

Abstract
The European Myeloma Network has organized two workshops on fluorescence in situ hybridization in multiple myeloma. The first aimed to identify specific indications and consensus technical approaches of current practice. A second workshop followed a quality control exercise in which 21 laboratories analyzed diagnostic cases of purified plasma cells for recurrent abnormalities. The summary report was discussed at the EHA Myeloma Scientific Working Group Meeting 2010. During the quality control exercise, there was acceptable agreement on more than 1,000 tests. The conclusions from the exercise were that the primary clinical applications for FISH analysis were for newly diagnosed cases of MM or frank relapse cases. A range of technical recommendations included: 1) material should be part of the first draw of the aspirate; 2) samples should be sent at suitable times to allow for the lengthy processing procedure; 3) most importantly, PCs must be purified or specifically identified; 4) positive cut-off levels should be relatively conservative: 10% for fusion or break-apart probes, 20% for numerical abnormalities; 5) informative probes should be combined to best effect; 6) in specialist laboratories, a single experienced analyst is considered adequate; 7) at least 100 PC should be scored; 8) essential abnormalities to test for are t(4;14), t(14;16) and 17p13 deletions; 9) suitable commercial probes should be available for clinically relevant abnormalities; 10) the clinical report should be expressed clearly and must state the percentage of PC involved and the method used for identification; 11) a retrospective European based FISH data bank linked to clinical data should be generated; and 12) prospective analysis should be centralized for upcoming trials based on the recommendations made. The European Myeloma Network aims to build on these recommendations to establish standards for a common European data base to define subgroups with prognostic significance.
Keywords: myeloma, cytogenetic, interphase FISH, recommendation
Introduction
Multiple myeloma (MM) is an orphan disorder of end-stage plasma cells with acquired genetic abnormalities of clinical importance not captured by conventional cytogenetic analysis.1
The acquired genetic evolution progresses through a stepwise transformation process initiated in half of the cases by a reciprocal translocation involving the IGH gene (14q32). Translocations involving this region show an array of promiscuous target genes including cyclin D1, D3, FGFR3/MMSET, MAF, and MAFB.2–9 In addition, secondary translocations have been observed in 50% during disease progression.2,3,10–13
The introduction of high-dose therapy and a range of new promising agents have changed the prognosis and extended the therapeutic possibilities. In parallel, the use of molecular cytogenetic techniques has led to the identification of recurrent genetic abnormalities with major prognostic impact and predictive information.14–18 However, the fact that the malignant clone in MM differs from other hematologic malignancies due to a high fraction of low proliferating malignant PC and multiple marrow infiltrates has been a challenge for standardization of cytogenetic analysis. Comparative genomic hybridization studies have confirmed that nearly all myelomas have karyotypic changes and interphase fluorescence in situ hybridization (FISH) has emerged as the most useful current cytogenetic assessment.18,19 However, the identification or selection of the malignant cells by morphology, immunophenotyping or through sorting of PC is required before FISH probes can give reliable results. Therefore, the European Myeloma Network (EMN) sponsored two technical workshops attempting to identify specific indications and to resolve outstanding technical issues and develop consensus approaches for interphase FISH analysis based on current practice.
This report combines the practical guidelines derived from consensus views and group data analysis performed at these workshops. Final recommendations for which FISH tests must be carried out are those of the IMWG as these are considered the most up to date data,18,19 although chromosome 1 probes are also strongly recommended.20,21
Co-ordinating strategy and the quality control exercise
The first workshop in London, organized by Fiona Ross, involved 31 European laboratories each of which had returned a questionnaire on local analysis methodology. Reports focused on clinician needs (Brian Durie), the advantages and disadvantages of PC purification (Hervé Avet-Loiseau), the advantages and disadvantages of simultaneous immunostaining (Johannes Drach), identification of PC by morphology in FISH preparations (Sheila O’Connor) and finally a presentation of the questionnaire results (Fiona Ross). The rest of the meeting was devoted to the drawing up of recommendations.
