

Abstract
Literature comparing national ambient air quality standards (AAQSs) globally is scattered and sparse. Twenty-four hour AAQSs for particulate matter <10 μm in aerodynamic diameter (PM10) and sulfur dioxide (SO2) in 96 countries were identified through literature review, an international survey, and querying an international legal database. Eighty three percent, of the 96 countries with information on the presence or absence of AAQSs, have 24-h AAQSs for either PM10 or SO2. Slightly more countries have 24-h AAQSs for SO2 (76 countries) than PM10 (69 countries). The average 24-h AAQSs for PM10 and SO2 are 95 μg/m3 (95% confidence interval [CI], 82–108 μg/m3, n = 68) and 182 μg/m3 (95% CI, 158–205 μg/m3, n = 73). The population-weighted average AAQS for PM10 is 98 and 155 μg/m3 for SO2. The average AAQS for both PM10 and SO2 are substantially higher than the recommended World Health Organization Air Quality Guideline (WHO AQG) value. Several countries have promulgated AAQSs at the WHO AQG value for PM10, but none for SO2. Further examination in selected countries found that air quality monitoring data, existing AAQSs in other countries, environmental epidemiology studies, and the WHO AQGs are considered the most often in establishing or revising AAQSs.
Electronic supplementary material
The online version of this article (doi:10.1007/s11869-010-0131-2) contains supplementary material, which is available to authorized users.
Keywords: World Health Organization, Air Quality Guidelines, Air pollutants, Particulate matter, Sulfur dioxide
Introduction
Considerable resources are devoted to developing and implementing ambient air quality standards (AAQSs), but few systematic investigations appear to have been conducted to review AAQSs globally or explore the evidence used to establish and revise AAQSs. Although there are publications that list the AAQSs in one region (Maggioria and Silva 2006; Schwela et al. 2006), in urban areas (Archer and Davidson 1996; Schwela et al. 2006) or in selected countries as part of a larger analysis of air quality management (International Union of Air Pollution Prevention Associations 1991; Elsom and Longhurst 2004), a comprehensive global analysis of AAQSs does not seem to have been conducted.
This paper reviews the 24-h national AAQSs for particulate matter less than ten micrometers in aerodynamic diameter (PM10) and sulfur dioxide (SO2) globally.1 In addition to tabulating AAQSs, we attempt to determine the type of scientific evidence considered by an agency when establishing or revising AAQSs, specifically the use of the World Health Organization Air Quality Guidelines.
In 2006, the World Health Organization (WHO) published global air quality guidelines (AQGs) for PM10, SO2, NO2 and ozone (WHO 2006; Krzyzanowski and Cohen 2008). Thus far, there have been four versions (WHO 1987, 2000a, b, 2006) of the World Health Organization Air Quality Guidelines (WHO AQGs). The guidelines which provide an international reference that countries, particularly those without the resources to conduct their own assessment, can use to develop AAQSs.
The 2006 WHO AQGs are composed of a single guideline value and interim targets (ITs). The interim targets provide a stepwise approach to achieving the air quality guideline value. The guideline values can be used by developed countries, with the capacity to implement a strict AAQS, while developing countries, with higher levels of air pollution, could select an interim target level achievable based on their own air quality management infrastructure, and progress towards the AQG value at their own pace.
Methods
This research focuses on both national AAQSs, which are legally binding, and voluntary ambient air quality guidelines (AAQGs). Although AAQSs and AAQGs are substantially different, when examining how they are implemented and enforced, these topics are not the focus of this review. As a result, both AAQSs and AAQGs are referred to as AAQSs unless explicitly stated otherwise. When available the type of AAQS, i.e., guideline, standard or directive, is indicated in the supplemental materials.
Literature review
The review was limited to countries recognized by the United Nations (UN). The AAQSs (standards) for 75 countries were acquired, from internet searches, legal databases, and secondary sources; of which 57 were from internet and legal database search engines. Web-based searches were limited to information from government websites (e.g., The Ministry of Environment), peer-reviewed journals, or reports produced by a governmental, international or regional organization (e.g., the European Union or Food and Agriculture Organization). AAQS in 18 additional countries were acquired from secondary sources (Maggioria and Lopez-Silva 2006; Schwela et al. 2006).
