

Abstract
Context:
Many anterior cruciate ligament (ACL) injury prevention training programs have been published, but few have assessed the effects of training on both ACL injury rates and athletic performance tests.
Objective:
To determine if ACL injury prevention programs have a positive influence on both injury rates and athletic performance tests in female athletes.
Data sources:
In August 2011, a search was conducted (1995–August 2011) of the PubMed, Science Direct, and CINAHL databases.
Study selection:
Selected studies determined the effect of ACL intervention training programs on ACL incidence rates (determined by athlete-exposures) and athletic performance tests, such as isokinetic strength, vertical jump height, speed, agility, and dynamic balance. Because no single article contained both criteria, investigations were cross-referenced to obtain data on both factors from the same training programs.
Data extraction:
The authors reviewed the selected studies for cohort population numbers, age, sports, duration of study, program components, duration of training, number of athlete-exposures, ACL injury incidence rates, and results of athletic performance tests.
Results:
Initially, 57 studies were identified that described 42 ACL injury prevention training programs. Of these, 17 studies that investigated 5 programs met the inclusion criteria. Two programs significantly reduced ACL injury rates and improved athletic performance tests: Sportsmetrics and the Prevent Injury and Enhance Performance program (PEP). Sportsmetrics produced significant increases in lower extremity and abdominal strength, vertical jump height, estimated maximal aerobic power, speed, and agility. Prevent Injury and Enhance Performance significantly improved isokinetic knee flexion strength but did not improve vertical jump height, speed, or agility. The other 3 programs (Myklebust, the “11,” and Knee Ligament Injury Prevention) did not improve both ACL injury rates and athletic performance tests.
Conclusions:
Only the Sportsmetrics and PEP ACL intervention training programs had a positive influence on injury reduction and athletic performance tests.
Keywords: anterior cruciate ligament, injury prevention, athletic performance tests
It is well known that adolescent and adult female athletes have a 4- to 8-fold higher incidence of sustaining a serious noncontact anterior cruciate ligament (ACL) injury compared with male athletes participating in the same sport or activity.1,12,17 For over 15 years, investigators have developed a variety of ACL injury prevention programs in an effort to decrease this problem. The programs vary greatly in the components that form the intervention, as well as the duration and intensity of training. Consensus statements from research retreats and committees agree that the ideal ACL injury prevention program remains somewhat unclear because of the complex, multifaceted problem of the injury itself.24,25 A recent meta-analysis of published programs determined that plyometric and strengthening components were more important than balance training and that the favorable effects of training were most pronounced in female soccer players younger than 18 years.30
Recently, investigators have recommended that ACL injury prevention programs be evaluated to determine their effect on athletic performance tests,25 because if these programs have a positive influence on both injury reduction and athletic performance factors, then compliance with training may be greatly increased. The tremendous short- and long-term consequences of ACL injuries lend credence to intervention programs becoming widespread. Convincing athletes, parents, coaches, and others of the necessity for injury prevention training may be less challenging if evidence exists that athletic performance indices will also benefit. However, to our knowledge, few of these training programs have undergone a rigorous assessment of their ability to decrease noncontact ACL injuries in female athletes and improve measures of athletic performance, such as strength, speed, agility, and dynamic balance. The purpose of this literature review was to determine if ACL injury prevention programs affect injury rates and results of athletic performance tests in female athletes.
Methods
Study Search Strategy
In August 2011, a search was conducted of the PubMed, Science Direct, and CINAHL databases (1995–August 2011). The start date was 1995 because that was the year of the first known published ACL injury intervention program.6 The following keywords were used: knee ligament injury prevention, anterior cruciate ligament injury prevention, ACL injury prevention, ACL injury prevention programs, and women knee ligament injury prevention. Manual searches were conducted of the following journals published during this period: American Journal of Sports Medicine, Arthroscopy, Journal of Bone and Joint Surgery (American and British volumes), Knee, Clinical Orthopaedics and Related Research, and Knee Surgery Sports Traumatology and Arthroscopy. Review articles and meta-analyses were initially included so that all possible original studies were located that examined the effects of ACL intervention training programs on ACL injury rates and athletic performance tests involving female athletes. Only studies in peer-reviewed journals were considered. In addition, the reference lists of included studies were searched for relevant articles. No dissertations, articles from meeting proceedings, or textbook chapters were reviewed.
