

Abstract
Background
A minority of patients with adult acute lymphoblastic leukemia who relapse are rescued. The aim of this population-based study was to assess the results of reinduction treatment and allogeneic stem cell transplantation in patients in second complete remission.
Design and Methods
Between 2003–2007, 76 adults (<66 years) with relapsed acute lymphoblastic leukemia (Burkitt’s leukemia excluded) were prospectively reported to The Swedish Adult Acute Leukemia Registry and later evaluated.
Results
Reinduction with: (i) mitoxantrone, etoposide, and cytarabine (MEA); (ii) fludarabine, cytarabine, pegylated-asparaginase plus granulocyte colony-stimulating factor (FLAG-Asp); and (iii) cytarabine, betamethasone, cyclophosphamide, daunorubicin, and vincristine (ABCDV) resulted in complete remission in 6/9 (67%), 10/16 (63%) and 9/21 (43%) of the patients, respectively. Allogeneic stem cell transplantation was performed during second complete remission in 29 patients. Multivariate analysis regarding overall survival after relapse revealed that age over 35 years at diagnosis and relapse within 18 months were negative prognostic factors. Overall survival rates at 3 and 5 years were 22% (95% CI: 13–32) and 15% (95% CI: 7–24). Of 19 patients less than 35 years at diagnosis who underwent allogeneic stem cell transplantation in second remission, ten (53%) are still alive at a median of 5.5 years (range, 4.2–8.3) after relapse, whereas all patients over 35 years old at diagnosis have died.
Conclusions
Allogeneic stem cell transplantation remains the treatment of choice for young adults with relapsed acute lymphoblastic leukemia. Both (i) mitoxantrone, etoposide, and cytarabine and (ii) fludarabine, cytarabine, pegylated-asparaginase plus granulocyte colony-stimulating factor seem effective as reinduction treatments and should be further evaluated. New salvage strategies are needed, especially for patients over 35 years old at diagnosis.
Keywords: adult acute lymphoblastic leukemia, relapse, salvage therapy, allogeneic stem cell transplantation, prognostic factors
Introduction
Acute lymphoblastic leukemia (ALL) in adults has an unsatisfactory prognosis despite efforts to improve long-term outcome with strategies such as adaptation of pediatric protocols,1,2 use of tyrosine kinase inhibitors in Philadelphia chromosome-positive disease3 and allogeneic stem cell transplantation (SCT) in first complete remission (CR1).4–6 Primary chemotherapy-resistant disease is unusual and CR1 can be reached in 90% of Philadelphia chromosome-negative patients with novel protocols,1,7 but relapse is frequent, especially in patients over 35 years of age at diagnosis. This age group is considered as high-risk both at diagnosis7,8 and relapse.9 Prognosis remains very poor for relapsing patients, with approximately 40% achieving second complete remission (CR2) through salvage regimens and only 7–12% becoming long-term survivors.10–12 Allogeneic SCT seems to be the best consolidation option for adult patients with relapsed ALL,10–12 although only a minority of such patients are eligible for the procedure as a result of poor performance status, lack of a donor or short duration of CR2. Achieving CR2 after relapse is an important aim for patients who are considered for allogeneic SCT.11 If relapse occurs after SCT the long-term outcome is dismal, although donor lymphocyte infusions with or without chemotherapy or a second transplant are used in attempts to improve survival.11
We present here the results of a national, multicenter, prospective, population-based study of outcome among adult patients aged 19 to 65 years with ALL relapse diagnosed during 2003–2007 in Sweden. Most of the patients had primary treatment according to national guidelines for ALL, as recommended by the Swedish Adult ALL Group (SVALL). The guidelines suggest two different treatment protocols for early relapses, and retreatment according to the initial therapy for late relapses, with the intention to proceed to allogeneic SCT in CR2 for eligible patients. The aim of the current study was to assess outcome among adult patients after first ALL relapse, and the utilization and efficacy of recommended protocols and of allogeneic SCT in this setting.
Design and Methods
Patients
Adult patients with first relapse of ALL were prospectively reported to The Swedish Acute Leukemia Registry in 2003–2007. The Swedish Acute Leukemia Registry is a truly population-based registry containing data on patients diagnosed with acute leukemia since 1997, with 98% coverage.13 Missing data were added retrospectively. Patients older than 66 years at relapse were excluded from this analysis as not being eligible for allogeneic SCT, as were patients with Burkitt’s leukemia. Informed consent was obtained from all patients. The date of last follow-up of the survivors was 3rd June 2011. The study was approved by the regional ethical review board in Uppsala.
Initial diagnostics and treatment
Diagnostics and treatment at primary diagnosis of ALL were performed at each center according to the national guidelines. Induction therapy consisted of cytarabine, betamethasone, cyclophosphamide, daunorubicin, and vincristine (ABCDV)/vincristine, cytarabine, betamethasone, and amsacrine (VABA) for B-precursor ALL, as previously described,14 and hyper-CVAD for T-ALL.15 Asparaginase was not incorporated in either the induction or consolidation protocol. Complementary use of tyrosine kinase inhibitors in Philadelphia chromosome-positive ALL was not mandatory in this period except for refractory or relapsed disease.
