
| Diabetes mellitus |
| Infection, sepsis and shock |
| Hypothyroidism |
| Major surgery and trauma |
| Fluid loading |
| Chemotherapy |
| Vasculitis and glomerulonephritis |
| Cardiopulmonary bypass |
| Ischaemia/reperfusion |
| Burns |
In acute respiratory distress syndrome (ARDS) and associated conditions, for example, COP may be of limited importance as a determinant of tissue hydration status. Pulmonary oedema may thus be more dependent on hydrostatic forces than on COP. Differential effects of colloids and crystalloids on fluid balance and oedema formation may consequently not be operative in ARDS. Such differential effects may, however, assume importance in particular time intervals during the course of certain critical illnesses.
If increasing COP is deemed clinically desirable, it can be accomplished by administration of either natural or artificial colloid. In hypovolaemic postoperative patients, for example, either albumin or hetastarch administration resulted in sustained COP increases [8]. Saline decreased COP. Albumin and hetastarch were found effective in patients with hypovolaemic and septic shock, both in raising COP and maintaining the COP-PAWP gradient, whereas saline conversely decreased COP and markedly reduced the COP-PAWP gradient [5]. A decreased COP-PAWP gradient in a study of 76 critically ill patients was associated with the occurrence and severity of pulmonary oedema and, in the subset of patients with circulatory shock, was also predictive of mortality [9].
In light of these observations, might the choice of resuscitation fluid influence pulmonary oedema formation? Available evidence bearing on this issue is highly limited. COP declined substantially in patients receiving Ringer's lactate but not 5% plasma protein fraction in a prospective study of 18 patients undergoing aortic reconstructive surgery. No corresponding difference could be demonstrated in extravascular lung water, however, as directly measured by a thermal green dye double indicator dilution technique [10]. This lack of difference might be attributable to a compensatory increase in lymphatic flow among the Ringer's lactate recipients.
Pulmonary oedema was indirectly assessed by alveolar to arterial oxygen gradient and intrapulmonary shunt in a RCT of 141 patients undergoing laparotomy for acute abdominal trauma [11]. Neither parameter differed significantly over the 5-day study observation period between patients receiving 4% albumin versus Ringer's lactate. The incidence of radiographically demonstrable pulmonary oedema in another RCT was, however, significantly higher in patients receiving saline than either albumin or hetastarch [5]. Fluid overload with colloid may, on the other hand, impair respiratory function as evaluated by the ratio between the fraction of inspired oxygen and the partial pressure of oxygen in arterial blood (PaO2/FiO2) [12].
Albumin versus artificial colloids
Artificial colloids such as hetastarch have been extensively investigated as alternatives to albumin. Although artificial colloids typically provide volume expansion comparable with that of albumin, they are nevertheless subject to certain disadvantages. For example, limitations in recommended doses may be exceeded in some patients, so that albumin may be required to meet the further fluid needs of the patient. Although available evidence is conflicting, hetastarch may be associated with impaired haemostasis [13]. Deposition of hetastarch in the skin can frequently lead to severe protracted pruritus [14]. Impaired renal function has also been documented in association with hetastarch usage [15]. Finally, the incidence of anaphylactoid reactions may be higher in hetastarch than albumin recipients [16].
In view of the potential deleterious effects that might result from colloid overload, as already indicated, one advantage of albumin vis-à-vis artificial colloids is the reduced likelihood of administering excessive fluid. COP is seldom measured on a routine basis. Overload with artificial colloids is hence not readily detected, and dose-dependent side effects may be difficult to avoid. Albumin concentration, in contrast, is a routine daily laboratory determination. Furthermore, more frequent albumin assays can be performed during resuscitation, and such monitoring can serve to prevent overtreatment with albumin.
Discussion
Two recent meta-analyses have raised questions regarding the safety of both albumin specifically [2] and colloids generally [1]. Mortality was adopted as the endpoint of these meta-analyses based upon RCTs involving various critical illnesses and fluid regimens. There was nevertheless no statistically significant difference in mortality between hypovolaemic patients in the albumin and control groups [2]. Similarly, mortality did not differ significantly between the colloid and control groups in RCTs involving trauma, surgery, burns and other indications [1]. Thus, neither meta-analysis provides convincing evidence that resuscitation is more hazardous with a colloid than a crystalloid. Furthermore, the RCTs included in both meta-analyses were strikingly heterogeneous with respect to indications for fluid administration, patient population, and resuscitation regimen. No attempt was made to exclude RCTs involving obvious colloid overload, which would be expected to contribute to adverse outcomes. Some unpublished data were included. The meta-analyses, importantly, also did not adequately address plausible mechanisms upon which potential mortality differences might be based. It is consequently difficult to draw unequivocal inferences from the meta-analyses.
