

Abstract
Suicide is the third leading cause of death among young adults worldwide. There is a growing recognition that prevention strategies need to be tailored to the region-specific demographics of a country and to be implemented in a culturally-sensitive manner. This review explores the historical, epidemiological and demographic factors of suicide in India and examines the strategies aimed at the prevention of suicide. There has been an increase in the rates of suicide in India over the years, although trends of both increases and decline in suicide rates have been present. Distinct from global demographic risk factors, In India, marital status is not necessarily protective and the female: male ratio in the rate of suicide is higher. The motives and modes of suicide are also distinct from western countries. Preventive strategies implemented at a community level and identifying vulnerable individuals maybe more effective than global strategies.
Keywords: Suicide, India, epidemiology, prevention
INTRODUCTION
Suicide‡ is among the top three causes of death among youth worldwide. According to the WHO, every year, almost one million people die from suicide and 20 times more people attempt suicide; a global mortality rate of 16 per 100,000, or one death every 40 seconds and one attempt every 3 seconds, on average. Suicide worldwide was estimated to represent 1.8% of the total global burden of disease in 1998; in 2020, this figure is projected to be 2.4% in countries with market and former socialist economies. According to the most recent World Health Organization (WHO) data that was available as of 2011,[1] the rates of suicide range from 0.7/100,000 in the Maldives to 63.3/100,000 in Belarus. India ranks 43rd in descending order of rates of suicide with a rate of 10.6/100,000 reported in 2009 (WHO suicide rates).[1] The rates of suicide have greatly increased among youth, and youth are now the group at highest risk in one-third of the developed and developing countries. The emerging phenomenon of “cyber-suicide” in the internet era is a further cause for concern;[2,3] also because the use of new methods of suicide are associated with epidemic increases in overall suicide rates.[4] Suicide is nevertheless a private and personal act and a wide disparity exists in the rates of suicide across different countries. A greater understanding of region-specific factors related to suicide would enable prevention strategies to be more culturally sensitive. This focus is also highlighted in the September 10, 2012 World Suicide Prevention Day theme “Suicide Prevention across the Globe: Strengthening Protective Factors and Instilling Hope”.[5] This qualitative review explores the historical and epidemiological aspects of suicide in with a special focus on India. We hope that exposure of the problem will facilitate primary prevention planning.
HISTORICAL PERSPECTIVE
The story of suicide is probably as old as that of man himself. Through the ages, suicide has variously been glorified, romanticized, bemoaned, and even condemned. Be it the tragic Greek heroes Aegeus, Lycurgus, Cato, Socrates, Zeno, Domesthenes or Seneca; or the Roman figures Brutus, Cassius, Mark Anthony or the Egyptian princess, Cleopatra; or Samson, Saul, Abimelech and Achitophel of the Old Testament; or the suicide bombers in the present world, the universality of suicide transcends religion and culture.[6]
An understanding of suicide in the Indian context calls for an appreciation of the literary, religious, and cultural ethos of the subcontinent because tradition has rarely permeated the lives of people for as long as it has in India. Ancient Indian texts contain stories of valor in which suicide as a means to avoid shame and disgrace was glorified. Suicide has been mentioned in the great epics of Ramayana and Mahabharata. When Lord Sri Ram died, there was an epidemic of suicide in his kingdom, Ayodhya. The sage Dadhichi sacrificed his life so that the Gods may use his bones in the war against the demons. The Bhagavad Gita condemns suicide for selfish reasons and posits that such a death cannot have “shraddha’, the all-important last rites. Brahmanical view had held that those who attempt suicide should fast for a stipulated period. Upanishads, the Holy Scriptures, condemn suicide and state that ‘he who takes his own life will enter the sunless areas covered by impenetrable darkness after death’.
However, the Vedas permit suicide for religious reasons and consider that the best sacrifice was that of one's own life. Suicide by starvation, also known as ‘sallekhana’, was linked to the attainment of ‘moksha’ (liberation from the cycle of life and death), and is still practiced to this day.[7] Sati, where a woman immolated herself on the pyre of her husband rather than live the life of a widow and Jahuar (Johar), in which Rajput women killed themselves to avoid humiliation at the hands of the invading Muslim armies, were practiced until as recently as the early half of the 20th century; stray cases continue to be reported*.[8,9]
EPIDEMIOLOGY
Suicide around the world
According to the World Health Organization (WHO), suicide in 2004 was the 8th leading cause of potential years of life lost worldwide among persons aged 15-44 years.[10] Suicide is the third leading cause of death among those aged 15-44 years, and the second leading cause of death in the 10-24 years age group in some countries; these figures do not include suicide attempts which may be up to 20 times more frequent than completed suicide. The rate of suicide is highest in Eastern European countries such as Belarus, Estonia, Lithuania, and the Russian Federation. High rates of suicide have also been reported in Sri Lanka, based on data from the WHO Regional Office for South-East Asia.[11] There is an interesting speculation that latitude and the daily amount of sunlight has an effect on rates of suicide.[12] Rates of suicide are higher in northern parts of Japan and in northern countries of Europe compared to the southern countries. However, countries at about the same latitude, such as the UK and Hungary, have substantially different rates of suicide (21.6/100,000 and 6.9/100,000, respectively, in 2009).[13] Low rates are found mainly in Latin America (notably Colombia and Paraguay) and some countries in Asia (eg., the Philippines and Thailand). Haiti reported no suicides in 2003. Countries in other parts of Europe, North America, and parts of Asia and the Pacific tend to fall in between these extremes. Eighty-six percent of all suicides occurred in the low and middle-income countries.[14]
A frequently cited cause for concern during recent decades is the global trend for increasing rates of suicide.[15] According to the WHO, suicide rates increased by 60% worldwide from 1950 to 1995.[16] The average rate of suicide increased from 10.1 per 100,000 in 1950 to 16 per 100,000 in 1995.[17] The global male suicide rates and total suicide rates in 1995 were the highest rates recorded in the 1950-1995 period (24.7 and 16 per 100,000, respectively). Interestingly, the global female suicide rate per 100,000 decreased from 8 in 1975-1980 to 6.9 in 1995.[17] However, the increase in global suicide rates must be interpreted with caution. The period from 1950 to 1995 witnessed changes in world politics and in reporting patterns which may have inflated the rates. For instance, the period witnessed the end of the USSR (which had an overall rate that was below the average) and its former republics (some of whom have the highest rates in the world) started to report individually, thus inflating the global rate. Secondly, the figures for 1950 were based on 11 countries only while the estimates in 1995 were based on 62 countries. It is likely that these 62 countries have higher rates and are countries where suicide is a major public health problem and were hence more likely to report on suicide mortality.[18]
Suicide in India
The suicide rate in India is comparable to that of Australia and the USA; and the increasing rates during recent decades is consistent with the global trend. Data on suicide in India are available from the National Crime Records Bureau (NCRB; Ministry of Home Affairs). The suicide rates in India rose from 6.3 per 100,000 in 1978 to 8.9 per 100,000 in 1990, an increase of 41.3% during the decade from 1980 to 1990, and a compound growth rate of 4.1% per year.[19] More recent data, however, reveal a different picture. The rate of suicide showed a declining trend from1999 to 2002 and a mixed trend during 2003-2006, followed by an increasing trend from 2006 to 2010.[20] During 2009, the rate was 10.9 per 100,000 population.[21] This represented a 1.7% increase in suicides since 2008.[22] In the most recent NCRB report the rate in 2010 rose to 11.4 per 100,000 population; an increase of 5.9% in the number of suicides.[20]
The NCRB data are based on police records. Sociocultural factors undermine the veracity of these records. Suicide attempt is a punishable offence under the Indian Penal Code (IPC Section 309); this results in under-reporting. Deaths in rural areas are certified by village headmen (“panchyatdars”) though all cases are investigated by the police. The process of registering a death is particularly inefficient in rural areas.[23] Eventually, only about 25% of deaths are registered and only about 10% are medically certified.[24,25] Death by suicide is frequently reported as due to illness or accident to avoid police investigation. The families of suicide victims usually do not want postmortems because of the fear of mutilation of the body, the time-consuming nature of the process, and the stigma involved. Statistics derived from police records hence under-report suicides.
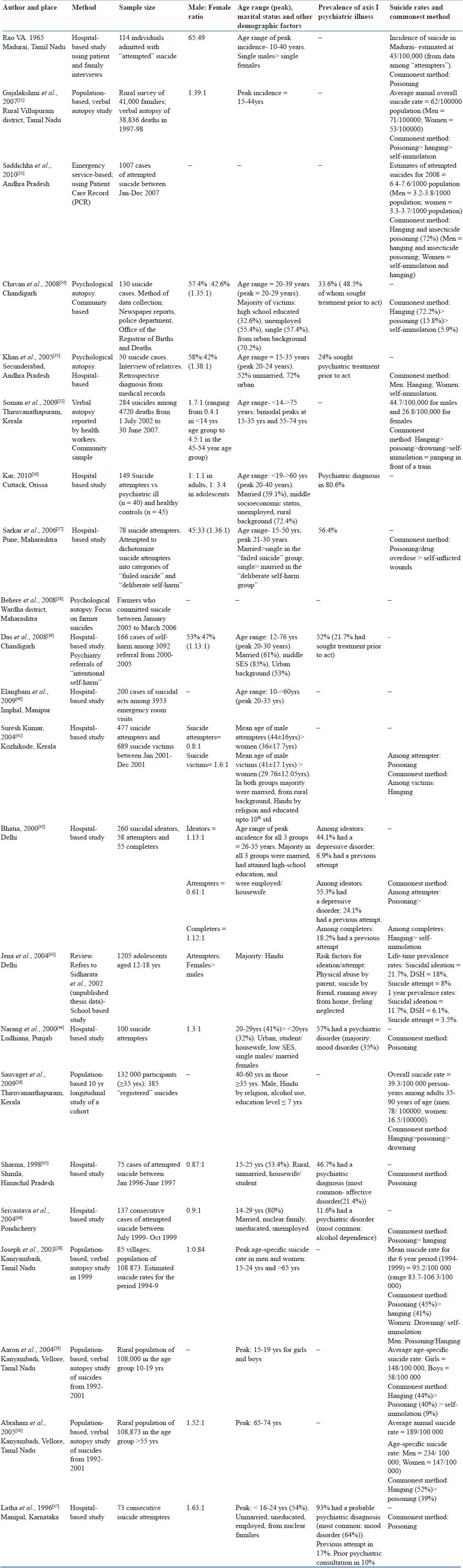
The suicide rates vary widely across the different states of India, ranging from 0.5/100,000 in Nagaland to 45.9/100,000 in Sikkim against the national average of 11.4/100,000 in 2010.[20] Some studies have estimated the annual suicide rate based on data from smaller samples and using different methods, such as hospital-based samples, longitudinal cohort,[26] emergency service[27] and verbal autopsy[28–32] [Table 1]. Studies using verbal autopsies report that suicide rates are 2-3 times higher than those reported in other studies.[28,31] The average annual suicide rate reported in these studies range from 62 per 100,000[31] to about 95 per 100,000 for the general population[28] with age-specific suicide rates as high as 148/100,000 and 58/ 100,000 for young women and men, respectively,[29] and 234/ 100,000 and 147/100,000 in elderly men and women, respectively.[30] This rate is about 9-10 times the rate reported by NCRB. It is important to remember that extrapolation of numbers based on small samples are likely to overestimate the true rate because it doesn’t factor in regional and age-, gender-specific variability which is likely to be present and is also reflected in the NRCB report. The true estimate is therefore likely to lie between the NCRB estimate and that reported in these studies.
