

Abstract
Capsule endoscopy (CE) is considered as a noninvasive and reliable diagnostic tool of examining the entire small bowel. CE has been performed frequently at many medical centers in South Korea; however, there is no evidence-based CE guideline for adequate diagnostic approaches. To provide accurate information and suggest correct testing approaches for small bowel disease, the guideline on CE was developed by the Korean Gut Image Study Group, a part of the Korean Society of Gastrointestinal Endoscopy. Operation teams for developing the guideline were organized into four areas: obscure gastrointestinal bleeding, small bowel preparation, Crohn's disease, and small bowel tumor. A total of 20 key questions were selected. In preparing this guideline, MEDLINE, Cochrane library, KMbase, KISS, and KoreaMed literature searches were performed. After writing a draft of the guideline, opinions from various experts were reflected before approving the final document. The guideline should be regarded as recommendations only to gastroenterologists in providing care to their patients. These are not absolute rules and should not be construed as establishing a legal standard of care. Although further revision may be necessary as new data appear, this guideline is expected to play a role for adequate diagnostic approaches of various small bowel diseases.
Keywords: Capsule endoscopy, Small bowel disease, Guideline
INTRODUCTION
The necessity
During the past decade since capsule endoscopy (CE) was introduced to the clinical environment at the outset of the 21st century, there have been numerous studies confirming that CE provides a noninvasive and highly reliable diagnostic means of examining the entire small intestinal mucosa. Accordingly, organized literature reviews and guidelines have been published primarily in America and Europe. Although CE was first introduced in Korea 8 years ago, there has yet to be an evidence-based CE guideline suitable for the country's circumstances. A proper CE guideline is expected to enhance efficient utilization of limited medical resources under the current situation in Korea, propose adequate diagnostic approaches for patients with various small intestinal diseases and substantially reduce the socioeconomic loss caused by excessive medical testing.
The objective
This guideline was prepared according to the circumstances surrounding the Korean medical industry by systematically reviewing literature published in Korea and abroad, and by compiling the opinions of CE experts in Korea regarding 20 key questions in clinicians' diagnoses of diseases in the small intestine. The objectives of this guideline are to provide accurate information and suggest correct testing approaches to the medical professionals providing care to patients with diseases of the small intestine. The guideline should also offer helpful information to patients diagnosed with such diseases.
The participants and development process of the CE guideline
The participants
To prepare this guideline, a multisociety CE guideline operation committee and a working committee were formed in April 2010 consisting of experts and clinical treatment guideline professionals recommended by The Korean Society of Gastroenterology, The Korean Society of Gastrointestinal Endoscopy, and Korean Association for the Study of Intestinal Diseases. Operation teams for developing the guideline were organized into four areas: obscure gastrointestinal bleeding (OGIB), small bowel preparation, Crohn's disease, and tumors in the small intestine. There was no conflict of interest among the participants in the development process of the guideline.
Choice of key questions
Since the guideline cannot address all of the questions related to CE, a survey was conducted based on a working committee meeting to select 20 key questions concerning diagnostic and testing procedures that are regarded as pivotal to medical professionals.
Literature search and selection
We performed online searches for CE-related clinical studies, comparative research, randomized controlled trials, meta-analyses, and guidelines published from January 2001 to August 2011. Searches were performed using MEDLINE and Cochrane library for foreign literature and KMbase, KISS, and KoreaMed for Korean literature to identify published research on CE. This initially produced a total of 3,271 article titles and abstracts. Of these, 2,525 articles that are unrelated to OGIB were excluded and then 705 articles falling under the exclusion criteria (unsuitable study population, other small bowel disease, abstracts only, case reports, comment/editorial/letter, and study in any language other than English) were also excluded. Finally, a total of 41 articles were selected. Materials relating to 10 key questions were extracted after a full review of the 41 articles. The 'PICO' rule was applied to the keywords used for searches in English. Among the initially selected publications, we reviewed the titles and abstracts to eliminate those that did not meet the criteria. When necessary, we carefully reviewed entire documents and created a standardized evidence table to extract information pertinent to the key questions. After creating an evidence table for each key question, we conducted meta-analyses for key questions with search results containing randomized controlled trials. We carefully reviewed the final candidate literature and wrote a recommendation based on comprehensive evidence, including the results of the meta-analyses. The meta-analyses were performed using the Stata 10.0 software (StataCorp, College Station, Texas, US).