Quality control results
Twenty-one laboratories took part in the quality control (QC) exercise. Hervé Avet-Loiseau shipped purified plasma cells from 10 diagnostic cases and asked the laboratories to test for t(4;14), t(11;14), t(14;16), del(13)(q14) and del(17)(p13), provided that they had the requisite probes. The QC exercise, therefore, only tested probe scoring ability without giving any information about the ability of the laboratories to select or identify PC. The results were presented and discussed at a second workshop in Nantes, which led to further refinement of the recommendations.
With 6 tests and 21 laboratories there was a theoretical total of 1,260 tests in the exercise. However, 3 laboratories did not have the t(14;16) probe and a number of other tests were not attempted, probably due to a perceived shortage of material by those who normally used identification rather than purification and so were not used to handling extremely small numbers of cells. Therefore, 1,173 tests were actually undertaken (Tables 1 and 2). Although there was good general agreement, the results emphasized the difficulties of myeloma FISH. Twenty-one tests failed. There were 15 false negative results: 3 missed the major abnormalities of IGH break-apart, t(4;14) and t(11;14), plus one 17p deletion was only recorded as being below the conservative cut-off level, and 11 numerical abnormalities were not recorded in fusion probe tests. Eleven false positive results were reported, even using the conservative cut-off levels (1 del(13q), 3 del(17p), 3 IGH break-apart, 1 t(4;14), and 3 cases with CCND1 gains). In addition, 3 IGH simple deletions were reported as rearrangements.
Table 1.
Summary of analysis of shipped samples.
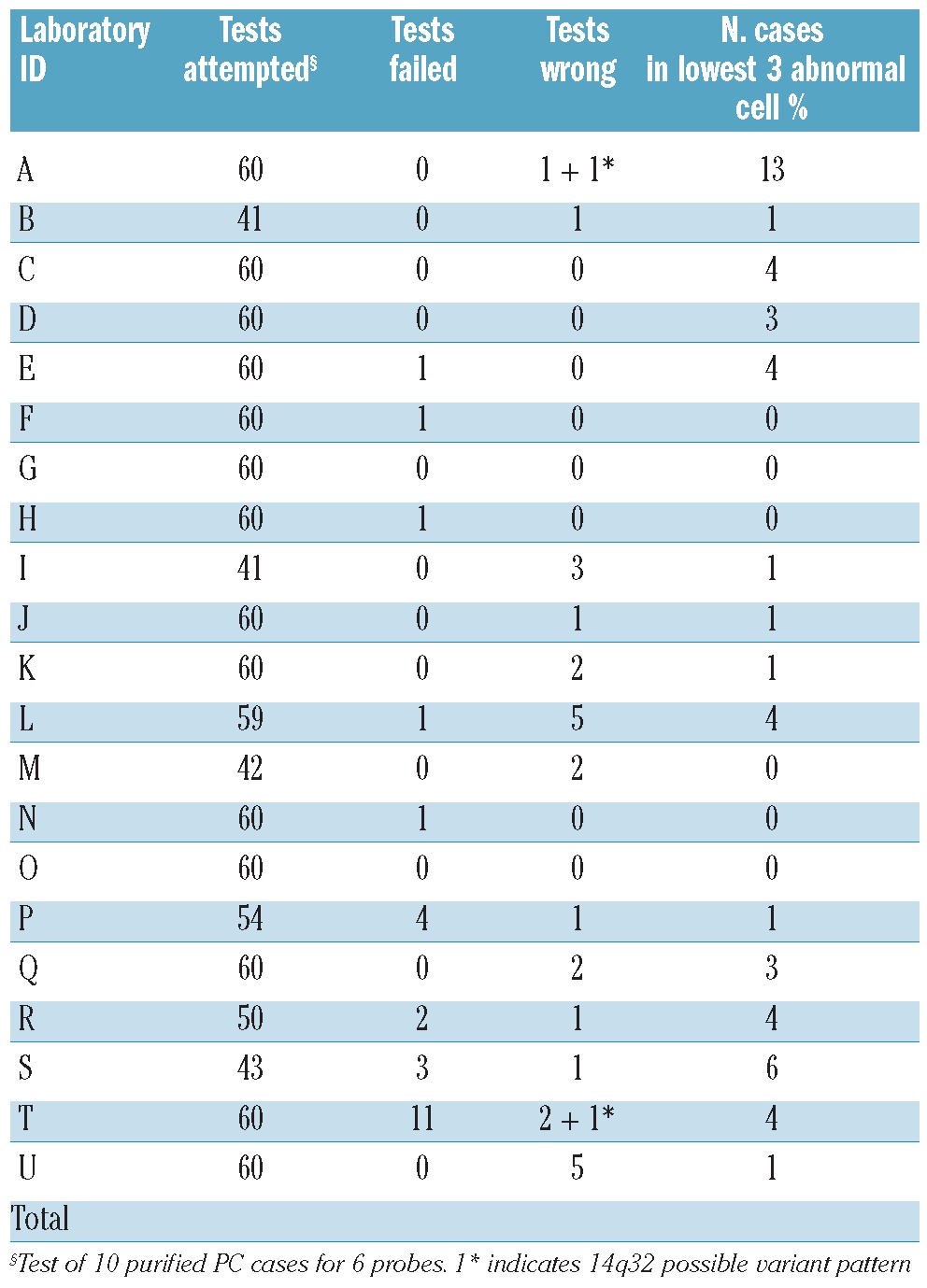
Table 2.