Table 1.
Summary of selected studies on suicide and attempted suicide in India
Demographics of suicide in India
Traditionally, in western literature risk factors associated with suicide, including suicidal attempts - include young age (15-24 years), female gender, low educational attainment, unemployment, living alone, and history of socioeconomic deprivation.[48] In this section, we examine the demographics of suicide in India.
Age
Although suicide rates were commonly highest among older adult males, rates among young people have been increasing. Young adults are a particularly vulnerable group and currently show the highest rates of suicide the world over. Suicide is responsible for 6% of all deaths among young people.[49] Developed countries show a second peak of increased suicide rate in the elderly (above 60 years).
An Indian study showed that the suicide rate was highest in the 15-29 years age group (38 per 100,000 population) followed by the 30-44 years group (34 per 100,000 population). The rates of suicide was 18 per 100,000 in those aged 45-59 years and 7 per 100,000 in those aged >60 years.[50] Since these figures are calculated for the general population and not the age-specific “population of interest”, the higher risk in youth may reflect a higher representation of youth in the population.
The National Crime Records Bureau report of 2009 shows a similar pattern.[21] Youth in the age group 15-29 years accounted for the largest proportion (34.5%) of suicides followed by those in the age group 30-44 years (34.2%). Other studies in India also indicate that young adults are at increased risk, with ages 20-24 years followed by 25-29 years showing the highest rates of suicide in a psychological autopsy study,[35] and the15-39 age group identified as the most vulnerable in another study.[51] Two-thirds of women who completed suicide were <25 years.[52,53]
This trend is also seen in attempted suicides. In one study, the mean age of attempters was 25.3 years.[46] Suicidal ideation was also more common in the 16-45 years age group in a study of suicidal ideators in a general hospital setting.[54]
Adolescents and young adults
Youth is a period of heightened risk of suicide[55] and suicide is a leading cause of death among young people in India.[29] In a study which evaluated the cause of death among those aged 10-19 years, in a rural population of 108,000 in south India, suicide accounted for about a quarter of all deaths in males and between 50% and 75% of all deaths in females aged 10-19 years. The average suicide rate for girls was 148 per 100,000, and for boys, 58 per 100,000[29]
Among young people, suicidal behavior was found to be associated with female gender, not attending school or college, independent decision making, premarital sex, physical abuse at home, lifetime experience of sexual abuse, and probable common mental disorders.[56] Violence and psychological distress were independently associated with suicidal behavior. Factors associated with gender disadvantage increased vulnerability, particularly in rural women.[56]
Elderly
There is a global trend toward increased suicide in late life, again mainly in men.[57,58] However, in a 5 year study of 6312 suicide attempters, only 47 were above the age of 60 years.[59] The low prevalence of suicide among the elderly in India may be because the aged are well-integrated and respected in the family; children take responsibility for their care. Also, life expectancy in the elderly is lower in India than elsewhere, contributing to the comparatively lower suicide rate.[60]
The ratio of completed suicide to attempted suicide in India is about 1:7 in the elderly, which is double the ratio of 1:15 in lower age groups.[59] This may reflect a poorer ability of the elderly to recover from the bodily insult of a suicide attempt. Although studies from the west implicate social isolation, as defined by ‘living along’ as a risk factor for suicide among the elderly, an early study speculated that for elderly in India ‘family and social integration’ were the real determinants of risk, even if they were living by themselves.[61] More recent studies from the west appear to support this position.[62]
Gender
Globally, attempted suicide is commoner in women and completed suicide is commoner in men.[63] In Chinese women, however, the suicide rate is approximately twice that of women elsewhere.[1,63] Men commonly use more lethal modes and plan the act more meticulously to avoid detection. In contrast, women commonly use less lethal modes, and are more impulsive, less well planned, and more likely to be found and rescued. The male:female suicide ratio is 3.8, 3.9, 4.1, and 3.4 in Australia, Canada, the United States, and the UK, respectively[64] and it is lower in Asian countries.[65]
What are the data for India? Although some Indian studies have found a higher incidence of suicide in men than in women,[50] others have found the contrary.[52] The male:female suicide ratio was 1.78 in India in 2008 and 2009. In children up to age 14 years, the ratio was 1.04; that is, almost equal between the sexes.[21] In young men and women in 1991-1997, the ratio was 1.3, contrasting with the male preponderance in developed countries.[66] The reasons for greater female suicide completion in India may be sociocultural. The common practice of arranged marriages in India result in social and family pressure for the woman to stay married even in an abusive relationship; this may increase the risk of suicide in women.[67] Also, stresses related to dowry demands may drive young brides to suicide.[68]
And what of suicide attempters in India? Although attempted suicide was as high as 1.2 times higher in women relative to men in some studies[41] others studies showed a male predominance, male: female ratio ranging from 1.13:1[39] to 1.63:1.[47] These differences may be reconciled by an appreciation of social changes in India, with a shift toward nuclear families and the cultural emphasis on the male stereotype which the individual tries to fulfill in vain.
Marital status
In the West, marriage is generally protective against suicide; this empirical regularity is referred to as the “coefficient of preservation” based on Durkheim's 1897 seminal monograph Le Suicide.[69] Divorced, separated, widowed, and single people are more likely to commit suicide than married people. Persons living alone are at particular risk.[48] This protective effect of marriage was seen more for men than for women and rates of suicide decreased in order from widowers to divorced, single, and married men. Young widowers were at highest risk. Lower rates of suicide among married compared to unmarried women may be explained by sociological theories based on marital status integration and social integration.[70]
Marriage is not a strong protective factor for suicide attempts in developing countries.[71] In 2009, 70.4% of all suicide victims in India were married and 21.9% were unmarried. Divorcees and individuals who were separated accounted for about 3.4%, while widows and widowers comprised 4.3% of the total suicide victims.[21] In individual studies, some show higher attempted suicides among unmarried persons[37,44,45,72] while others show a higher rate among those who are married.[46,47] Among attempters, men were more likely to be single and women, married.[73] In a general hospital study, no suicide attempter was separated or living alone. Those who were unmarried were living with their extended families.[47] Widowed, separated and divorced individuals were commoner among cases of completed suicide relative to controls in a study of 100 suicide cases.[51]
The quality of marital relationship, emotional warmth, extended family support, and ability to handle stresses related to marriage and child rearing are more important than marital status, per se, but these qualifiers of marital status are difficult to study.
Education
Low intelligence results in a 2-3-fold increased risk of suicide. Possible explanations are that persons with low intelligence are less able to compete for jobs and therefore acquire lower income and social status. They may also be less efficient in coping with stress. Finally, neurodevelopmental vulnerabilities may increase their risk of a psychiatric disorder.[74]
Level of educational attainment is a surrogate marker of intelligence, though drawing conclusions on this premise is problematic when education is not universally available. The NCRB data reveal that 25.3% of suicide victims were educated up to primary level, 23.7% had a middle-school education, 21.4% were illiterate, and 3.1% were graduates or postgraduates.[21] These percentages, however, may reflect the proportion of persons with different educational attainment in India.
In one study of attempted suicide in India, 55.5% were uneducated.[46] In another study, 54% of suicide attempters had received high school education or higher.[47] Women attempting suicide tended to have a lower educational status compared to men.[72] Again, it is hard to interpret these percentages in the absence of information about the educational attainment of the population from which the samples originated.
Family structure
The sociological theory of suicide emphasizes social integration, a theme reflected in John Donne's “No Man is an Island”. People who are well integrated with their families and community have a good support system during crises, protecting them against suicide. Risk factors related to the family include parenting style, family history of mental illness and suicide, and physical and sexual abuse in childhood. “Affectionless control”, a parenting style characterized by a combination of low levels of emotional warmth and high levels of parental control or overprotection, is associated with a three-fold increase in the risk of suicidal behavior.[75] Suicide attempters with a history of sexual or physical abuse in childhood show more suicidal behavior and are at a higher risk for mental disturbances in adulthood even after controlling for other contributory factors.[76]
India has witnessed a change in family structure during recent decades, with more people moving out of joint and extended families into nuclear family structures. The effect of this change on suicide rate has not been systematically studied. Varying results in research may tap a secular trend. The majority of suicide attempters were from nuclear families,[46,47] possibly reflecting the role of social integration, though an earlier study shows that more suicide attempters come from joint families.[77] A study on burns victims found that being in a joint family was a risk factor for dowry deaths.[78] Another study found that family and marital conflict was a major reason for suicide.[36]
Urban vs. rural residence
The suicide rate is generally reported to be higher in urban areas because of a variety of stressors related to living and working in cities, including overcrowding and social isolation. In India, during the year 2000, though the suicide rate for the country was 10.8, the rate in urban areas was slightly lower at 9.94.[79] There has since been an increase in urban suicide rates to 11.4% in 2005, around 13% in 2006 and 2007, and 12.1% to 12.5% in 2008 and 2009.[21] Studies in recent years are consistent in this regard: suicide[35] and attempted suicide were more common in persons living in urban areas.