Quality of evidence and grade of a recommendation
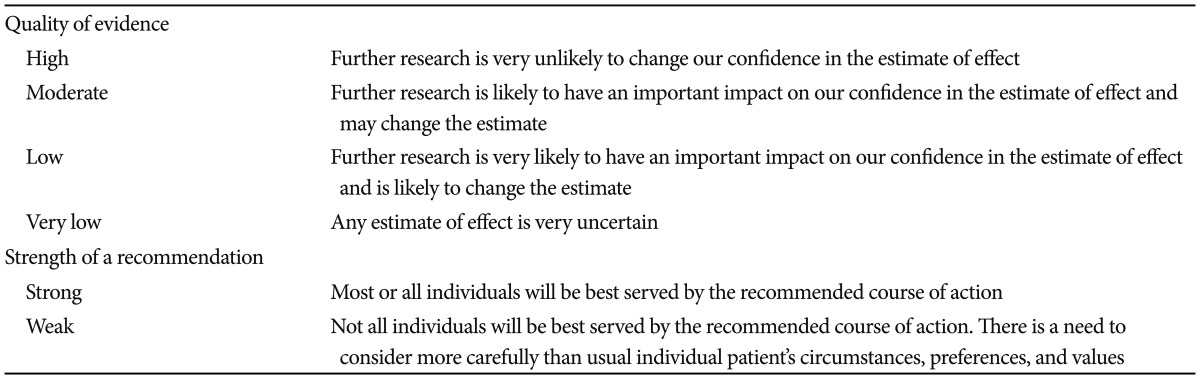
The methodology proposed by the Grading of Recommendations Assessment, Development and Evaluation Working Group was used to determine the quality of evidence, which indicated the level of scientific evidence of the recommendation, and the strength of recommendation, which indicates the level of strength at which the recommendation should be made (Table 1).1,2
Table 1.
Quality of Evidence and Strength of a Recommendation
Draft making of statements and approval
After writing a draft of the CE guideline based on the search results of Korean and foreign literature, we conducted an internet survey to reflect the medical environment in Korea and to assess how CE was being provided by medical professionals in actual clinical settings. Opinions from various professionals in Korea were drawn and compiled before having the draft recommendation approved.
Supply and implementation of the CE guideline
The published guideline will be posted on the websites of the Korean Society of Gastroenterology, the Korean Society of Gastrointestinal Endoscopy, and Korean Association for the Study of Intestinal Diseases. A summary of the guideline highlighting important recommendations will be prepared and distributed to medical professionals free of charge.
SUBJECTS
Is CE effective as an initial diagnostic method for evaluating patients with OGIB?
CE is an effective initial diagnostic method for evaluating patients with OGIB (evidence grade, moderate; recommendation grade, strong).
For evaluating patients with OGIB, diverse diagnostic modalities are used including CE, small bowel barium radiography, enteroclysis, computed tomography angiography (CTA), computed tomography enteroclysis (CTEC), push enteroscopy (PE), and double balloon enteroscopy (DBE).
In general, to be used as an initial diagnosing method, a modality should have superior diagnostic yield compared to other available examinations and it should be safe, noninvasive and easy to perform.
In a meta-analysis using 14 prospective studies including 396 patients with OGIB, CE was superior to PE and small bowel barium radiography for diagnosing clinically significant small bowel pathology. In this study, CE also showed superior or at least had comparable diagnostic yield compared to CTEC, angiography, and small bowel magnetic resonance imaging.3 Currently, diagnostic yield of CE in patients with OGIB ranges from 50% to 60%.3-5
Many diagnostic modalities for small bowel evaluation such as enteroclysis and DBE require considerable time and are usually accompanied by patient discomfort, which may result in low compliance for the examinations. In contrast to these modalities, CE is safe and noninvasive method that is easy to perform and consequently shows high compliance.
Is CE required for evaluating patients with iron deficiency anemia (IDA) if no bleeding focus can be found outside the gastrointestinal tract?
CE is an effective initial diagnostic method for evaluating patients with IDA if no bleeding focus can be found outside the gastrointestinal tract (evidence grade, moderate; recommendation grade, strong).
