

Abstract
Data from the Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) trial (N=2,802) were analyzed to examine whether word list learning predicts future everyday functioning. Using stepwise random effects modeling, measures from the modified administrations of the Hopkins Verbal Learning Test (HVLT) and the Auditory Verbal Learning Test (AVLT) were independently predictive of everyday IADL functioning, problem-solving, and psychomotor speed. Associations between memory scores and everyday functioning outcomes remained significant across follow-up intervals spanning five years. HVLT total recall score was consistently the strongest predictor of each functional outcome. Results suggest that verbal memory measures are uniquely associated with both current and future functioning and that specific verbal memory tests like the HVLT and AVLT have important clinical utility in predicting future functional ability among older adults.
Keywords: functional ability, HVLT, AVLT, verbal memory
Introduction
The ability to function independently in the community is important for most older adults (Grigsby, Kaye, Baxter, Shetterly, & Hamman, 1998). Everyday functioning declines with age, and functional impairment leads to adverse health care outcomes, such as nursing home admissions and hospitalizations (Fillenbaum, 1985; Fogel, Hyman, Rock, & Wolk-Klein, 2000). A variety of social, physical, and cognitive factors contribute to an individual’s ability to function independently (Galanos, Fillenbaum, Cohen, & Burchett, 1994; Galasko, 1998; Stuck, Walthert, Nikolaus, Bula, Hohmann, & Beck, 1999). Declines in cognitive abilities are associated with subsequent functional impairment (Stuck et al., 1999), and cognitive functioning has been shown to be a stronger predictor of capacity for daily activities than depression or health characteristics (Burdick, Rosenblatt, Samus, Steele, Baker, et al., 2005). Therefore, the ability to predict functional decline using cognitive tests is an active area of research (e.g., Schmitter-Edgecombe, Woo, & Greeley, 2009; Jefferson, Paul, Ozonoff, & Cohen, 2006). Neuropsychologists and other clinicians are frequently asked to assess a patient’s ability to live independently and make health care decisions (Galanos, Fillenbaum, Cohen, & Burchett, 1994; Rabin, Barr, & Burton, 2005). Because memory complaints are prevalent among older adults and memory assessment is central to the neuropsychology of evaluation of the elderly, this study will examine the ability of several memory tests to predict everyday functioning.
Everyday functional abilities
Everyday functional abilities refer to the general knowledge and skills needed to independently care for oneself in the community (Katz, Ford, Moskowitz, Jackson, & Jaffe, 1963; Loewenstein & Mogosky, 1999; Willis, 1996). A variety of methods, from self-report to objective task performance, are used to measure everyday functioning among older adults (Farias et al., 2003; Heaton et al., 2004). It is also important to carefully define the scope of functional abilities because particular abilities can have different associations with different predictors (Hertzog, Kramer, Wilson, & Lindenberger, 2008; Royall et al., 2007). Functioning may sometimes refer to multidimensional global capacities or to more specific abilities, such as driving a car or walking up steps (e.g., Hakamies-Blomqvist & Wahlstrom, 1998). In this study, everyday functional ability is conceptualized as consisting of three continuously distributed constructs: instrumental activities of daily living (IADL) functioning, problem-solving ability, and psychomotor speed. Each construct is measured with validated, objective tools that are either performance-based or self-reported.
Functional ability can be assessed by asking about one’s ability to perform IADLs such as preparing food, managing money, and other important everyday activities (Lawton & Brody, 1969; Richardson et al., 1995; Royall et al., 2007). In addition to self-reports of one’s ability to perform certain tasks, objective measures of performance on physical and cognitive tasks important to occupational and everyday functioning are also available (e.g., Nadler, Richardson, & Malloy, 1993; Willis & Marsiske, 1993). Two other aspects of everyday functioning are everyday cognition and psychomotor speed of cognitive processing. Everyday cognition refers to the application of domain-specific knowledge and mental abilities to solving problems common in complex real-world contexts, and so measures everyday problem-solving should assess skills that older adults need to adapt to everyday living (Allaire & Marsiske, 1999; 2002; Eysenck & Keane, 1995). In laboratory-based tests of everyday cognition, problem difficulty varies by the extent to which circumstances surrounding the goal or the process of reaching the goal are well-defined or ill-defined (Allaire & Marsiske, 2002). Mental processing speed refers to the time it takes to process a stimulus and respond to that stimulus; it is an important cognitive resource for handling information (Botwinick, Brinley, & Birren, 1957; Kramer & Madden, 2008). Mental processing slows with age and can be measured with combinations of simple and complex reaction time tasks (Salthouse, 1991).
Cognitive predictors of everyday functioning
The predictive validity of particular neuropsychological tests in cognitively normal older adults has not been studied in great detail (Spooner & Pachana, 2006). There are many potential cognitive predictors of everyday functioning, including global predictors such as the Mini-Mental State Exam (MMSE) and more specific constructs like executive functioning, speed of processing, and memory (Burton et al., 2006; Folstein, Folstein, & McHugh, 1975; Royall et al., 2007). Global cognitive function has been shown to be a strong predictor of functional impairment (Burdick et al., 2005), and domain-specific neuropsychological tests have been found to be associated with concurrent functional ability and decline (Stuck et al., 1999). Van der Elst, Van Boxtel, Van Breukelen, and Jolles (2008) reported a general cognitive composite that was the strongest predictor of several measures of everyday functioning, but also an executive functioning composite that independently explained up to 20% of the variance in some functioning measures. Measures of executive function such as Part B of the Trail Making Test and working memory predict IADL impairment and even subsequent dementia among older adults (Aretouli & Brandt, 2010; Bell-McGinty, Podell, Franzen, Baird, & Williams, 2002; Cahn-Weiner, Boyle, & Malloy, 2002; Royall et al., 2007).