Study Selection Criteria
The inclusion criteria were English-language studies that contained (1) ACL injury prevention training programs for female athletes, (2) athlete-exposure data, (3) effect of training on ACL incidence rates for female athletes as determined by athlete-exposures, and (4) assessment of athletic performance tests before and after participation in the ACL intervention program. The exclusion criteria were studies of ACL injury intervention programs involving only male athletes, studies that combined data from male and female athletes, and investigations that used only video awareness or cognitive training techniques. In addition, studies were not included that used only a portion of an original program described elsewhere.
Initially, 57 studies were identified that described 42 ACL injury prevention training programs (Figure 1). Each study was reviewed to determine if the other inclusionary criteria were met. No single study contained athlete-exposures, ACL incidence rates, and changes in athletic performance tests resulting from an intervention program. Therefore, studies that provided data on athletic performance tests as a result of training were cross-referenced to determine if the same intervention program had published athlete-exposures and ACL injury incidence rates elsewhere. In a similar manner, studies that published ACL injury incidence rates were manually checked to determine if another study had determined changes in athletic performance tests as a result of the same program. Studies were included that added exercises or drills to an original program but did not delete any portion of the original program.
Figure 1.

Schema for selected studies in the systematic review.
Data Analysis and Abstraction
The data from each study that met the inclusion criteria were abstracted for (1) cohort population numbers, age, sports, duration of study; (2) ACL injury intervention program components and duration of training; (3) number of athlete-exposures; (4) ACL injury incidence rates according to athlete-exposures; (5) athletic performance tests; and (6) the results of the athletic performance tests before and after the ACL intervention program. A standardized rating of each study was not included in this review.
Results
Study Selection
Of the initial 57 studies, 40 were excluded (Figure 1), leaving 17 studies (Table 1). There were 5 ACL intervention programs assessed in these studies: Sportsmetrics,3,9,10,19-21,29 Myklebust,11,18 Knee Ligament Injury Prevention (KLIP),13,23 Prevent Injury and Enhance Performance (PEP),7,15,16,28 and the “11.”26,27
Table 1.
Studies selected for review: 5 ACL intervention programs.a
| Program | Factors Studied | Additional Program Components | Program Duration | |
|---|---|---|---|---|
| Exposures, ACL Injuries | Athletic Performance Tests | |||
| Sportsmetricsb | ||||
| Hewett10 | No | Yes | None | 60-90 min, 3 d/wk for 6 wk |
| Hewett9 | Yes | No | None | 60-90 min, 3 d/wk for 6 wk |
| Wilkerson29 | No | Yes | None | 60-90 min, 3 d/wk for 6 wk |
| Noyes19 | No | Yes | None | 60-90 min, 3 d/wk for 6 wk |
| Barber-Westin3 | No | Yes | Tennis-specific agility and performance drills, core and upper body strength, speed. | 90 min, 3 d/wk for 6 wk |
| Noyes20 | No | Yes | Volleyball-specific performance and agility drills, core and upper body strength, speed, reaction. | 90-120 min, 3 d/wk for 6 wk |
| Noyes21 | No | Yes | Basketball-specific performance and agility drills, core and upper body strength, speed, reaction, endurance. | 90-120 min, 3 d/wk for 6 wk |
| Myklebustc | ||||
| Myklebust18 | Yes | No | None | 15 min, 3 d/wk for 5-7 wk, then 1 d/wk for season |
| Holm11 | No | Yes | None | 15 min, 3 d/wk for 5-7 wk, then 1 d/wk for season |
| KLIPd | ||||
| Pfeiffer23 | Yes | No | None | 20 min, 2 d/wk for 1 season |
| Irmischer13 | No | Yes | None | 20 min, 2 d/wk for 9 wk, off-season |
| PEPe | ||||
| Mandelbaum16 | Yes | No | None | 20 min, warm-up for 1 season |
| Gilchrist7 | Yes | No | None | 20 min, warm-up for 1 season |
| Lim15 | No | Yes | Added 5 alternative exercises for warm-down | 20 min, warm-up for 8 wk in-season |
| Vescovi28 | No | Yes | None | 20 min, warm-up for 12 wk in-season |
| the “11”f | ||||
| Steffen27 | Yes | No | None | 15 min, warm-up 15 sessions, then 1 d/wk for rest of season |
| Steffen26 | No | Yes | None | 15 min, warm-up, 3 d/wk for 10 wk in season |
ACL, anterior cruciate ligament. KLIP, Knee Ligament Injury Prevention program; PEP, Prevent Injury and Enhance Performance.
