

Abstract
Manipulation of a pacemaker with consequent malfunction of the device has been called Twiddler's syndrome. Use of active-fixation leads and subpectoral pacemaker pockets has been considered to help in avoiding this problem. We describe a child in whom twiddling was not prevented despite implantation of a lumenless atrial lead and insertion of the pacemaker generator in a subpectoral pocket.
Keywords: Active fixation, children, pacemaker failure, pacemaker, Twiddler's syndrome
INTRODUCTION
Permanent pacing is an efficient treatment to improve symptoms and clinical outcome in children with congenital heart block or sick sinus syndrome. The lead system is the most vulnerable part of the pacing system, particularly in growing children. Possible mechanisms of lead failure include lead fracture, dislodgement, and insulation break. We describe a child with a rare cause of pacemaker malfunction.
CASE REPORT
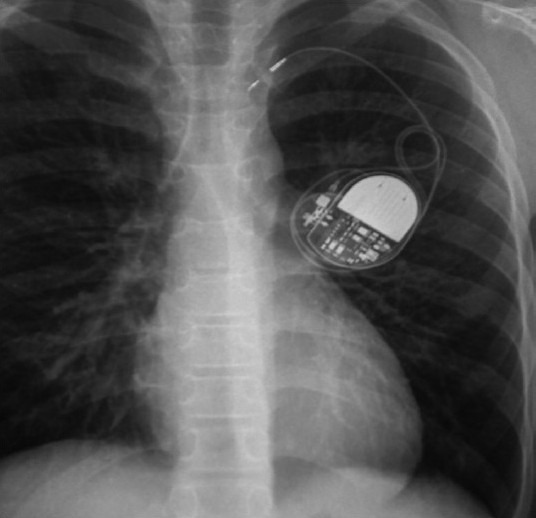
A 10-year-old boy was admitted with uncontrollable spontaneous muscular movements and twisting of his left shoulder and arm. Two weeks earlier he had undergone implantation of a single-chamber transvenous pacing system for symptomatic sick sinus syndrome. A bipolar, active-fixation, lumenless 4.1-F endocardial lead (Medtronic Model 3830) had been implanted in his right atrium. The pacemaker generator had been inserted in a left-sided subpectoral pocket [Figure 1a].
Figure 1a.
A chest radiograph demonstrating the implanted pacemaker system
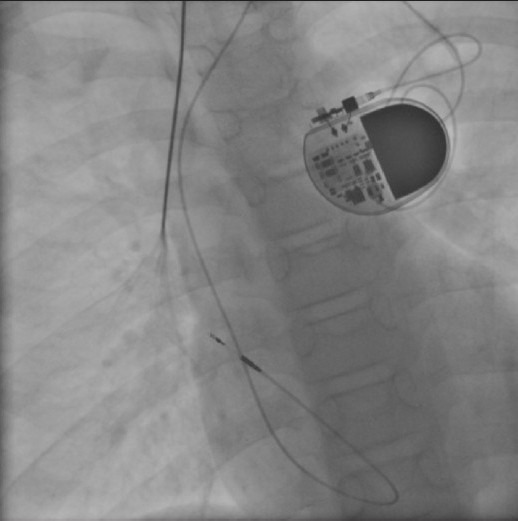
Examination of his chest and arm showed rhythmical twitching of his left pectoral muscles and arm. Interrogation of his pacing system confirmed atrial non-capture. A chest x-ray demonstrated that the lead tip had moved far away from the original insertion site. Moreover, loops of pacing lead were seen coiled around the generator [Figure 1b]. These findings suggested that repeated manipulation and twisting of the pacemaker device, deliberately or unintentionally, had pulled the lead out of the right atrium and wrapped it concentrically around the generator. The boy denied any deliberate manipulation of the pacemaker. At the time of lead revision, the entire lead was found to be extravascular. A new, conventional, active-fixation lead was implanted (Medtronic). At 12 months' follow-up there was no recurrence of lead dislodgement.
Figure 1b.
Twiddler's syndrome. Repeated twisting of the pacemaker generator resulted in retraction of the atrial lead to the subclavian vein
CASE DISCUSSION
Manipulation of a pacemaker or implantable cardioverter defibrillator with consequent malfunction of the device has been known as twiddler's syndrome.[1] The pacemaker is most often rotated on its long axis within the pocket.[2] The lead dislodges, resulting in pacemaker malfunction, non-capture, and unintended stimulation of nearby nerves. The left brachial plexus may be stimulated by the dislodged lead, as in this case, causing rhythmical twitching of the left pectoral muscles and arm. Other signs and symptoms include abdominal pulsations, diaphragmatic pacing, presyncope, and syncope.[1–4]
Although this self-inflicted problem has been recognized in adults for many years, it is very rare in children. Only four other pediatric cases of twiddler's syndrome have been described.[2–4] Use of conventional active-fixation leads and subpectoral pacemaker pockets have been considered to help avoid this problem. However, in our patient, twiddling was not prevented despite these measures. The thin diameter of the Medtronic Model 3830 lumenless lead may not allow secure fixation of the lead at the entry site into the blood vessel. Therefore, a conventional active-fixation lead was implanted during revision of the pacing system. This new lead was securely anchored using nonabsorbable sutures at the entry site into the blood vessel. Important management options for preventing or treating twiddling may include positioning the pacemaker in an abdominal pocket, creating a smaller pacemaker pocket, suturing the device to the fascia, and individualized patient/parent education.[1–5]
Physicians caring for children with pacemakers should be aware of this problem when confronted with acute pacemaker malfunction.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Veltri EP, Mower MM, Reid PR. Twiddler's syndrome: a new twist. Pacing Clin Electrophysiol. 1984;7:1004–9. doi: 10.1111/j.1540-8159.1984.tb05652.x. [DOI] [PubMed] [Google Scholar]
- 2.Abrams S, Peart I. Twiddler's syndrome in children: an unusual cause of pacemaker failure. Br Heart J. 1995;73:190–2. doi: 10.1136/hrt.73.2.190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ellis AR, Reed JH, Fairbrother D. A tangled affair: Pacemaker malfunction and syncope in a child due to Twiddler's syndrome. Cardiol Young. 2007;17:220–2. doi: 10.1017/S1047951107000157. [DOI] [PubMed] [Google Scholar]
- 4.Berul CI, Hill SL, Estes NA., 3rd A teenager with pacemaker twiddler syndrome. J Pediatr. 1997;131:496–97. [PubMed] [Google Scholar]
- 5.Riezebos RK, de Ruiter GS. Twiddler's syndrome: An unusual cause of pacemaker dysfunction. Am J Geriatr Cardiol. 2008;17:53–4. doi: 10.1111/j.1076-7460.2007.05830.x. [DOI] [PubMed] [Google Scholar]