IDA occurs in 2% to 5% of adult men and postmenopausal women. The causes of IDA are different according to age and gender.6 While menstrual blood loss is the most common cause of IDA in premenopausal women, blood loss from the gastrointestinal tract is the most common cause in adult men and postmenopausal women. In addition, intravascular hemolysis, iron malabsorption, and urological and gynecological disorders such as renal cell carcinoma and uterine myoma also can cause IDA.7 Therefore, for premenopausal women with IDA, gynecological examination is initially required. For adult men and postmenopausal women, esophagogastroduodenoscopy and colonoscopy should be performed unless another specific disease is suspected in history taking and basic laboratory tests including urine testing for blood.
If no specific bleeding focus is found in esophagogastroduodenoscopy and colonoscopy, and bleeding is not overt, observation with iron supplementation without further imaging of the small bowel can be a reasonable option.7 However, in case of overt bleeding or inadequate response to iron therapy, CE, a primary diagnosing method for OGIB, may be helpful to detect a bleeding focus.8
Is CE more effective than small bowel barium radiography in determining the cause of OGIB?
CE has higher diagnostic yield than small bowel barium radiography in patients with OGIB (evidence grade, moderate; recommendation grade, strong).
To date, there has been no prospective randomized study comparing CE and small bowel barium radiography. Only one prospective study and one retrospective study are currently available. In the prospective study including 13 patients with OGIB, diagnostic yield of CE and small bowel barium radiography were 30.8% and 7.7%, respectively (p<0.05).9 In the retrospective study including 40 patients with OGIB, CE also showed superior diagnostic yield compared to small bowel barium radiography (47.5% vs. 2.5%, p<0.001).10
In conclusion, when compared with small bowel barium radiography, CE has higher diagnostic yield in patients with OGIB.
Is CE more effective than enteroclysis in determining the cause of OGIB?
CE is more effective than enteroclysis in determining the cause in patient with OGIB (evidence grade, moderate; recommendation grade, strong).
No randomized controlled trials have been conducted to determine whether CE has a higher diagnostic yield compared to enteroclysis in patients with OGIB. To date, only one prospective11 and one retrospective study12 have been published on this topic. The prospective study compared the diagnostic yield of CE with that of enteroclysis in 51 patients with IDA; upper and lower endoscopic findings were negative and other forms of anemia were excluded. The likely causes of IDA were identified by CE in 29/51 patients (57%), whereas enteroclysis revealed the likely cause of IDA in only 6/51 patients (11.8%, p<0.0001).11
In the retrospective study that compared CE with enteroclysis, 23 patients with OGIB were selected from a sample of 64 patients with small bowel disease. The diagnostic yield of CE was higher (14/23 patients, 60.8%) than that of enteroclysis (9/23 patients, 39%).12
In conclusion, CE is considered more effective than enteroclysis in determining the cause in patient with OGIB.
Is CE more effective than CTA in determining the cause in patients with OGIB?
CE could be more helpful than CTA in determining the cause in patients with OGIB (evidence grade, low; recommendation grade, weak).
No randomized controlled trials have compared the use of CE with that of CTA in patients with OGIB, but a prospective study13 has been published. The prospective study of 25 patients with OGIB found that the source of bleeding could be detected in significantly more patients with CE (18/25, 72%; 95% confidence interval [CI], 50.6% to 87.9%) than with CTA (four-channel multidetector computed tomography [MDCT]; 6/25, 24%; 95% CI, 9.4% to 45.1%; p=0.005).13 Moreover, lesions with negative CTA findings were detected by CE (63% [12/19] of patients). Consequently, CE was a more useful tool than CTA, as CE impacted the therapeutic plan in 9/19 patients (47%) with only positive CE finding.13
In conclusion, CE could be more helpful than CTA for determining the cause in patients with OGIB.
Is CE more effective than computed tomography enterography (CTE)/CTEC in determining the cause in patients with OGIB?
CTE/CTEC as a complementary examination to CE could be helpful in determining the cause in patients with OGIB (evidence grade, low; recommendation grade, weak).
To date, four prospective studies14-17 and three retrospective studies10,12,18 have compared the effectiveness of CE with CTE/CTEC in the diagnosis of patients with OGIB. The results of these studies, however, have been inconsistent. To our knowledge, no randomized controlled trials have examined this topic.
