

Abstract
Hypoxia has been a frightening term for doctors and medical students because of the possibility of damage to cells, tissues and organs. However, we now know that brief, episodic hypoxia gives rise to several adaptive responses. These responses in general prepare the body for better tolerating such hypoxic episodes, and also offer protection against several other types of insults. Indeed, scientists at the erstwhile U.S.S.R. have developed what is known as ‘hypoxia therapy’ and reaped the benefits of brief intermittent hypoxia for the last several decades. In India, yogic treatment of various diseases is common. A lesser known but important variety of Pranayama is ‘nisshesha rechaka’, which may be described as breath holding at residual volume. Studies done at our centre have demonstrated that Nisshesha rechaka is the easiest way to produce brief, intermittent hypoxia. There is therefore reason to believe that Nisshesha rechaka pranayama may offer benefits through this mechanism.
Keywords: Adult stem cell migration, breath holding, erythropoietin, expiration, intermittent hypoxia, vascular endothelial growth factor, yogic Pranayama
Introduction
Recombinant biological molecules, such as Erythropoietin (EPO)[1] and Vascular Endothelial Growth Factor (VEGF)[2] are finding increasing use as therapeutic agents for various disease conditions. Injectable Recombinant Human Erythropoietin is already in use for anemia associated with chronic renal failure and to stimulate erythropoiesis for autologous blood transfusion; and efforts are on to use it to stimulate nerve growth after mechanical nerve injury,[3] in peripheral neuropathies associated with diabetes mellitus, and in autonomic neuropathies.[4] Recombinant VEGF is waiting to find clinical use in revascularization in diseased coronary and other vascular beds as an alternative to angioplasty and bypass grafting.
At the same time, the stem cells–related research is looking forward to find a cure for a number of as-yet incurable diseases. Embryonic stem cells (ESC) obtained from umbilical cord blood have already been effectively used in the treatment of sickle cell anemia, leukemia, non-Hodgkin's lymphoma, other forms of cancer, life-threatening anemias, and autoimmune diseases.[5] Stem cells may hold the key to replacing cells lost in situations, such as spinal cord injury and many progressive, devastating diseases, such as Parkinson's disease, multiple sclerosis, Alzheimer's disease, diabetes, chronic heart failure, end-stage renal disease, liver failure and cancer. Lately stem cell use has been tried in the treatment of burns, infertility, lupus, and deafness.
Stem cells survival and self-renewal has been found to be better at low tissue oxygen levels. In other words, stem cells are kind of a minority of anerobic cells in the multimillion populations of aerobic cells of the body. It is therefore these cells which are most susceptible to oxidative injury. Yogic diet allows for huge amounts of antioxidants in the diet.
Mobilization of stem cells from the bone marrow can come to use in the therapy of a number of degenerative diseases, including type-2 diabetes mellitus and Idiopathic Parkinson's disease and Osteoarthritis. Indeed this is the frontier area of research these days. Scientists are trying to harvest stem cells from the bone marrow, suitably multiply them, and then plant them at the place of need.
Transportation of stem cells from the bone marrow to the tissues can be hindered at the oxygen levels prevalent in the bloodstream. It can be facilitated by brief, episodic hypoxia. Intermittent hypoxia therapy has been tried, developed, and practiced by Russian scientists for the last 50 years.
Studies done at the Antar Prakash Centre for Yoga, Haridwar, have shown that Nisshesha rechaka, a type of Pranayama described in Hatha Pradeepika (H.P.) is the easiest way to produce brief, intermittent hypoxia. According to H.P., it can work on any organ on which the practitioner wants it to work by focusing the mind on that organ while performing the rechaka.
Oxygen and hypoxia
Oxygen has been considered essential for life since its discovery in the late 18th century. Earliest experiments showed a rat dying when enclosed under a bell jar, further, if a burning candle was also enclosed under a bell jar it would get extinguished and the remaining air would not support life. These experiments established the role of oxygen as essential for our life, and hypoxia, or lack of oxygen has been considered as injurious underlying serious diseases, such as ischemic strokes and myocardial infarctions. That a whole world of anaerobic organisms exists was not known till that time—this discovery came much later.