Survey
Information on and the evidence used to establish AAQSs in 24 countries were gathered from respondents to surveys sent to the Ministry of Environment in 153 countries through the postal service and email in September and October 2007, and May 2008. The contact information of each agency was acquired from the Ministry of Environment or equivalent website for each country, the Clean Air Initiative—Asia Center, The National Association of Clean Air Agencies, the United Nations Environmental Programme, and the Global Environmental Facility website. A pre-addressed, postage-paid international business reply envelope was included with each paper survey. The surveys were sent to self-identified developing countries, defined here as members of the G77 (group of 77) or G24 (group of 24) within the UN, and European countries that were not members of the European Union (EU) in 2007. Although Iraq and Afghanistan fulfilled the inclusion criteria; surveys were not sent to either.
Each survey was sent with a cover letter requesting that the survey be completed by a representative who was responsible for drafting or revising their national ambient air quality standards (see supplemental materials for a copy of the survey). The exact role of the survey respondent in the AAQS revision process was not confirmed.
The 31 question survey covered three broad topics: background information on AAQSs; awareness of the WHO AQGs and their role in determining AAQSs; and the standard setting process, specifically the evidence-base used to establish or revise AAQSs. In some circumstances, agencies were asked to answer questions based on information projected into the future. For example, if an agency did not have AAQSs for PM, but they were in the process or had plans to establish them, then they were asked to answer a question such as “Who are the participants involved in setting the AAQSs?” based on the type of participants that they expected to be involved in future standard setting.
Results
AAQS
Information regarding the presence or absence of national daily AAQSs for PM10 and SO2 was found for 96 out of 192 UN member countries (50%). These countries contain 5.6 billion people, or 84% of the world population. Eighty (83%) of the 96, have a 24-h AAQS for either PM10 or SO2. Slightly more countries have a 24-h AAQS for SO2 (n = 76; 79%) than for PM10 (n = 69; 72%).
The average 24-h AAQS for PM10 and SO2 is 95 μg/m3 (95% confidence interval [CI], 82–108 μg/m3, n = 68) and 182 μg/m3 (95% CI, 158–205 μg/m3, n = 73). The population-weighted average AAQS for PM10 is 98 and 155 μg/m3 for SO2, respectively. The average 24-h AAQS was established or last revised for PM10 in 2004 (95% CI 2003–2005, n = 65) and SO2 in 2004 (95% CI 2002–2005, n = 64).
Figures 1 and 2 present the range of AAQSs found in each country. A list of the AAQSs used to create Figs. 1 and 2 is provided in the Online Supplement. If a country has an AAQS, but the exact value is unknown, it was included in the >IT-1 category in both Figures.
Fig. 1.
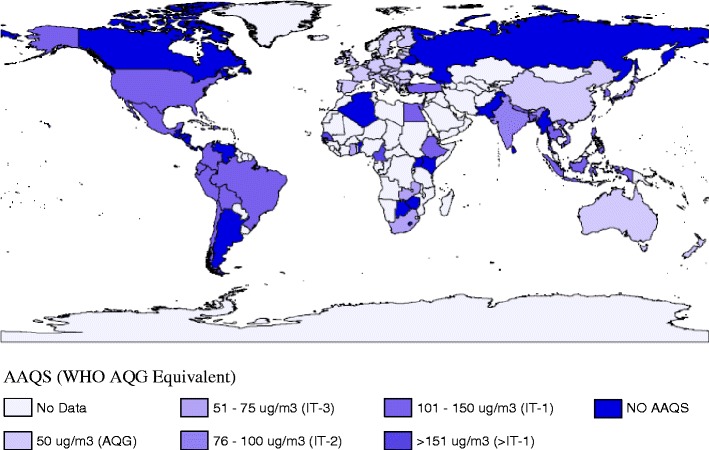
Map of national 24-h AAQS for PM10 AAQS (WHO AQG equivalent)
Fig. 2.