Verbal episodic memory has also been shown to be associated with functioning, although, to date, few studies have comprehensively examined the ability of verbal memory to predict a wide variety of IADL measures. In a critical review of existing research, Royall et al. (2007) reported that memory variables explained on average 1.9% of the variance in functional outcomes. The Hopkins Verbal Learning Test (HVLT) was the best single memory predictor (R2=9%). Allaire and Marsiske (2002) reported that a verbal declarative memory factor, composed of the sum of HVLT learning trials 1, 2, and 3, was associated with everyday cognition (standardized effect size = 0.22). This factor was, in turn, statistically significantly associated with self-rated everyday functioning in a sample of community-residing older adults.
Few prospective studies have examined the relationship between memory and future functioning (but see Sliwinski, Stawski, Hall, Katz, Verghese, & Lipton, 2006 and Van der Elst et al., 2008). The ability of memory to predict future functioning affords the opportunity to anticipate future care needs, thereby helping older adults and their families to plan ahead. Identifying the best predictors of functioning can also inform neuropsychologists and cognitive researchers who are frequently asked about a patient’s ability to function independently given results from cognitive tests. It is also important to see if the strength of the relationship between memory and future functioning differs as a function of interval between measurements of the two.
The current study’s purpose was to examine the independent contributions of verbal memory tests in predicting three aspects of current and future everyday functional ability: everyday IADL functioning, problem-solving ability, and psychomotor speed. It was hypothesized that word list recall, and particularly tests relying more on semantic processing to organize the words during encoding and retrieval, would predict everyday functioning. Second, the predictive value of memory assessed at different time intervals between specific verbal memory measures and everyday functional abilities was assessed. A third goal was to examine if cognitive training interventions modified the relationships between any episodic memory measure and everyday functioning. It was hypothesized that, if memory is predictive of functioning, cognitive training specifically in memory but not other domains would modify the relationship between memory and functional ability. We addressed these questions using data from a large sample of community-dwelling older adults who were part of the Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) cohort.
Methods
Study population
The ACTIVE study is a large multi-center, controlled, randomized trial of cognitive training in older adults. Community-dwelling adults age 65 and over (N=2,802) were recruited from six metropolitan sites across the United States and randomized to one of three types of cognitive interventions: memory, reasoning, or speed of information processing training. A no-contact control group comprised a fourth group. Further details of the study design and recruitment strategy are described elsewhere (Ball et al., 2002; Jobe et al., 2001; Willis et al., 2006). The memory training intervention involved practicing several mnemonic strategies, such as organization, association, visualization, and the method of loci. Participants in the reasoning training condition were taught strategies for identifying patterns from a series of letters, words, and other items. Participants in the speed of processing condition were trained to more quickly search and identify objects on a computer screen in divided attention contexts. Each intervention was administered in 10 small-group training sessions, each lasting 60 to 75 minutes, offered over the course of six weeks. Data used in this analysis were taken from participants assessed at baseline and followed up at immediate post-test, and at 1 year, 2 years, 3 years, and 5 years after the initial training.
Outcome measures
The influence of memory performance at baseline on three composite measures of everyday functioning – IADL functioning, problem-solving, and psychomotor speed – was investigated. Each outcome was constructed from either one score or two component test scores that were standardized at each time point to their baseline mean and standard deviation, weighted to be equal, and averaged. These Blom-transformed variables have been used previously to describe aspects of functional ability (Blom, 1958; Willis et al., 2006). Everyday IADL functioning was measured by the self-reported IADL difficulty subscore from the Minimum Dataset - Home Care (MDS-HC) which assesses performance in the past 7 days on a variety of IADL functions (Morris, Fries, Steel, Ikegami, Bernabei, et al., 1997; Teresi, Lawton, Holmes, & Ory, 1997). An everyday problem-solving score was constructed from two measures, the Everyday Problems Test (EPT) and the Observed Tasks of Daily Living (OTDL). The EPT assesses cognitive IADLs with 15 sets of common comprehension and reasoning tasks that older adults encounter in a typical day, such as reading medication labels, recipes, and telephone bills (Willis & Marsiske, 1993). The OTDL is a performance-based test of cognitive functioning that involves assorted tasks including nutrition, telephone use, and checkbook balancing (Diehl, Marsiske, Horgas, Rosenberg, Saczynski, et al., 2005). Psychomotor speed was measured by a composite score from the Timed IADL (TIADL) test and Complex Reaction Time (CRT) test (Ball, 2000; Owsley et al., 2002). Each composite outcome was adjusted so that higher scores indicate better functioning.
Verbal episodic memory predictors
Four measures were used to describe verbal episodic memory, two of which were derived from the Auditory Verbal Learning Test (AVLT) and two from the Hopkins Verbal Learning Test (HVLT). The HVLT uses a 12-word list consisting of three sets of four semantically related words repeated three times to participants (Brandt, 1991; Brandt & Benedict, 2001). In a modification to the test’s standard administration, the word lists were presented via audiotape and participants were asked to write down as many words as they could after each trial. The AVLT uses a 15-word list composed of unrelated words repeated over five trials in a similar fashion, after which an interference list and short-tern recall trial were given (Rey, 1941; Schmidt, 2004). For both instruments, recall trials were followed after a delay by a recognition trial on which participants were asked to discriminate between words from the recall list and distractor words. Both the total recall and recognition discrimination scores were used from each test. The HVLT and AVLT total recall scores were the sum of three recall trials and five recall trials, respectively. The discrimination score in each case was calculated as the difference between the number of true positive recognitions (“hits”) and the number of false positive recognitions (“false alarms”). Each score was standardized so that coefficient magnitudes from statistical models would be comparable. A verbal memory composite score was not constructed to summarize these four measures because the primary motivation behind this study was to investigate the extent to which particular measures from these specific word list memory tests are useful in clinical contexts for predicting current and future functional ability among older adults.