Summary of results by probe.
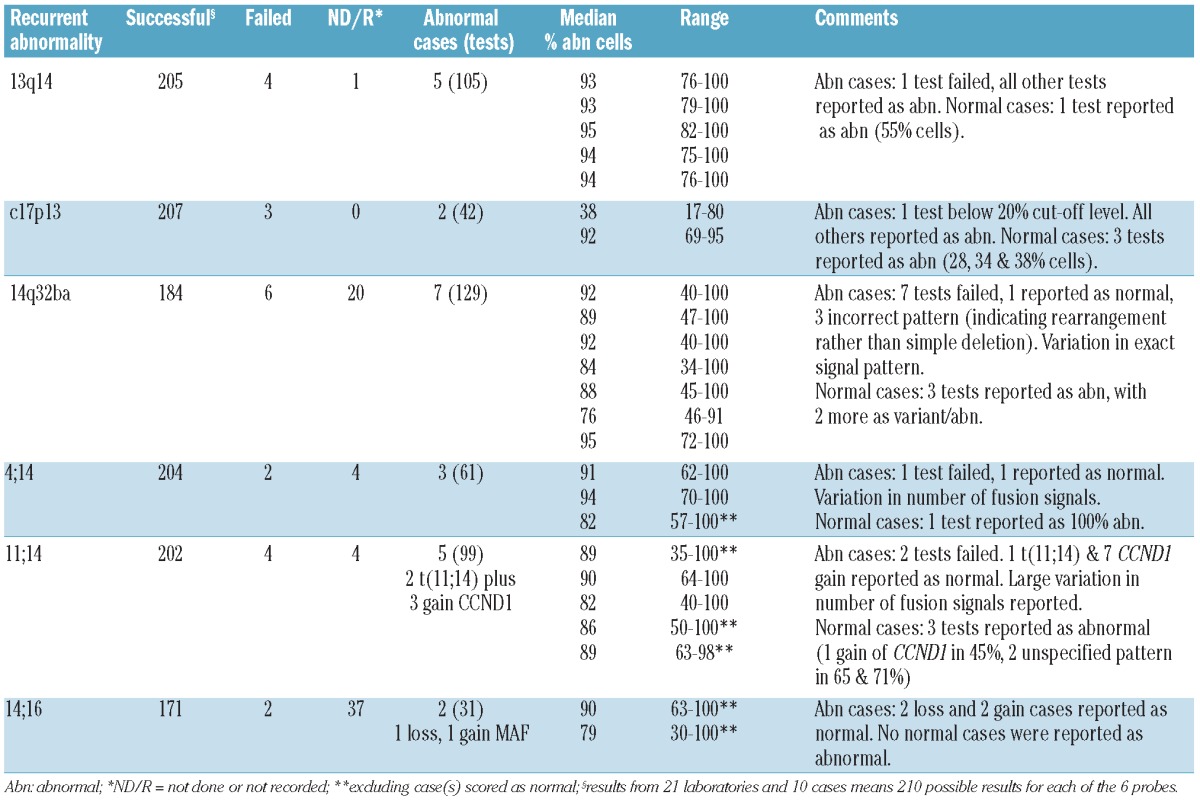
As well as these incorrect results, there was a considerable range in both the proportion of abnormal cells reported in abnormal cases (up to 66% difference) and in the exact signal patterns for fusion and break-apart probes. Most of the problems were shared out between 16 of the 21 laboratories rather than any one laboratory performing consistently poorly. One laboratory consistently recorded low numbers of affected cells in the abnormal cases but this did not translate into a high false negative rate. It is notable that at the time of the QC exercise, several of the laboratories had only recently started performing MM FISH. It is to be hoped that greater familiarity with procedures and QC exercises will result in greater consistency in abnormality levels and fewer incorrect results.