However, lately we have started realizing the multifold benefits of episodic, brief intermittent hypoxia. It is now well recognized that episodic hypoxia leads to adaptive responses in the tissues which protect them from ischemic and other injuries.
In the former USSR this knowledge has come to develop into a full-fledged therapy.
Hypoxia therapy
In the erstwhile USSR, for the last 50 years research was being carried out on finding uses of and ways to produce hypoxia.[6] Initially the scientists simulated the hypoxic conditions of high altitudes in the plains to train the pilots of small fighter aircrafts and the mountaineers. Thereafter, it took the form of a training tool for athletes, and ultimately developed into a full-fledged therapeutic modality. At that time the Russian scientific community was completely cut off from the rest of the world and these studies were not available elsewhere. It is only recently that some English translations of the studies have come out.
The Russian scientists have used several different techniques to produce hypoxia. They include the following:
Hypobaric chambers
Quick ascent to high altitudes for short durations.
Normobaric hypoxic gas mixtures. To deliver such gas mixtures, there they have commercially available “Hypoxicators”,[7] that is, instruments that deliver a hypoxic gas mixture containing 10% oxygen. This mixture is called “HGM-10.”
Intermittent hypoxia is defined as repeated episodes of hypoxia with intervening periods of normoxia. The actual durations used in different experimental studies vary widely, with hypoxia periods ranging from 3 to 90 min.
Beneficial effects of intermittent hypoxia
All the effects of hypoxia are generated through the now well-documented “Hypoxia-Inducible-Factor-1” (HIF-1).[8] Its molecular structure has been studied in great detail. In various tissues, the HIF-1 produces different chemicals, such as the EPO in the kidney and the VEGF in several other tissues.
Hypoxia has been shown to increase hemoglobin levels through the formation of EPO.
In ischemic tissues, hypoxia leads to the formation of growth factors, such as the VEGF, and this leads to formation of new blood vessels (angiogenesis). In ischemic myocardium this can lead to the formation of coronary collaterals.
Hypoxia induces the enzyme Nitric Oxide Synthase (NOS). Nitric oxide has been assigned different roles in different tissues. Widely, it is one of the defense mechanisms against oxidative damage. Thus more of nitric oxide is able to protect the tissues better. Nitric oxide contributes to dilatation of coronary arteries when needed. It is also involved in the quick vasodilatation required for the erection of penis,[9,10] and intermittent hypoxia can be an effective treatment for erectile dysfunction.
Hypoxia has been shown to increase resistance of tissues to various insults and injuries, including radiation injuries and aging.
Hypoxia induces p53 “Guardian of the genome.”[11] p53 is a transcription regulation factor. It has a protective role in DNA damage. It is well known that during the process of normal cell division some DNA damage does occur. There are in-built processes for the repair of such damage. If the damage goes beyond repair, then p53 is involved in activating the apoptosis program.
Stem cells only survive in hypoxia.[12] Stem cells are abundant in fetal circulation where the partial pressure of oxygen (pO2) is low. They disappear from the circulation soon after birth. They survive in various locations (Niches) in the body in adulthood. A young individual has an abundance of these stem cells. Old age is when the stem cell population reduces. It is possible that stem cells from the bone marrow migrate to various tissues, and such migration may be facilitated by even a few minutes of hypoxia every day. Thus hypoxia can be of benefit in a host of the so-called degenerative disorders, including Idiopathic Parkinson's disease, Alzheimer's disease, and Osteoarthritis, which is also called as “Joint Failure.”
Hypoxia and stem cell life cycle
Stem cells are in one of the frontier areas of research these years. Stem cells are those wonderful cells that have enormous capacity to differentiate into virtually any kind of cell in our body. This knowledge has become the foundation stone of regenerative medicine, whereby we dream of being able to produce any lost or damaged organ.
In the mother's womb the fetus develops from a single cell, the zygote, which is formed by fusion of the ovum of the mother and the sperm of the father. This single cell gives rise to the vast diversity of tissues in the developed human body. During embryonic life, differentiation goes on at a very fast pace. By about the third month of intrauterine life the development of all the organs is nearly complete.