High-risk ALL was defined by the presence of at least one of the following criteria: white blood cell (WBC) count >30×109/L (>100×109/L for T-ALL), central nervous system disease, more than one course required to achieve CR1, Philadelphia-positive chromosome-positive or t(4;11), and for patients first diagnosed in 2003–2007, high levels of minimal residual disease (>1% after induction or >0.1% after consolidation). Myeloablative allogeneic SCT in CR1 was recommended for these patients but not for patients with standard-risk ALL. The CR1 rate and 3-year overall survival after diagnosis for all patients treated with the ABCDV/VABA protocol were 86% and 29%, respectively, as reported previously.14
Relapse treatment
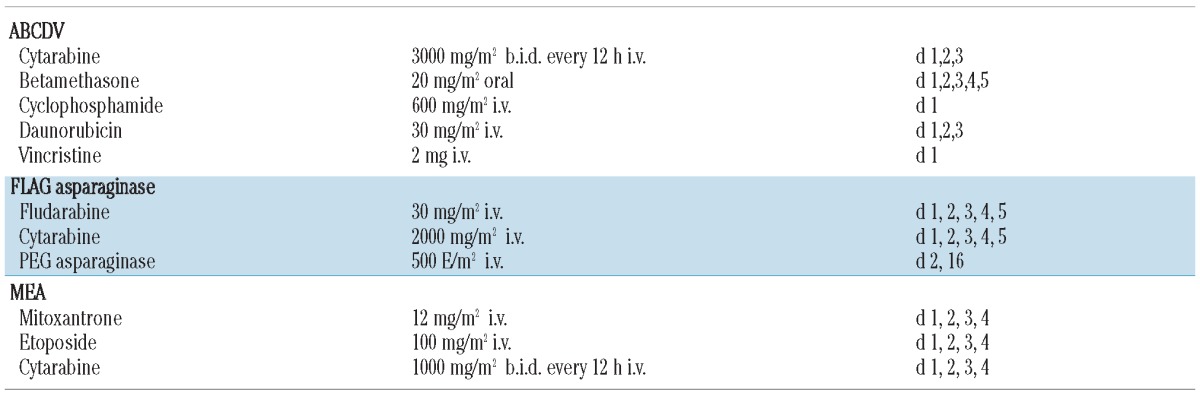
Between 2003 and 2007, the national guidelines recommended retreatment with ABCDV for late relapses (>2 years since initial diagnosis) and two treatment alternatives for early relapses: fludarabine, cytarabine, pegylated-asparaginase plus granulocyte colony-stimulating factor (FLAG-Asp) and mitoxantrone, etoposide, and cytarabine (MEA) (Table 1). For patients not undergoing transplantation in CR1 the aim was to perform myeloablative allogeneic SCT in CR2. The final decision on the choice of relapse treatment was left to the treating physicians.
Table 1.
The most commonly used salvage regimens, recommended in national guidelines 2003–2007.
Statistical methods
Overall survival was calculated from the time of first relapse to death or time of last follow-up. Distributions of overall survival were estimated by the Kaplan-Meier method and differences in overall suvival according to risk factors were analyzed by the log-rank test. In addition, univariate and multivariate Cox regression analyses were performed to evaluate the effects of relevant covariates on overall survival. Ninety-five percent confidence intervals (95% CI) for hazard ratios (HR) were obtained. Correlations between variables and achievement of CR2 were evaluated by logistic regression. This method was also used to estimate differences in the distribution of risk factors in two age groups (<35 and >35 years at diagnosis). Statistical analyses were performed with SPSS or StatView statistical packages.
Results
Patients’ characteristics
According to The Swedish Acute Leukemia Registry there were 76 adult patients aged <66 years with ALL relapse in the years between 2003 and 2007 in Sweden. A flow chart illustrating treatment in the whole cohort is presented in Figure 1. Five patients (7%) received palliative treatment: with cyclophosphamide (n=1), thioguanine/mercaptopurine (n=1), corticosteroids (n=1) or supportive care only (n=2). The median age in this group was 60 years (range, 30–63) and the median overall survival was 1 month (range, 0.5–14). These five patients were excluded from further analysis.
Figure 1.

Treatment overview regarding 76 patients with ALL relapse.
The characteristics of the 71 remaining patients treated with intensive chemotherapy and/or tyrosine kinase inhibitors are shown in Table 2. There was a slight male predominance (60%). The median age at first ALL diagnosis was 39 years (range, 15–65) for all patients and 36 years (range, 15–65) for the 57 patients not undergoing transplantation in CR1. The median age at relapse for all patients was 39 years (range, 19–65). B-precursor ALL was more common (82%) than T-ALL (18%). Data on cytogenetics were available for 67 patients (94%). Fourteen cases (20%) had Philadelphia chromosome-positive ALL, detected by the presence of t(9;22) and/or bcr-abl, and two cases (3%) had t(4;11). Twenty-seven patients had normal karyotypes (38%) and 24 had miscellaneous abnormalities (34%). A high WBC count (as defined previously) was present in 13 cases, all with B-precursor ALL.