EMN consensus for FISH assays in monoclonal gammopathies
Discussions of the key issues for FISH on BM samples at diagnosis are summarized with identification of consensus approaches where available. Unless otherwise stated, the methods refer to the characterization of PC in bone marrow samples.
Diagnostic material, handling and plasma cell identification
Accurate quantitation of the plasma cell burden in bone marrow is essential for the correct diagnosis of plasma cell disorders. This is usually assessed from morphological examination of stained bone marrow aspirate smears or trephine sections. There are some discrepancies with other techniques as the marrow samples taken for morphological review are often the highest quality ‘first-pull’ marrow aspirate samples while those sent for laboratory investigations are often secondary aspirate samples with a higher degree of peripheral blood contamination.
The commonly low median proportion of plasma cells, ranging from 1–20%, within the bone marrow aspirates experienced by the InterGroupe Francophone du Myelome (IFM), LLR UK Myeloma Forum Cytogenetic Database and the Nordic Myeloma Study Group (NMSG) indicate that the FISH technique cannot be performed directly as in other hematologic malignancies. The plasma cells need to be selected, either by flow cytometry or immunomagnetic-bead based PC sorting or by the concomitant labeling of the cytoplasmic immunoglobulin light chain, allowing unambiguous identification. More recently, image analysis systems allowing morphological assessment of plasma cells and FISH scoring only in those cells designated as PC have become available. All of these methods give good results and the choice should be left to individual laboratories. However, cell sorting provides a pure PC population that enables further analyses to be performed by, for example, global gene expression, copy number analyses and methylation. A significant fraction of samples will have too few PCs to allow such analyses to be made and will censor some patients in subsequent clinical evaluation. A small proportion will be too poor to yield enough purified cells even for FISH analysis, so it is advisable to have alternative methods available where comprehensive results are essential.
Although laboratories involved in providing the FISH analysis for clinical trials will make every effort to ‘rescue’ poor samples, it is strongly recommended that referring clinicians should also maximize the chances of adequate results being obtained. This means that the material sent must be part of the first draw of the aspirate or the needle must be repositioned for further aspiration, rather than continuing to withdraw marrow blood from the puncture.
All methods require immediate processing of samples when received by the laboratory, which should be with minimum delay. They are also all time consuming so that referring clinicians must take into account how the sample is to be transported (ideally arriving the next morning) and not to arrive after midday on Fridays, or at weekends for obvious reasons.
Given the problems with obtaining good specimens from diagnostic and relapse myeloma samples, it was agreed that FISH in plasma cell disorders with very low level marrow infiltration, such as MGUS, AL amyloidosis and myeloma disease monitoring should remain firmly a research activity. In fact, there is already evidence that some abnormalities have a different prognosis when the patient relapses; the workshops did not discuss whether probe selection should change at relapse.
Material and identification consensus
Sample quality is a key factor and it is essential to use a ‘first-pull’ or repositioned aspirate sample for FISH and other molecular studies to reduce sampling artefact.
Timing of samples should take into consideration processing which is time-consuming.
Morphological assessment of plasma cell percentage is necessary for concordance with the current diagnostic criteria and is helpful in providing a global assessment of the sample. The morphological assessment of the bone marrow smears cannot be used to decide whether or not to purify the sample for FISH; this must be made on the part sent for analysis.