Occupation
There is a fairly strong association between unemployment rates and suicide, but the nature of this association is complex. Unemployment may drive up the suicide risk through factors such as poverty, social deprivation, domestic difficulties, and hopelessness. Furthermore, persons with psychiatric disorders are at higher risk of suicide and are also more likely to be unemployed; this may be a double whammy. Adding to the complexity is recent loss of employment vs long-term unemployment; the former is associated with greater risk.[80] The association between unemployment and suicide may also be more significant for young adults.[81] In India, in one study of suicide attempters, 46% were unemployed.[46] In another study, >50% of patients were employed, 12% were unemployed and some were either students or housewives.[47]
The NCRB data shows that housewives account for 18.6% of total persons committing suicides and for 52.8% of the total female victims. Those involved in farming and agriculture form the next largest group, comprising 11.9% of the total victims followed by those working in the private sector (7.8%) and unemployed (7.5%). and public sector (7.8% and 2.2%, respectively). Students accounted for 5.5% of total suicides while unemployed persons accounted for 5.5% and 7.5%, respectively. Those employed in the public sector (2.2% of total suicides) and government servants (1.3% of total suicides) were the least represented group.[20]
Precipitating event
The relationship of suicide to negative life events, stress, object loss, and negative interaction needs to be understood in the framework of a model of vulnerability, support, coping, and problem-solving. Rich and Bonner[82] found in a stress-vulnerability model that negative life events and stress accounted for 30% of the variance in suicidal ideation. Indian society, being sociocentric, lays importance on interpersonal relationships. It is therefore unsurprising that marital conflict is the commonest cause of suicide among women, while interpersonal conflict is the commonest cause among men.[20,52]
Other suicide triggers include physical illness, bankruptcy, illicit relationships, and drug intoxication. An interesting finding, rarely seen in the West, is the high rate of suicide associated with sexual abuse and illegitimate pregnancy.[20] This may be a reflection of cultural taboos related to sexuality in India.
A similar trend is seen for attempted suicide with interpersonal conflict, financial stressors, and educational burden being the most common triggers.[35,45,46,83] Chronic pain and illness is featured as a common reason in some studies.[46]
Studies which measured stressful life events found that approximately 90% of suicide attempters reported negative life events[47] and about 35% experienced stressful life events in the previous 6 months.[46] However, in the absence of a control group, it is hard to interpret the significance of life events. After all, everybody experiences stressful or negative life events.
Mode of suicide
The difference between countries in methods employed for suicide may reflect differences in socioeconomic factors, availability of lethal means, and firearms legislation, rather than differences in the nature of the behavior, per se. Common methods used in developed countries include firearms, car exhaust asphyxiation, and poisoning whereas in developing countries, pesticide poisoning, hanging, and self-immolation lead the list.
In India, during 2009 consumption of a poison (33.6%), hanging (31.5%), self immolation (9.2%), and drowning (6.1%) were the commonest modes of suicide.[21] Jumping from buildings accounted for 1.5%. This pattern is recapitulated in the NCRB 2010 report.[20]
Studies show that consumption of pesticides, such as the readily available agricultural pesticides in rural areas, is the commonest means of suicide and attempted suicide in India[45,46,52] and in rural areas of low income countries.[84] Agricultural chemical poisoning has also been reported in Japan,[85] Thailand,[86] Sri Lanka,[87] Bangladesh,[88] and the USA.[89] Men are more likely to use organophosphate poisons and women are more likely to use plant poisons.[72] The use of plant poisons as a means of suicide/attempted suicide is more common in India and south-east Asia.[90] It is however, interesting to note that the increased accessibility to plant poisons over the internet has led to reports of their use in other parts of the world as well.[91,92] The use of aluminium phosphide, a fumigant used to protect grain stores, is associated with a case fatality of >70% and is a particular feature of self-poisoning in northern India.[93]
Suicide by hanging is the next most frequent method in India.[22,35,94] The profile of victims comprises married females or unmarried males in the age group of 21-30 years, faced with stressors in the form of unemployment, harassment for dowry, prolonged illness, failure in examinations, financial duress, or interpersonal problems.[95] Drug overdose using medically prescribed and non-prescribed drugs is another common though less frequent method.[96] Violent methods such as drowning, jumping from a height, and strangulation are less common.[47]
Self-immolation accounts for <1% of suicides in western studies[97] but has strong sociocultural motivations in Indian culture, and accounts for a substantial proportion of suicides. With the practice of Sati and Jauhar, in ancient India, self-immolation was seen as an escape from hardship and humiliation. More recently, self-immolation has been employed in India as a means of protest against government policy,[98] as by Buddhist monks in South Vietnam and Sri Lanka. Indian women may be over-represented in the population of self-immolators with domestic issues as a trigger.[72,99]
MOTIVES FOR SUICIDE
A truism in suicide literature is that “not all persons who commit suicide want to die and not all persons who want to die commit suicide”. The intentionality and lethality of suicide are important dimensions which describe the motive behind the act. Lethality is a function of the mode of suicide and has already been examined in an earlier section. Motives may go beyond Freud's concept of the ‘wish to kill’, the ‘wish to die’ and the ‘wish to be killed’, and beyond Durkhiem's sociological typology; and may be more complex than just a cry for help. The motive for suicide may be as diverse as a need for identification as in the case of ‘copy-cat’ suicides (also called the Werther effect) to delusional beliefs as in the case of Klingsor syndrome (genital self-mutilation based on religious delusions).[100]
An Indian study of suicide attempters classified motivation into ‘the wish for change’ and ‘the wish to die’ groups and found that the former had low lethality, lack of planning for their attempt, more likelihood of rescue and were not intoxicated during the attempt. The latter group utilized more drastic measures, such as hanging and was more likely to have a psychiatric disorder with comorbid alcoholism.[101]
In India, the top 10 causes or correlates of suicide in 2009 were family problems (23.7%), illness (21%) [including insanity/mental illness (6.7%)], unemployment (1.9%), love affairs (2.9%), drug abuse/addiction (2.3%), failure in examination (1.6%), bankruptcy or sudden change in economic status (2.5%), poverty (2.3%), and dowry dispute (2.3%).[21] The high rates of suicide among persons with mental illness and drug abuse/addiction, though not a measure of intent, are of much concern. Many of the remaining causes [namely, suspected/illicit relation, cancellation/nonsettlement of marriage, not having children (barrenness/impotency), death of a dear one, dowry dispute, divorce, ideological causes/hero worship, illegitimate pregnancy, physical abuse (rape, incest, etc.), poverty, professional/career problem][21] reflect the unique social structure of our society and the social pressures that individuals face.
Studies on suicide notes report that a last wish was mentioned in 30%.[94] Mass suicides are seen as suicide pacts in couples or families[20] rather than as part of religious cults as in western societies. Suicide pacts are rare, accounting for <1% of all suicides, and there is a trend in western literature showing a decrease in rates over the years.[102] Suicide pacts almost always involve people well known to each other, mostly spouses, most of them childless.[103] However, there is an emerging trend for cyber-based internet-facilitated suicide pacts which increasingly involve two or more strangers who meet on the internet and share similar world views.[2] Such cases have been reported in the press, but have not been studied in a scientific manner.
Psychiatric diagnosis
Mental disorders (particularly depression and alcohol use disorders) are a major risk factor for suicide in Europe and North America; however, in Asian countries impulsiveness plays an important role. It is often reported that rates of psychiatric disorders are higher among suicide completers in developed countries relative to developing countries, though under-diagnosis in developing countries is a possible explanation.
Studies in India show varying results with rates of psychiatric disorders ranging from 9.5 to 24.9%.[104,105] In one psychological autopsy study, 24% of suicides had a psychiatric diagnosis, namely major depressive disorder, bipolar affective disorder, or schizophrenia; substance abuse was prevalent in 18%.[35] In a study of attempted suicide, 11.6% had a psychiatric diagnosis with alcohol dependence followed by depression being the commonest diagnoses; schizophrenia, conduct disorder, and personality disorder comprised the rest.[46] In a psychological autopsy of 100 consecutive suicides in a rural population, 37% had a DSM-III-R psychiatric diagnosis; alcohol dependence (16%) and adjustment disorders (15%) were the commonest diagnoses, and schizophrenia, major depressive episode, and dysthymia constituted a smaller proportion (2% each).[106]
Rates of psychiatric diagnosis as high as 46.7%,[45] 59.7%,[54] 57%[107] and even 93%[47] have been described among suicide attempters. Mood disorders, particularly depressive disorders, were the most common diagnosis followed by alcohol abuse.[47,107] Neurotic, stress-related, and somatoform disorders were diagnosed in 14.5%[108]
In a study of patients with major depressive disorder with suicidal ideation, incidence of suicidal attempt was 16.6%, all attempters were <30 years old.[73] Suicidal attempt has also been found to be positively correlated with severity of depression.[109]
Dysthymia underlying suicidal behavior is commoner in India than in the West.[47,108] In a general hospital study on suicidal ideation, psychiatrically ill patients were overrepresented: 59.74% had depression followed by substance abuse and psychosis in 9.74% each. 9.09% were diagnosed with bipolar disorder and 7.14% constituted a group with neurotic disorders.[54]
In a study of 1560 patients with schizophrenia, the rate of attempted suicide was 4.7%. These patients did not differ in illness duration from patients with depression who had attempted suicide.[110]
Personality disorders
Multiple suicide attempts of low intentionality and lethality are typically associated with maladaptive coping and impulsivity in personality disorders. The rate of personality disorders among those who attempt suicide in India ranges from 7 to 50% in various studies.[47,108,110] The most common diagnoses were schizoid, borderline, and antisocial personality disorders.[110] In a study of personality disorder among first attempters, the most common diagnoses were anankastic and histrionic personality disorder.[108] In a 16-PF study of personality, self-immolators were found to lack ego strength, lack frustration tolerance, be emotionally less stable, and be impulsive.[111] The association of impulsivity and marital discord among self-immolators has been frequently reported in Indian[99] and other Asian studies.[112]
Physical illness
Chronic physical illness, abnormal vaginal discharge, and tobacco use are risk factors for common mental disorders among women in India.[113] A similar pattern is seen among suicide attempters. About one-fifth were found to have a physical illness in one study with dysmenorrhoea being the commonest ailment, followed by peptic ulcer disease; hypertension, bronchial asthma and arthritis comprised the remaining.[46] Pain in the abdominal and pelvic regions has been reported more frequently among attempters.[46,114] This finding was also reported in Hispanics[115] and Americans.[116]
OTHER RISK FACTORS
In one study, depression and suicidal tendency were associated with early parental deprivation, recent bereavement, and family history of suicidal behavior.[117] In another study, suicidal attempt was positively correlated with severity of depression, male sex, being married, employed, and <35 years of age.[109]
Alcoholism is another risk factor with both high rates of suicide among alcoholics and high proportion of alcoholics among suicide attempters (Agarwal et al.1996). The risk of suicide is higher with early onset of alcohol use, dependence pattern of use, family history of alcohol dependence and depression, and comorbid antisocial personality disorder.[118] Spouses of alcoholics are also at increased risk of attempted suicide.[105,119] Determinants of suicidal attempts in this subpopulation include financial difficulties, marital discord, delusional jealousy, and suicidal ideation expressed by the alcohol abuser. Of significance is the emotional reaction of women in response to suspicion of their fidelity, reflecting the value Indian culture imposes on chastity.[120]
Predicting suicide
In a 10-year prospective study of patients admitted with suicidal ideation, Beck et al. found that only the Hopelessness Scale and pessimism items on the Beck Depressive Inventory predicted suicides. A score of 10 or more on the Hopelessness Scale correctly identified 91% of eventual suicides.[121] Hopelessness has been found to have a positive correlation with degree of suicidal intent.[122] 85% of children and adolescents in the 12-19 years age group had expressed suicidal ideation prior to the event.[123]
Scales used to identify suicidal risk include SAD PERSONS scale, Beck Suicidal Intent Scale and the Suicidal Intent Questionnaire (SIQ) validated in the Indian setting.[124] The SIQ consists of a 10-item questionnaire which is scored as 0, 1 or 2. The scale was initially piloted in 40 patients with suicidal ideas and 40 controls, and subsequently tested in a clinical sample (n=278) consisting of patients with schizophrenia, bipolar disorder and “neurosis”. The scale identified suicidal ideation in about 35% of this sample. In a more recent study of communication of suicidal intent among suicide attempters, Srivastava et al.[109] reported that the majority of the sample (73.3%) communicated suicidal intent using the SIQ. The scores on the SIQ showed a low positive correlation with the Hamilton Depression scale.[109]
Attempted suicide is of particular interest as it has been found to be one of the predictors of future suicide.[125] This fact is reiterated in studies which show that about 18% of suicide victims had a previous suicide attempt.[42]
Attempters vs. completers
Are persons who attempt suicide different from those who succeed? An Indian study which compared these two groups found more similarities than differences. Both groups consisted of predominantly middle aged, unemployed, married males and housewives, with high school education and from rural background. The study concluded that attempters with high intent/lethality and completers were overlapping populations.[41] These findings are unlike the younger age for attempters and higher age for completers reported in western studies.[126]
The significant risk factors for fatal suicide includes presence of previous suicidal attempt, interpersonal conflicts and marital disharmony, alcoholism, presence of a mental illness, sudden economic bankruptcy, domestic violence, and unemployment.[67] Individuals completing suicides did not have a positive outlook toward life, problem-solving approaches, and coping skills.