Other covariates
To account for potential confounding, age, sex, race, years of education, intervention group, and assessment time were included in models. Age was centered at 70 years, and education was coded continuously in years and centered at 12 years. A baseline measure of vocabulary knowledge was used to represent global cognitive ability, and was converted to a z-score to be comparable in scale with the verbal memory measures. Because of the unequal spacing between ACTIVE assessments, follow-up visits were treated categorically in models rather than continuously. The ACTIVE study design included booster training at 11 and 35 months after the initial training for about 50% of participants in each training group, but booster status was not considered here because prior analyses have shown no effects from booster training on memory outcomes (Ball et al., 2002; Willis et al., 2006).
Analysis plan
Descriptive analyses were carried out on the study sample. The main analysis was then conducted in three phases. In the first phase, a series of stepwise random intercept models were implemented to evaluate the predictive ability of each of the four verbal memory measures (HVLT and AVLT total recall and recognition discrimination scores) for each of the three baseline functional outcomes of everyday IADL functioning, problem-solving, and psychomotor speed (Laird & Ware, 1982). Random intercept models use all available data, account for within-person homogeneity that arises from repeated measures on the same people over the study period, and accommodate data that are missing at random (Donders et al., 2006). Unobserved heterogeneity between persons is represented by person-specific latent intercepts that enable the total outcome variance to be partitioned into within-subjects and between-subjects components (Cnaan, Laird, & Slasor, 1997; Rabe-Hesketh & Skrondal, 2008). The basic random intercept model is written below:
There are three functioning outcomes and four separate memory measures, resulting in 12 such models. In the equation above, person i’s functioning outcome at time j is a function of a common intercept β0 and a subject-specific intercept U1i, a series of person-specific covariates, and a random error εij for each person at each time. The random intercept U1i is assumed to be normally distributed in the population, and the random error εij is assumed to be normally distributed with a variance σ2 around mean 0. Slope coefficients that are significantly associated with a functioning score would indicate the covariate is associated with person-specific changes in the score over time.
Adding observation-level covariates such as vocabulary score or a verbal memory measure to a model reduces the between-subjects variance in the predicted value of the outcome, meaning that prospectively measured outcomes five years in the future will be better predicted (Cnaan, Laird, & Slasor, 1997). This predictive ability can be quantified by a coefficient of determination (R2), which quantifies the proportionate reduction in the between-subjects variance of each functional outcome explained by adding covariates to a nested model. To estimate coefficients of determination, each functional composite was first regressed on categorical indicators for assessment time. This served as a null model. The four standardized verbal memory scores were then added separately to estimate the proportion of between-subjects variance independently attributable to each measure above and beyond that accounted for by time (step 1). Second, the baseline standardized vocabulary score was added to these models to estimate the R2 attributable to global cognitive status (step 2). In a final step, demographic characteristics were added to examine their contribution to the prediction of each functioning variable (step 3). These steps were performed separately for each functional outcome.
For the second analysis phase, we investigated the strength of associations between episodic memory measures and prospectively collected future functional ability as remote as five years later. Everyday functioning measures from follow-up assessments at 1, 2, 3, and 5 years after training were regressed on baseline verbal memory measures using linear regressions.
In a third analysis phase, we tested whether any of the ACTIVE cognitive training interventions modified the relationship between episodic memory and everyday functional abilities. Interaction terms were added between indicator variables for cognitive training condition, time, and each standardized verbal memory test score in random coefficient models with everyday problem-solving, IADL functioning, or psychomotor speed as outcomes. These interactions tested whether the relationship between verbal memory measures and functional ability differed as a function of cognitive training condition at each point in time. All combinations of two-way interactions between time, test, and training group were also included.
Results
Baseline demographic characteristics and test scores are shown in Table 1. Memory measures and composite functional ability did not differ by training status at baseline (all p>0.98). The proportion of data missing over time was not significantly associated with any cognitive variables, training status, or demographic characteristics except for older age. Therefore, all analyses were conducted with observed cases without imputed data.
Table 1.
Baseline characteristics and test scores of the Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) cohort
| ACTIVE Cohort (N=2,802) | Range | |
|---|---|---|
| Age, mean (SD) | 73.6 (5.9) | 65, 94 |
| Years of Education, mean (SD) | 13.5 (2.7) | 4, 20 |
| Sex, n % female | 2,126 (76%) | |
| Race, n % white | 2,042 (73%) | |
| Training Group, n | ||
| Memory Training | 703 (25%) | |
| Reasoning Training | 699 (25%) | |
| Speed Training | 702 (25%) | |
| Control | 698 (25%) | |
| Baseline Cognitive Measures, mean (SD) | ||
| MMSE | 27.3 (2.0) | 23, 30 |
| Vocabulary | 12.4 (3.9) | 0, 18 |
| AVLT | ||
| Sum of Trials 1-5 | 48.5 (10.6) | 6, 73 |
| Recognition Discrimination | 8.4 (5.8) | -18, 15 |
| HVLT | ||
| Sum of Trials 1-3 | 25.9 (5.5) | 1, 36 |
| Recognition Discrimination | 10.5 (1.8) | -6, 12 |
| Baseline Functioning measures, mean (SD) | ||
| Everyday IADL functioning | 0 (2.0) | -2.5, 8.6 |
| MDS-HC (raw) | 4.3 (4.9) | 0, 26 |
| Everyday problem-solving | 0 (1.8) | -5.9, 5.30 |
| EPT (raw) | 18.6 (5.7) | 0, 28 |
| OTDL (raw) | 17.6 (4.4) | 1, 28 |
| Everyday problem-solving | 0 (2.5) | -8.8, 9.1 |
| CRT (raw) | 0.30 (0.89) | -3.4, 3.5 |
| TIADL (raw) | 0.069 (1.02) | -3.9, 3.3 |
Are verbal memory measures predictive of functional ability?
All verbal memory measures were significant predictors of each functional outcome. Coefficient magnitudes in Tables 2, 3, and 4 are interpretable as the expected change in an individual’s outcome for a one standard deviation change in the cognitive predictor. In general, the HVLT total recall score consistently emerged as the best verbal memory predictor for each functional outcome, and its association with each outcome was the least attenuated after accounting for global cognition. The prediction of each everyday functioning measure improved across the board by between 7% and 22% when non-cognitive demographic variables were included.