Purification or identification of PC is essential but the method used should be decided by each laboratory from their own expertise and requirements in accordance with the EMN based technical recommendations.
Cytogenetic analysis by FISH is reproducible with care and sufficient expertise and may provide reliable information predicting outcome in myeloma. However, further studies are required before it is routinely used to make treatment decisions outside the context of a clinical trial. The evidence is good enough to suggest that clinical trials ought to incorporate diagnostic FISH analysis in order to interpret outcomes correctly. Routine analysis should be confined to diagnostic or relapse myeloma samples, with earlier stage disease and myeloma disease monitoring remaining, for the present, a subject for research only.
Probe selection
It was the experience that all 13q probes give similar results and there was no justification for recommending any particular probe or set of probes.
Everyone had experience with the IGH break-apart probe. Its main benefit is to determine whether there is significant loss of the der(14) but this was not felt to be sufficiently important to insist on the use of this probe in the light of the significant problems that it poses for the interpretation of results. Although everyone was satisfied with the various dual fusion probes used, there were significant variations between laboratories in the proportion of single and dual fusions reported in the positive t(4;14) and t(11;14) results on the quality assessment exercise. These differences were not simply due to using probes from different manufacturers.
Most laboratories using 1q probes had developed them in-house. Where laboratories had used more than one probe, the results confirmed that the majority of abnormalities are gain of the whole arm but several different probes showed discordant amplification in a few cases. The Cytocell Aquarius CDKN2C/CKS1B probe is, therefore, a suitable commercial probe for chromosome 1.
Many laboratories were using the Vysis 5/9/15 combination to estimate ploidy but no-one took a strong position on this. Subsequent work has suggested that 5q, rather than 5p, may be important for prognosis, therefore laboratories investigating ploidy may wish to reconsider their choice of probe sets.
The objections to using two ‘deletion’ probes to control for each other expressed at the first workshop were withdrawn at the second workshop and, in fact, use of a 13q probe with a 17p probe was recommended as a sensible way to maximize the small amounts of material involved.
Most laboratories were using Vysis probes that meant that we could not make any useful comments about choice of probe manufacturer.
The determination of cut-off levels was the most controversial issue. At the first workshop, there was an agreement of 10% for fusions and 20% for numerical abnormalities on the basis of plasma cell controls run by the few groups able to obtain such material. At the second workshop, there was less agreement; a few laboratories prefered to use their own in-house established mean +3 standard deviation, (SD) from normal bone marrow controls and report anything above this as abnormal. The significant variation in reporting levels seen on the QC exercise would appear to support the argument for conservative cut-off levels, as does the frequent need to use two probes which may be abnormal to control for each other due to the shortage of material. It should also be noted that in purified or selected populations, diagnostic myeloma samples are expected to show essentially all cells with the primary abnormality.
However, other suggested prognostic markers are clearly secondary changes and may only be present in subpopulations. Hervé Avet-Loiseau reported that the IFM group used a 30% cut off for del(13) and 50% for del17p on the basis of their own previous results. It was agreed that EMN should take the initiative by running survival curves on data and varying cut-off levels to establish whether the size of the clone is important.
Discussion about the number of cells to analyze was primarily concerned with suboptimal samples. It was agreed that, wherever possible, 100 cells should be scored, but there was disagreement about the minimum number of cells that could be reported. Where high purity/identified PC were being used, 50 cells should be adequate to report a normal result for a primary abnormality in a diagnostic situation, but for potential secondary changes the report should be qualified. In some situations, a uniformly abnormal result on as few as 10 cells could be reported, but the uncertainty due to the low number should be clearly stated.
Probe selection consensus
Abnormalities to test for are: t(4;14)(p16;q32), t(14;16)(q32;q23) and 17p13 deletions. The recent availability of a 1p/1q commercial probe means that these areas should also be tested. An extended panel may include testing for t(11;14)(q13;q32), t(14;20), ploidy status, and chromosome 12 and 13 abnormalities. In the context of clinical validation trials, attempts should be made to test for more than just the 3 essential probes.
Positive cut-off levels should be relatively conservative.