Original ACL intervention program components: plyometrics, strength, agility, flexibility. All studies done preseason.
Original ACL intervention program components: agility, balance mats and boards.
Original ACL intervention program components: plyometrics, agility.
Original ACL intervention program components: plyometrics, strength, agility, flexibility.
Original ACL intervention program components: plyometrics, strength, agility, balance mats and boards.
ACL Intervention Programs
All the intervention programs included agility exercises, and all but Myklebust18 included plyometrics. Strength training was conducted in the Sportsmetrics, PEP, and the “11” programs10,16,27; flexibility, Sportsmetrics and PEP10,16; and balance mats or boards, Myklebust and the “11.”18,27 Training varied from 15 minutes to 90 to 120 minutes. PEP, Myklebust, and the “11”16,18,23,27 were done during the season, while Sportsmetrics10 was conducted for 6 weeks before the athletic season began. The subjects in the programs were usually high school or collegiate athletes, although Myklebust’s program was done in elite female handball players whose ages were not provided.18
The Sportsmetrics and PEP programs resulted in statistically significant decreases in the ACL injury incidence rates as determined by athlete-exposures in high school female athletes participating in basketball and soccer (Table 2).9,16 In a separate analysis of collegiate athletes, the PEP program7 approached statistical significance in reduction of the ACL injury rate (P = 0.066). Myklebust, KLIP, and “11”18,23,27 failed to have a significant effect on ACL injury incidence rates.
Table 2.
Athlete exposures and ACL injury rates from studies selected for review.a
| Program | Population, Sport, Age Group | Athlete-Exposures, No. | ACL Injury Incidence Rate, No.b | P |
|---|---|---|---|---|
| Sportsmetrics | ||||
| Hewett9 | High school soccer, basketball, volleyball players | Noncontact ACL injuries | 0.01 | |
| Female trained (n = 366) | 23 138 trained females | 0 trained females | ||
| Female control (n = 463) | 17 222 control females | 5 (0.35) control females | ||
| Male control (n = 434) | 21 390 control males | 1 (0.05) control males | ||
| Myklebust | ||||
| Myklebust18 | Elite team handball players | |||
| Female trained (n = 1705) | 359 497 trained females | 29 (0.14) trained | 0.15 | |
| Female control (n = 942) | 208 936 control | 40 (0.11) control | ||
| KLIP | ||||
| Pfeiffer23 | High school soccer players | Noncontact ACL injuries | NS | |
| Female trained (n = 189) | 17 954 trained | 3 trained (0.167) trained | ||
| Female control (n = 244) | 38 662 control | 3 control (0.078) control | ||
| PEP | ||||
| Mandelbaum16 | High school soccer players | Noncontact ACL injuries | < 0.0001 | |
| Female trained (n = 1885) | 67 860 trained | 6 trained (0.09) trained | ||
| Female control (n = 3818) | 137 448 control | 67 control (0.49) control | ||
| Gilchrist7 | Collegiate soccer players | Noncontact ACL injuries | 0.066 | |
| Female trained (n = 583) | 35 220 trained | 2 (0.057) trained | ||
| Female control (n = 852) | 52 919 control | 10 (0.189) control | ||
| the “11” | ||||
| Steffen27 | High school soccer players | All ACL injuries | ||
| Female trained (n = 1073) | 66 423 trained | 4 (0.06) trained | 0.73 | |
| Female control (n = 947) | 65 725 control | 5 (0.08) control | ||
ACL, anterior cruciate ligament; KLIP, Knee Ligament Injury Prevention program; PEP, Prevent Injury and Enhance Performance; NS, not significant (P value not given).
Per 1000 athlete-exposures.
Aspects of Athletic Performance
Nine factors that represented athletic performance were measured in a total of 270 female athletes in 11 investigations (Table 3): vertical jump height,10,13,15,20,21,26,28 lower extremity isokinetic strength,10,11,15,19,26,29 speed,3,21,26,28 abdominal strength,3,20 lower limb symmetry on hop tests,3,11 estimated maximal aerobic power (VO2 max),20,21 agility,3,28 hip muscle strength,15,26 and sports-specific tasks.3
Table 3.