In an analysis of suicide attempters which distinguished between those who had intended to die but accidentally survived (failed suicide group) and those who had not intended to die (deliberate self-harm group), Sarkar et al. found that, in the former, the attempts were planned, intentionality and lethality were high, and most attempted to conceal the act. The latter comprised adolescents and young adults who were unmarried and had emotionally unstable and/or histrionic personality traits. The attempts in this group were impulsive, of low intentionality and lethality, and most sought help after the attempt.[37]
Locations of suicide
The location of suicide offer clues to the individual's psychological state and to the intentionality of suicide. Few studies reported this detail. In one study, home was the most common place for committing suicide.[94] Approximately a third of males preferred sites outside their homes, especially hotel rooms, river beds, and the work place. Most males who consumed an insecticide or resorted to self-immolation did so at home.[127] In another study, indoor incidence was almost double the outdoor incidence, mostly in rainy season, and almost equally during day and night.[83] A negligible proportion of women chose a site outside their homes, possibly reflecting the sociocultural traditions that restrict the movement of women outside the household.[127–129]
Special populations
Cancer
Cancer was found to be related to 0.6% of all suicides in 2010.[20] In a study of terminally ill cancer patients, 18.5% expressed suicidal ideation.[130] The rates of depression among patients with cancer range from 16.7[130] to 34.4%.[131] Depression, hopelessness and poorly controlled pain are significant predictors of suicide[132] whereas spiritual coping is associated with a better quality of life.[133] The particular challenges in reducing the risk of suicide among patients with cancer relate to the stigma of cancer and suicide, the fear of criticism at harboring suicidal thoughts, the lack of awareness of the diagnosis of cancer or what it means, cultural taboos and degree of family support.
Epilepsy
Psychiatric morbidity is known to be higher among patients with epilepsy relative to the general population, with rates of suicide being five times higher.[134] In a hospital-based study, the rate of attempted suicide was 16% among epileptics with 88% of patients having overdosed themselves with antiepileptic drugs.[135]
Farmer suicides
Farmer suicides are a particular concern in the India, although this phenomenon has been reported in England and Wales as well.[136] In India, 182,936 farmers were recorded to have committed suicide between 1997 and 2007.[137] The actual numbers may be larger, partly because the NCRB defines ‘farmers’ as men (but not women) who work in agriculture. About two-thirds of these suicides were in 5 of the 28 states and 7 union territories: Maharashtra, Karnataka, Andhra Pradesh, Madhya Pradesh and Chattisgarh account for about a third of the country's population but two-thirds of farmer suicides. Factors contributing to the high rate of suicide in this vulnerable population include economic adversity, exclusive dependence on rainfall for agriculture, and possibly monetary compensation to the family following suicide.[38]
NEUROBIOLOGY
Studies on the neurobiology of suicide have implicated dysfunction of serotonin, dopamine, acetylcholine, adrenaline, noradrenaline, opioid, GABA, and glutamate systems. Abnormalities have been reported in the hypothalamic-pituitary-adrenal axis, lipid metabolism, polyamines, growth factors, and astrocytes and other glial cell.[138] An Indian study reported low levels of CSF 5-HIAA in a subgroup of patients with depression.[139] This finding was also obtained in patients with schizophrenia and nondepressed, nonpsychotic persons who attempted suicide.[140] The low CSF 5-HIAA levels may be a marker of violent suicide attempts.[141] In another study, very low levels of melatonin were found to correlate with hopelessness and could hence constitute a predictor of suicide.[142]
There is some literature that lipid-lowering agents may increase deaths due to suicide or violence, presumably via increased insulin secretion and low serotonin turnover.[143,144] Suicide attempters were found to have lower total serum cholesterol levels compared to controls in one Indian study.[144]
Role of the media
The role of the media is becoming increasingly relevant. The media and internet have been identified as playing a crucial role in the dispersion of information about novel suicide methods.[145] A case in point is the trend of suicide epidemics in South-East Asia, namely the epidemics of charcoal burning in Hong Kong (1998-2002) and self-poisoning with seeds of the yellow oleander tree in Northern Sri Lanka (1980s to mid 1990s).[84,145–147] These two methods were initially rarely observed within national suicide statistics. However, extensive media reporting of a few cases was blamed for the subsequent increase in popularity of these methods.
In Vienna, media guidelines for the responsible reporting of suicides were introduced in 1987, banning newspapers from reporting the method of suicides.[148] It was hypothesized that the 80% reduction in the rates of subway suicides observed in the subsequent 6 months was due to the introduction of these guidelines. A more recent study using interrupted time series analysis has confirmed these findings and the authors believed that the effects were due to changes in the quality and quantity of reporting.[149]
The media can also have a positive influence. The ‘Papageno’ protective effect of media reporting describes how articles on individuals who adopted coping strategies other than suicidal behavior in adverse circumstances, were negatively associated with suicide.[150] The media can also be a source of information about where to seek help and advice. In an interesting study, Ramdas et al.,[151] evaluated the effectiveness of a one-day workshop wherein journalists and mental health professionals devised a guideline aimed at responsible reporting of suicide by the media, paying specific attention to avoid normalizing, idealizing, or sensationalizing suicide, and encouraging readers to seek help themselves or refer those in need. The quality of media reports that appeared in a leading newspaper were assessed at 1 year, 2 years and 6 years after the workshop. Although the study found a non-significant improvement in reporting standards, newspaper reports continued to normalize/glorify suicides and report suicide as the only method of coping.
PREVENTION
Suicide is an important, largely preventable public health problem. The problem is however a difficult one; as aptly expressed by Gajalakshmi et al as “a complex array of factors such as poverty, low literacy level, unemployment, family violence, breakdown of the joint family system, unfulfilled romantic ideals, inter-generational conflicts, loss of job or loved one, failure of crops, growing costs of cultivation, huge debt burden, unhappy marriages, harassment by in-laws and husbands, dowry disputes, depression, chronic physical illness, alcoholism/drug addiction, and easy access to means of suicide.”[31]
In 2000, the WHO launched the multisite intervention study on suicidal behaviors (SUPRE-MISS) which aimed to increase knowledge about suicidal behaviors and about the effectiveness of interventions for suicide attempters in culturally diverse places around the world.
Early detection and adequate treatment of a primary psychiatric disorder is of paramount importance. In psychiatrically ill subjects, lithium,[152–154] clozapine.[155–157] olanzapine,[158] antidepressants,[159] and behavioral interventions such as dialectical behavior therapy, DBT[160] have been shown to have antisuicidal effects.
Since the greatest predictor of completed suicide is the presence of a previous suicide attempt, interventions aimed at suicide attempters may be the most effective in reducing suicide rates. Vijayakumar et al., 2011[161] examined the efficacy of brief intervention and regular contact in a randomized controlled trial in suicide attempters and found that it did reduce rates of completed suicide over an 18-month period. Importantly however, the care received by the treatment-as-usual arm in this study was below desirable standards because it was limited to the acute management of the somatic sequelae of the suicide attempt and did not include psychiatric or psychological assessment or treatment.
In a psychological autopsy, 24% of suicide completers had consulted a psychiatrist/ physician before the event and family of the victim were aware of their suicidal intent in 68% of cases.[35] This finding is similar to data from the west, where two-third visited their general practitioners in the month prior to death and 40% in the week before.[162] This calls for adequate training of general practitioners in detection and referral of patients with common mental disorders, which may result in a significant decline in suicide rates.[163] This may also have to be culturally sensitive; the higher rate of somatic symptoms, rather than cognitive symptoms, among depressed patients in the Indian setting, is a case in point.[164]
The early identification and treatment of vulnerable populations with risk factors for suicide across the life-span is another strategy. Given the strong link between negative life-events early in childhood and suicide risk, it is important to identify populations that have been exposed to traumatic childhood experiences, such as sexual/physical abuse and parental domestic violence. The identification of such individuals requires a multidisciplinary approach with active participation from teachers and school authorities, health professionals and the legal system. Primary prevention strategies include promoting positive health and instilling adaptive coping stategies among children; improving awareness among parents, teachers and healthcare professionals regarding child-rearing practices and early intervention for maldaptive coping styles. At the community level, the establishment of social programs such as child and family support programs and programs aimed at achieving gender and socio-economic equality maybe prove useful.[165]
The need for a strategy which will raise awareness and help make suicide prevention a national priority has long been recognized.[166] Such a national strategy will need a comprehensive approach that encompasses the promotion, coordination, and support of activities to be implemented across the country at national, regional, and local levels. The program would need to be tailored for populations at risk. For example, prevention programs aimed at children and young adults would have to address issues related to gender inequality, physical/sexual abuse, violence and mental illness.[56] Strategies with empirical evidence in western literature such as the Universal, Selective, Indicated (USI) model,[167] ‘gatekeeper training’[168] and outpatient follow-up and emergency outreach[169] may also be relevant to India. The USI model outlines ‘universal’ preventive strategies for the population as a whole (eg., restricted access to lethal means), ‘selective’ strategies targeting at-risk individuals (eg. psychiatrically ill, homeless, socially-excluded groups) and ‘indicated prevention’ strategies targeting suicide attempters (eg. outpatient contact and emergency outreach). Gatekeeper training focuses on skill development to enable community members such as teachers, coaches and others in the community to identify signs of depression and suicide-related behaviors among youth. It encourages individuals to maintain a high index of suspicion and to inquire directly about distress, persuade suicidal individuals to accept help, and serve as a link for local referrals. Such approaches would also require a multidisciplinary team approach involving psychiatrists, general physicians, psychiatric nurses, psychiatric social workers, and non-governmental organizations (NGOs).