The mother's womb provides the fetus a protected environment. The watery amniotic fluid protects it from mechanical shocks and provides a constant ambient temperature. All its nutritional requirements are met through the umbilical cord, which also serves to take away the waste products.
The mother's womb also provides a further valuable gift that commonly goes unsung: A hypoxic environment. The embryo breathes in a very low partial pressure of oxygen, about equal to that present at the Mount Everest. It is this hypoxic environment that is so important for the multiplication and growth of the stem cells, with differentiation being the natural consequence. The number of stem cells in the circulating blood is maximum during fetal life. In the laboratory, embryonic stem cells are obtained from the umbilical cord blood samples just after birth. Currently, the practice to store the umbilical cord blood for future use is being popularized.
Just after birth, when the newborn is exposed to the atmospheric air containing high pO2 and as the pO2 of the arterial blood rises, the stem cells soon disappear from the blood circulation. In the adult they survive only in certain locations called “niches.” One such location is the bone marrow where the blood circulation is sluggish, oxygen extraction is more, and there is relative hypoxia. In addition, anatomically the niche allows the cells to remain in clusters where the stem cells stay in the center, surrounded by more differentiated cells, which consume a large amount of oxygen, thus creating a hypoxic zone for the stem cells. In other words, the stem cells and more mature cells are distributed along an oxygen gradient—primitive stem cells residing in the most hypoxic areas of the bone marrow where oxygen content is low.
It has been shown in rats that the number of Mesenchymal Stem Cells (MSC) in the peripheral blood increases by as much as 15 folds by hypoxia.[13] Hypoxia enhances proliferation of mouse embryonic stem cell–derived neural cells.[14] Since cells cannot circulate in clusters, it is understandable what difficulty the marrow stem cells would encounter had they had to circulate in the blood. That probably explains why some of us are not able to regenerate lost tissues and suffer from such diseases as diabetes mellitus, osteoarthritis of the knees, and idiopathic Parkinson's disease.
It may be of interest to note that the prevalence of osteoarthritis of the knees has been found to be less in hilly areas. Although some scientists believe this difference may be due the fact that the residents of hills get more exercise having to walk up and down the hills; there may be something more to it. The hypoxic environment of the hills may contribute to the persistence of stem cells in the articular cartilages, or their migration from niches like the bone marrow.
That the stem cells survive better when cultured in hypoxic environment is now well recognized. Artificial culture of stem cells in different environmental conditions showed that stem cells retain their self-renewing character if cultured under hypoxic conditions, in 2% oxygen as compared with the 20% present in air.
However, the direction of regenerative medicine appears misguided. The scientists are trying to capture stem cells from the bone marrow, cultivate them, and then inject them at the site of desired organogenesis or organ repair. This may be a little out of place; given the wisdom of the body. The way we do not need to capture, cultivate, and re-inject the bone marrow cells to generate more blood cells, we should not need to do the same for any other organ, because the whole body is well connected through a meticulous network of blood vessels, and the stem cells should be able to circulate and relocate themselves at the place of need guided by chemotactic factors as yet unrecognized. What then prevents the bone marrow stem cells from circulating and relocating themselves to the place of need? – Oxygen!
Oxidative stress and injuries
It is now well recognized that oxidative stress is a great damaging force that causes degenerative diseases. Diseases believed to result from oxidative injuries include osteoarthritis and Idiopathic Parkinson's disease. The bone marrow stem cells and the mesenchymal stem cells are poor in number of mitochondria, that is, they are adapted to anaerobic survival.
From the discussion in the previous paragraphs it must be clear that the cells most likely to suffer damage from excess of oxygen are the stem cells.
Examples of disease conditions where self-administered brief intermittent hypoxia can work
Type-2 Diabetes mellitus
This has acquired epidemic proportions. A patient affected with Type-2 Diabetes Mellitus (T2DM) gradually loses the β-cell mass. The current therapeutic strategies include stimulating insulin release from the β cells by sulfonylureas, stimulating peripheral utilization of glucose by biguanides, and reducing insulin resistance using thiazolidinedione derivatives. These drugs need to be taken continuously; and over the years their effect vanishes. Incretin mimetics, such as GLP-1 analogs (eg, Exenatide) hold promise as they stimulate the proliferation and inhibit the apoptosis of β cells. Drugs inhibiting breakdown of endogenous GLP-1, for example, vildagliptine are other agents used for the treatment of T2DM.