A single experienced analyst is considered adequate to examine the majority of cases but all those with low-level positive results or a low level of selected PC should be checked by a second analyst. At least 2 analysts should be used when laboratories first start performing FISH analysis.
In general, 100 PC should be scored.
Clinical reporting and use of results
Each national or regional myeloma group has its own data registration system that is activated during clinical trials. There is no current standard minimal data set, thus inter-study comparability is hampered. One objective for EMN has been to construct a minimal set of clinical data to be collected from clinical trials available from different sources. This data set will be used to investigate correlations between results from laboratory investigations, clinical disease characteristics and results of therapeutic intervention.
In the absence of uniform reporting systems, the report to clinicians must be expressed clearly. Use of full FISH ISCN is likely to complicate the report and make it more difficult for clinicians to understand and, therefore, this is not recommended. The report should include the method used for PC identification, the probes used, the number of cells scored for each abnormality, and the percentage of abnormal cells.
Clinical reporting consensus
Reports should be clearly expressed and include the method used for PC identification, the probes used, and the number and percentage of cells scored for each abnormality.
A full set of EMN case report forms (CRF) should be defined with a minimal set of data that is required to describe the state of disease, relevant characteristics of diagnosis and clinical course, treatment effects and outcome, and include demographic data of late effects.
A European based FISH data bank linked to clinical data should be generated from the recommendations given in this report.
Central laboratories have to perform the analysis in common clinical trials.
Clinical validation trials
In general, the implementation of new tests into clinical practice suffers from the lack of a formalized stepwise system to evaluate their role and accelerate implementation from the laboratory bench to the clinic. New diagnostic, prognostic and predictive assays will have to pass different stages before they are successfully validated. Similarly to therapeutic trials, four different phases (phases 1–4) are necessary for clinical validation of laboratory data and techniques. In phase 1, the technique is established in the laboratory and analyzed for specificity, sensitivity, reproducibility and accuracy. Phase 2 documents the likely clinical influence in single centers analyzing retrospective data. Phase 3 prepares convincing single center prospective evaluation evolving into the most important phase 4, a multi center prospective evaluation based upon important clinical end points. Ideally, phases 2 and 3 document the usefulness of an assay convincing one or more centers to participate in a prospective phase 4 validation trial. However, no phase 4 studies have yet been performed. Similar development of evidence based recommendations for good clinical practice will benefit from streamlined strategies and form the basis for trials focusing on improving health care.
Clinical validation trials consensus
Participation in prospective phase 4 validation trials is recommended.
Slides should be prepared for central analysis to reduce technical and interlaboratory variations.
Conclusion
Since its introduction, fluorescence in situ hybridization (FISH) analysis has revolutionized genetic analysis and enabled a more precise determination of the presence and frequency of genetic abnormalities. In particular, it is indispensable in myeloma where metaphase cytogenetics has proved problematic given the largely quiescent cells.
FISH probes have been used extensively in myeloma to detect non-random abnormalities in interphase nuclei and the true incidence of chromosome abnormalities has been proven to be much higher than that detected by conventional chromosomal analysis. The availability of a comprehensive line of commercial probes for rapid identification of critical genetic aberrations has contributed to the widespread use of this technique. This has started to identify high-risk populations in myeloma that can be targeted for aggressive therapy; however, more work is needed before this goal is achieved.
Wherever possible, testing should carried out for t(4;14)(p16;q32), t(14;16)(q32;q23), 17p13 deletions, 1q gains (and 1p deletions in patients suitable for autograft). An extended panel may include testing for t(11;14) (q13;q32), t(14;20)(q32;q12), ploidy status, and chromosome 12 and 13 abnormalities. In the context of clinical validation trials, attempts should be made to test for the entire first group of abnormalities.
For a proper understanding of the pathogenesis of plasma cell dyscrasias, it should be realized that the most benefit will come from coordinating and integrating the present and future activities in the various countries.
This document provides some specific recommendations for performing FISH in myeloma and related disorders. The European Myeloma Network aims to build on these initial workshops to provide further education, define standard approaches for specific protocols and establish a common European database, with the aim of defining the emerging molecular genetic subgroups with prognostic and predictive significance.