Results of athletic performance tests from studies selected for review.a
| Program/Author: Test | Participants: Results |
|---|---|
| Sportsmetrics | |
| Hewett10 | High school volleyball players: female trained (n = 11), male control (n = 9) |
| Strength | Isokinetic knee flexion: increased nondominant leg (P = 0.01) Hamstrings power: increased dominant leg (P = 0.0001) and nondominant leg (P = 0.02) Hamstrings:quadriceps ratio: increased nondominant leg (P < 0.01) and dominant leg (P < 0.05) |
| Vertical jump | Countermovement: increased mean 3.81 ± 1.27 cm (P = 0.016) |
| Wilkerson29 | Collegiate female basketball players: trained (n = 11), control (n = 8) |
| Strength | Isokinetic knee flexion: increased dominant leg (P = 0.008) |
| Noyes19 | High school female athletes: trained (n = 62) |
| Strength | Isokinetic knee flexion: increased both legs (P < 0.0001) Hamstrings:quadriceps ratio: increased nondominant leg (P = 0.001) |
| Barber-Westin3 | Tennis: trained females (n = 10), trained males (n = 5), 11-16 y |
| Strength | Abdominal endurance test: increased mean, 53 s (P = 0.01) |
| Speed | Improved 1-court (P < 0.0001) and 2-court (P = .02) suicide runs |
| Agility | Improved forehand (P = .006), backhand (P = .0008) baseline tests Improved service line test (P = 0.0009) |
| Limb symmetry, dynamic balance | Single-leg crossover triple hop for distance: increased both legs (P ≤ 0.05) Single-leg hop for distance: no significant increase |
| Noyes20 | High school female volleyball players: trained (n = 34) |
| Strength | Sit-up test: increased mean 2.7 ± 4.8 reps (P = 0.03) |
| Vertical jump | Countermovement: increased mean 1.2 ± 5.2 cm (P = 0.05) |
| Estimated VO2 max (mL·kg·min) | Increased mean from 39.4 ± 4.8 to 41.4 ± 4.0 (P < 0.001) |
| Noyes21 | High school female basketball players: trained (n = 57) |
| Vertical jump | Countermovement: increased mean 2.3 ± 3.4 cm (P < 0.0001) |
| Speed | 18 m: no significant increase |
| Estimated VO2 max (mL·kg·min) | Increased mean from 34.6 ± 4.5 to 39.5 ± 5.7 (P < 0.0001) |
| Myklebust | |
| Holm11 | Elite female team handball players: trained (n = 27) |
| Strength | Isokinetic: no significant increase knee flexors or extensors or hamstrings:quadriceps ratio |
| Limb symmetry, dynamic balance | 2-leg dynamic balance test: significant improvement (P = 0.01) Single-leg hop, triple jump, stair hop: no significant increase |
| KLIP | |
| Irmischer13 | Collegiate female active students: trained (n = 14), control (n = 14) |
| Vertical jump | Countermovement: no significant increase |
| PEP | |
| Lim15 | High school female basketball players: trained (n = 11), control (n = 11) |
| Strength | Isokinetic: significant increase hip abductors, hip extensors, knee flexors (P < 0.05), significant improvement hamstrings:quadriceps ratio (P = 0.02) |
| Vertical jump | Rebound jump: no significant increase |
| Vescovi28 | High school female soccer players: trained (n = 15), control (n = 16) |
| Vertical jump | Countermovement: no significant increase |
| Speed | 9.1 m, 18.2 m: no significant improvement 27.3 m, 36.6 m: small improvements (< 0.10 s) after 6 weeks, return baseline values at 12 weeks |
| Agility | Illinois, pro-agility tests: 2%-4% decline |
| the “11” | |
| Steffen26 | High school female soccer players: trained (n = 18), control (n = 16) |
| Strength | Isokinetic and isometric: no significant increase lower extremity or hip strength |
| Vertical jump | Countermovement, drop jump, rebound jump: no significant increase |
| Speed | 40 m: no significant increase |
| Sport-specific tasks | Speed dribbling, shooting distance: no significant increase |
KLIP, Knee Ligament Injury Prevention program; PEP, Prevent Injury and Enhance Performance.