Human embryonic stem cells can be directed to differentiate into cells that produce insulin.[15] The adult body is endowed with a population of adult stem cells, which by definition are capable of self-renewal as well as differentiation in any one of several different types of adult tissues.
It is wise to expect that nature must have provided for the regeneration of β cells through the use of stem cells. Mice have been seen to regenerate β-cell mass after ablation of 70%–80% of it. In them the source of new beta cells is the adult, differentiated beta cell. The capacity of hemopoietic stem cells to differentiate to insulin-producing cells has been at the center of debate for the past 5 years and it now seems that their role could more likely be that of helper cells able to facilitate survival or stimulate proliferation of endogenous β cells.[16]
Coronary artery disease
In addition to the existing therapies with drugs, stents, and bypasses, the scientists are keen to find other ways to regenerate the blocked coronary arteries in a more natural way. Stimulating the formation of coronary collaterals “Natural Bypasses” has been pointed out to be a neglected field.[17]
The major disease affecting the coronary arteries is atherosclerosis, which is the underlying cause for angina pectoris and myocardial infarction. When the narrowing of the coronary artery is gradual, it is associated with the development of collateral channels. The mechanism involved is thought to be tissue hypoxia leading to formation of VEGF. Physical exercise also must offer relief in coronary artery disease through generating brief hypoxia. Coincidentally, patients with sleep apnea and hypoxic spells have been found to have developed better coronary collaterals![18]
Osteoarthritis
Osteoarthritis, rightly named “Joint Failure” is a degenerative disease, thereby meaning a disease of old age caused by progressive damage to the joint cartilage at a rate the body is not able to repair. The factors that lead to destruction of the joint cartilage are the same over all the ages, but in children as well as young adults the cartilage that gets damaged due to wear and tear gets completely repaired by the body's regenerative process on a day-to-day basis. It is when either the rate of destruction increases or the rate of repair lags behind that the problem manifests clinically.
The destructive forces are wear and tear, and with the weight-bearing joints, such as the knees, the damage increases in proportion to the body weight. It is important to understand the role of oxidative damage to the regenerative tissues so that the use of antioxidants in the diet can be promoted.
Natural reparative process is largely carried out by the chondrocytes, which secrete the extracellular matrix. Cellular damage to the chondrocytes is made good by chondroblasts and deficiency of chondroblasts can be made good by stem cells present in the near vicinity. With insufficiency of stem cells more stem cells can be mobilized from the bone marrow, which serves as the storehouse. This process occurs under the influence of chemotactic factors. Some of such factors may be inhibited by the Non Steroidal Anti-Inflammatory Drugs (NSAIDs).
Scientists are trying to harness stem cells from the bone marrow, suitably multiply them in culture and then plant them at the site of injury to replenish the cartilage.[19] Infrapatellar fat pad (IPFP) is a possible source of stem cells for the repair of articular cartilage defects.[20] Hypoxic conditions increase hypoxia-inducible transcription factor HIF-2α and enhance chondrogenesis in stem cells from the infrapatellar fat pad of osteoarthritis patients.[21]
Parkinson's disease
Parkinson's disease (PD) affects around 3% of people aged over 65 years. It occurs as a result of the loss of dopamine-producing brain cells in specific location called the substantia nigra. Symptoms of PD are tremor, or trembling in hands, arms, legs, jaw, and face; rigidity, or stiffness of the limbs and trunk; bradykinesia, or slowness of movement; paucity of facial expression and postural instability, that is, impaired balance and coordination. These symptoms are gradually progressive and some patients may have difficulty walking, talking, or performing simple day-to-day tasks. PD usually affects people over the age of 50 years.
At present, there is no cure for PD. Bradykinesia and rigidity respond best to treatment with levodopa, whereas tremors respond better to anticholinergics, such as trihexyphenydyl. Other drugs, such as bromocriptine mimic the role of dopamine in the brain.