Colloids are clearly more efficient than crystalloids in attaining resuscitation endpoints, since much less fluid volume is required. The Starling equation provides a theoretical basis for the expectation that colloids will be less likely than crystalloids to contribute to interstitial oedema and deleterious sequelae thereof. The clinical significance of this theoretical difference in the properties of resuscitation fluids nevertheless remains to be established. Although recent data in cirrhosis patients suggest that albumin may, at least in certain clinical settings, reduce morbidity and mortality, present evidence supporting the ability of albumin or other colloids to improve such clinical outcomes in a broad range of patients is inadequate and inconclusive.
Albumin remains the standard of comparison for colloids, and this natural colloid offers certain advantages over artificial alternatives. The cost of albumin, however, places limitations on its use.
What approaches to fluid management are appropriate in light of the evidence reviewed? Crystalloids are clearly suitable as first-line fluids in the hypovolaemic patient. Colloids can be considered in cases of severe or acute shock or hypovolaemia resulting from sudden plasma loss. A combined regimen of crystalloid and colloid may also be useful for patients who might require large volumes of crystalloid alone.
Current understanding of the advantages and limitations associated with different resuscitation fluids remains far from complete. Further studies are needed to address the unresolved issues in fluid management. For instance, some useful answers might be furnished by further clinical trials comparing crystalloids with natural and artificial colloids with respect to pulmonary side effects such as fluid accumulation and permeability, as measured using radiolabelled proteins or albumin, following a given intravascular fluid challenge to a target PAWP.
Conclusion
Crystalloids are appropriate as first-line resuscitation fluid in patients with hypovolaemia. Colloids may be considered in patients with severe or acute shock or hypovolaemia due to sudden plasma loss. It may be useful, since the volume of crystalloid needed to achieve resuscitation endpoints exceeds that of colloid by two- to threefold, to combine a colloid with a crystalloid in the fluid management regimen of patients who might require large volumes of crystalloid alone. Further studies are needed to define the comparative merits of particular resuscitation fluids.
Commentary
Jean-Louis Vincent, MD, PhD: What are the patient populations that might be enrolled in clinical trials of respiratory function in relation to resuscitation fluid?
AB Johan Groeneveld, MD: Patients with established ARDS and others with risk factors for ARDS such as sepsis, trauma, or surgery. Membrane permeability will be increased in the cases of established ARDS, and differences between colloids and crystalloids may not be demonstrable in this indication, although there is the possibility that some types of artificial colloids might exert a sealant effect on the membranes.
Uwe Kreimeier, MD: The distinct properties of particular colloids such as albumin, dextran, hetastarch, and gelatin are well recognized. It may also be important to differentiate between particular crystalloids, for example with respect to effects on pH. In a recent study, rapid infusion of 0.9% saline but not Ringer's lactate resulted in hyperchloraemic acidosis among patients undergoing gynaecologic surgery [17]. So particularly if large volumes of crystalloid are to be infused, it is important to be aware of the potential of particular crystalloids to alter blood pH and possibly cause severe perturbations in blood flow.
Andrew R Webb, MD: Although COP is not routinely measured in most critical care settings, these measurements can be quite important in patients with renal failure on artificial renal support who are receiving artificial colloids, particularly hydroxyethyl starches. In that group of patients COP can become elevated, impairing glomerular filtration and prolonging the renal failure.
William J Sibbald, MD: At our institution, a RCT has been recently completed comparing pentastarch and albumin in cardiopulmonary bypass patients. The presumption was that the two fluids would prove equivalent. Indeed, with respect to nearly all postoperative endpoints, there were no significant between-group differences. However, the patients receiving pentastarch required on average 1.2 units more blood, even though no measurable coagulation defect was observed. The difference in blood requirement convinced our cardiac surgeons that albumin should remain the fluid of choice in these patients.