In a recent study of 123 patients with overt OGIB, the diagnostic yield of CE was significantly greater than that of CTE (16-channel MDCT; 57.7% vs. 30%; p=0.01).14 The diagnostic yield of CE was also greater (40/49 patients, 81.6%) than that of CTE (33/49 patients, 67.4%) in 49 patients with surgically confirmed diagnoses, but this difference was not significant (p>0.05).14 In a retrospective study of 52 patients who underwent CE for various reasons, OGIB (43/52, 82.6%) was the most common cause.10 Among these 52 patients, 19 underwent CTE (four-channel MDCT), and the diagnostic yield of CE was significantly greater than that of CTE (63% vs. 21%; p=0.02).10
In another prospective study of 58 patients with OGIB (occult, 25 patients [43%]; overt, 33 patients [57%]), a small bowel bleeding source was identified with reference standard (surgery or DBE) in 28% of the patients (16/58).17 The diagnostic yield for CTE (64 or 128-channel MDCT) was significantly greater than that of CE (88% [14/16 patients] vs. 38% [6/16 patients], respectively; p=0.008).17 The results, however, had been contradictory to those of other studies. Nine of 16 patients (56%) in this study were confirmed to have a small bowel tumor, thereby increasing the diagnostic yield of CTE (9/9, 100%) in comparison with that of CE (3/9, 33%).
A retrospective study investigated the sensitivity and specificity of CE and CTEC (64-channel MDCT) to detect lesions in 32 patients with OGIB.18 The reported sensitivities were 87% for CE and 69% for CTEC, and specificities were 81% for CE and 100% for CTEC.18 Moreover, the overall accuracy was 84% for both CE and CTEC. In a prospective study that included 22 patients with suspected small bowel disease (8/22 with OGIB), the diagnostic yields of CE (4/8 patients, 50%) and CTEC (1/8 patients, 12.5%) did not differ significantly (p=0.1).15
In contrast, a retrospective study of 16 patients with OGIB who underwent both CTEC and CE reported a higher diagnostic yield for CE (5/16 patients, 31.3%) than for CTEC (3/16 patients, 18.6%).12 The most recent prospective study included 45 patients with unexplained IDA and it also reported a higher diagnostic yield with CE compared to with CTEC (four-channel MDCT; 77.8% [35/45] vs. 22.2% [10/45], respectively; p=0.01).16 Specifically, CE achieved a better diagnostic yield than CTEC when lesions were limited to the mucosa (i.e., arteriovenous malformation, 100% vs. 0%; small bowel Crohn's disease, 88% vs. 50%, respectively).
In conclusion, although the diagnostic yields of CE and CTE/CTEC depend on the causes of small bowel bleeding, CTE/CTEC as a complementary examination to CE could be helpful in determining the cause of OGIB in patients.
Is CE more effective than PE in OGIB?
CE has a higher diagnostic yield than PE in patients with OGIB (evidence grade, low; recommendation grade, strong).
PE used for evaluation of OGIB has the disadvantage of difficulty in shortening the bowel, permitting examination of only 60 to 120 cm from the ligament of Treitz. Prospective studies comparing CE with PE in patients with OGIB who had undergone both studies have consistently revealed a superior diagnostic yield in the CE group (70%) than in the PE group (19% to 25%).19,20 However, these cross-sectional studies have several limitations, such as the absence of a gold standard modality and subjective criteria for positive findings of CE.
A 1 year follow-up study using a clinical outcome after the follow-up period as a gold standard also showed higher diagnostic yields and sensitivity in the CE group versus the PE group, but similar results in positive and negative predictive values, and lower specificity in the CE group were noted (48% compared to 80%).21 Another randomized controlled follow-up study involving a total of 78 patients with OGIB reported a higher diagnostic yield and sensitivity in the CE group, but there specificity as well as positive and negative predictive values were similar. This study also showed that a lower proportion of patients needed additional diagnostic and therapeutic exploration in the group using CE as the first exploration modality.22
In conclusion, when compared with PE, CE has a higher diagnostic yield and also decreases requirements for additional exploration in patients with OGIB, so it should be considered prior to PE.
Is it beneficial to perform CE as soon as possible in OGIB?
Performing CE as soon as possible in OGIB is effective in improving the diagnostic yield (evidence grade, moderate; recommendation grade, strong).
It is widely assumed that the type of OGIB and timing of a study in the course of OGIB are important factors affecting the diagnostic yield of CE. However, there is lack of prospective studies focusing on the relation between diagnostic yield and the type of OGIB as well as the timing of CE as a primary end point.