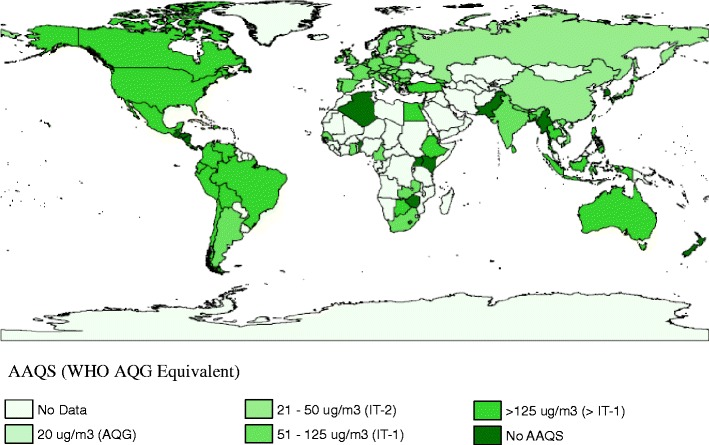
Map of national 24-h AAQS for SO2 AAQS (WHO AQG equivlent)
Association between AAQS stringency and selected demographics
A statistical analysis (using STATA software) of the stringency of each AAQS comparing selected demographic variables (population, urban population, gross domestic product per capita, energy use per capita, health expenditure per capita, average annual exposure to PM10, and government expenditure; see Table 1 in the supplemental materials for details) yielded the results presented in Table 1 for PM10 AAQSs. The only variables with significant associations (p < 0.05) to SO2 AAQSs were government expenditure (β = −7.52, 95% confidence internal −12.02 to −3.02, R 2 = 0.15) and energy use per capita (β = −25.68, 95% confidence interval −51.18 to −0.17, R 2 = 0.06).
Table 1.
Individual association between various demographics and PM10 AAQS
| Demographica | β | Confidence interval | R 2 |
|---|---|---|---|
| Energy use per capita (kg of oil equivalent, 2007) | −35.61** | −46.47 to −24.76 | 0.40 |
| Government expenditure (% of GDP, 2008) | −5.93** | −7.88 to −3.97 | 0.39 |
| Health expenditure per capita ($US, 2007) | −16.86** | −23.19 to −10.53 | 0.30 |
| PM10 (country level, ug/m,3 2006) | 44.55** | 25.44 to 63.66 | 0.25 |
| Population (2008) | 7.68* | 0.43 to 14.94 | 0.06 |
aThe natural logarithm of the following variables was used in order to adjust for skewed distributions—health expenditure per capita, energy use per capita, population and average annual exposure to PM10.
*p < 0.05, **p < 0.01
Participants involved in the AAQS process
The results presented in the following sections are based entirely on the survey discussed above. The geographical distribution and selected demographics of the survey respondents and non-respondents are summarized in the web supplement. The type of participants involved in the process of establishing or revising AAQSs were government or parliament scientists, followed by consultants, academic scientists, and government or parliament officials (see Table 2).
Table 2.
The type of players involved in setting or revising the AAQSs
| Type of participant | Percent countries where players involved (n = 18) |
|---|---|
| Government parliament officials | 100 |
| Consultants | 89 |
| Academic scientists | 89 |
| Government parliament scientists | 72 |
| NGOs | 67 |
| Lawyers | 50 |
| Businesses | 50 |
| Economists | 44 |
| CBOs | 44 |
| Development organizations | 17 |
| Government institutions | 6 |
NGO non-governmental organization, CBO community based organization
Evidence used to determine AAQSs
Air quality monitoring data, followed by environmental epidemiology studies, was used the most often to establish or revise AAQSs. Most agencies require the epidemiology studies used to set their AAQSs to be conducted in their own country (78%, n = 18) and peer-reviewed (75%, n = 16).
As shown in Table 3, most of the agencies also base their AAQSs on secondary evaluations of scientific evidence such as the AAQS in another country (71%, n = 21—see Table 4) or the WHO AQGs (79%, n = 19).
Table 3.
The type of evidence used to set or revise AAQS (n = 17)
| Type of study or secondary evaluation | Number of countries | |
|---|---|---|
| Primary data | Air quality monitoring data | 17 |
| Environmental epidemiology | 12 | |
| Occupational epidemiology | 5 | |
| Controlled human exposure studies | 3 | |
| Toxicology studies | 3 | |
| Secondary assessments | AAQSs from other Countries | 14 |
| WHO AQGs | 12 | |
| NGO reports | 5 | |
| IARCa designation | 3 |
aThe International Agency for Research on Cancer (IARC) is a separate agency of the WHO that evaluates the carcinogenicity of a substance
Table 4.