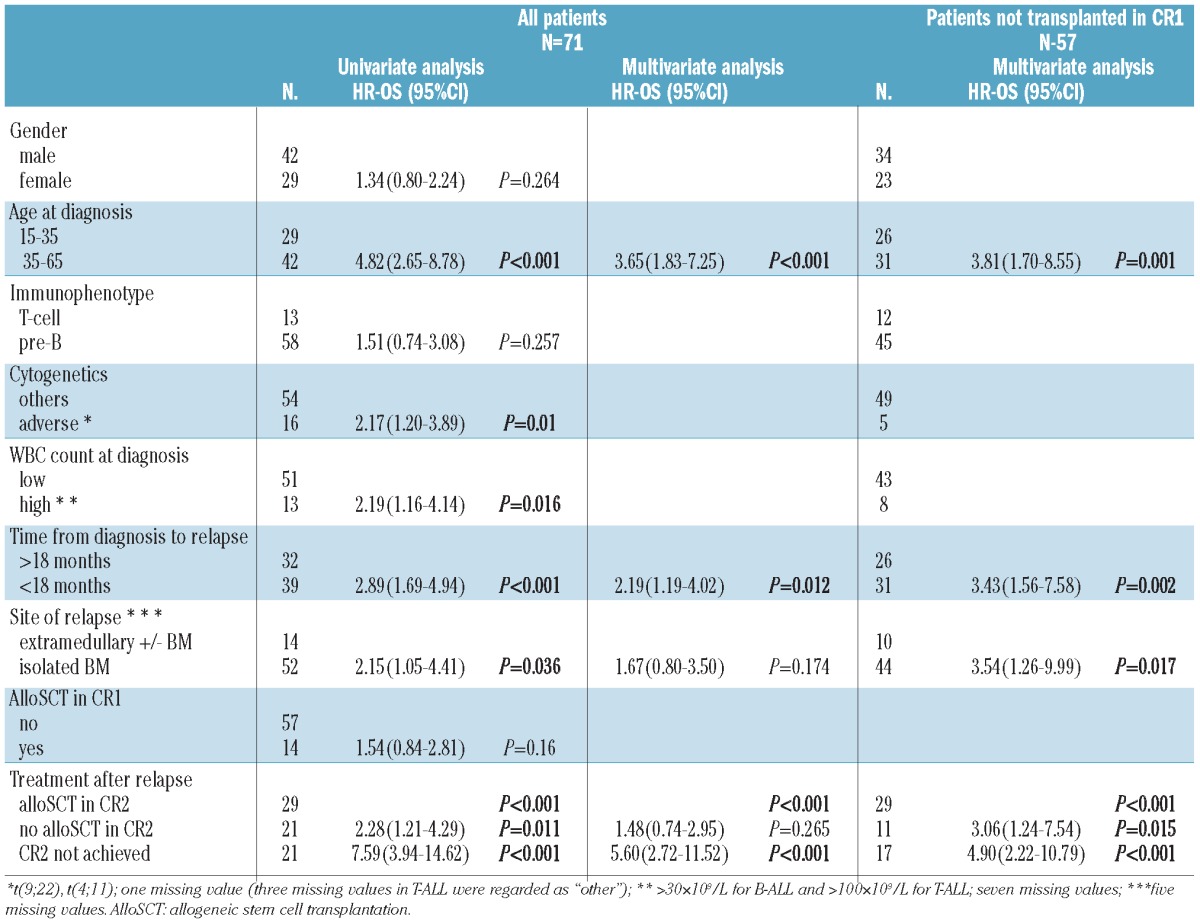
Table 2.
Patients’ characteristics and treatment factors analyzed by way of univariate and multivariate Cox regression for effects on overall survival.
The median time from diagnosis to relapse was 13 months (range, 2–82), with 55% relapsing within 18 months.
Isolated bone marrow relapse was most common (51/71, 72%). Extramedullary relapse at a single site was seen in five patients: central nervous system (n=3), testes (n=1) and extremities (n=1). Disease recurrence in both bone marrow and an extramedullary site occurred in nine patients: central nervous system (n=3), testes (n=1), mediastinum (n=1), uterus (n=1), lymph nodes (n=2) and base of the skull (n=1).
Overall, allogeneic SCT was performed in 14 patients and autologous SCT in three patients in CR1. This cohort of 17 patients included 13 patients with the pretreatment high-risk factors of high WBC count and/or adverse cytogenetics [t(4;11) or Philadelphia chromosome], two patients with late CR1, one with a complex karyotype and one patient unable to tolerate maintenance therapy.
Second complete remission rate after salvage therapy
The CR2 rate after the first salvage treatment was 52% (37/71). With additional treatment CR2 was achieved in 70% (50/71) of patients: 11 and two patients received two and three reinduction courses, respectively. Three patients died as a result of toxicity/infection after reinduction without reaching CR2. Gender, immunophenotype, cytogenetics, WBC count at diagnosis, site of relapse and allogeneic SCT performed during CR1 did not significantly influence either the CR2 rate after first salvage or the final CR2 rate. Final achievement of CR2 was negatively influenced by age >35 years at diagnosis (60% versus 86%) (P=0.012), and also by time to relapse <18 months (54% versus 91%) (P=0.001).