Retrospective studies aiming to determine the clinical outcomes of patients with OGIB who underwent CE and prospective studies comparing the diagnostic yield between CE and intraoperative endoscopy in OGIB consistently showed that diagnostic yield of CE was higher in the overt OGIB group that in the occult OGIB group.23-25 In addition, those studies showed a time dependent relationship; in other words, shorter intervals between the timing of CE and the last bleeding episode increased the diagnostic yield.23,24 One consideration in this topic is whether the presence of blood without definite bleeding focus should be regarded as a positive finding. When excluding the presence of blood as a positive finding, the time dependent relationship disappeared in one study.24 Considering the development of deep enteroscopy such as balloon assisted enteroscopy,26 the presence of blood at CE could provide useful information on the management strategy of OGIB such as the site and amount of bleeding, and this should be considered as a significant finding.
In conclusion, diagnostic yield of CE is higher in patients with overt OGIB than in those with OGIB and a shorter time interval between examination and the last bleeding episode also increases the diagnostic yield.
Is CE better than DBE for the diagnosis of patients with OGIB?
CE and DBE provide similar diagnostic yields in patients with OGIB (evidence grade, low; recommendation grade, strong).
The development of CE and DBE has revolutionized the diagnostic and therapeutic approaches for OGIB.5,27 Two meta-analyses comparing CE and DBE have previously been published, both finding similar results with respect to overall diagnostic yields between the two modalities.28,29 However, these analyses relied on a small number of observational studies; additionally, the relative yields of CE and DBE were compared for the investigation of small bowel diseases, and were not specifically restricted to patients with OGIB. There has been no randomized controlled trial comparing the efficacy of CE and DBE in OGIB, but there are six prospective and three retrospective studies on the diagnostic yields of CE and DBE specifically in OGIB.30-38 We have performed a meta-analysis using those nine studies to compare the diagnostic yields of CE and DBE in OGIB. The meta-analysis comparing the successful localization of the bleeding source in each study revealed that the pooled odds ratio for the diagnostic yield with CE compared to with DBE was 1.48 (95% CI, 0.90 to 2.43; p=0.16) (Fig. 1).
Fig. 1.

Diagnostic yield of capsule endoscopy (CE) compared with double balloon enteroscopy (DBE) in obscure gastrointestinal bleeding. CI, confidence interval.
In summary, the results from this meta-analysis demonstrate that CE and DBE have similar diagnostic yields for the evaluation of OGIB.
Is it better to perform CE prior to DBE for the diagnosis of patients with OGIB?
It is recommended to perform CE prior to DBE for the diagnosis of patients with OGIB (evidence grade, low; recommendation grade, strong).
Although two economic analyses have found that initial DBE is a more cost-effective strategy,39,40 the prevailing opinion is that patients should be investigated first by CE.41 In Korea, CE is less expensive to DBE and CE directed DBE is cost-effective. There has been no randomized controlled trial to help this decision on which is the best way between the two modalities to evaluate the source of bleeding in patients with OGIB, but five prospective and two retrospective studies have been published in this regard.30-33,35,36,38 We performed a meta-analysis using these seven studies and the odds ratio for the yield of DBE performed after a previously positive CE was 1.79 (95% CI, 1.09 to 2.96; p=0.02) compared with that of DBE performed in all patients (Fig. 2). A limitation of the analysis is that, in most studies, CE was performed prior to DBE and the endoscopist performing DBE was not blinded to the CE results. Since the diagnostic yield of DBE increased significantly when performed after a positive CE, having the results from CE available may have created a detection bias in the yield of DBE. Nevertheless, the results from this analysis reveals that the diagnostic algorithm for OGIB might begin with CE in most cases, in particular because of the relatively noninvasive nature of CE in comparison to enteroscopy and because the yield of DBE is significantly enhanced when guided by a previously positive capsule study.
Fig. 2.

Increased diagnostic yield of double balloon enteroscopy (DBE) performed after positive capsule endoscopy (CE) in obscure gastrointestinal bleeding. CI, confidence interval.
In summary, it is recommended to perform CE prior to DBE in the diagnosis of patients with OGIB.
CONCLUSIONS
CE is an effective initial diagnostic method for evaluating patients with OGIB (evidence grade, moderate; recommendation grade, strong).
CE is an effective initial diagnostic method for evaluating patients with IDA if no bleeding focus can be found outside the gastrointestinal tract (evidence grade, moderate; recommendation grade, strong).
CE has higher diagnostic yield than small bowel barium radiography in patients with OGIB (evidence grade, moderate; recommendation grade, strong).