Countries that based their AAQS on the AAQSs of another country or region (n = 14)
| Existing standard | Agencies that used the existing standard to determine their own AAQS |
|---|---|
| US NAAQS | Brunei Darussalam, Chile, Mexico, Egypt, Philippines, Thailand |
| EU directives | Republic of Serbia, Chile, Croatia |
| CARB standards | Switzerland, Thailand |
| Russia Federation | Georgia, Armenia |
| South Africa | Lesotho |
| Singapore | Brunei Darussalam |
| Senegal | Cameroon |
| Nigeria | Cameroon |
| Egypt | Cameroon |
| Asian countries and East Asian regions | Philippines |
| India | Nepal |
US NAAQS United States National Ambient Air Quality Standards, EU European Union, CARB California Air Resources Board
Large fractions of agencies require a risk assessment (61%, n = 18) and an economic analysis (47%, n = 17) to be conducted before setting an AAQS.
WHO AQGs
Prior to reading the questionnaire used in this research, almost all of the respondents (91%, n = 23) were aware of at least one version of the WHO air quality guidelines. Awareness was slightly higher for the global AQGs (81%, n = 21) than the European AQGs (79%, n = 19). We found the Global or European AQGs have played a major role in the determination of AAQSs for PM or SO2 in the majority of the respondent countries with AAQSs (79%, n = 15). Most of the respondents (91%) also indicated that they now plan to use the WHO AQGs (2005) to revise or establish at least one of their AAQSs for either PM10, PM2.5, SO2, NO2 (nitrogen dioxide), or ozone (n = 22). In addition, 17% of the countries that utilized one of the versions of the WHO AQGs referenced them in a legal act.
Discussion
Information regarding the presence or absence of 24-h AAQSs for PM10 and SO2 was ascertained for 96 countries, which represent 84% of the global population. Most countries (83%) had AAQSs for PM10 or SO2 at the time of this research.
There are at least two numeric values for each AAQS that account for the majority of the AAQSs globally. AAQSs set at 50 and 150 μg/m3 comprise 82% (n = 68) of the PM10 AAQS. These coincide with the WHO AQG value (50 μg/m3) and the US PM10 NAAQS (150 μg/m3), which has not changed since 1997 (US EPA 2008). Standards set at 125 and 365 μg/m3 represent 64% (n = 73) of the AAQSs for SO2—equivalent to the first WHO interim target (125 μg/m3) for SO2 and the US SO2 NAAQS (365 μg/m3). This suggests that the WHO AQGs and the US NAAQS have influenced the selection of AAQSs in numerous countries.
Comparison to the WHO AQGs
Tables 5 and 6 provide a summary on the number of countries that have AAQGs that have reached each WHO IT for PM10 and SO2. Most of the global population lives in a country that has not implemented an AAQS that meets the WHO AQG target for PM10 (72%) or SO2 (100%). The average 24-h PM10 AAQS (95 μg/m3) is slightly lower then WHO IT-2 (100 μg/m3), out of three possible ITs, and almost twice the recommended WHO AQG (50 μg/m3). The mean 24-h SO2 AAQS (182 μg/m3) is well above WHO IT-1 (125 μg/m3), out of two possible ITs, and more than nine times the WHO AQG (20 μg/m3) (WHO 2006). The population-weighted average AAQS for both PM10 and SO2 is slightly different than the unadjusted averages, but within the same WHO IT range. The global average PM10 AAQS is much closer to the AQG value than the average SO2 AAQS. This is because the European Union, which consisted of 27 countries at the time of this research, adopted the AQG value for PM10, but the first interim target level (IT-1) for SO2.
Table 5.
Summary of PM10 AAQS and WHO targets (WHO, 2006)
| WHO AQG equivalent | PM10 (ug/m3) | Number of countries with AAQS in rangea | Million people covered (2008) | Percent of global population (2008) |
|---|---|---|---|---|
| AQG | 50 | 34 | 1870 | 28 |
| IT-3 | 51–75 | 4 | 86 | 1 |
| IT-2 | 76–100 | 3 | 1270 | 19 |
| IT-1 | 101–150 | 25 | 1700 | 25 |
| >IT-1 | >151 | 2 | 31 | <1 |
| No AAQS | 27 | 661 | 10 | |
| No data | 95 | 1040 | 16 |
aPlease note that this table excludes countries with AAQS, whose values are unknown (n = 1)
Table 6.