Footnotes
Funding: this project has been supported by the European Myeloma Network an independent organization supporting research in Europe and in part by the Danish Research Council #2101-07-0007. HEJ was supported by the EU 6th FP to MSCNET (LSHC-CT-2006-037602). The workshops were supported by unrestricted grants to HA-L from Abbott Molecular, Janssen-Cilag and Celgene.
Authorship and Disclosures
The information provided by the authors about contributions from persons listed as authors and in acknowledgments is available with the full text of this paper at www.haematologica.org.
Financial and other disclosures provided by the authors using the ICMJE (www.icmje.org) Uniform Format for Disclosure of Competing Interests are also available at www.haematologica.org.
References
- 1.Hallek M, Bergsagel PL, Anderson KC. Multiple myeloma: increasing evidence for a multistep transformation process. Blood. 1998;91(1):3–21. [PMC free article] [PubMed] [Google Scholar]
- 2.Bergsagel PL, Chesi M, Nardini E, Brents LA, Kirby SL, Kuehl WM. Promiscuous translocations into immunoglobulin heavy chain switch regions in multiple myeloma. Proc Natl Acad Sci USA. 1996;93(24):13931–6. doi: 10.1073/pnas.93.24.13931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chesi M, Bergsagel PL, Brents LA, Smith CM, Gerhard DS, Kuehl WM. Dysregulation of cyclin D1 by translocation into an IgH gamma switch region in two multiple myeloma cell lines. Blood. 1996;88(2):674–81. [PubMed] [Google Scholar]
- 4.Bergsagel PL, Kuehl WM. Chromosome translocations in multiple myeloma. Oncogene. 2001;20(40):5611–22. doi: 10.1038/sj.onc.1204641. [DOI] [PubMed] [Google Scholar]
- 5.Kuehl WM, Bergsagel PL. Multiple myeloma: evolving genetic events and host interactions. Nat Rev Cancer. 2002;2(3):175–87. doi: 10.1038/nrc746. [DOI] [PubMed] [Google Scholar]
- 6.Bergsagel PL, Kuehl WM. Critical roles for immunoglobulin translocations and cyclin D dysregulation in multiple myeloma. Immunol Rev. 2003;194:96–104. doi: 10.1034/j.1600-065x.2003.00052.x. [DOI] [PubMed] [Google Scholar]
- 7.Fonseca R, Debes-Marun CS, Picken EB, Dewald GW, Bryant SC, Winkler JM, Blood E, Oken MM, Santana-Dávila R, González-Paz N, Kyle RA, Gertz MA, Dispenzieri A, Lacy MQ, Greipp PR. The recurrent IgH translocations are highly associated with nonhyperdiploid variant multiple myeloma. Blood. 2003;102(7):2562–7. doi: 10.1182/blood-2003-02-0493. [DOI] [PubMed] [Google Scholar]
- 8.Fonseca R, Barlogie B, Bataille R, Bastard C, Bergsagel PL, Chesi M, Davies FE, Drach J, Greipp PR, Kirsch IR, Kuehl WM, Hernandez JM, Minvielle S, Pilarski LM, Shaughnessy JD, Jr, Stewart AK, Avet-Loiseau H. Genetics and cytogenetics of multiple myeloma: a workshop report. Cancer Res. 2004;64(4):1546–58. doi: 10.1158/0008-5472.can-03-2876. [DOI] [PubMed] [Google Scholar]
- 9.Avet-Loiseau H, Brigaudeau C, Morineau N, Talmant P, Laï JL, Daviet A, Li JY, Praloran V, Rapp MJ, Harousseau JL, Facon T, Bataille R. High incidence of cryptic translocations involving the Ig heavy chain gene in multiple myeloma, as shown by fluorescence in situ hybridization. Genes Chromosomes Cancer. 1999;24(1):9–15. doi: 10.1002/(sici)1098-2264(199901)24:1<9::aid-gcc2>3.0.co;2-k. [DOI] [PubMed] [Google Scholar]
- 10.Avet-Loiseau H, Li JY, Morineau N, Facon T, Brigaudeau C, Harousseau JL, Grosbois B, Bataille R. Monosomy 13 is associated with the transition of monoclonal gammopathy of undetermined significance to multiple myeloma. Intergroupe Francophone du Myélome. Blood. 1999;94(8):2583–9. [PubMed] [Google Scholar]