The role of the media is becoming increasingly relevant. A delicate balance needs to be maintained between press freedom and responsibility of the press to minimize the harm to vulnerable individuals. The role of advocacy and legislature cannot be over-emphasized. Laws restricting availability of lethal agents such as firearms have been advocated by the WHO. NGOs can play an important role in advocacy as exemplified by the proactive stance taken by the NGO Sneha which found that the suicide rate was highest among students who had failed in one subject. Subsequently, the government introduced a new scheme in 2002 wherein students who fail in one subject can rewrite their examination within a month and can pursue their further studies without losing an academic year.[170]
The task of suicide prevention is daunting. Although suicide attempters are at increased risk of completed suicide, about 10% of attempters persistently deny suicidal intent. This group may continue to be vulnerable. Though restricting availability of lethal means appears to be a possible solution,[171] an early study in India in West Bengal, where legislation was introduced to restrict sale of a pesticide, found no reduction in the overall suicide rate, but merely a change in the modes of suicide.[53] The solutions to suicide prevention may prove to be more complex than the problem of suicide itself.
Footnotes
‡The word “suicide” was first used by the English author, Sir Thomas Browne in 1642 in his treatise “Religio Medici”. The word originated from SUI (of oneself) and CAEDES (murder).
*Vijayakumar, 2004[8] refer to Sati and Jahuar as “altruistic suicides” while they may be classified more accurately as “fatalistic suicides”.
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.World Health Organization. Suicide rates per 100,000 by country, year and sex. [Last accessed on 2012 Mar 27]. Available from: http://www.who.int/mental_health/prevention/suicide_rates/en/index.html .
- 2.Rajagopal S. Suicide pacts and the internet. BMJ. 2004;329:1298–9. doi: 10.1136/bmj.329.7478.1298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Birbal R, Maharajh HD, Clapperton M, Jarvis J, Ragoonath A, Uppalapati K. Cybersuicide and the adolescent population: Challenges of the future? Int J Adolesc Med Health. 2009;21:151–9. [PubMed] [Google Scholar]
- 4.Thomas K, Chang SS, Gunnell D. Suicide epidemics: The impact of newly emerging methods on overall suicide rates - a time trends study. BMC Public Health. 2011;11:314. doi: 10.1186/1471-2458-11-314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.International Association for Suicide Prevention. World Suicide Prevention Day. Sep 10, [Last cited in 2011]. Available from: http://www.iasp.info/wspd/2011_wspd.php .
- 6.Evans G, Norman L. The Encyclopedia of Suicide. New York, NY: Facts on File; 1988. Farberow. [Google Scholar]
- 7.Braun W. Sallekhana: The ethicality and legality of religious suicide by starvation in the Jain religious community. Med Law. 2008;27:913–24. [PubMed] [Google Scholar]
- 8.Bhugra D. Sati: A type of nonpsychiatric suicide. Crisis. 2005;26:73–7. doi: 10.1027/0227-5910.26.2.73. [DOI] [PubMed] [Google Scholar]
- 9.Vijayakumar L. Altruistic suicide in India. Arch Suicide Res. 2004;8:73–80. doi: 10.1080/13811110490243804. [DOI] [PubMed] [Google Scholar]
- 10.World Health Organization. Global Burden of Disease. 2004. [Last cited in 2004]. Update. Available from: http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf .
- 11.Gururaj GA, Isaac MK, Latif MA, Abeyasinghe R, Tantipiwatanaskul P. SEA/Ment/118. New Delhi: WHO/SEARO; 2001. Suicide prevention- emerging from darkness. [Google Scholar]
- 12.Terao T, Soeda S, Yoshimura R, Nakamura J, Iwata N. Effect of latitude on suicide rates in Japan. Lancet. 2002;360:1892. doi: 10.1016/S0140-6736(02)11761-2. [DOI] [PubMed] [Google Scholar]
- 13.Hawton K, van Heeringen K. Suicide. Lancet. 2009;373:1372–81. doi: 10.1016/S0140-6736(09)60372-X. [DOI] [PubMed] [Google Scholar]
- 14.Department of injuries and violence prevention. Noncommunicable Diseases and Mental Health Cluster. Geneva: WHO; 2002. WHO. The Injury Chart Book. A graphical overview of the global burden of injuries. http://whqlibdoc.who.int/publications/924156220x.pdf . [Google Scholar]
- 15.Diekstra RF. Suicide and the attempted suicide: An international perspective. Acta Psychiatr Scand Suppl. 1989;354:1–24. doi: 10.1111/j.1600-0447.1989.tb03043.x. [DOI] [PubMed] [Google Scholar]
- 16.WHO. Suicide prevention (SUPRE) [Last accessed on 2012 Mar 27]. Available from: http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/
- 17.Department of Mental Health, Social Change and Mental Health. Geneva: WHO; 1999. WHO. Figures and facts about suicide 1999. http://whqlibdoc.who.int/hq/1999/WHO_MNH_MBD_99.1.pdf . [Google Scholar]
- 18.Bertolote JM, Fleischmann A. Suicide and psychiatric diagnosis: A worldwide perspective. World Psychiatry. 2002;1:181–5. [PMC free article] [PubMed] [Google Scholar]
- 19.Accidental Deaths and Suicides in India 1990. New Delhi: Ministry of Home Affairs, Government of India; 1992. National Crime Records Bureau. [Google Scholar]
- 20.Accidental Deaths and Suicides in India 2008. New Delhi: Ministry of Home Affairs, Government of India; 2010. National Crime Records Bureau. [Google Scholar]
- 21.Accidental Deaths and Suicides in India 2007. New Delhi: Ministry of Home Affairs, Government of India; 2009. National Crime Records Bureau. [Google Scholar]
- 22.Accidental Deaths and Suicides in India 2006. New Delhi: Ministry of Home Affairs, Government of India; 2008. National Crime Records Bureau. [Google Scholar]
- 23.Bose A, Konradsen F, John J, Suganthy P, Muliyil J, Abraham S. Mortality rate and years of life lost from unintentional injury and suicide in south India. Trop Med Int Health. 2006;11:1553–6. doi: 10.1111/j.1365-3156.2006.01707.x. [DOI] [PubMed] [Google Scholar]
- 24.Bhat M. Vol. 7. Minneapolis, MI, United States: Centre for Population Analysis and Policy, Humphrey Institute of Public Affairs, University of Minnesota; 1991. Mortality from accidents and violence in India and China, Research Report 91-06-1. [Google Scholar]
- 25.Ruzicka LT. Suicide in countries and areas of the ESCAP region. Asia Pac Popul J. 1998;13:55–74. [PubMed] [Google Scholar]
- 26.Sauvaget C, Ramadas K, Fayette JM, Thomas G, Thara S, Sankaranarayanan R. Completed suicide in adults of rural Kerala: Rates and determinants. Natl Med J India. 2009;22:228–33. [PubMed] [Google Scholar]
- 27.Saddichha S, Prasad MN, Saxena MK. Attempted suicides in India: A comprehensive look. Arch Suicide Res. 2010;14:56–65. doi: 10.1080/13811110903479060. [DOI] [PubMed] [Google Scholar]
- 28.Joseph A, Abraham S, Muliyil JP, George K, Prasad J, Minz S, et al. Evaluation of suicide rates in rural India using verbal autopsies, 1994-9. BMJ. 2003;326:1121–2. doi: 10.1136/bmj.326.7399.1121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Aaron R, Joseph A, Abraham S, Muliyil J, George K, Prasad J, et al. Suicides in young people in rural southern India. Lancet. 2004;363:1117–8. doi: 10.1016/S0140-6736(04)15896-0. [DOI] [PubMed] [Google Scholar]
- 30.Abraham VJ, Abraham S, Jacob KS. Suicide in the elderly in Kaniyambadi block, Tamil Nadu, south India. Int J Geriatr Psychiatry. 2005;20:953–5. doi: 10.1002/gps.1385. [DOI] [PubMed] [Google Scholar]
- 31.Gajalakshmi V, Peto R. Suicide rates in rural Tamil Nadu, south India: Verbal autopsy of 39 000 deaths in 1997-98. Int J Epidemiol. 2007;36:203–7. doi: 10.1093/ije/dyl308. [DOI] [PubMed] [Google Scholar]
- 32.Soman CR, Safraj S, Kutty VR, Vijayakumar K, Ajayan K. Suicide in south India: A community-based study in Kerala. Indian J Psychiatry. 2009;51:261–4. doi: 10.4103/0019-5545.58290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Saddichha S, Vibha P, Saxena MK, Methuku M. Behavioral emergencies in India: A population based epidemiological study. Soc Psychiatry Psychiatr Epidemiol. 2010;45:589–93. doi: 10.1007/s00127-009-0103-8. [DOI] [PubMed] [Google Scholar]