Summary of SO2 AAQS and WHO targets
| WHO AQG equivalent | SO2 (ug/m3) | Number of countries with AAQS in rangea | Million people covered (2008) | Percent of global population (2008) |
|---|---|---|---|---|
| AQG | 20 | 0 | 0 | 0 |
| IT-2 | 21–50 | 3 | 1470 | 22 |
| IT-1 | 51–125 | 42 | 2050 | 31 |
| >IT-1 | >125 | 28 | 1640 | 24 |
| No AAQS | 18 | 379 | 6 | |
| No data | 96 | 1090 | 16 |
aPlease note that this table excludes countries with AAQS, whose values are unknown (n = 3)
Association between AAQS stringency and selected demographics
As shown in Table 1, the stringency of AAQSs for PM10 is moderately associated with a number of national demographic indicators. Energy use, health/government expenditure, and country level PM10 concentration had the strongest association to PM10 AAQS stringency. Combining energy use and PM10 concentration into one model yielded slightly better results (R 2 = 0.46). Although, the low R 2 for each indicator signifies that the variability in each country’s AAQS is largely attributed to other factors. These findings are line with the survey results, which identified air quality monitoring data, AAQS in other countries, environmental epidemiology studies, and the WHO AQGs as the primary determinants of a countries AAQS. However, since air quality monitoring data were a main determinant in the survey results one might expect country level PM10 to have a stronger association than observed. Government expenditure was associated to AAQS stringency for both pollutants.
The relationship between disability adjusted life years (DALYs) due to urban air pollution and AAQS stringency was not significant. However, the analysis was limited because data on DALYs are aggregated by region.
Evidence used to establish and revise AAQSs
The participants responsible for establishing or revising the AAQSs for each country encompassed a wide variety of professionals ranging from academic scientists to members of community based organizations. As expected, government or parliament officials participated in setting or revising the AAQSs in all of the respondent countries with a higher percentage relying on government or parliament officials (100%) than government scientists (72%). There was also an extremely high participation of consultants (89%), which was equal to that of non-government academic scientists. Approximately half of the participants were business representative (50%) or economist (44%). The extremely diverse nature of the participants suggests that science was not the only factor considered when determining an AAQS.
Air quality monitoring data (e.g., baseline air quality) were considered the most often when setting and revising AAQSs; followed by AAQSs in other countries, environmental epidemiology studies, and the WHO AQGs. This suggests that secondary assessments of the risk of air pollution are just a relevant as peer-reviewed literature. Most of the respondents (77%) indicated they only use epidemiology studies that have been conducted in their own country and require the epidemiology studies used for standard setting to be peer-reviewed (75%). This should be considered when funding projects in developing countries. The high weight given to monitoring data could signify the importance of ensuring AAQSs are feasible. Although, less than half of the respondents require an economic analysis to be conducted before an AAQS is set.
Toxicology studies were not considered nearly as much as epidemiology studies, they were only utilized by one fifth of the respondents and their importance rating was equal to NGO reports.
The US NAAQS, EU Directives, and the CARB air quality standards were utilized by other countries to set AAQSs regardless of the geographical region that the country is located in. It was common for an agency to base their standards on the AAQS of another country in their geographical region. However, the US NAAQS, EU Directives, and the CARB air quality standards were utilized by other countries to set AAQSs regardless of the geographical region that the country is located in.
The WHO AQGs
Almost all (91%, n = 23) of the respondents were aware that the WHO publishes air quality guidelines that are globally applicable or for Europe. Most (79%, n = 19) of the respondents used one of the four versions of the air quality guidelines to determine their AAQSs, and significantly more (91%, n = 22) of the respondents plan on using the most recent publication Air Quality Guidelines: Global Update 2005 to set or revise their AAQSs. One of the two countries that did not plan to use the WHO AQGs currently has no AAQSs, and has no plans to establish any.
Most of the agencies that used one of the WHO AQGs documents to set or revise an AAQS evaluated the evidence in the document, compared it to their local conditions, and then decided on a standard. In the case of the PM standard, the more recent the WHO publication the more likely a country was to modify the WHO AQG for local conditions. This finding suggests it would be useful for the WHO to develop a method to aid agencies in evaluating how the WHO AQGs compare to country-specific characteristics in their next edition.
Limiting factors
There was a disproportionate lack of information about African, Middle Eastern, and Central European countries. Possible explanations for this could be a lack of actual AAQSs, a deficit in published information regarding AAQSs or language barriers—Arabic is difficult to translate with free online translation services. In addition, of course, the survey was printed in English.