The Sportsmetrics program resulted in significant increases in athletic performance in several investigations encompassing 185 females.3,10,19-21,29 The original Sportsmetrics program improved isokinetic knee flexion peak torque values,10,19,29 hamstrings:quadriceps ratio,10,19 and countermovement vertical jump (CVJ) height.10 Sports-specific Sportsmetrics programs demonstrated significant improvements in abdominal strength,3,20 estimated VO2 max using the multistage fitness test20,21 (Figure 2), CVJ height,20,21 speed on suicide runs,3 distance hopped on a single-leg crossover hop,3 and agility measures specific for tennis players.3 Two performance indices measured did not show significant improvement: the 18-m sprint in basketball players21 and the single-leg hop for distance in tennis players.3
Figure 2.

A significant difference was found in the multistage fitness test in the distribution of female basketball players in the categories shown before and after Sportsmetrics training (P < 0.0001) for estimated VO2 max (mL·kg−1·min−1): poor, < 31.0; fair, 31 to 34.9; good, 35.0 to 38.9; excellent/superior, ≥ 39.0.21
The PEP program significantly improved isokinetic peak torques for hip abduction, hip extension, knee flexion, and hamstrings:quadriceps ratio in 11 high school female basketball players who were trained for 8 weeks (Figure 3).15 However, there was no significant improvement in vertical jump height on a rebound task. In a separate study, no significant improvements were noted in CVJ height, sprint speed (9.1, 18.2, 27.3, or 36.6 m), or agility on the Illinois and pro-agility tests in 15 high school soccer athletes who trained for 12 weeks.28
Figure 3.
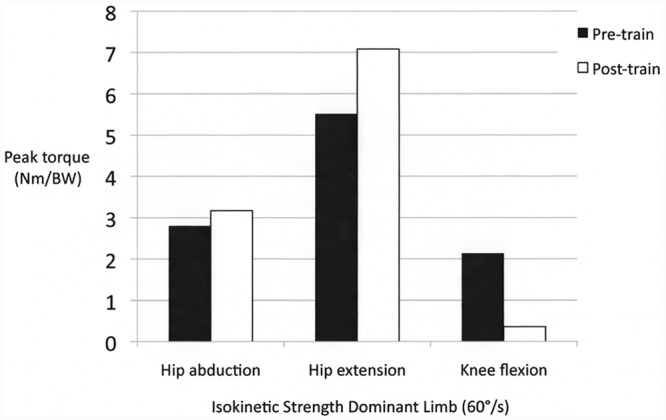
Statistically significant improvements were found in the mean isokinetic peak torque values for hip abduction, hip extension, and knee flexion in 11 collegiate female basketball players following neuromuscular training based on the Prevent Injury and Enhance Performance program (P < 0.05).14
For 27 female elite team handball players, the Myklebust ACL intervention program significantly improved 2-legged dynamic balance measured on a moveable platform device (KAT 2000, OEM Medical, Carlsbad, California) after 1 year of training.11 However, there were no significant increases in isokinetic lower extremity muscle strength, single-leg static balance, or distance hopped on single-leg function tests.
The “11” program failed to significantly improve CVJ height, 40-m sprint speed, a speed dribbling test, or a shooting distance test in 18 athletes who trained for 10 weeks.26 The KLIP program did not produce a significant increase in CVJ height in 14 athletes who trained for 9 weeks.13
Discussion
The goal of this review was to determine if ACL injury prevention training programs have a positive influence on ACL injury reduction and athletic performance tests. The literature search yielded 57 studies published from 1995 to 2011 that described 42 ACL injury prevention training programs. Only 5 of these programs have published data regarding the effect of training on both criteria. Many studies have focused on only the effect of ACL intervention training on knee kinematics and kinetics without determining if the program significantly reduces the incidence of this injury in female athletes. While the ability of neuromuscular, cognitive, and other methods of training to alter potentially deleterious moments, forces, and body mechanics is important to understand, the transfer of these changes to real-world athletic competition and reduction of noncontact ACL injury rates is just as crucial.