- 34.Chavan BS, Singh GP, Kaur J, Kochar R. Psychological autopsy of 101 suicide cases from northwest region of India. Indian J Psychiatry. 2008;50:34–8. doi: 10.4103/0019-5545.39757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Khan FA, Anand B, Devi MG, Murthy KK. Psychological autopsy of suicide-a cross-sectional study. Indian J Psychiatry. 2005;47:73–8. doi: 10.4103/0019-5545.55935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kar N. Profile of risk factors associated with suicide attempts: A study from Orissa, India. Indian J Psychiatry. 2010;52:48–56. doi: 10.4103/0019-5545.58895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sarkar P, Sattar FA, Gode N, Basannar DR. Failed suicide and deliberate self-harm: A need for specific nomenclature. Indian J Psychiatry. 2006;48:78–83. doi: 10.4103/0019-5545.31594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Behere PB, Behere AP. Farmers’ suicide in Vidarbha region of Maharashtra state: A myth or reality? Indian J Psychiatry. 2008;50:124–7. doi: 10.4103/0019-5545.42401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Das PP, Grover S, Avasthi A, Chakrabarti S, Malhotra S, Kumar S. Intentional self-harm seen in psychiatric referrals in a tertiary care hospital. Indian J Psychiatry. 2008;50:187–91. doi: 10.4103/0019-5545.43633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Elangbam V, Singh AB, Devi KS, Devi LU. Suicidal acts reported at a teaching hospital in manipur. Indian J Community Med. 2009;34:357–8. doi: 10.4103/0970-0218.58400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Suresh Kumar PN. An analysis of suicide attempters versus completers in Kerala. Indian J Psychiatry. 2004;46:144–9. [PMC free article] [PubMed] [Google Scholar]
- 42.Bhatia MS, Aggarwal NK, Aggarwal BB. Psychosocial profile of suicide ideators, attempters and completers in India. Int J Soc Psychiatry. 2000;46:155–63. doi: 10.1177/002076400004600301. [DOI] [PubMed] [Google Scholar]
- 43.Jena S, Sidhartha T. Non-fatal suicidal behaviors in adolescents. Indian J Psychiatry. 2004;46:310–8. [PMC free article] [PubMed] [Google Scholar]
- 44.Narang RL, Mishra BP, Nitesh M. Attempted suicide in Ludhiana. Indian J Psychiatry. 2000;42:83–7. [PMC free article] [PubMed] [Google Scholar]
- 45.Sharma RC. Attempted suicide in Himachal Pradesh. Indian J Psychiatry. 1998;40:50–4. [PMC free article] [PubMed] [Google Scholar]
- 46.Srivastava MK, Sahoo RN, Ghotekar LH, Dutta S, Danabalan M, Dutta TK, et al. Risk factors associated with attempted suicide: A case control study. Indian J Psychiatry. 2004;46:33–8. [PMC free article] [PubMed] [Google Scholar]
- 47.Latha KS, Bhat SM, D’Souza P. Suicide attempters in a general hospital unit in India: Their socio-demographic and clinical profile--emphasis on cross-cultural aspects. Acta Psychiatr Scand. 1996;94:26–30. doi: 10.1111/j.1600-0447.1996.tb09820.x. [DOI] [PubMed] [Google Scholar]
- 48.Schmidtke A, Bille-Brahe U, DeLeo D, Kerkhof A, Bjerke T, Crepet P, et al. Attempted suicide in Europe: Rates, trends and sociodemographic characteristics of suicide attempters during the period 1989-1992. Results of the WHO/EURO Multicentre Study on Parasuicide. Acta Psychiatr Scand. 1996;93:327–38. doi: 10.1111/j.1600-0447.1996.tb10656.x. [DOI] [PubMed] [Google Scholar]
- 49.Patton GC, Coffey C, Sawyer SM, Viner RM, Haller DM, Bose K, et al. Global patterns of mortality in young people: A systematic analysis of population health data. Lancet. 2009;374:881–92. doi: 10.1016/S0140-6736(09)60741-8. [DOI] [PubMed] [Google Scholar]
- 50.Gururaj G, Isaac MK. Epidemiology of suicides in Bangalore. Bangalore: National Institute of Mental Health and Neuro Sciences; 2001. Report No.: Publication No 43. [Google Scholar]
- 51.Vijayakumar L, Rajkumar S. Are risk factors for suicide universal? A case-control study in India. Acta Psychiatr Scand. 1999;99:407–11. doi: 10.1111/j.1600-0447.1999.tb00985.x. [DOI] [PubMed] [Google Scholar]
- 52.Banerjee G, Nandi DN, Nandi S, Sarkar S, Boral GC, Ghosh A. The vulnerability of Indian women to suicide a field-study. Indian J Psychiatry. 1990;32:305–8. [PMC free article] [PubMed] [Google Scholar]
- 53.Nandi DN, Banerjee G, Boral GC, Chowdhury A, Bose J. Is suicide preventable by restricting the availability of lethal agents? A rural survey of West Bengal. Indian J Psychiatry. 1979;21:251–5. [Google Scholar]
- 54.Unni SK, Mani AJ. Suicidal ideators in the psychiatric facility of a general hospital - a psychodemographic profile. Indian J Psychiatry. 1996;38:79–85. [PMC free article] [PubMed] [Google Scholar]
- 55.Vijayakumar L, John S, Pirkis J, Whiteford H. Suicide in developing countries (2): Risk factors. Crisis. 2005;26:112–9. doi: 10.1027/0227-5910.26.3.112. [DOI] [PubMed] [Google Scholar]
- 56.Pillai A, Andrews T, Patel V. Violence, psychological distress and the risk of suicidal behaviour in young people in India. Int J Epidemiol. 2009;38:459–69. doi: 10.1093/ije/dyn166. [DOI] [PubMed] [Google Scholar]
- 57.Crepet P, Caracciolo S, Casoli R, Fabbri D, Florenzano F, Grassi GM, et al. Suicidal behavior in Italy: Data, trends and guidelines for a suicide intervention/prevention policy. Suicide Life Threat Behav. 1991;21:263–78. [PubMed] [Google Scholar]
- 58.Adamek ME, Kaplan MS. The growing use of firearms by suicidal older women, 1979-1992: A research note. Suicide Life Threat Behav. 1996;26:71–8. [PubMed] [Google Scholar]
- 59.Rao AV, Madhavan T. Depression and suicide behaviour in the aged. Indian J Psychiatry. 1983;25:251–9. [PMC free article] [PubMed] [Google Scholar]
- 60.Shukla GD, Verma BL, Mishra DN. Suicide in Jhansi city. Indian J Psychiatry. 1990;32:44–51. [PMC free article] [PubMed] [Google Scholar]
- 61.Rao AV. Suicide in the elderly: A report from India. Crisis. 1991;12:33–9. [PubMed] [Google Scholar]
- 62.Purcell B, Heisel MJ, Speice J, Franus N, Conwell Y, Duberstein PR. Family connectedness moderates the association between living alone and suicide ideation in a clinical sample of adults 50 years and older. Am J Geriatr Psychiatry. 2011 doi: 10.1097/JGP.0b013e31822ccd79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Phillips MR, Yang G, Li S, Li Y. Suicide and the unique prevalence pattern of schizophrenia in mainland China: A retrospective observational study. Lancet. 2004;364:1062–8. doi: 10.1016/S0140-6736(04)17061-X. [DOI] [PubMed] [Google Scholar]
- 64.Desjarlais RE, Good B, Kleinman A. World mental health: Problems and priorities in low-income countries. New York: Oxford University Press; 1995. Suicide. [Google Scholar]
- 65.Lester D. Suicide in an international perspective. Suicide Life Threat Behav. 1997;27:104–11. [PubMed] [Google Scholar]
- 66.Mayer P, Ziaian T. Suicide, gender, and age variations in India. Are women in Indian society protected from suicide? Crisis. 2002;23:98–103. doi: 10.1027//0227-5910.23.3.98. [DOI] [PubMed] [Google Scholar]
- 67.Gururaj G, Isaac MK, Subbakrishna DK, Ranjani R. Risk factors for completed suicides: A case-control study from Bangalore, India. Inj Control Saf Promot. 2004;11:183–91. doi: 10.1080/156609704/233/289706. [DOI] [PubMed] [Google Scholar]
- 68.Kumar V. Poisoning deaths in married women. J Clin Forensic Med. 2004;11:2–5. doi: 10.1016/j.jcfm.2003.10.010. [DOI] [PubMed] [Google Scholar]
- 69.Durkheim E. Le Suicide: Etude de Sociologie. Paris: Presses Universitaires de France; 1897. [Google Scholar]
- 70.Cutright P, Stack S, Fernquist R. Marital status integration, suicide disapproval, and societal integration as explanations of marital status differences in female age-specific suicide rates. Suicide Life Threat Behav. 2007;37:715–24. doi: 10.1521/suli.2007.37.6.715. [DOI] [PubMed] [Google Scholar]
- 71.World Report on Violence and Health. Geneva: WHO; 2002. WHO. [Google Scholar]
- 72.Sudhir Kumar CT, Mohan R, Ranjith G, Chandrasekaran R. Gender differences in medically serious suicide attempts: A study from south India. Psychiatry Res. 2006;144:79–86. doi: 10.1016/j.psychres.2005.11.012. [DOI] [PubMed] [Google Scholar]
- 73.Srivastava AS, Kumar R. Suicidal ideation and attempts in patients with major depression: Sociodemographic and clinical variables. Indian J Psychiatry. 2005;47:225–8. doi: 10.4103/0019-5545.43059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Gunnell D, Magnusson PK, Rasmussen F. Low intelligence test scores in 18 year old men and risk of suicide: Cohort study. BMJ. 2005;330:167. doi: 10.1136/bmj.38310.473565.8F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Martin G, Waite S. Parental bonding and vulnerability to adolescent suicide. Acta Psychiatr Scand. 1994;89:246–54. doi: 10.1111/j.1600-0447.1994.tb01509.x. [DOI] [PubMed] [Google Scholar]
- 76.van Egmond M, Garnefski N, Jonker D, Kerkhof A. The relationship between sexual abuse and female suicidal behavior. Crisis. 1993;14:129–39. [PubMed] [Google Scholar]
- 77.Adityanjee DR. Suicide attempts and suicides in India: Cross-cultural aspects. Int J Soc Psychiatry. 1986;32:64–73. doi: 10.1177/002076408603200208. [DOI] [PubMed] [Google Scholar]
- 78.Gupta RK, Srivastava AK. Study of fatal burns cases in Kanpur (India) Forensic Sci Int. 1988;37:81–9. doi: 10.1016/0379-0738(88)90096-5. [DOI] [PubMed] [Google Scholar]
- 79.Accidental Deaths and Suicides in India. New Delhi: NCRB; 2000. [Google Scholar]
- 80.A Resource for General Physicians. Geneva: WHO; 2000. Preventing Suicide. [Google Scholar]
- 81.Pritchard C. Is there a link between suicide in young men and unemployment? A comparison of the UK with other European Community Countries. Br J Psychiatry. 1992;160:750–6. doi: 10.1192/bjp.160.6.750. [DOI] [PubMed] [Google Scholar]