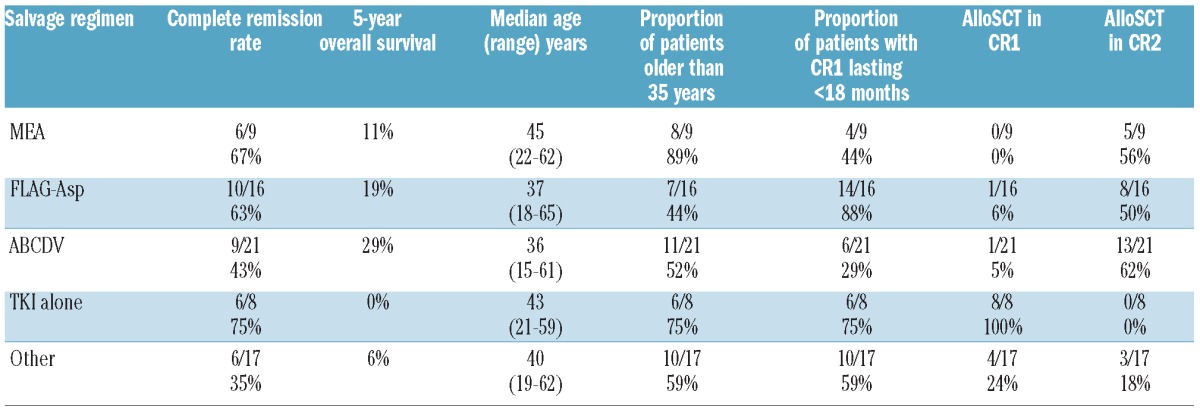
The outcomes of the applied salvage regimens and characteristics of the patients treated are presented in Table 3. Both recommended options for early relapsing patients, i.e. MEA and FLAG-Asp, resulted in CR2 in high proportions of patients (67% and 63%, respectively). Reinduction with ABCDV, which was recommended for late-relapsing patients, induced CR2 in 43% of cases after one course, suggesting poorer efficacy than for MEA and FLAG-Asp, although statistically not proven. Other therapy options used as first salvage treatment were: hyper-CVAD (n=2), hyper-CVAD in combination with a tyrosine kinase inhibitor (n=2), a tyrosine kinase inhibitor (n=8), FLAG-idarubicin (n=2), FLAG (n=2), MEA with nelarabine (n=1) or rituximab (n=1), high-dose cytarabine (n=1), combinations of cytarabine and anthracyclines (n=1) or cytarabine and methotrexate (n=1), a combination of radio- and chemotherapy (n=1), and a modified NHL-BFM 90 protocol16 (n=3). Subsequent treatments in refractory disease were heterogeneous and not reported for all patients. Those used as second-line therapy achieving CR2 were VABA14 (n=4), a tyrosine kinase inhibitor (n=1), FLAG-Asp (n=4), hyper-CVAD (n=1), and the NHL-BFM 90 protocol (n=1). Effective third-line salvage therapies were hyper-CVAD with gemtuzumab ozogamicin (n=1) and induction according to a pediatric protocol (NOPHO-92)17 (n=1).
Table 3.
Complete remission rates after the first reinduction course and patients’ characteristics according to the applied salvage regimens.
Overall survival after relapse
The median overall survival of the 71 patients receiving intensive chemotherapy was 9 months (range, 0.5–100). The overall survival rate at 1 year was 41% (95% CI: 29–52%), after 3 years it was 22% (95% CI: 13–32%), and the projected 5-year overall survival rate was 15% (95% CI: 7–24%). Eleven patients (15%), all below 35 years of age at diagnosis, are still alive at a median of 5.5 years (range, 4–8.2) after relapse. A majority of the 60 dead patients (n=43, 72%) died of leukemia. Other common causes of death were infection (n=8, 13%) and graft-versus-host disease (n=3, 5%).
In order to analyze the influence of CR2 and subsequent allogeneic SCT on overall survival the study population was divided into three groups. Kaplan-Meier survival curves for these groups are shown in Figure 2, with advantageous outcome for patients receiving allogeneic SCT in CR2 (Figure 2, curve A) compared to patients achieving CR2 but with no subsequent allogeneic SCT (Figure 2, curve B), and the worst outcome for patients not achieving CR2 (Figure 2, curve C). Three patients from group B died within 119 days of relapse (the median time until allogeneic SCT in CR2). Their causes of death were second relapse of ALL, aspergillosis and complications after a liver biopsy. The difference in overall survival between patients in groups A and B remained statistically significant even when these patients were excluded (data not shown).
Figure 2.
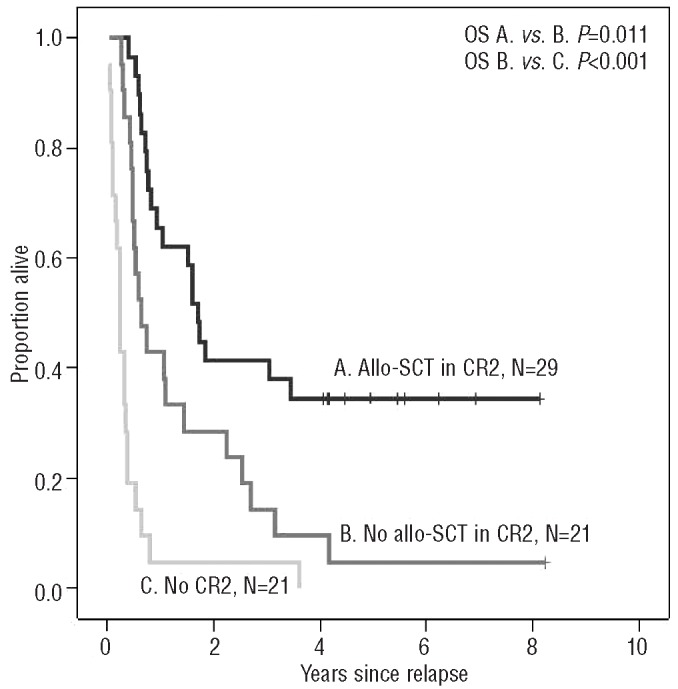
Effects of allogeneic SCT (allo-SCT) in CR2, and CR2 achievement on overall survival (OS).