Some studies reporting ACL injury rates following intervention programs did not use athlete-exposures to determine the injury rates. Noyes et al22 and Knowles et al14 stressed the importance of using incidence rates (number of injuries divided by the number of athlete-exposures) for sports injury research because this unit of measure is based on the epidemiologic concept of person-time at risk and it accounts for variation in exposure between athletes and teams. This method is widely preferred over that of a clinical incidence rate, which is calculated by dividing the number of injuries by the number of athletes at risk. The clinical incidence method does not provide a valid estimate or a true rate of injury.14
Shultz et al25 recently summarized findings from the 2010 ACL Research Retreat V, which observed that a public health approach should be developed to help prevent ACL injuries in young athletes. Questions were raised pertaining to improved participation, compliance, and effectiveness of ACL injury prevention programs. These include developing an understanding of the multiple factors that influence the successful implementation of these programs; one recommendation was to evaluate if injury prevention programs positively or negatively affect athletic performance indices. This systematic review determined that few published ACL intervention programs have both significantly reduced the incidence of ACL injury and improved aspects of athletic performance, such as strength, speed, and agility (Table 4). The number of athletes who underwent performance testing after training was typically small, ranging from 11 to 27. Another problem is that all programs except Sportsmetrics were conducted during the course of an athletic season. It is therefore not possible to determine whether the changes in such indices as strength and balance occurred as a result of the intervention training program, participation in practices and games, sports-specific training, or a combination thereof. Significant increases in hamstrings isokinetic strength and improvements in the hamstrings:quadriceps ratio were achieved with only the Sportsmetrics and PEP programs. It has been well established that female athletes typically have poor hamstrings strength,4 which is considered one possible risk factor for ACL ruptures.2
Table 4.
Findings for ACL injury prevention training programs.a
| Athletic Performance Tests, No. | |||
|---|---|---|---|
| Program | ACL Incidence Rate Significantly Reduced? | Improved | Not Improved |
| Sportsmetrics | Yes | 9b | 2c |
| PEP: high school basketball | Yes | 4d | 3e |
| Myklebust | No | 1f | 3g |
| KLIP | No | 0 | 1h |
| the “11” | No | 0 | 5i |
| PEP: high school soccer | No | 0 | 7j |
ACL, anterior cruciate ligament; KLIP, Knee Ligament Injury Prevention program; PEP, Prevent Injury and Enhance Performance.
Isokinetic knee flexion, hamstrings power, hamstrings:quadriceps ratio, abdominal strength, vertical jump, speed on suicide runs, agility, estimated VO2 max, distance hopped on single-leg triple crossover hop.
18-m sprint, distance hopped on single-leg hop.
Isokinetic hip abduction, hip extension, knee flexion, hamstrings:quadriceps ratio.
Vertical jump, speed, agility.
2-leg dynamic balance.
Isokinetic strength knee flexors or extensors, hamstrings:quadriceps ratio, distance hopped on 3 single-leg tests.
Vertical jump.
Isokinetic leg strength, isometric hip strength, vertical jump, speed, sports-specific tasks.
Vertical jump; sprints (9.1, 18.2, 27.3, 36.6 m); Illinois agility, pro-agility tests.
Debate continues regarding the components that ACL injury prevention training programs should contain, as well as the frequency and duration of training (Figure 4). Compliance rates with training vary widely, and the factors causing this discrepancy remain unclear. Steffen et al26,27 concluded that the disappointing results from their studies on the “11” training program were due to low volume and training intensity and poor athlete compliance. Pfeiffer et al23 believed that the lack of strength training may have played a role in the lack of a training effect of their KLIP program on the ACL injury rate. This occurred even though a previous study13 had found a beneficial effect of this program on reduced peak impact forces on landing. That study involved 14 collegiate women who were physically active, while the Pfeiffer study focused on high school soccer players. Although Myklebust et al18 did not find a significant reduction in noncontact ACL injury rates with their training program in female team handball players, they did note a compliance effect in the subgroup of elite players. The authors speculated that the elite teams may have had a greater motivation to perform the training program because of problems with players sustaining ACL injuries in previous years. They also had more practices per week than other teams, which could have provided more opportunities to complete the training program.
Figure 4.