Table 2.
Predictive associations with everyday functioning among older adults: Data from the ACTIVE Study (N=2,802)
| Everyday Functioning | |||||
|---|---|---|---|---|---|
| Step and Predictor | β (95% CI) | Adjusted R2 | Incremental Adjusted R2 | -2LL | |
| 1a | HVLT Trials 1-3 | ||||
| Unadjusted | 0.08 (0.07, 0.09) | 8.28% | 41376.7 | ||
| 2a | 8.93% | 0.65% | 41242.5 | ||
| Adjusted for Vocabulary | 0.09 (0.08, 0.10) | ||||
| Vocabulary | -0.14 (-0.22, -0.07) | ||||
| 3a | |||||
| Adjusted for Global Cognition, Demographics | 0.05 (0.04, 0.07) | 16.29% | 7.36% | 41042.6 | |
| 1b | HVLT Recognition Discrimination | ||||
| Unadjusted | 0.18 (0.14, 0.21) | 3.35% | 46251.3 | ||
| 2b | 3.42% | 0.07% | 46128.5 | ||
| Adjusted for Vocabulary | 0.18 (0.14, 0.21) | ||||
| Vocabulary | 0.01 (-0.06, 0.08) | ||||
| 3b | |||||
| Adjusted for Global Cognition, Demographics | 0.09 (0.05, 0.13) | 13.55% | 10.13% | 45854.9 | |
| 1c | AVLT Trials 1-5 | ||||
| Unadjusted | 0.05 (0.04, 0.05) | 8.16% | 45895.5 | ||
| 2c | 8.50% | 0.34% | 45794.6 | ||
| Adjusted for Vocabulary | 0.05 (0.04, 0.05) | ||||
| Vocabulary | -0.08 (-0.15, -0.01) | ||||
| 3c | |||||
| Adjusted for Global Cognition, Demographics | 0.03 (0.02, 0.04) | 15.41% | 6.91% | 45593.3 | |
| 1d | AVLT Recognition Discrimination | ||||
| Unadjusted | 0.06 (0.05, 0.07) | 4.14% | 46017.2 | ||
| 2d | 4.40% | 0.26% | 45955.5 | ||
| Adjusted for Vocabulary | 0.06 (0.05, 0.07) | ||||
| Vocabulary | -0.05 (-0.13, 0.02) | ||||
| 3d | |||||
| Adjusted for Global Cognition, Demographics | 0.04 (0.02, 0.05) | 13.78% | 9.38% | 45688.9 | |
Table 3.
Predictive associations with everyday problem-solving among older adults: Data from the ACTIVE Study (N=2,802)
| Everyday Problem-solving | |||||
|---|---|---|---|---|---|
| Step and Predictor | β (95% CI) | Adjusted R2 | Incremental Adjusted R2 | -2LL | |
| 1a | HVLT Trials 1-3 | ||||
| Unadjusted | 0.17 (0.16, 0.18) | 37.25% | 29919.6 | ||
| 2a | 52.49% | 15.24% | 29247.6 | ||
| Adjusted for Vocabulary | 0.13 (0.12, 0.14) | ||||
| Vocabulary | 0.67 (0.62, 0.72) | ||||
| 3a | |||||
| Adjusted for Global Cognition, Demographics | 0.09 (0.08, 0.10) | 62.99% | 10.50% | 28688.8 | |
| 1b | HVLT Recognition Discrimination | ||||
| Unadjusted | 0.33 (0.29, 0.36) | 12.98% | 33928.3 | ||
| 2b | 42.88% | 29.90% | 32817.5 | ||
| Adjusted for Vocabulary | 0.23 (0.20, 0.26) | ||||
| Vocabulary | 0.88 (0.83, 0.93) | ||||
| 3b | |||||
| Adjusted for Global Cognition, Demographics | 0.14 (0.12, 0.17) | 58.42% | 15.55% | 32028.8 | |
| 1c | AVLT Trials 1-5 | ||||
| Unadjusted | 0.08 (0.07, 0.08) | 26.04% | 33334.1 | ||
| 2c | 48.99% | 22.96% | 32374.1 | ||
| Adjusted for Vocabulary | 0.06 (0.05, 0.06) | ||||
| Vocabulary | 0.79 (0.74, 0.84) | ||||
| 3c | |||||
| Adjusted for Global Cognition, Demographics | 0.04 (0.03, 0.04) | 60.45% | 11.46% | 31744.6 | |
| 1d | AVLT Recognition Discrimination | ||||
| Unadjusted | 0.15 (0.14, 0.16) | 28.36% | 33266.1 | ||
| 2d | 48.91% | 20.55% | 32414.9 | ||
| Adjusted for Vocabulary | 0.10 (0.09, 0.11) | ||||
| Vocabulary | 0.76 (0.71, 0.80) | ||||
| 3d | |||||
| Adjusted for Global Cognition, Demographics | 0.07 (0.06, 0.08) | 60.38% | 11.47% | 31774.8 | |
Table 4.