A visual analysis of Figs. 1 and 2 indicates that there might be a spatial correlation in the AAQSs in particular regions. After more data are gathered, particularly in Africa and the Middle East, a spatial analysis might be warranted to test if there is an underlying trend of clustering. Until then, this review has produced a useful reference of 24-h PM10 and SO2 AAQSs for policymakers in the developed and developing world.
Conclusion
In summary, most countries have 24-h AAQSs for both PM10 and SO2. The average AAQS for both PM10 and SO2 is substantially higher than the WHO AQG value. Several countries have promulgated AAQSs at the AQG value for PM10, but not SO2. Although AAQSs that pertain to 84% of the global population were identified, the global conclusions are limited by the lack of information in several regions. In the countries with data, however, air quality monitoring data seem to be considered the most frequently when setting and revising AAQS, followed by existing AAQSs in other countries, environmental epidemiology studies, and the WHO AQGs.
Relevance of findings
These findings, which cover 84% of the world population, have provided a set of benchmarks for evaluating the status of AAQSs. These benchmarks can provide policy makers with a broader perspective, when establishing and revising their own AAQSs. International organizations, such as the WHO, might also find these benchmarks useful when revising the AQGs. The information presented in this paper could also be utilized to advance econometric analyses of air quality regulations and economic and social indicators; and to promote further research on the implementation and enforcement of AAQSs.
Electronic supplementary material
Below is the link to the electronic supplementary material.
PDF 1.11 mb
Acknowledgments
We thank Aaron Cohen and Michal Krzyzanowski for their guidance, the Brian and Jennifer Maxwell Endowed Chair at the School of Public Health for partial funding, and Maureen Lahiff for statistical support.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Footnotes
Given time and resource constraints and the variety of averaging times for AAQSs, it was not feasible to conduct a comprehensive review of the national AAQSs for every pollutant in every country. Instead, this review was limited to daily (24-h averaging time) AAQSs for PM10 and SO2. This averaging time was selected because preliminary research indicated that 24-h is the most common averaging time for both pollutants. PM10 was selected instead of PM2.5 (particulate matter <2.5 μm in aerodynamic diameter) because preliminary results indicated that a larger proportion of countries have AAQSs for PM10 than PM2.5.
Contributor Information
Candace Vahlsing, Phone: +1-510-6430793, FAX: +1-510-6425815, Email: cvahlsing@gmail.com.
Kirk R. Smith, Email: krksmith@berkeley.edu
References
- Archer G, Davidson RD. In: GEMS/AIR: air quality management and assessment capabilities in 20 major cities. Williams W, editor. London: Monitoring and Assessment Center (MARC); 1996. [Google Scholar]
- Elsom D, Longhurst J, editors. Regional and local aspects of air quality management. Southampton: WIT; 2004. [Google Scholar]
- International Union of Air Pollution Prevention Associations . In: Clean air around the world: national and international approaches to air pollution control. 2. Murley L, editor. Brighton: International Union of Air Pollution Prevention Associations; 1991. [Google Scholar]
- Krzyzanowski M, Cohen A. Update of WHO air quality guidelines. Air Qual Atmos Health. 2008;1:7–13. doi: 10.1007/s11869-008-0008-9. [DOI] [Google Scholar]
- Maggioria CD, Lopez-Silva JA (2006) Vulnerability to Air Pollution in Latin America and the Caribbean Region. Latin America and Caribbean Region Sustainable Development Working Paper 28. The World Bank
- Schwela D, Haq G, Huizenga C, Wha-Jin H, Fabian H, Ajero M. Urban air pollution in Asian cities: status, challenges, and management. London: Earthscan; 2006. [Google Scholar]
- US EPA (2008) PM Standards Revision—2006. Available at: www.epa.gov. Accessed on Dec 2008
- WHO . Air quality guidelines for Europe. European series no. 23. Copenhagen: WHO Regional Publications; 1987. [PubMed] [Google Scholar]
- WHO . Air quality guidelines for Europe: 2nd ed, in European series, No. 91. Copenhagen: WHO Regional Publications; 2000. [PubMed] [Google Scholar]
- WHO . Guidelines for air quality. Geneva: World Health Organization; 2000. [Google Scholar]
- WHO . Air quality guidelines: global update 2005. Copenhagen: WHO Regional Office for Europe; 2006. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
PDF 1.11 mb