Training examples from the 2 training programs that had a positive influence on anterior cruciate ligament injury reduction and athletic performance test results in female athletes: Sportsmetrics and Prevent Injury and Enhance Performance. A, barrier hop forward-backward20; B, barrier hop side-to-side; C, walking lunge; and D, agility reaction–instructor cued.20
Even though some authors maintain that ACL intervention programs that involve 60 to 120 minutes of training for 3 days a week are difficult to conduct,5,8 the most effective program in this review in regard to athletic performance enhancement was Sportsmetrics, which requires this amount of time. It is not known if the newer sports-specific programs are also effective in significantly reducing the incidence of ACL injuries. It is also not known if the improvement in fitness and functional indices as a result of ACL injury prevention training translates into enhanced player performance during competition. Future studies of programs shorter in duration may consider conducting the intervention before the start of the athletic season so that the effect of the training alone on athletic performance indices may be measured.
Conclusions
This systematic review identified 42 ACL injury prevention training programs in the English literature. Only the Sportsmetrics and PEP programs had a positive influence on injury reduction and athletic performance test results in female athletes.
References
- 1. Agel J, Arendt EA, Bershadsky B. Anterior cruciate ligament injury in national collegiate athletic association basketball and soccer: a 13-year review. Am J Sports Med. 2005;33(4):524-530 [DOI] [PubMed] [Google Scholar]
- 2. Alentorn-Geli E, Myer GD, Silvers HJ, et al. Prevention of non-contact anterior cruciate ligament injuries in soccer players: part 1. Mechanisms of injury and underlying risk factors. Knee Surg Sports Traumatol Arthrosc. 2009;17(7):705-729 [DOI] [PubMed] [Google Scholar]
- 3. Barber-Westin SD, Hermeto AA, Noyes FR. A 6-week neuromuscular training program for competitive junior tennis players. J Strength Cond Res. 2010;24(9):2372-2382 [DOI] [PubMed] [Google Scholar]
- 4. Barber-Westin SD, Noyes FR, Galloway M. Jump-land characteristics and muscle strength development in young athletes: a gender comparison of 1140 athletes 9 to 17 years of age. Am J Sports Med. 2006;34(3):375-384 [DOI] [PubMed] [Google Scholar]
- 5. Chappell JD, Limpisvasti O. Effect of a neuromuscular training program on the kinetics and kinematics of jumping tasks. Am J Sports Med. 2008;36(6):1081-1086 [DOI] [PubMed] [Google Scholar]
- 6. Ettlinger CF, Johnson RJ, Shealy JE. A method to help reduce the risk of serious knee sprains incurred in alpine skiing. Am J Sports Med. 1995;23(5):531-537 [DOI] [PubMed] [Google Scholar]
- 7. Gilchrist J, Mandelbaum BR, Melancon H, et al. A randomized controlled trial to prevent noncontact anterior cruciate ligament injury in female collegiate soccer players. Am J Sports Med. 2008;36(8):1476-1483 [DOI] [PubMed] [Google Scholar]
- 8. Herrington L. The effects of 4 weeks of jump training on landing knee valgus and crossover hop performance in female basketball players. J Strength Cond Res. 2010;24(14):3427-3432 [DOI] [PubMed] [Google Scholar]
- 9. Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes: a prospective study. Am J Sports Med. 1999;27(6):699-706 [DOI] [PubMed] [Google Scholar]
- 10. Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes: decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24(6):765-773 [DOI] [PubMed] [Google Scholar]
- 11. Holm I, Fosdahl MA, Friis A, Risberg MA, Myklebust G, Steen H. Effect of neuromuscular training on proprioception, balance, muscle strength, and lower limb function in female team handball players. Clin J Sport Med. 2004;14(2):88-94 [DOI] [PubMed] [Google Scholar]
- 12. Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train. 2007;42(2):311-319 [PMC free article] [PubMed] [Google Scholar]
- 13. Irmischer BS, Harris C, Pfeiffer RP, DeBeliso MA, Adams KJ, Shea KG. Effects of a knee ligament injury prevention exercise program on impact forces in women. J Strength Cond Res. 2004;18(4):703-707 [DOI] [PubMed] [Google Scholar]