- 82.Rich AR, Bonner RL. Concurrent validity of a stress-vulnerability model of suicidal ideation and behavior: A follow-up study. Suicide Life Threat Behav. 1987;17:265–70. doi: 10.1111/j.1943-278x.1987.tb00067.x. [DOI] [PubMed] [Google Scholar]
- 83.Mohanty S, Sahu G, Mohanty MK, Patnaik M. Suicide in India: A four year retrospective study. J Forensic Leg Med. 2007;14:185–9. doi: 10.1016/j.jcfm.2006.05.007. [DOI] [PubMed] [Google Scholar]
- 84.Gunnell D, Fernando R, Hewagama M, Priyangika WD, Konradsen F, Eddleston M. The impact of pesticide regulations on suicide in Sri Lanka. Int J Epidemiol. 2007;36:1235–42. doi: 10.1093/ije/dym164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Sato T, Takeichi M, Hara T. Suicide attempts by agricultural chemicals. Indian J Psychiatry. 1993;35:209–10. [PMC free article] [PubMed] [Google Scholar]
- 86.Lotrakul M. Suicide in Thailand during the period 1998-2003. Psychiatry Clin Neurosci. 2006;60:90–5. doi: 10.1111/j.1440-1819.2006.01465.x. [DOI] [PubMed] [Google Scholar]
- 87.Jeyaratnam J. Health problems of pesticide usage in the Third World. Br J Ind Med. 1985;42:505–6. doi: 10.1136/oem.42.8.505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Khan N. Poisoning in a medical unit of Dhaka medical college hospital in 1983. Bangladesh Med J. 1985;14:9–12. [Google Scholar]
- 89.Langley R, Sumner D. Pesticide mortality in the United States 1979-1998. Vet Hum Toxicol. 2002;44:101–5. [PubMed] [Google Scholar]
- 90.Gaillard Y, Krishnamoorthy A, Bevalot F. Cerbera odollam: A ‘suicide tree’ and cause of death in the state of Kerala, India. J Ethnopharmacol. 2004;95:123–6. doi: 10.1016/j.jep.2004.08.004. [DOI] [PubMed] [Google Scholar]
- 91.Kawohl W, Habermeyer E. Plant poisonings - a problem extending the scope of ethnopharmacology. J Ethnopharmacol. 2005;100:138–9. doi: 10.1016/j.jep.2005.06.010. [DOI] [PubMed] [Google Scholar]
- 92.Jang DH, Hoffman RS, Nelson LS. Attempted suicide, by mail order: Abrus precatorius. J Med Toxicol. 2010;6:427–30. doi: 10.1007/s13181-010-0099-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Chugh SN, Dushyant, Ram S, Arora B, Malhotra KC. Incidence & outcome of aluminium phosphide poisoning in a hospital study. Indian J Med Res. 1991;94:232–5. [PubMed] [Google Scholar]
- 94.Bhatia MS, Verma SK, Murty OP. Suicide notes: Psychological and clinical profile. Int J Psychiatry Med. 2006;36:163–70. doi: 10.2190/5690-CMGX-6A1C-Q28H. [DOI] [PubMed] [Google Scholar]
- 95.Bastia BK, Kar N. A psychological autopsy study of suicidal hanging from Cuttack, India: Focus on stressful life situations. Arch Suicide Res. 2009;13:100–4. doi: 10.1080/13811110802572221. [DOI] [PubMed] [Google Scholar]
- 96.Nagendra Gouda M, Rao SM. Factors related to attempted suicide in Davanagere. Indian J Community Med. 2008;33:15–8. doi: 10.4103/0970-0218.39237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Weissman MM. The epidemiology of suicide attempts, 1960 to 1971. Arch Gen Psychiatry. 1974;30:737–46. doi: 10.1001/archpsyc.1974.01760120003001. [DOI] [PubMed] [Google Scholar]
- 98.Singh SP, Santosh PJ, Avasthi A, Kulhara P. A psychosocial study of ‘self-immolation’ in India. Acta Psychiatr Scand. 1998;97:71–5. doi: 10.1111/j.1600-0447.1998.tb09966.x. [DOI] [PubMed] [Google Scholar]
- 99.Venkoba Rao A, Mahendran N, Gopalakrishnan C, Reddy TK, Prabhakar ER, Swaminathnan R, et al. One hundred female burns cases: A study in suicidology. Indian J Psychiatry. 1989;31:43–50. [PMC free article] [PubMed] [Google Scholar]
- 100.Bhargava SC, Sethi S, Vohra AK. Klingsor syndrome: A case report. Indian J Psychiatry. 2001;43:349–50. [PMC free article] [PubMed] [Google Scholar]
- 101.Unni KE, Rotti SB, Chandrasekaran R. An exploratory study of the motivation in suicide attempters. Indian J Psychiatry. 1995;37:169–75. [PMC free article] [PubMed] [Google Scholar]
- 102.Brown M, Barraclough B. Epidemiology of suicide pacts in England and Wales, 1988-92. BMJ. 1997;315:286–7. doi: 10.1136/bmj.315.7103.286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Bardale RV, Dixit PG. Dying together: A report of two-suicide pacts and an overview of the phenomenon. Calicut Med J. 2007;5:e6. [Google Scholar]
- 104.Rao A. Attempted suicide. Indian J Psychiatry. 1965;7:253–64. [Google Scholar]
- 105.Ponnudurai R, Jeyakar J, Saraswathy M. Attempted suicides in Madras. Indian J Psychiatry. 1986;28:59–62. [PMC free article] [PubMed] [Google Scholar]
- 106.Manoranjitham SD, Rajkumar AP, Thangadurai P, Prasad J, Jayakaran R, Jacob KS. Risk factors for suicide in rural south India. Br J Psychiatry. 2010;196:26–30. doi: 10.1192/bjp.bp.108.063347. [DOI] [PubMed] [Google Scholar]
- 107.Jain V, Singh H, Gupta SC, Kumar S. A study of hopelessness, suicidal intent and depession in cases of attempted suicide. Indian J Psychiatry. 1999;41:122–30. [PMC free article] [PubMed] [Google Scholar]
- 108.Chandrasekaran R, Gnanaseelan J, Sahai A, Swaminathan RP, Perme B. Psychiatric and personality disorders in survivors following their first suicide attempt. Indian J Psychiatry. 2003;45:45–8. [PMC free article] [PubMed] [Google Scholar]
- 109.Srivastava S, Kulshreshtha N. Expression of suicidal intent in depressives. Indian J Psychiatry. 2000;42:184–7. [PMC free article] [PubMed] [Google Scholar]
- 110.Gupta SC, Singh H, Trivedi JK. Evaluation of suicidal risk in depressives and schizophrenics: A 2-year follow-up study. Indian J Psychiatry. 1992;34:298–310. [PMC free article] [PubMed] [Google Scholar]
- 111.Kannapiran T, Haroon AE, Vivekanandan S, Arunagiri S. Personality profiles of self-immolators. Indian J Psychiatry. 1997;39:37–40. [PMC free article] [PubMed] [Google Scholar]
- 112.Suk JH, Han CH, Yeon BK. Suicide by burning in Korea. Int J Soc Psychiatry. 1991;37:141–5. doi: 10.1177/002076409103700209. [DOI] [PubMed] [Google Scholar]
- 113.Patel V, Kirkwood BR, Pednekar S, Weiss H, Mabey D. Risk factors for common mental disorders in women.Population-based longitudinal study. Br J Psychiatry. 2006;189:547–55. doi: 10.1192/bjp.bp.106.022558. [DOI] [PubMed] [Google Scholar]
- 114.Rao AV. Suicide attempters in Madurai. J Indian Med Assoc. 1971;57:278–83. [PubMed] [Google Scholar]
- 115.Magni G, Rigatti-Luchini S, Fracca F, Merskey H. Suicidality in chronic abdominal pain: An analysis of the Hispanic Health and Nutrition Examination Survey (HHANES) Pain. 1998;76:137–44. doi: 10.1016/s0304-3959(98)00035-9. [DOI] [PubMed] [Google Scholar]
- 116.Smith MT, Edwards RR, Robinson RC, Dworkin RH. Suicidal ideation, plans, and attempts in chronic pain patients: Factors associated with increased risk. Pain. 2004;111:201–8. doi: 10.1016/j.pain.2004.06.016. [DOI] [PubMed] [Google Scholar]
- 117.Badrinarayana A. Study of suicidal risk factors in depressive illness. Indian J Psychiatry. 1980;22:81–3. [PMC free article] [PubMed] [Google Scholar]
- 118.Black DW, Yates W, Petty F, Noyes R, Jr, Brown K. Suicidal behavior in alcoholic males. Compr Psychiatry. 1986;27:227–33. doi: 10.1016/0010-440x(86)90046-5. [DOI] [PubMed] [Google Scholar]
- 119.Ponnudurai R, Jeyakar J. Suicide in madras. Indian J Psychiatry. 1980;22:203–5. [PMC free article] [PubMed] [Google Scholar]
- 120.Ponnudurai R, Uma TS, Rajarathinam S, Krishnan VS. Determinants of suicidal attempts of wives of substance abusers. Indian J Psychiatry. 2001;43:230–4. [PMC free article] [PubMed] [Google Scholar]
- 121.Beck AT, Steer RA, Kovacs M, Garrison B. Hopelessness and eventual suicide: A 10-year prospective study of patients hospitalized with suicidal ideation. Am J Psychiatry. 1985;142:559–63. doi: 10.1176/ajp.142.5.559. [DOI] [PubMed] [Google Scholar]
- 122.Dyer JA, Kreitman N. Hopelessness, depression and suicidal intent in parasuicide. Br J Psychiatry. 1984;144:127–33. doi: 10.1192/bjp.144.2.127. [DOI] [PubMed] [Google Scholar]
- 123.Shafii M, Carrigan S, Whittinghill JR, Derrick A. Psychological autopsy of completed suicide in children and adolescents. Am J Psychiatry. 1985;142:1061–4. doi: 10.1176/ajp.142.9.1061. [DOI] [PubMed] [Google Scholar]
- 124.Gupta SC, Anand R, Trivedi JK. Development of a suicidal intent questionnaire. Indian J Psychiatry. 1983;25:57–62. [PMC free article] [PubMed] [Google Scholar]
- 125.Hawton K, Fagg J. Suicide, and other causes of death, following attempted suicide. Br J Psychiatry. 1988;152:359–66. doi: 10.1192/bjp.152.3.359. [DOI] [PubMed] [Google Scholar]
- 126.Roy A. Suicide. In: Kaplan HI, editor. Comprehensive Textbook of Psychiatry. Maryland, Baltimore, USA: Williams & Wilkins; 1995. pp. 1739–91. [Google Scholar]
- 127.Ponnudurai R, Patnaik KA, Sathianathan R, Subhan K. A study on the venues of suicide. Indian J Psychiatry. 1997;39:34–6. [PMC free article] [PubMed] [Google Scholar]
- 128.Sathyavathi K, Murthy Rao DL. A study of suicide in Bangalore. Trans All India Institute Mental Health. 1962;3:5–25. [Google Scholar]
- 129.Ganapathi MN, Rao AV. A study of suicide in Madurai. J Indian Med Assoc. 1966;46:18–23. [PubMed] [Google Scholar]