Along with a failure to achieve CR2 and no allogeneic SCT in CR2, other negative prognostic factors with regards to overall survival in univariate analyses were age >35 years at diagnosis (P<0.001), time to relapse <18 months (P<0.001), adverse cytogenetics (P=0.007), high WBC count (P=0.016) and isolated bone marrow relapse (P=0.036) (Table 2).
In the multivariate model for overall survival the variables cytogenetics and WBC count at diagnosis had to be omitted, as no patients with high-risk features (high WBC count and/or adverse cytogenetics) underwent transplantation in CR2. Five of the 71 patients had missing information on relapse site and these patients were excluded from the multivariate analysis. Age >35 years at diagnosis (P<0.001), time to relapse <18 months (P=0.011) and lack of achievement of CR2 (P<0.001) had significant negative impacts on overall survival after relapse (Table 2).
The patients were divided into four subgroups with differing overall survival rates depending on age and time to relapse: <35 years with relapse after >18 months, <35 years with relapse in <18 months, >35 years with relapse after >18 months, and >35 years with relapse in <18 months (Figure 3). No patients older than 35 years were rescued compared with projected 5-year overall survival rates of 25% (95% CI: 0–50%) and 47% (95% CI: 23–71%) among young adults with relapse in <18 months and after >18 months, respectively.
Figure 3.
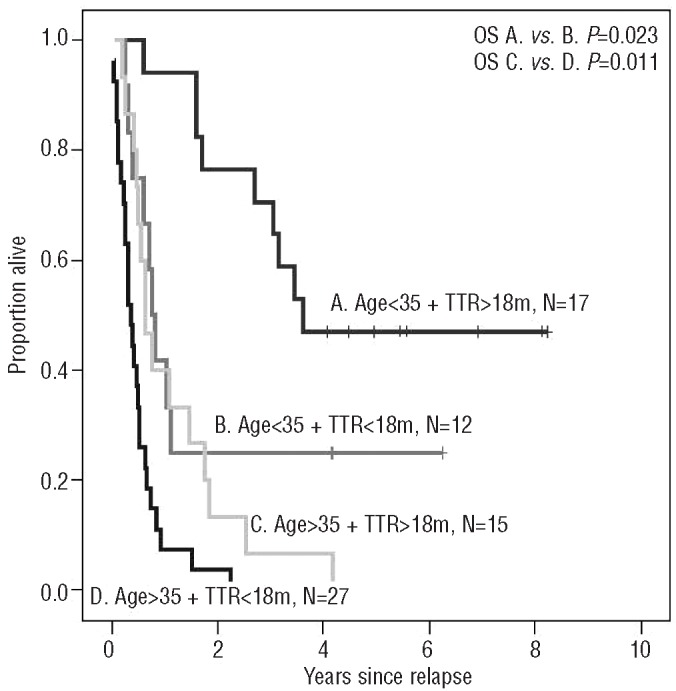
Overall survival (OS) according to age at diagnosis and time to relapse (TTR).
Patients >35 years old at diagnosis had more high-risk features compared with those <35 years old: adverse cytogenetics (36% versus 7%, P=0.004) and high WBC counts (32% versus 8%, P=0.017). Isolated bone marrow relapse (86.5% versus 69%, P=0.084) and time to relapse <18 months (64% versus 41%, P=0.056) were also slightly more common in older patients. Fewer patients >35 years old versus <35 years old proceeded to allogeneic SCT in CR2 (24% versus 65.5%, P<0.001).
Outcome in patients who relapsed after allogeneic stem cell transplantation in first complete remission
All patients who relapsed after allogeneic SCT in CR1 (n=14) died at a median of 7 months (range, 1–51) after relapse. As shown in Table 2, their overall survival was not significantly different from that of patients who relapsed and who had not undergone transplantation in CR1 (P=0.16) when analyzed overall. Ten patients carried the Philadephia chromosome and one had t(4;11). The median time between SCT and relapse was 10 months (range, 2–45). Having a transplant from an unrelated donor (7/14) was associated with a longer time to first relapse (P=0.042, log-rank test) and longer overall survival after first relapse (P=0.037, log-rank test) compared with having a transplant from a related donor (7/14). Donor lymphocyte infusions were given to 9/14 patients, in combination with tyrosine kinase inhibitors, chemotherapy or both. Donor lymphocyte infusions had no significant influence on overall survival (log-rank test). One relapsed patient underwent a second allogeneic transplant but died from an early second relapse.
Outcome in patients who did not receive allogeneic stem cell transplantation in first complete remission
The median overall survival of the 57 patients who did not undergo allogeneic SCT in CR1 was 9 months (range, 0.5–99), with 11 patients still alive belonging to this group. Forty (70%) achieved CR2 after the first (n=28), second (n=10) or third (n=2) salvage treatment and 29 (51%) proceeded subsequently to allogeneic SCT from an HLA identical related donor (n=13), a mismatched related donor (n=1), a 10/10 antigen matched unrelated donor (n=7), a mismatched unrelated donor (n=7) and unrelated cord blood (n=1). Myeloablative conditioning (mainly cyclophosphamide/total body irradiation) was used in 25 cases and reduced-intensity conditioning in four cases. The source of stem cells was peripheral blood (n=25), bone marrow (n=2), peripheral blood and bone marrow (n=1) and cord blood (n=1). The median time from relapse to transplantation was 119 days (range, 51–226). The remaining patients (n=23) received chemotherapy only (n=21) or autologous SCT (n=2). Autologous SCT was performed during active disease in one patient who died 31 months later (CR2 was reached after the SCT) and in one patient with isolated testis relapse who is alive after 8 years of follow-up. None of the patients who achieved CR2 but did not proceed to SCT became long-time survivors.