Chantilly, France. 15 October 1999
References
- Schierhout G, Roberts I. Fluid resuscitation with colloid or crystalloid solutions in critically ill patients: a systematic review of randomised trials. BMJ. 1998;316:961–964. doi: 10.1136/bmj.316.7136.961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cochrane Injuries Group Albumin Reviewers: Human albumin administration in critically ill patients: systematic review of randomised controlled trials. BMJ. 1998;317:235–240. doi: 10.1136/bmj.317.7153.235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sort P, Navasa M, Arroyo V. et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N Engl J Med. 1999;341:403–409. doi: 10.1056/NEJM199908053410603. [DOI] [PubMed] [Google Scholar]
- McGee S, Abernethy WB, Simel DL. Is this patient hypovolemic? JAMA. 1999;281:1022–1029. doi: 10.1001/jama.281.11.1022. [DOI] [PubMed] [Google Scholar]
- Rackow EC, Falk JL, Fein IA. et al. Fluid resuscitation in circulatory shock: a comparison of the cardiorespiratory effects of albumin, hetastarch, and saline solutions in patients with hypovolemic and septic shock. Crit Care Med. 1983;11:839–850. [PubMed] [Google Scholar]
- Packman MI, Rackow EC. Optimum left heart filling pressure during fluid resuscitation of patients with hypovolemic and septic shock. Crit Care Med. 1983;11:165–169. doi: 10.1097/00003246-198303000-00003. [DOI] [PubMed] [Google Scholar]
- Hauser CJ, Shoemaker WC, Turpin I, Goldberg SJ. Oxygen transport responses to colloids and crystalloids in critically ill surgical patients. Surg Gynecol Obstet. 1980;150:811–816. [PubMed] [Google Scholar]
- Lazrove S, Waxman K, Shippy C, Shoemaker WC. Hemodynamic, blood volume, and oxygen transport responses to albumin and hydroxyethyl starch infusions in critically ill postoperative patients. Crit Care Med. 1980;8:302–306. doi: 10.1097/00003246-198005000-00007. [DOI] [PubMed] [Google Scholar]
- Rackow EC, Fein IA, Siegel J. The relationship of the colloid osmotic-pulmonary artery wedge pressure gradient to pulmonary edema and mortality in critically ill patients. Chest. 1982;82:433–437. doi: 10.1378/chest.82.4.433. [DOI] [PubMed] [Google Scholar]
- Shires GT, Peitzman AB, Albert SA. et al. Response of extravascular lung water to intraoperative fluids. Ann Surg. 1983;197:515–519. doi: 10.1097/00000658-198305000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lowe RJ, Moss GS, Jilek J, Levine HD. Crystalloid vs colloid in the etiology of pulmonary failure after trauma: a randomized trial in man. Surgery. 1977;81:676–683. [PubMed] [Google Scholar]
- Weaver DW, Ledgerwood AM, Lucas CE. et al. Pulmonary effects of albumin resuscitation for severe hypovolemic shock. Arch Surg. 1978;113:387–392. doi: 10.1001/archsurg.1978.01370160045006. [DOI] [PubMed] [Google Scholar]
- Cope JT, Banks D, Mauney MC. et al. Intraoperative hetastarch infusion impairs hemostasis after cardiac operations. Ann Thorac Surg. 1997;63:78–82. doi: 10.1016/S0003-4975(97)00092-1. [DOI] [PubMed] [Google Scholar]
- Gall H, Kaufmann R, von Ehr M, Schumann K, Sterry W. Persistierender Pruritus nach Hydroxyäthylstärke-Infusionen: retrospektive Langzeitstudie an 266 Fällen. Hautarzt. 1993;44:713–716. [PubMed] [Google Scholar]
- Cittanova ML, Leblanc I, Legendre C. et al. Effect of hydroxyethylstarch in brain-dead kidney donors on renal function in kidney-transplant recipients. Lancet. 1996;348:1620–1622. doi: 10.1016/S0140-6736(96)07588-5. [DOI] [PubMed] [Google Scholar]
- Ring J, Messmer K. Incidence and severity of anaphylactoid reactions to colloid volume substitutes. Lancet. 1977;1:466–469. doi: 10.1016/S0140-6736(77)91953-5. [DOI] [PubMed] [Google Scholar]
- Scheingraber S, Rehm M, Sehmisch C, Finsterer U. Rapid saline infusion produces hyperchloremic acidosis in patients undergoing gynecologic surgery. Anesthesiology. 1999;90:1265–1270. doi: 10.1097/00000542-199905000-00007. [DOI] [PubMed] [Google Scholar]