Predictive associations with everyday psychomotor speed among older adults: Data from the ACTIVE Study (N=2,802)
| Everyday Speed | |||||
|---|---|---|---|---|---|
| Step and Predictor | β (95% CI) | Adjusted R2 | Incremental Adjusted R2 | -2LL | |
| 1a | HVLT Trials 1-3 | ||||
| Unadjusted | 0.24 (0.23, 0.26) | 30.48% | 44123.5 | ||
| 2a | 33.49% | 3.00% | 43905.1 | ||
| Adjusted for Vocabulary | 0.22 (0.20, 0.23) | ||||
| Vocabulary | 0.45 (0.36, 0.53) | ||||
| 3a | |||||
| Adjusted for Global Cognition, Demographics | 0.15 (0.14, 0.17) | 49.12% | 15.63% | 43271.2 | |
| 1b | HVLT Recognition Discrimination | ||||
| Unadjusted | 0.50 (0.45, 0.55) | 13.17% | 49559.2 | ||
| 2b | 22.90% | 9.74% | 49135.4 | ||
| Adjusted for Vocabulary | 0.42 (0.37, 0.46) | ||||
| Vocabulary | 0.76 (0.68, 0.85) | ||||
| 3b | |||||
| Adjusted for Global Cognition, Demographics | 0.26 (0.21, 0.30) | 44.82% | 21.92% | 48260.2 | |
| 1c | AVLT Trials 1-5 | ||||
| Unadjusted | 0.12 (0.11, 0.12) | 25.87% | 48875.2 | ||
| 2c | 31.71% | 5.84% | 48581.8 | ||
| Adjusted for Vocabulary | 0.10 (0.09, 0.11) | ||||
| Vocabulary | 0.60 (0.52, 0.69) | ||||
| 3c | |||||
| Adjusted for Global Cognition, Demographics | 0.07 (0.06, 0.08) | 48.23% | 16.52% | 47861.3 | |
| 1d | AVLT Recognition Discrimination | ||||
| Unadjusted | 0.19 (0.18, 0.21) | 21.72% | 49050.9 | ||
| 2d | 27.22% | 5.50% | 48807.5 | ||
| Adjusted for Vocabulary | 0.16 (0.15, 0.17) | ||||
| Vocabulary | 0.59 (0.51, 0.68) | ||||
| 3d | |||||
| Adjusted for Global Cognition, Demographics | 0.10 (0.08, 0.11) | 45.49% | 18.27% | 48041.7 | |
HVLT and AVLT recall sum scores independently accounted for 8% of the between-subjects variance in IADL functioning and the recognition discrimination scores accounted for about 4% of the variance (Table 2). Global cognitive status made a small contribution to the prediction of this outcome (incremental adjusted R2<1%; Table 2). Models containing demographic variables explained an extra 7% to 10% of the variance in everyday IADL functioning. Similar analyses for everyday problem-solving revealed that memory predictors were responsible for 13% to 37% of the between-subjects variance in the outcome, with the HVLT recall sum score independently explaining the most variance (Table 3). Global cognition enhanced the predictive value, particularly for verbal memory predictors that were independently weaker predictors of the outcome. Global cognition and verbal memory predictors together explained approximately 50% of the between-subjects variance in everyday problem-solving (Table 3). In the final steps for each cognitive predictor of everyday problem-solving (step 3), approximately 60% of the between-subjects variance was explained by these measures together with demographic characteristics. Associations with everyday psychomotor speed followed a similar pattern in that the HVLT recall sum score was the best predictor of the outcome and demographic characteristics explained an extra 18% of the variance above and beyond cognitive predictors (Table 4).
Are verbal memory measures predictive of future functional ability?
Coefficients of determination at each time between episodic verbal memory measure and each functional domain 1, 2, 3, and 5 years after the baseline measurement are shown in Figure 1, which has panels for each outcome. Everyday IADL functioning was poorly predicted by all verbal memory measures at each time interval. HVLT total recall was the best predictor of both everyday problem-solving and psychomotor speed at all time intervals. The coefficient of determination for psychomotor speed declined over time for each memory predictor. There was no such decline in predictive value for everyday problem-solving.
Figure 1.
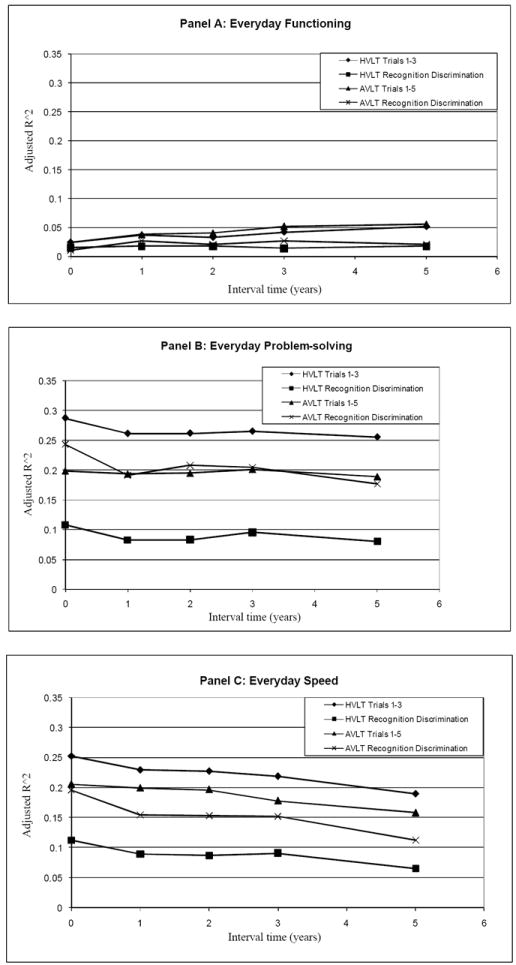
Interval associations between functional ability and HVLT and AVLT measures: Data from the ACTIVE Study (N=2,802)
Note. Coefficients are interpretable as changes in functional ability domain score for every 1 SD change in cognitive score.
Did ACTIVE training programs modify predictive strengths of verbal memory measures?
Separately for everyday IADL functioning, problem-solving, and psychomotor speed, random coefficient models were next fit with three-way interaction terms between training status, time, and memory test scores in order to test for effect modification by training status at each time point. Models adjusted for age, sex, education, race, and vocabulary score. We found no consistently significant relationships between any particular memory tests for any functional outcome. This replicates prior findings from ACTIVE (Willis et al., 2006).