For the eight patients with pretreatment high-risk factors whose treatment did not include SCT in CR1, the outcome was dismal. Their median age was 52 years (range, 22–61) and the median time from diagnosis to relapse was 6 months (range, 2–12). In this cohort of patients all but one had a WBC count of >30×109/L, three had Philadelphia chromosome-positive leukemia, one had t(4;11), one had a complex karyotype and two had tetraploid leukemia; only one patient reached CR2 and their median overall survival was 3.9 months (range, 0.5–7.7).
A projected 5-year overall survival rate of 34% (95% CI: 17–52%) for patients who underwent allogeneic SCT in CR2 compares with 9% (95% CI: 0–26%) for patients who achieved CR2 but were treated without allogeneic SCT, and 0% for those without achievement of CR2. Cox multivariate regression concerning overall survival was performed. Other variables tested in this model were time to relapse, age, and site of relapse (isolated bone marrow versus extramedullary ± bone marrow), with the results shown in Table 2. A survival advantage for the allogeneic SCT group was found compared with both the group of patients not reaching CR2 (HR 4.90, P<0.001) and those reaching CR2 but not treated with allogeneic SCT (HR 3.06, P=0.015). Along with age >35 years at diagnosis and time to relapse <18 months, isolated bone marrow relapse also had a negative impact on overall survival compared with extramedullary ± bone marrow relapse (HR 3.54, P=0.017).
Within the cohort of 29 patients who underwent allogeneic SCT in CR2, all ten patients >35 years old at diagnosis were identified as a high-risk group, with all patients dying because of leukemia (5/10), infection (3/10) or graft-versus-host disease (2/10) within a median period of 5.5 months (range, 1–18) after transplantation. In comparison, among 19 patients treated with allogeneic SCT who were <35 years old at diagnosis, ten are still alive after a median of 5.5 years (range, 4.2–8.3). Among the patients <35 years at diagnosis, the projected 5-year overall survival rate in allogeneic SCT-treated patients is 53%. The only young patient surviving in the non-allogeneic SCT-treated group underwent autologous transplantation, as mentioned above.
Overall survival was not significantly influenced by type of donor, with projected 5-year overall survival rates of 43% (95% CI: 17–69%) versus 29% (95% CI: 5–52%) for unrelated and related donors, respectively.
Discussion
This study is unique as a population-based survey of adult patients (age <66 years) with relapsed ALL potentially eligible for allogeneic SCT, covering all relapsing patients reported to the Swedish Acute Leukemia Registry during the period from 2003 to 2007. Reinduction protocols used in cases of relapsed ALL lead to CR2 in 0–80% of patients.11 It is, however, extremely difficult to compare their efficacy, as no randomized or population-based studies are available and selection is often present in the populations of patients. Intensified chemotherapy at relapse can increase overall survival.18 Many protocols involving various combinations of anthracyclines, vincristine, steroids, cyclophosphamide, cytarabine and other cytostatics are available, illustrating the lack of uniform treatment guidelines for relapsed ALL.
Both recommended reinduction protocols for early relapsing patients, MEA and FLAG-Asp, were effective in achieving CR2 in our study, whereas ABCDV, which was used for late relapses, resulted in a somewhat lower CR2 rate. However, no significant differences in CR2 achievement among the applied protocols were observed. Final achievement of CR2 was more likely in younger patients and in cases of late relapse, as reported previously.10 One could speculate that the MEA and FLAG-Asp regimens might produce at least as good CR2 results if applied in cases of late relapse and thereby be more suitable choices for these patients also. If CR2 is not reached by means of front-line salvage it can be reached via second-line regimens, as we and other groups have shown.
Achieving CR2 is essential with regards to the outcome of allogeneic SCT, as patients undergoing transplantation during active relapse have little chance of long-term survival.11,19 Even though no patients became long-time survivors without SCT, achieving CR2 as such can improve survival time, as illustrated in our study. Patients who underwent transplantation in CR1 and who subsequently suffered relapse were beyond rescue, although it is noteworthy that CR2 was reached in a high proportion of Philadelphia chromosome-positive cases after administration of tyrosine kinase inhibitors (Table 3).
Age is an important prognostic factor in adult ALL and a high-risk disease pattern in ALL (adverse cytogenetics, high WBC count) in older patients is well known.8 Other factors often contributing to worse outcome in this population are poor performance status and chemotherapy-related complications. Probably a combination of the above-mentioned factors meant that none of the patients aged over 35 years old at diagnosis became long-term survivors in our study.
There are conflicting data regarding whether or not central nervous system disease, which is the most common extramedullary ALL manifestation, has an adverse effect on survival at diagnosis8 and/or relapse.10–12 In our limited number of patients we found that isolated bone marrow relapse was correlated with shorter overall survival time (at least in the SCT setting) compared with extramedullary disease alone or in combination with bone marrow relapse. This finding needs to be confirmed in other studies but it indicates that allogeneic SCT can be an effective treatment option in CR2 for patients with extramedullary relapse.