The possible approach of taking stem cells, growing them into new brain cells and transplanting these into the patient is currently being discussed.[22] Jaslok Hospital, Mumbai, is trying to study the safety and efficacy of bone marrow–derived mesenchymal stem cells transplant in Parkinson's disease.[23]
Chronic renal failure
In developed as well as developing countries, Chronic Renal Failure (CRF) is a great public health problem. In the developing countries, people commonly cannot afford the cost of dialysis and the average life span of a patient after diagnosis is short, up to 3 years.
For the treatment of anemia of CRF, injections of recombinant Human Erythropoietin are commonly employed whether the patient is on dialysis or not.
However, researches have shown that the diseased kidney still has intact capacity to secrete EPO. Acute hypoxic stress is associated with increased levels of EPO. Hence it is thought that the EPO deficiency of chronic renal failure is a result of a functional disturbance.[24,25]
Hypoxia induced by breath holding in full expiration (Nisshesha rechaka pranayama) as described can greatly help patients by increasing endogenous EPO production, thus cutting down expenditure on EPO injections and reducing cost of treatment.
Erectile dysfunction
Erectile dysfunction (ED) occurs in about 5% of 40-year-old men and in 15%–25% of 65-year-old men. It is defined as an inability to achieve penile erection sufficient for satisfactory sexual activity. The penis contains two elongated structures called the corpora cavernosa, consisting of spongy tissue, which run the length of the organ. The corpora cavernosa are surrounded by a membrane, called the tunica albuginea.
Erection begins with sensory or mental stimulation, or both. The tunica albuginea helps trap the blood in the corpora cavernosa, thereby sustaining erection. This requires a quick vasodilatation, which is mediated by some neurotransmitters, such as the vasoactive intestinal peptide (VIP) released from the supplying nerves. Nitric oxide plays a very important role in the quick vasodilatation.[26] Nitric oxide is produced by vascular endothelium and diffuses into the smooth muscle cells of the arteries where it leads to the release of cyclic GMP. Drugs such as sildenafil act by inhibiting the metabolizing enzyme phosphodiesterase-5 (PDE5), thus inhibiting the breakdown and prolonging the effect of the endogenous cyclic GMP.
Brief intermittent hypoxia induces Nitric Oxide Synthase (NOS) thereby facilitating the quick vasodilatation in the penile arteries thus enabling quick and hard erection. Possible mechanism of brief intermittent hypoxia is different disease condition has been depicted at Figure 1.
Figure 1.
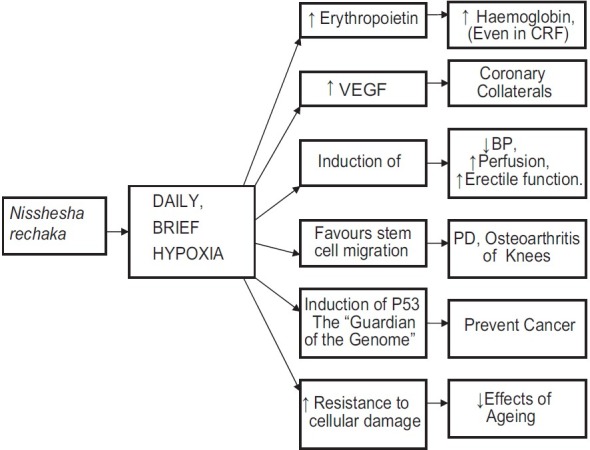
Diagrammatic representation. (CRF: Chronic renal failure, VEGF: Vascular endothelial growth factor, NOS: Nitric oxide synthase,BP: Blood pressure, PD: Parkinson's disease)
My hypothesis
Daily Self-Administered brief, intermittent hypoxia may cause release of endogenous EPO and VEGF, induce nitric oxide synthase and p-53 “the guardian of the genome” and offer a multitude of benefits in health and a variety of disease conditions. This may be the basis of the claims made about the benefits of the yogic technique of Pranayama.
Daily Self-Administered brief, intermittent hypoxia may help stem cell migration. My hypothesis is that the high pO2 present in the arterial blood in adult human beings is a deterrent to the migration of the stem cells. It is like a curfew imposed in a city where the oxygen-sensitive stem cells cannot circulate freely, and that a few minutes’ hypoxia is like a relaxation in that curfew whereby the stem cells can freely circulate for sometime and can settle down in organs, which require them in response to the chemotactic stimuli produced by the tissues.