CE is more effective than enteroclysis in determining the cause in patient with OGIB (evidence grade, moderate; recommendation grade, strong).
CE could be more helpful than CTA in determining the cause in patient with OGIB (evidence grade, low; recommendation grade, weak).
CTE/CTEC as a complementary examination to CE could be helpful in determining the cause in patient with OGIB (evidence grade, low; recommendation grade, weak).
CE has higher diagnostic yield than PE in patients with OGIB (evidence grade, low; recommendation grade, strong).
Performing CE as soon as possible in OGIB is effective in improving the diagnostic yield (evidence grade, moderate; recommendation grade, strong).
CE and DBE provide similar diagnostic yields in patients with OGIB (evidence grade, low; recommendation grade, strong).
It is recommended to perform CE prior to DBE for the diagnosis of patients with OGIB (evidence grade, low; recommendation grade, strong).
The current proposed approach to the diagnosis of OGIB is summarized in the Appendix 1. However, if better testing methods are developed or the overall cost changes, this recommendation can be changed.
Appendix
Appendix 1

Proposed approach to diagnosis and management of obscure gastrointestinal bleeding. Dashed arrows indicate less-preferred options. GI, gastrointestinal; EGD, esophagogastroduodenoscopy; CE, capsule endoscopy; CTE, computed tomography enterography; DE, deep enteroscopy; PE, push enteroscopy; SB, small bowel; IOE, intraoperative enteroscopy.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–926. doi: 10.1136/bmj.39489.470347.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Atkins D, Best D, Briss PA, et al. Grading quality of evidence and strength of recommendations. BMJ. 2004;328:1490. doi: 10.1136/bmj.328.7454.1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Triester SL, Leighton JA, Leontiadis GI, et al. A meta-analysis of the yield of capsule endoscopy compared to other diagnostic modalities in patients with obscure gastrointestinal bleeding. Am J Gastroenterol. 2005;100:2407–2418. doi: 10.1111/j.1572-0241.2005.00274.x. [DOI] [PubMed] [Google Scholar]
- 4.ASGE Standards of Practice Committee. Fisher L, Lee Krinsky M, et al. The role of endoscopy in the management of obscure GI bleeding. Gastrointest Endosc. 2010;72:471–479. doi: 10.1016/j.gie.2010.04.032. [DOI] [PubMed] [Google Scholar]
- 5.Raju GS, Gerson L, Das A, Lewis B American Gastroenterological Association. American Gastroenterological Association (AGA) Institute technical review on obscure gastrointestinal bleeding. Gastroenterology. 2007;133:1697–1717. doi: 10.1053/j.gastro.2007.06.007. [DOI] [PubMed] [Google Scholar]
- 6.Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG, Woodman RC. Prevalence of anemia in persons 65 years and older in the United States: evidence for a high rate of unexplained anemia. Blood. 2004;104:2263–2268. doi: 10.1182/blood-2004-05-1812. [DOI] [PubMed] [Google Scholar]
- 7.Goddard AF, James MW, McIntyre AS, Scott BB British Society of Gastroenterology. Guidelines for the management of iron deficiency anaemia. Gut. 2011;60:1309–1316. doi: 10.1136/gut.2010.228874. [DOI] [PubMed] [Google Scholar]
- 8.Fireman Z, Kopelman Y. The role of video capsule endoscopy in the evaluation of iron deficiency anaemia. Dig Liver Dis. 2004;36:97–102. doi: 10.1016/j.dld.2003.10.009. [DOI] [PubMed] [Google Scholar]
- 9.Costamagna G, Shah SK, Riccioni ME, et al. A prospective trial comparing small bowel radiographs and video capsule endoscopy for suspected small bowel disease. Gastroenterology. 2002;123:999–1005. doi: 10.1053/gast.2002.35988. [DOI] [PubMed] [Google Scholar]
- 10.Hara AK, Leighton JA, Sharma VK, Fleischer DE. Small bowel: preliminary comparison of capsule endoscopy with barium study and CT. Radiology. 2004;230:260–265. doi: 10.1148/radiol.2301021535. [DOI] [PubMed] [Google Scholar]