Discussion
This study’s objective was to investigate the association of memory tests with three domains of prospectively measured everyday functioning. We showed that measures from modified administrations of the HVLT and AVLT list-learning tests are predictors of a variety of performance-based measures of everyday problem-solving and psychomotor speed assessed across five years in community-dwelling older adults. These relationships were maintained even after accounting for global cognitive status. Non-cognitive demographic characteristics improved the prediction of everyday functioning by between 7% and 22% across all outcomes and predictors. This study builds on previous research showing that verbal memory is associated with concurrent functional ability by demonstrating that verbal memory measures, particularly the HVLT, are also predictive of future functional ability. The HVLT recall score was the strongest predictor of each functional outcome. Significant associations between verbal memory and future functioning persisted in this sample for five years. No type of cognitive training altered the relationship between verbal memory and functional ability.
The everyday tasks measured with instruments like the EPT, OTDL, and TIADL are much more cognitively complex than the abilities measured by individual neuropsychological tests. This study’s findings are consistent with the hypothesis that verbal memory makes a significant contribution to the prediction of problem-solving and psychomotor speed elements of everyday functioning. All verbal memory measures together with global cognition explained 55% and 40% of the variance in everyday problem-solving and psychomotor speed, respectively, although no combination of predictors explained more than 16% of the variance in everyday IADL functioning. Memory has obvious roles in everyday function, from the need to monitor sequences of actions to awareness of past decisions when evaluating future options (Shallice & Burgess, 1996; Zanini, Rumiati, & Shallice, 2002). In the face of a physical disability, good memory can help an individual maintain independence for longer periods than otherwise expected.
ACTIVE included a large, diverse sample of older adults, and so findings should be generalizable to older community-dwelling adults. Prospectively collected measures for the exposure and outcome provide robust support for our findings. In light of these strengths, several limitations are important to mention. Significant functional decline was seen in the ACTIVE sample by the fifth year (Willis et al., 2006), but our findings may not generalize to more disabled older adults. Verbal episodic memory measures may not be as strongly associated with functional ability in such populations, or components of functioning may be less associated with memory.
This study has important clinical and research implications. Ecological validity refers to the degree of correspondence between neuropsychological test performance and everyday functioning in real-world situations, and it is important to identify neuropsychological measures that are ecologically valid (Sbordone, 1996). Clinicians are often limited by the amount of time they can spend with patients, and older adults characteristically show wide variability not only in health status, but also in disease presentation. Memory function can be a robust indicator of future functional capacity, and so neuropsychological testing of memory in unimpaired older adults may be a productive endeavor. The HVLT is a relatively brief, easy test to administer, and perhaps better tolerated by patients than other memory tests. Future research should seek to replicate our findings among more disabled older adults as well as those with more prospectively observed functional decline.
Acknowledgments
Dr. Rebok is a consultant for Compact Disc Incorporated (CDI), which is at this time in the process of developing an electronic version of the ACTIVE memory training program. He has received no financial support from them for ACTIVE. Dr. Brandt receives royalty income from Psychological Assessment Resources, Inc., on sales of the Hopkins Verbal Learning Test-Revised. Inferences expressed here are those of the authors and are not necessarily reflective of the academic or funding agencies involved.
Funding This work was supported by grants from the National Institute on Aging and the National Institute of Nursing Research to Hebrew Senior Life (U01NR04507), Indiana University School of Medicine (U01 NR04508), Johns Hopkins University (U01AG14260), New England Research Institutes (U01AG14282), Pennsylvania State University (U01AG14263), the University of Alabama at Birmingham (U01 AG14289), and the University of Florida (U01AG14276).
Footnotes
Drs. Rebok’s and Brandt’s relationships are managed by the Johns Hopkins University according to its established conflict of interest policies
References
- Albert M. The neuropsychology of the development of Alzheimer’s disease. In: Craik FIM, Salthouse TA, editors. The Handbook of aging and cognition. 4. London: Academic Press; 2008. pp. 97–132. [Google Scholar]
- Allaire JC, Marsiske M. Everyday cognition: age and intellectual ability correlates. Psychology and Aging. 1999;14:627–644. doi: 10.1037//0882-7974.14.4.627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allaire JC, Marsiske M. Well– and ill–defined measures of everyday cognition: relationship to older adults’ intellectual ability and functional status. Psychology and Aging. 2002;17:101–115. doi: 10.1037/0882-7974.17.1.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aretouli E, Brandt J. Everyday functioning in mild cognitive impairment and its relationship with executive cognition. International Journal of Geriatric Psychiatry. 2010;25:224–233. doi: 10.1002/gps.2325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ball K. Increased mobility and reducing accidents of older drivers. In: Schaie K, Pietrucha M, editors. Mobility and transportation in the elderly. Vol. 5. New York, NY: Springer; 2000. [Google Scholar]