Breathholding in full expiration [at residual volume (RV)], —a variety of the yogic technique Pranayama—is the easiest way to produce daily brief, intermittent hypoxia!
There have been several studies in human beings on breathholding, which have recently been reviewed by Parkes.[27] The breathhold duration is the easiest parameter to study, and it has been found that the duration is prolonged by physical inactivity, larger initial lung volume, hyperoxia and hypocapnia and is shortened by the opposite conditions. Endtidal partial pressures of oxygen (PetO2) (Lin, 1974) could be lowered to 62 mmHg (SpO2 about 60%).
It has been found that the central respiratory rhythm (in the pontomedullary respiratory center) continues during breathholding and that it is totally involuntary. One can only suppress the expression of this rhythm by voluntary contraction of some of the respiratory muscles, or closing the glottis at any chosen volume of the chest. Parkes has also suggested the terms “breathholding at vital capacity” (after the deepest inspiration) and “breathholding at functional residual volume (FRV)” (at the end of a normal expiration). The experimenters have not studied breathholding at the deepest expiration, that is, at RV for fear of atelectasis. As we shall see, in our experiments atelectasis was not encountered in any case despite the breathholding at RV.
In the above review the objective was to identify a maneuver that could enable one to hold breath to unconsciousness. So far it has not been possible for normal human being breathing air at sea level to hold breath till loss of consciousness. Hypoxia or hypoxia therapy was not their concern, and therefore no study seems to have been performed to identify maneuvers to produce brief, intermittent hypoxia. Using daily breathholding as a therapeutic maneuver has never been considered in conventional medicine except in the oriental Pranayama.
Our studies at the Antar Prakash centre for yoga
At our Antar Prakash Centre for Yoga, the different varieties of Pranayama were studied for their efficiency in producing hypoxia; using a pulse oximeter. We recorded the SpO2 during different breathholding maneuvers. The findings have been published in the book entitled ‘Yoga Book for Doctors’[28] and are verifiable (Even a public demonstration was held during a conference at Lonavla in December 2006).
We have since studied the phenomenon further. Nisshesha rechaka means holding the breath in full expiration (at RV). Then the lung alveoli are empty and the blood flowing in alveolar capillaries returns without oxygenation. We found that it is best performed in two settings.
Following a 15-min recitation of “Om.” Traditionally, Omkar japa is performed sitting still in a comfortable asana, by reciting “Om” once in a single breath, repeating several times. Thus while reciting “Om,” one takes deep inspirations and the breath is prolonged to 30 s or even more. We introduced a 3-breath Nisshesha rechaka after the Omkar japa. A hypoxia of SpO2 of about 90% or below is achievable very comfortably.
A particular sequence ‘Bhastrika followed by Nisshesha rechaka’ is very efficient in producing hypoxia. Translated in physiological jargon it means ‘hyperventilation followed by breath holding in full expiration (at RV)’. The physiological explanation is as follows: The hyperventilation washes out carbon dioxide which constitutes a major stimulus for normal respiration. Once that is done, the breath can be held for a longer duration.
It has been shown that even a novice, in the first attempt can get hypoxia to bring the SpO2 down to 88% hemoglobin saturation, and with persistent effort it may be brought down to 80% or below.
Now if all the Russian wisdom gained from the studies on hypoxia created by administration of hypoxic gas mixtures is applied to the Indian Pranayama, we can conclude that Nisshesha rechaka pranayama is the easiest technique to produce hypoxia and can offer all the benefits as obtained by hypoxia therapy.
Conclusion
Pranayama is an ancient Indian yogic technique of regulation of breath included in the daily routine of the yogis.[29] It involves gradual training of the respiratory apparatus for prolonging the breathhold time. The aspirant is required to practice every day and advance very slowly over several days to months for perfection. In the yogic literature there are more than 8 types of Pranayama, which involve breathing through one or the other nostril, or through the rolled tongue made like a tube; and holding the breath in inspiration, expiration, or somewhere between the two.