Scoring systems and risk-group stratification regarding outcome in cases of ALL relapse based on parameters such as age, duration of CR1, Philadelphia chromosome status, WBC count, blast count and lactate dehydrogenase level have been proposed.19,20 Our results confirm the previously reported, strong prognostic value of age and time to relapse.10–12 These factors, together with the effect of allogeneic SCT in CR2, seem to influence the possibility of long-term survival strongly. Since patients with high-risk factors had undergone SCT in CR1 or had been found not eligible or suffered from early relapses prohibiting SCT, a scoring system including pretreatment high-risk factors was not really possible.
Intensive chemotherapy followed by allogeneic SCT is regarded as the optimal treatment strategy for relapsed adult ALL, but usually only a minority of patients (17–30%) are considered eligible for such an approach.10–12 In comparison, the proportion of patients among the intensively treated subjects who underwent allogeneic SCT in CR2 in our study was as high as 41% (51% among those who did not undergo transplantation in CR1), with a high overall survival rate of 38%. Whereas 53% of post-relapse allogeneic SCT patients in the younger age group showed sustained survival, no positive long-term effect was seen among patients >35 years of age at the time of diagnosis. We interpret this apparent lack of success in “older” adults as being partly a result of our low numbers of patients, and also a result of the well-known efficacy and toxicity problems of allogeneic SCT in this age group, in which five of our ten transplanted patients died of infection/graft-versus-host disease. Likewise, very few older survivors have been reported in other relapse studies,11,12 but non-myeloablative SCT may be a possible approach in this age group.21 Conversely, for young, standard-risk patients, the results of allogeneic SCT after relapse seem good enough to indicate that withholding transplantation in CR1 may be advisable, especially in the era of more effective pediatric-based protocols. When relapses occur in such young patients, an urgent search for a donor should be performed, regardless of the availability of related donors.
It is noteworthy that autologous SCT after relapse can also be effective in selected cases, as exemplified by two of our patients, of whom one is showing sustained survival and the other (SCT without prior CR2 achievement) survived for 3.5 years. In a recently published study, six of 14 relapsed patients who received autologous SCT showed sustained survival.10 Long-term survival proportions after autologous SCT (15%) and unrelated donor allogeneic SCT (16%) performed as treatment after relapse were comparable in another large study, in which sibling allogeneic SCT was associated with the highest survival rate (23%) and chemotherapy alone with the lowest (4%).12
In summary, our results show encouraging long-term survival rates after intensive salvage chemotherapy followed by allogeneic SCT in CR2 for relapsed patients <35 years of age at diagnosis. The overall prognosis after ALL recurrence is, however, still unsatisfactory, with only a minority of adult patients being rescued. Simple risk-group stratification based on age and time to relapse aid in predicting outcome. MEA and FLAG-Asp seem effective as reinduction therapies, although our small numbers treated preclude solid conclusions. Efforts should continue to identify effective reinduction protocols to increase the number of patients eligible for allogeneic SCT in CR2. However, as regards relapses after allogeneic SCT performed in CR1, and patients >35 years of age at diagnosis, allogeneic SCT in CR2 is often either not achievable or is ineffective at improving survival. Prevention of relapse is essential to improve prognosis, especially in older patients, and new salvage treatments are urgently needed.
Footnotes
Authorship and Disclosures
The information provided by the authors about contributions from persons listed as authors and in acknowledgments is available with the full text of this paper at www.haematologica.org.
Financial and other disclosures provided by the authors using the ICMJE (www.icmje.org) Uniform Format for Disclosure of Competing Interests are also available at www.haematologica.org.
References
- 1.Huguet F, Leguay T, Raffoux E, Thomas X, Beldjord K, Delabesse E, et al. Pediatric-inspired therapy in adults with Philadelphia chromosome-negative acute lymphoblastic leukemia: the GRAALL-2003 study. J Clin Oncol. 2009;27(6):911–8. doi: 10.1200/JCO.2008.18.6916. [DOI] [PubMed] [Google Scholar]
- 2.Al-Khabori M, Minden MD, Yee KW, Gupta V, Schimmer AD, Schuh AC, et al. Improved survival using an intensive, pediatric-based chemotherapy regimen in adults with T-cell acute lymphoblastic leukemia. Leuk Lymphoma. 2010;51(1):61–5. doi: 10.3109/10428190903388376. [DOI] [PubMed] [Google Scholar]
- 3.Ottmann OG, Pfeifer H. Management of Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ ALL) Hematology Am Soc Hematol Educ Program. 2009:371–81. doi: 10.1182/asheducation-2009.1.371. [DOI] [PubMed] [Google Scholar]