- 11.Drach J, Angerler J, Schuster J, Rothermundt C, Thalhammer R, Haas OA, Jäger U, Fiegl M, Geissler K, Ludwig H, Huber H. Interphase fluorescence in situ hybridization identifies chromosomal abnormalities in plasma cells from patients with monoclonal gammopathy of undetermined significance. Blood. 1995;86(10):3915–21. [PubMed] [Google Scholar]
- 12.Gutiérrez NC, Camps J, Hernández JM, García JL, Prat E, González MB, Miró R, San Miguel JF. Multicolor fluorescence in situ hybridization studies in multiple myeloma and monoclonal gammopathy of undetermined significance. Hematol J. 2003;4(1):67–70. doi: 10.1038/sj.thj.6200226. [DOI] [PubMed] [Google Scholar]
- 13.Fonseca R, Bailey RJ, Ahmann GJ, Rajkumar SV, Hoyer JD, Lust JA, Kyle RA, Gertz MA, Greipp PR, Dewald GW. Genomic abnormalities in monoclonal gammopathy of undetermined significance. Blood. 2002;100(4):1417–24. [PubMed] [Google Scholar]
- 14.Gutiérrez NC, Castellanos MV, Martín ML, Mateos MV, Hernández JM, Fernández M, et al. Prognostic and biological implications of genetic abnormalities in multiple myeloma undergoing autologous stem cell transplantation: t(4;14) is the most relevant adverse prognostic factor, whereas RB deletion as a unique abnormality is not associated with adverse prognosis. Leukemia. 2007;21(1):143–50. doi: 10.1038/sj.leu.2404413. [DOI] [PubMed] [Google Scholar]
- 15.Stewart AK, Fonseca R. Review of molecular diagnostics in multiple myeloma. Expert Rev Mol Diagn. 2007;7(4):453–9. doi: 10.1586/14737159.7.4.453. [DOI] [PubMed] [Google Scholar]
- 16.Chng WJ, Glebov O, Bergsagel PL, Kuehl WM. Genetic events in the pathogenesis of multiple myeloma. Best Pract Res Clin Haematol. 2007;20(4):571–96. doi: 10.1016/j.beha.2007.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Avet-Loiseau H. Role of genetics in prognostication in myeloma. Best Pract Res Clin Haematol. 2007;20(4):625–35. doi: 10.1016/j.beha.2007.08.005. [DOI] [PubMed] [Google Scholar]
- 18.Fonseca R, Bergsagel PL, Drach J, Shaughnessy J, Gutierrez N, Stewart AK, et al. International Myeloma Working Group molecular classification of multiple myeloma: spotlight review. Leukemia. 2009;23(12):2210–21. doi: 10.1038/leu.2009.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dimopoulos M, Kyle R, Fermand JP, Rajkumar SV, San Miguel J, Chanan-Khan A, et al. Consensus recommendations for standard investigative workup: report of the International Myeloma Workshop Consensus Panel 3. Blood. 2011;117(18):4701–5. doi: 10.1182/blood-2010-10-299529. [DOI] [PubMed] [Google Scholar]
- 20.Wu KL, Beverloo B, Lokhorst HM, Segeren CM, van der Holt B, Steijaert MM, et al. Abnormalities of chromosome 1p/q are highly associated with chromosome 13/13q deletions and are an adverse prognostic factor for the outcome of high-dose chemotherapy in patients with multiple myeloma. Br J Haematol. 2007;136(4):615–23. doi: 10.1111/j.1365-2141.2006.06481.x. [DOI] [PubMed] [Google Scholar]
- 21.Boyd KD, Ross FM, Chiecchio L, Dagrada GP, Konn ZJ, Tapper WJ, et al. A novel prognostic model in myeloma based on co-segregating adverse FISH lesions and the ISS: analysis of patients treated in the MRC Myeloma IX trial. Leukemia. 2012;26(2):349–55. doi: 10.1038/leu.2011.204. [DOI] [PMC free article] [PubMed] [Google Scholar]