In the last few years, Yoga is gradually getting established as a therapy. In the recent edition of the ancient text H.P. published by Kaivalyadhama, a chapter has been added that contains a very useful method of yogic treatment of various disorders (that can arise during practice of Yoga). It is called the “Nisshesha rechaka”[29] (The literal translation is “full exhalation with no residual air,” and the physiological translation is “breathholding at RV”).
Pranayama is being taught to millions of people via the television channels by the Yoga Gurus, and it is commonly adorned as “providing extra oxygen to the system.” This explanation comes to them most naturally but does not convince the medical professionals who have 100% oxygen available at their disposal and know that it cannot cure all ills. The truth is that while extra oxygen cannot cure all ills, intermittent hypoxia can. The yoga gurus are so far unaware of the beneficial effects of brief, intermittent hypoxia, and little do they realize that of the 8 varieties of Pranayama, only Nisshesha Rechaka leads to hypoxia.
References
- 1.Langston CE, Reine NJ, Kittrell D. The use of erythropoietin. Vet Clin North Am Small Anim Pract. 2003;33:1245–60. doi: 10.1016/s0195-5616(03)00101-3. [DOI] [PubMed] [Google Scholar]
- 2.Freedman SB, Isner JM. Therapeutic angiogenesis for ischemic cardiovascular disease. J Mol Cell Cardiol. 2001;33:379–93. doi: 10.1006/jmcc.2000.1329. [DOI] [PubMed] [Google Scholar]
- 3.Yin ZS, Zhang H, Gao W. Erythropoietin promotes functional recovery and enhances nerve regeneration after peripheral nerve injury in rats. Am J Neuroradiol. 2010;31:509–15. doi: 10.3174/ajnr.A1820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lipton SA. Erythropoietin for neurologic protection and diabetic neuropathy. N Engl J Med. 2004;350:2516–7. doi: 10.1056/NEJMcibr041121. [DOI] [PubMed] [Google Scholar]
- 5.Stem cell basics, Stem cell information. The National Institute of Health resource for stem cell research. [Accessed on April 16, 2010]. Available from: http://stemcells.nih.gov/info/basics/basics6.asp .
- 6.Strelkov RB. Application of interrupted normobaric hypoxia stimulation on healthy people. Fiziol Zh. 2003;49:45–9. [PubMed] [Google Scholar]
- 7.Strelkov RB. The prospects for the use of a method of intermittent normobaric hypoxic stimulation (hypoxitherapy) in medical practice. Vopr Kurortol Fizioter Lech Fiz Kult. 1997;6:37–40. [PubMed] [Google Scholar]
- 8.Déry MA, Michaud MD, Richard DE. Hypoxia-inducible factor 1: Regulation by hypoxic and non-hypoxic activators. Int J Biochem Cell Biol. 2005;37:535–40. doi: 10.1016/j.biocel.2004.08.012. [DOI] [PubMed] [Google Scholar]
- 9.Burnett A. Nitric Oxide in the Penis: Physiology and Pathology. J Urol. 1997;157:320–4. [PubMed] [Google Scholar]
- 10.Burnett AL. The role of nitric oxide in erectile dysfunction: Implications for medical therapy. J Clin Hypertens (Greenwich) 2006;8(12 Suppl 4):53–62. doi: 10.1111/j.1524-6175.2006.06026.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.An WG, Kanekal M, Simon MC. Stabilization of wild-type p53 by hypoxia-inducible factor 1 alpha. Nature. 1998;392:405–8. doi: 10.1038/32925. [DOI] [PubMed] [Google Scholar]
- 12.Cipolleschi MG, Dello Sbarba P, Olivotto M. The role of hypoxia in the maintenance of hematopoietic stem cells. Blood. 1993;82:2031–7. [PubMed] [Google Scholar]
- 13.Rochefort GY, Delorme B, Lopez A, Hérault O, Bonnet P, Charbord P, et al. Multipotential mesenchymal stem cells are mobilized into peripheral blood by hypoxia. Stem Cells. 2006;24:2202–8. doi: 10.1634/stemcells.2006-0164. [DOI] [PubMed] [Google Scholar]