- Ball K, Berch DB, Helmers KF, Jobe JB, Leveck MD, Marsiske M, et al. Effects of cognitive training interventions with older adults: A randomized controlled trial. Journal of the American Medical Association. 2002;288:2271–2281. doi: 10.1001/jama.288.18.2271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bell–McGinty S, Podell K, Franzen M, Baird AD, Williams MJ. Standard measures of executive function in predicting instrumental activities of daily living in older adults. International Journal of Geriatric Psychiatry. 2002;17:828–834. doi: 10.1002/gps.646. [DOI] [PubMed] [Google Scholar]
- Blom G. Statistical estimates and transformed beta variables. New York: John Wiley & Sons, Inc; 1958. [Google Scholar]
- Botwinick J, Brinley JF, Birren JE. Set in relation to age. Journal of Gerontology. 1957;12:300–305. doi: 10.1093/geronj/12.3.300. [DOI] [PubMed] [Google Scholar]
- Brandt J. The Hopkins Verbal Learning Test: development of a new memory test with six equivalent forms. The Clinical Neuropsychologist. 1991;5:125–142. [Google Scholar]
- Brandt J, Benedict RHB. Hopkins Verbal Learning Test–Revised: Professional manual. Odessa, FL: Psychological Assessment Resources; 2001. [Google Scholar]
- Burdick DJ, Rosenblatt A, Samus QM, Steele C, Baker A, Harper M, et al. Predictors of Functional Impairment in Residents of Assisted–Living Facilities: The Maryland Assisted Living Study. The Journals of Gerontology: Series A, Biological Sciences and Medical Sciences. 2005;60:258–264. doi: 10.1093/gerona/60.2.258. [DOI] [PubMed] [Google Scholar]
- Burton CL, Strauss E, Hultsch DF, Hunter MA. Cognitive functioning and everyday problem solving in older adults. The Clinical Neuropsychologist. 2006;20:432–452. doi: 10.1080/13854040590967063. [DOI] [PubMed] [Google Scholar]
- Cahn–Weiner DA, Boyle PA, Malloy PF. Tests of executive function predict instrumental activities of daily living in community–dwelling older individuals. Applied Neuropsychology. 2002;9:187–191. doi: 10.1207/S15324826AN0903_8. [DOI] [PubMed] [Google Scholar]
- Cnaan A, Laird NM, Slasor P. Using the general linear mixed model to analyse unbalanced repeated measures and longitudinal data. Statistics in Medicine. 1997;16:2349–2380. doi: 10.1002/(sici)1097-0258(19971030)16:20<2349::aid-sim667>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- Diehl M, Marsiske M, Horgas AL, Rosenberg A, Saczynski J, Willis SL. The Revised Observed Tasks of Daily Living: a performance–based assessment of everyday problem solving in older adults. Journal of Applied Gerontology. 2005;24:211–230. doi: 10.1177/0733464804273772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donders AR, van der Heijden GJ, Stijnen T, Moons KG. Review: A gentle introduction to imputation of missing values. Journal of Clinical Epidemiology. 2006;59:1087–1091. doi: 10.1016/j.jclinepi.2006.01.014. [DOI] [PubMed] [Google Scholar]
- Eysenck MW, Keane MT. Cognitive psychology: A Student’s handbook. Hillsdale, NJ: Erlbaum; 1995. [Google Scholar]
- Farias ST, Harrell E, Neumann C, Houtz A. The relationship between neuropsychological performance and daily functioning in individuals with Alzheimer’s disease: Ecological validity of neuropsychological tests. Archives of Clinical Neuropsychology. 2003;18:655–672. [PubMed] [Google Scholar]
- Fillenbaum GG. Screening the elderly: A brief instrumental activities of daily living measure. Journal of the American Geriatrics Society. 1985;33:698–706. doi: 10.1111/j.1532-5415.1985.tb01779.x. [DOI] [PubMed] [Google Scholar]
- Fogel JF, Hyman RB, Rock B, Wolk–Klein G. Predictors of hospital length of stay and nursing home placement in an elderly medical population. Journal of the American Medical Directors Association. 2000;1:202–210. [PubMed] [Google Scholar]
- Folstein MF, Folstein SE, McHugh PR. “Mini–mental state”: A practical guide for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research. 1975;12:189–198. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- Galanos AN, Fillenbaum GG, Cohen HJ, Burchett BM. The comprehensive assessment of community dwelling elderly: why functional status is not enough. Aging. 1994;6:343–352. doi: 10.1007/BF03324263. [DOI] [PubMed] [Google Scholar]
- Galasko D. An integrated approach to the management of Alzheimer’s disease: Assessing cognition, function and behavior. European Journal of Neurology. 1998;5:S9–S27. [Google Scholar]
- Grigsby J, Kaye K, Baxter J, Shetterly SM, Hamman RF. Executive cognitive abilities and functional status among community–dwelling older persons in the San Luis Valley Health and Aging Study. Journal of the American Geriatrics Society. 1998;46:590–596. doi: 10.1111/j.1532-5415.1998.tb01075.x. [DOI] [PubMed] [Google Scholar]
- Hakamies–Blomqvist L, Wahlstrom B. Why do older drivers give up driving? Accident Analysis and Prevention. 1998;30:305–312. doi: 10.1016/s0001-4575(97)00106-1. [DOI] [PubMed] [Google Scholar]
- Heaton RK, Marcotte TD, Mindt MR, Sadek J, Moore DJ, Bentley H, et al. the HNRC group. The impact of HIV-associated neuropsychological impairment on everyday functioning. Journal of the International Neuropsychological Society. 2004;10:317–331. doi: 10.1017/S1355617704102130. [DOI] [PubMed] [Google Scholar]
- Hertzog C, Kramer AF, Wilson RS, Lindenberger U. Enrichment effects on adult cognitive development: Can the functional capacity of older adults be preserved and enhanced? Psychological Science in the Public Interest. 2008;9:1–65. doi: 10.1111/j.1539-6053.2009.01034.x. [DOI] [PubMed] [Google Scholar]
- Jefferson AL, Paul RH, Ozonoff A, Cohen RA. Evaluating elements of executive functioning as predictors of instrumental activities of daily living (IADLs) Archives of Clinical Neuropsychology. 2006;21:311–320. doi: 10.1016/j.acn.2006.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jobe JB, Smith DM, Ball K, Tennstedt SL, Marsiske M, Willis SL, et al. ACTIVE: A cognitive intervention trial to promote independence in older adults. Controlled Clinical Trials. 2001;22:453–479. doi: 10.1016/s0197-2456(01)00139-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged: the index of ADL: a standardized measure of biological and psychosocial functioning. Journal of the American Medical Association. 1963;185:914–919. doi: 10.1001/jama.1963.03060120024016. [DOI] [PubMed] [Google Scholar]