- 4.Goldstone AH, Richards SM, Lazarus HM, Tallman MS, Buck G, Fielding AK, et al. In adults with standard-risk acute lymphoblastic leukemia, the greatest benefit is achieved from a matched sibling allogeneic transplantation in first complete remission, and an autologous transplantation is less effective than conventional consolidation/maintenance chemotherapy in all patients: final results of the International ALL Trial (MRC UKALL XII/ECOG E2993) Blood. 2008;111(4):1827–33. doi: 10.1182/blood-2007-10-116582. [DOI] [PubMed] [Google Scholar]
- 5.Bachanova V, Weisdorf D. Unrelated donor allogeneic transplantation for adult acute lymphoblastic leukemia: a review. Bone Marrow Transplant. 2008;41(5):455–64. doi: 10.1038/sj.bmt.1705889. [DOI] [PubMed] [Google Scholar]
- 6.Bartolozzi B, Bosi A, Orsi C. Allogeneic hematopoietic stem cell transplantation as part of postremission therapy improves survival for adult patients with high-risk acute lymphoblastic leukemia: a meta-analysis. Cancer. 2007;109(2):343. doi: 10.1002/cncr.22406. author reply 44. [DOI] [PubMed] [Google Scholar]
- 7.Rowe JM, Buck G, Burnett AK, Chopra R, Wiernik PH, Richards SM, et al. Induction therapy for adults with acute lymphoblastic leukemia: results of more than 1500 patients from the international ALL trial: MRC UKALL XII/ECOG E2993. Blood. 2005;106(12):3760–7. doi: 10.1182/blood-2005-04-1623. [DOI] [PubMed] [Google Scholar]
- 8.Faderl S, O’Brien S, Pui CH, Stock W, Wetzler M, Hoelzer D, et al. Adult acute lymphoblastic leukemia: concepts and strategies. Cancer. 2010;116(5):1165–76. doi: 10.1002/cncr.24862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Goldstone AH, Rowe JM. Transplantation in adult ALL. Hematology Am Soc Hematol Educ Program. 2009:593–601. doi: 10.1182/asheducation-2009.1.593. [DOI] [PubMed] [Google Scholar]
- 10.Oriol A, Vives S, Hernandez-Rivas JM, Tormo M, Heras I, Rivas C, et al. Outcome after relapse of acute lymphoblastic leukemia in adult patients included in four consecutive risk-adapted trials by the PETHEMA Study Group. Haematologica. 2010;95(4):589–96. doi: 10.3324/haematol.2009.014274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tavernier E, Boiron JM, Huguet F, Bradstock K, Vey N, Kovacsovics T, et al. Outcome of treatment after first relapse in adults with acute lymphoblastic leukemia initially treated by the LALA-94 trial. Leukemia. 2007;21(9):1907–14. doi: 10.1038/sj.leu.2404824. [DOI] [PubMed] [Google Scholar]
- 12.Fielding AK, Richards SM, Chopra R, Lazarus HM, Litzow MR, Buck G, et al. Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood. 2007;109(3):944–50. doi: 10.1182/blood-2006-05-018192. [DOI] [PubMed] [Google Scholar]
- 13.Juliusson G, Karlsson K, Hallbook H. Population-based analyses in adult acute lymphoblastic leukemia. Blood. 2010;116(6):1011. doi: 10.1182/blood-2010-03-272724. author reply 12. [DOI] [PubMed] [Google Scholar]
- 14.Hallbook H, Simonsson B, Ahlgren T, Bjorkholm M, Carneskog J, Grimfors G, et al. High-dose cytarabine in upfront therapy for adult patients with acute lymphoblastic leukaemia. Br J Haematol. 2002;118(3):748–54. doi: 10.1046/j.1365-2141.2002.03685.x. [DOI] [PubMed] [Google Scholar]
- 15.Kantarjian HM, O’Brien S, Smith TL, Cortes J, Giles FJ, Beran M, et al. Results of treatment with hyper-CVAD, a dose-intensive regimen, in adult acute lymphocytic leukemia. J Clin Oncol. 2000;18(3):547–61. doi: 10.1200/JCO.2000.18.3.547. [DOI] [PubMed] [Google Scholar]
- 16.Hoelzer D, Ludwig WD, Thiel E, Gassmann W, Loffler H, Fonatsch C, et al. Improved outcome in adult B-cell acute lymphoblastic leukemia. Blood. 1996;87(2):495–508. [PubMed] [Google Scholar]
- 17.Hallböök H, Gustafsson G, Smedmyr B, Söderhäll S, Heyman M Swedish Adult Acute Lymphocytic Leukemia Group; Swedish Childhood Leukemia Group. Treatment outcome in young adults and children >10 years of age with acute lymphoblastic leukemia in Sweden: a comparison between a pediatric protocol and an adult protocol. Cancer. 2006;107(7):1551–61. doi: 10.1002/cncr.22189. [DOI] [PubMed] [Google Scholar]
- 18.Camera A, Annino L, Chiurazzi F, Fazi P, Cascavilla N, Fabbiano F, et al. GIMEMA ALL - Rescue 97: a salvage strategy for primary refractory or relapsed adult acute lymphoblastic leukemia. Haematologica. 2004;89(2):145–53. [PubMed] [Google Scholar]
- 19.Advani A, Jin T, Bolwell B, Copelan E, Sekeres M, Sobecks R, et al. A prognostic scoring system for adult patients less than 60 years of age with acute lymphoblastic leukemia in first relapse. Leuk Lymphoma. 2009;50(7):1126–31. doi: 10.1080/10428190902962838. [DOI] [PubMed] [Google Scholar]
- 20.Duval M, Klein JP, He W, Cahn JY, Cairo M, Camitta BM, et al. Hematopoietic stem-cell transplantation for acute leukemia in relapse or primary induction failure. J Clin Oncol. 2010;28(23):3730–8. doi: 10.1200/JCO.2010.28.8852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ribera JM. Allogeneic stem cell transplantation for adult acute lymphoblastic leukemia: when and how. Haematologica. 2011;96(8):1083–6. doi: 10.3324/haematol.2011.048348. [DOI] [PMC free article] [PubMed] [Google Scholar]