- 14.Rodrigues CA, Diogo MM, da Silva CL, Cabral JM. Hypoxia enhances proliferation of mouse embryonic stem cell-derived neural stem cells. Biotechnol Bioeng. 2010;106:260–70. doi: 10.1002/bit.22648. [DOI] [PubMed] [Google Scholar]
- 15.Gupta DK, Sharma S. Stem cell therapy - Hope and scope in pediatric surgery. J Indian Assoc Pediatr Surg. 2005;10:138–41. [Google Scholar]
- 16.Sordi V, Piemonti L. The contribution of hematopoietic stem cells to beta-cell replacement. Curr Diab Rep. 2009;9:119–24. doi: 10.1007/s11892-009-0021-x. [DOI] [PubMed] [Google Scholar]
- 17.Koerselman J, van der Graaf Y, de Jaegere PP, Grobbee DE. Coronary collaterals: An important and underexposed aspect of coronary artery disease. Circulation. 2003;107:2507–11. doi: 10.1161/01.CIR.0000065118.99409.5F. [DOI] [PubMed] [Google Scholar]
- 18.Steiner S. Occurrence of coronary collateral vessels in patients with sleep apnea and total coronary occlusion. Chest. 2010;137:516–20. doi: 10.1378/chest.09-1136. [DOI] [PubMed] [Google Scholar]
- 19.Murphy JM, Fink DJ, Hunziker EB, Barry FP. Stem cell therapy in a caprine model of osteoarthritis. Arthritis Rheum. 2003;48:3464–74. doi: 10.1002/art.11365. [DOI] [PubMed] [Google Scholar]
- 20.Khan WS, Tew SR, Adesida AB, Hardingham TE. Human infrapatellar fat pad-derived stem cells express the pericyte marker 3G5 and show enhanced chondrogenesis after expansion in fibroblast growth factor-2. Arthritis Res Ther. 2008;10:R74. doi: 10.1186/ar2448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Khan WS, Adesida AB, Hardingham TE. Hypoxic conditions increase hypoxia-inducible transcription factor 2 alpha and enhance chondrogenesis in stem cells from the infrapatellar fat pad of osteoarthritis patients. Arthritis Res Ther. 2007;9:R55. doi: 10.1186/ar2211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Panchision DM. Repairing the Nervous System with Stem Cells. Stem Cell Information, The National Institutes of Health resource for stem cell research. [Last accessed on 2010 Apr 16]. Available from: http://stemcells.nih.gov/info/2006report/2006Chapter3.htm .
- 23.Jaslok Hospital and Research Centre. [Last accessed on 2010 Apr 16]. Available from: http://www.clinicaltrials.gov/ct2/show/NCT00976430?term=parkinson%27s+stem+cellsandrank=1 .
- 24.Kurtz A, Eckardt KU. Erythropoietin production in chronic renal disease before and after transplantation. Contrib Nephrol. 1990;87:15–25. doi: 10.1159/000419475. [DOI] [PubMed] [Google Scholar]
- 25.Chandra M, Clemons GK, Mc Vicar MI. Relation of serum erythropoietin levels to renal excretory function: Evidence for lowered set point for erythropoietin production in chronic renal failure. J Pediatr. 1988;113:1015–21. doi: 10.1016/s0022-3476(88)80573-0. [DOI] [PubMed] [Google Scholar]
- 26.Burnett AL. The role of nitric oxide in erectile dysfunction: Implications for medical therapy. J Clin Hypertens (Greenwich) 2006;8(12 Suppl 4):53–62. doi: 10.1111/j.1524-6175.2006.06026.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Parkes MJ. Breath-holding and its breakpoint. Exp Physiol. 2006;91:1–15. doi: 10.1113/expphysiol.2005.031625. [DOI] [PubMed] [Google Scholar]
- 28.Malshe PC. ‘Yoga Book for Doctors’. Haridwar, India: Antar Prakash Centre for Yoga; 2005. ISBN 81-903298-1-2. [Google Scholar]
- 29.Digambaraji S, Kokaje RS, editors. Haţhapradipika of Swatmarama. Lonavala, Dist. Pune, India: S.M.Y.M.Samiti; 1970. ISBN:81-89485-12-1. [Google Scholar]