- Kramer AF, Madden DJ. Attention. In: Craik FIM, Salthouse TA, editors. The Handbook of Aging and Cognition. 4. London: Academic Press; 2008. pp. 189–250. [Google Scholar]
- Laird NM, Ware JH. Random effects models for longitudinal data: an overview of recent results. Biometrics. 1982;38:963–974. [PubMed] [Google Scholar]
- Lawton MP, Brody EM. Assessment of older people: self–maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179–186. [PubMed] [Google Scholar]
- Loewenstein DA, Mogosky BJ. The functional assessment of the older adult patient. In: Lichtenberg PA, editor. Handbook of assessment in clinical gerontology. New York: John Wiley & Sons, Inc; 1999. pp. 529–554. [Google Scholar]
- Morris JN, Fries BE, Steel K, Ikegami N, Bernabei R, Carpenter GI. Comprehensive clinical assessment in community setting: applicability of the MDS–HC. Journal of the American Geriatrics Society. 1997;45:1017–1024. doi: 10.1111/j.1532-5415.1997.tb02975.x. [DOI] [PubMed] [Google Scholar]
- Nadler JD, Richardson ED, Malloy PF. The ability of the Dementia Rating Scale to predict everyday functioning. Archives of Clinical Neuropsychology. 1993;8:449–460. [PubMed] [Google Scholar]
- Owsley C, Sloane M, McGwin G, Jr, Ball K. Timed instrumental activities of daily living tasks: relationship to cognitive function and everyday performance assessments in older adults. Gerontology. 2002;48:254–265. doi: 10.1159/000058360. [DOI] [PubMed] [Google Scholar]
- Rabe–Hesketh S, Skrondal A. Multilevel and longitudinal modeling using Stata. 2. College Station, TX: Stata Press; 2008. [Google Scholar]
- Rabin L, Burton L, Barr W. Utilization rates of ecologically oriented instruments among clinical neuropsychologists. The Clinical Neuropsychologist. 2007;21:727–743. doi: 10.1080/13854040600888776. [DOI] [PubMed] [Google Scholar]
- Rey A. L’examen psychologique dans les cas d’encephalopathie tramatique. Archives de Psychologie. 1941;28:286–340. [Google Scholar]
- Richardson ED, Nadler JD, Malloy PF. Neuropsychologic prediction of performance measures of daily living skills in geriatric patients. Neuropsychology. 1995;9:565–572. [Google Scholar]
- Royall DR, Lauterbach EC, Kaufer D, Malloy P, Coburn KL, Black KJ, et al. The cognitive correlates of functional status: A review from the Committee on Research of the American Neuropsychiatric Association. Journal of Neuropsychiatry and Clinical Neuroscience. 2007;19:249–265. doi: 10.1176/jnp.2007.19.3.249. [DOI] [PubMed] [Google Scholar]
- Salthouse TA. Theoretical perspectives on cognitive aging. Hillsdale, NJ: Lawrence Erlbaum Associates; 1991. [Google Scholar]
- Sbordone RJ. Ecological validity: Some critical issues for the neuropsychologist. In: Sbordone RJ, Long CJ, editors. Ecological validity of neuropsychological testing. Delray Beach, Florida: GR Press/St. Lucie Press; 1996. pp. 15–42. [Google Scholar]
- Schmidt M. Rey Auditory Verbal Learning Test: A handbook. Los Angeles, CA: Western Psychological Services; 2004. [Google Scholar]
- Schmitter–Edgecombe M, Woo E, Greeley DR. Characterizing multiple memory deficits and their relation to everyday functioning in individuals with mild cognitive impairment. Neuropsychology. 2009;23:168–177. doi: 10.1037/a0014186. [DOI] [PubMed] [Google Scholar]
- Shallice T, Burgess P. The domain of supervisory processes and temporal organization of behaviour. Philosophical Transactions of the Royal Society of London: Series B, Biological Sciences. 1996;351:1405–1411. doi: 10.1098/rstb.1996.0124. [DOI] [PubMed] [Google Scholar]
- Sliwinski MJ, Stawski RS, Hall CB, Katz M, Verghese J, Lipton R. Distinguishing preterminal and terminal cognitive decline. European Psychologist. 2006;11:172–181. [Google Scholar]
- Spooner DM, Pachana NA. Ecological validity in neuropsychological assessment: A case for greater consideration in research with neurologically intact populations. Archives of Clinical Neuropsychology. 2006;21:327–337. doi: 10.1016/j.acn.2006.04.004. [DOI] [PubMed] [Google Scholar]
- Stuck AE, Walthert JM, Nikolaus T, Büla CJ, Hohmann C, Beck JC. Risk factors for functional status decline in community–living elderly people: a systematic literature review. Social Science & Medicine. 1999;48:445–469. doi: 10.1016/s0277-9536(98)00370-0. [DOI] [PubMed] [Google Scholar]
- Teresi J, Lawton M, Holmes D, Ory M. Measurement in elderly chronic care populations. In: Morris J, Morris S, editors. ADL assessment measures for use with frail elders. New York, NY: Springer Publishing Co; 1997. [Google Scholar]
- Van der Elst W, Van Boxtel MPJ, Van Breukelen GJP, Jolles J. A large-scale cross-sectional and longitudinal study into the ecological validity of neuropsychological test measures in neurologically intact people. Archives of Clinical Neuropsychology. 2008;23:787–800. doi: 10.1016/j.acn.2008.09.002. [DOI] [PubMed] [Google Scholar]
- Willis SL. Everyday cognitive competence in elderly persons: Conceptual issues and empirical findings. Gerontologist. 1996;36:595–601. doi: 10.1093/geront/36.5.595. [DOI] [PubMed] [Google Scholar]
- Willis S, Marsiske M. Manual for the Everyday Problems Test. University Park: Pennsylvania State University; 1993. [Google Scholar]
- Willis SL, Tennstedt SL, Marsiske M, Ball K, Elias J, Koepke KM, et al. Long–term effects of cognitive training on everyday functional outcomes in older adults. Journal of the American Medical Association. 2006;296:2805–2814. doi: 10.1001/jama.296.23.2805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zanini S, Rumiati RI, Shallice T. Action sequencing deficit following frontal lobe lesion. Neurocase. 2002;8:88–99. doi: 10.1093/neucas/8.1.88. [DOI] [PubMed] [Google Scholar]