- 14. Knowles SB, Marshall SW, Guskiewicz KM. Issues in estimating risks and rates in sports injury research. J Athl Train. 2006;41(2):207-215 [PMC free article] [PubMed] [Google Scholar]
- 15. Lim BO, Lee YS, Kim JG, An KO, Yoo J, Kwon YH. Effects of sports injury prevention training on the biomechanical risk factors of anterior cruciate ligament injury in high school female basketball players. Am J Sports Med. 2009;37(9):1728-1734 [DOI] [PubMed] [Google Scholar]
- 16. Mandelbaum BR, Silvers HJ, Watanabe DS, et al. Effectiveness of a neuromuscular and proprioceptive training program in preventing anterior cruciate ligament injuries in female athletes: 2-year follow-up. Am J Sports Med. 2005;33(7):1003-1010 [DOI] [PubMed] [Google Scholar]
- 17. Mountcastle SB, Posner M, Kragh JF, Jr, Taylor DC. Gender differences in anterior cruciate ligament injury vary with activity: epidemiology of anterior cruciate ligament injuries in a young, athletic population. Am J Sports Med. 2007;35(10):1635-1642 [DOI] [PubMed] [Google Scholar]
- 18. Myklebust G, Engebretsen L, Braekken IH, Skjolberg A, Olsen OE, Bahr R. Prevention of anterior cruciate ligament injuries in female team handball players: a prospective intervention study over three seasons. Clin J Sport Med. 2003;13(2):71-78 [DOI] [PubMed] [Google Scholar]
- 19. Noyes FR, Barber-Westin SD, Fleckenstein C, Walsh C, West J. The drop-jump screening test: difference in lower limb control by gender and effect of neuromuscular training in female athletes. Am J Sports Med. 2005;33(2):197-207 [DOI] [PubMed] [Google Scholar]
- 20. Noyes FR, Barber-Westin SD, Smith ST, Campbell T. A training program to improve neuromuscular indices in female high school volleyball players. J Strength Cond Res. In press, 2012 [DOI] [PubMed] [Google Scholar]
- 21. Noyes FR, Barber-Westin SD, Tutalo Smith S, Campbell T, Garrison TT. A training program to improve neuromuscular and performance indices in female high school basketball players. J Strength Cond Res. 2011;25(8):2151-2160 [DOI] [PubMed] [Google Scholar]
- 22. Noyes FR, Lindenfeld TN, Marshall MT. What determines an athletic injury (definition)? Who determines an injury (occurrence)? Am J Sports Med. 1988;16(suppl 1):S65-S68 [DOI] [PubMed] [Google Scholar]
- 23. Pfeiffer RP, Shea KG, Roberts D, Grandstrand S, Bond L. Lack of effect of a knee ligament injury prevention program on the incidence of noncontact anterior cruciate ligament injury. J Bone Joint Surg Am. 2006;88(8):1769-1774 [DOI] [PubMed] [Google Scholar]
- 24. Renstrom P, Ljungqvist A, Arendt E, et al. Non-contact ACL injuries in female athletes: an International Olympic Committee current concepts statement. Br J Sports Med. 2008;42(6):394-412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Shultz SJ, Schmitz RJ, Nguyen AD, et al. ACL Research Retreat V: an update on ACL injury risk and prevention, March 25-27, 2010, Greensboro, NC. J Athl Train. 2010;45(5):499-508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Steffen K, Bakka HM, Myklebust G, Bahr R. Performance aspects of an injury prevention program: a ten-week intervention in adolescent female football players. Scand J Med Sci Sports. 2008;18(5):596-604 [DOI] [PubMed] [Google Scholar]
- 27. Steffen K, Myklebust G, Olsen OE, Holme I, Bahr R. Preventing injuries in female youth football: a cluster-randomized controlled trial. Scand J Med Sci Sports. 2008;18(5):605-614 [DOI] [PubMed] [Google Scholar]
- 28. Vescovi JD, VanHeest JL. Effects of an anterior cruciate ligament injury prevention program on performance in adolescent female soccer players. Scand J Med Sci Sports. 2010;20(3):394-402 [DOI] [PubMed] [Google Scholar]
- 29. Wilkerson GB, Colston MA, Short NI, Neal KL, Hoewischer PE, Pixley JJ. Neuromuscular changes in female collegiate athletes resulting from a plyometric jump-training program. J Athl Train. 2004;39(1):17-23 [PMC free article] [PubMed] [Google Scholar]
- 30. Yoo JH, Lim BO, Ha M, et al. A meta-analysis of the effect of neuromuscular training on the prevention of the anterior cruciate ligament injury in female athletes. Knee Surg Sports Traumatol Arthrosc. 2010;18(6):824-830 [DOI] [PubMed] [Google Scholar]