- 130.Latha KS, Bhat SM. Suicidal behaviour among terminally ill cancer patients in India. Indian J Psychiatry. 2005;47:79–83. doi: 10.4103/0019-5545.55950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Mendonsa RD, Appaya P. Psychiatric morbidity in outpatients of gynecological oncology clinic in a tertiary care hospital. Indian J Psychiatry. 2010;52:327–32. doi: 10.4103/0019-5545.74307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Anguiano L, Mayer DK, Piven ML, Rosenstein D. A literature review of suicide in cancer patients. Cancer Nurs. 2012;35:E14–26. doi: 10.1097/NCC.0b013e31822fc76c. [DOI] [PubMed] [Google Scholar]
- 133.Kandasamy A, Chaturvedi SK, Desai G. Spirituality, distress, depression, anxiety, and quality of life in patients with advanced cancer. Indian J Cancer. 2011;48:55–9. doi: 10.4103/0019-509X.75828. [DOI] [PubMed] [Google Scholar]
- 134.Matthews WS, Barabas G. Suicide and epilepsy: A review of the literature. Psychosomatics. 1981;22:515–24. doi: 10.1016/S0033-3182(81)73498-4. [DOI] [PubMed] [Google Scholar]
- 135.Jacob R, Suresh Kumar M, Rajkumar R, Palaniappun V. A study to assess depression, its correlates and suicidal behaviour in epilepsy. Indian J Psychiatry. 2002;44:161–4. [PMC free article] [PubMed] [Google Scholar]
- 136.Hawton K, Fagg J, Simkin S, Harriss L, Malmberg A. Methods used for suicide by farmers in England and Wales.The contribution of availability and its relevance to prevention. Br J Psychiatry. 1998;173:320–4. doi: 10.1192/bjp.173.4.320. [DOI] [PubMed] [Google Scholar]
- 137.Sainath P. The largest wave of suicides in history. Counterpunch. 2009 http://www.counterpunch.org/2009/02/12/the-largest-wave-of-suicides-in-history/ [Google Scholar]
- 138.Ernst C, Mechawar N, Turecki G. Suicide neurobiology. Prog Neurobiol. 2009;89:315–33. doi: 10.1016/j.pneurobio.2009.09.001. [DOI] [PubMed] [Google Scholar]
- 139.Palaniappan V, Ramachandran V, Somasundaram O. Suicidal ideation and biogenic amines in depression. Indian J Psychiatry. 1983;25:286–92. [PMC free article] [PubMed] [Google Scholar]
- 140.Trivedi JK. Serotonin and its metabolites as biological markers of suicidal behaviour. Indian J Psychiatry. 1992;34:174–97. [PMC free article] [PubMed] [Google Scholar]
- 141.Trivedi JK, Pandey S, Dalal PK, Dubey MP, Sinha PK. Csf 5 - hiaa in violent and non-violent suicide attempters. Indian J Psychiatry. 1997;39:41–8. [PMC free article] [PubMed] [Google Scholar]
- 142.Rao AV, Devi PS, Reddy KT. Depression, cognitive disorder and melatonin profile. Ann Natl Acad Med Sci. 1988;25:41–9. [Google Scholar]
- 143.Muldoon MF, Manuck SB, Matthews KA. Lowering cholesterol concentrations and mortality: A quantitative review of primary prevention trials. BMJ. 1990;301:309–14. doi: 10.1136/bmj.301.6747.309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Verma S, Trivedi JK, Singh H, Dalal PK, Asthana OP, Srivastava JS, et al. Serum lipid profile in suicide attempters. Indian J Psychiatry. 1999;41:300–6. [PMC free article] [PubMed] [Google Scholar]
- 145.Yip PS. Charcoal-burning suicides and strategies for prevention. Crisis. 2007;28:21–7. doi: 10.1027/0227-5910.28.S1.21. [DOI] [PubMed] [Google Scholar]
- 146.Lee WJ, Cha ES, Park ES, Kong KA, Yi JH, Son M. Deaths from pesticide poisoning in South Korea: Trends over 10 years. Int Arch Occup Environ Health. 2009;82:365–71. doi: 10.1007/s00420-008-0343-z. [DOI] [PubMed] [Google Scholar]
- 147.Saravanapavananthan N, Ganeshamoorthy J. Yellow oleander poisoning--a study of 170 cases. Forensic Sci Int. 1988;36:247–50. doi: 10.1016/0379-0738(88)90150-8. [DOI] [PubMed] [Google Scholar]
- 148.Etzersdorfer E, Sonneck G. Preventing suicide by influencing mass media reporting: The Viennese experience 1980-1996. Arch Suicide Res. 1998;4:64–74. [Google Scholar]
- 149.Niederkrotenthaler T, Sonneck G. Assessing the impact of media guidelines for reporting on suicides in Austria: Interrupted time series analysis. Aust N Z J Psychiatry. 2007;41:419–28. doi: 10.1080/00048670701266680. [DOI] [PubMed] [Google Scholar]
- 150.Niederkrotenthaler T, Voracek M, Herberth A, Till B, Strauss M, Etzersdorfer E, et al. Media and suicide. Papageno v Werther effect. BMJ. 2010;341:c5841. doi: 10.1136/bmj.c5841. [DOI] [PubMed] [Google Scholar]
- 151.Ramadas S, Kuttichira P. The development of a guideline and its impact on the media reporting of suicide. Indian J Psychiatry. 2011;53:224–8. doi: 10.4103/0019-5545.86812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Muller-Oerlinghausen B, Muser-Causemann B, Volk J. Suicides and parasuicides in a high-risk patient group on and off lithium long-term medication. J Affect Disord. 1992;25:261–9. doi: 10.1016/0165-0327(92)90084-j. [DOI] [PubMed] [Google Scholar]
- 153.Greil W, Ludwig-Mayerhofer W, Erazo N, Schochlin C, Schmidt S, Engel RR, et al. Lithium versus carbamazepine in the maintenance treatment of bipolar disorders--a randomised study. J Affect Disord. 1997;43:151–61. doi: 10.1016/s0165-0327(96)01427-9. [DOI] [PubMed] [Google Scholar]
- 154.Rao AV, Hariharasubramanian N, Devi SP, Sugumar A, Srinivasan V. Lithium prophylaxis in affective disorder. Indian J Psychiatry. 1982;24:22–30. [PMC free article] [PubMed] [Google Scholar]
- 155.Meltzer HY, Okayli G. Reduction of suicidality during clozapine treatment of neuroleptic-resistant schizophrenia: Impact on risk-benefit assessment. Am J Psychiatry. 1995;152:183–90. doi: 10.1176/ajp.152.2.183. [DOI] [PubMed] [Google Scholar]
- 156.Walker AM, Lanza LL, Arellano F, Rothman KJ. Mortality in current and former users of clozapine. Epidemiology. 1997;8:671–7. doi: 10.1097/00001648-199710000-00010. [DOI] [PubMed] [Google Scholar]
- 157.Munro J, O’Sullivan D, Andrews C, Arana A, Mortimer A, Kerwin R. Active monitoring of 12,760 clozapine recipients in the UK and Ireland.Beyond pharmacovigilance. Br J Psychiatry. 1999;175:576–80. doi: 10.1192/bjp.175.6.576. [DOI] [PubMed] [Google Scholar]
- 158.Tran PV, Hamilton SH, Kuntz AJ, Potvin JH, Andersen SW, Beasley C, Jr, et al. Double-blind comparison of olanzapine versus risperidone in the treatment of schizophrenia and other psychotic disorders. J Clin Psychopharmacol. 1997;17:407–18. doi: 10.1097/00004714-199710000-00010. [DOI] [PubMed] [Google Scholar]
- 159.Binks CA, Fenton M, McCarthy L, Lee T, Adams CE, Duggan C. Pharmacological interventions for people with borderline personality disorder. Cochrane Database Syst Rev. 2006;25 doi: 10.1002/14651858.CD005653. CD005653. [DOI] [PubMed] [Google Scholar]
- 160.Linehan MM, Comtois KA, Murray AM, Brown MZ, Gallop RJ, Heard HL, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. 2006;63:757–66. doi: 10.1001/archpsyc.63.7.757. [DOI] [PubMed] [Google Scholar]
- 161.Vijayakumar L, Umamaheswari C, Shujaath Ali ZS, Devaraj P, Kesavan K. Intervention for suicide attempters: A randomized controlled study. Indian J Psychiatry. 2011;53:244–8. doi: 10.4103/0019-5545.86817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Houston K, Haw C, Townsend E, Hawton K. General practitioner contacts with patients before and after deliberate self harm. Br J Gen Pract. 2003;53:365–70. [PMC free article] [PubMed] [Google Scholar]
- 163.Rutz W, von Knorring L, Walinder J. Frequency of suicide on Gotland after systematic postgraduate education of general practitioners. Acta Psychiatr Scand. 1989;80:151–4. doi: 10.1111/j.1600-0447.1989.tb01318.x. [DOI] [PubMed] [Google Scholar]
- 164.Derasari S, Shah VD. Comparison of symptomatology of depression between India and U.S.A. Indian J Psychiatry. 1998;30:129–34. [PMC free article] [PubMed] [Google Scholar]
- 165.Sharma BR, Gupta M, Sharma AK, Sharma S, Gupta N, Relhan N, et al. Suicides in northern India: Comparison of trends and review of literature. J Forensic Leg Med. 2007;14:318–26. doi: 10.1016/j.jcfm.2006.08.009. [DOI] [PubMed] [Google Scholar]
- 166.Manoranjitham S, Abraham A, Jacob KS. Towards a national policy to reduce suicide in India. Natl Med J India. 2005;18:118–22. [PubMed] [Google Scholar]
- 167.Nordentoft M. Prevention of suicide and attempted suicide in Denmark.Epidemiological studies of suicide and intervention studies in selected risk groups. Dan Med Bull. 2007;54:306–69. [PubMed] [Google Scholar]
- 168.Isaac M, Elias B, Katz LY, Belik SL, Deane FP, Enns MW, et al. Gatekeeper training as a preventative intervention for suicide: A systematic review. Can J Psychiatry. 2009;54:260–8. doi: 10.1177/070674370905400407. [DOI] [PubMed] [Google Scholar]
- 169.Soomro GM. Deliberate self-harm (and attempted suicide) Clin Evid (Online) 2008;2008 [PMC free article] [PubMed] [Google Scholar]
- 170.Vijayakumar L. Suicide prevention: The urgent need in developing countries. World Psychiatry. 2004;3:158–9. [PMC free article] [PubMed] [Google Scholar]
- 171.Vijayakumar L, Satheesh-Babu R. Does ‘no pesticide’ reduce suicides? Int J Soc Psychiatry. 2009;55:401–6. doi: 10.1177/0020764008095340. [DOI] [PubMed] [Google Scholar]