- 11.Apostolopoulos P, Liatsos C, Gralnek IM, et al. The role of wireless capsule endoscopy in investigating unexplained iron deficiency anemia after negative endoscopic evaluation of the upper and lower gastrointestinal tract. Endoscopy. 2006;38:1127–1132. doi: 10.1055/s-2006-944736. [DOI] [PubMed] [Google Scholar]
- 12.Rajesh A, Sandrasegaran K, Jennings SG, et al. Comparison of capsule endoscopy with enteroclysis in the investigation of small bowel disease. Abdom Imaging. 2009;34:459–466. doi: 10.1007/s00261-008-9427-1. [DOI] [PubMed] [Google Scholar]
- 13.Saperas E, Dot J, Videla S, et al. Capsule endoscopy versus computed tomographic or standard angiography for the diagnosis of obscure gastrointestinal bleeding. Am J Gastroenterol. 2007;102:731–737. doi: 10.1111/j.1572-0241.2007.01058.x. [DOI] [PubMed] [Google Scholar]
- 14.Zhang BL, Jiang LL, Chen CX, Zhong BS, Li YM. Diagnosis of obscure gastrointestinal hemorrhage with capsule endoscopy in combination with multiple-detector computed tomography. J Gastroenterol Hepatol. 2010;25:75–79. doi: 10.1111/j.1440-1746.2009.06016.x. [DOI] [PubMed] [Google Scholar]
- 15.Voderholzer WA, Ortner M, Rogalla P, Beinhölzl J, Lochs H. Diagnostic yield of wireless capsule enteroscopy in comparison with computed tomography enteroclysis. Endoscopy. 2003;35:1009–1014. doi: 10.1055/s-2003-44583. [DOI] [PubMed] [Google Scholar]
- 16.Milano A, Balatsinou C, Filippone A, et al. A prospective evaluation of iron deficiency anemia in the GI endoscopy setting: role of standard endoscopy, videocapsule endoscopy, and CT-enteroclysis. Gastrointest Endosc. 2011;73:1002–1008. doi: 10.1016/j.gie.2011.01.006. [DOI] [PubMed] [Google Scholar]
- 17.Huprich JE, Fletcher JG, Fidler JL, et al. Prospective blinded comparison of wireless capsule endoscopy and multiphase CT enterography in obscure gastrointestinal bleeding. Radiology. 2011;260:744–751. doi: 10.1148/radiol.11110143. [DOI] [PubMed] [Google Scholar]
- 18.Khalife S, Soyer P, Alatawi A, et al. Obscure gastrointestinal bleeding: preliminary comparison of 64-section CT enteroclysis with video capsule endoscopy. Eur Radiol. 2011;21:79–86. doi: 10.1007/s00330-010-1896-2. [DOI] [PubMed] [Google Scholar]
- 19.Mata A, Bordas JM, Feu F, et al. Wireless capsule endoscopy in patients with obscure gastrointestinal bleeding: a comparative study with push enteroscopy. Aliment Pharmacol Ther. 2004;20:189–194. doi: 10.1111/j.1365-2036.2004.02067.x. [DOI] [PubMed] [Google Scholar]
- 20.Adler DG, Knipschield M, Gostout C. A prospective comparison of capsule endoscopy and push enteroscopy in patients with GI bleeding of obscure origin. Gastrointest Endosc. 2004;59:492–498. doi: 10.1016/s0016-5107(03)02862-1. [DOI] [PubMed] [Google Scholar]
- 21.Saurin JC, Delvaux M, Vahedi K, et al. Clinical impact of capsule endoscopy compared to push enteroscopy: 1-year follow-up study. Endoscopy. 2005;37:318–323. doi: 10.1055/s-2005-861114. [DOI] [PubMed] [Google Scholar]
- 22.de Leusse A, Vahedi K, Edery J, et al. Capsule endoscopy or push enteroscopy for first-line exploration of obscure gastrointestinal bleeding? Gastroenterology. 2007;132:855–862. doi: 10.1053/j.gastro.2006.12.002. [DOI] [PubMed] [Google Scholar]
- 23.Pennazio M, Santucci R, Rondonotti E, et al. Outcome of patients with obscure gastrointestinal bleeding after capsule endoscopy: report of 100 consecutive cases. Gastroenterology. 2004;126:643–653. doi: 10.1053/j.gastro.2003.11.057. [DOI] [PubMed] [Google Scholar]
- 24.Carey EJ, Leighton JA, Heigh RI, et al. A single-center experience of 260 consecutive patients undergoing capsule endoscopy for obscure gastrointestinal bleeding. Am J Gastroenterol. 2007;102:89–95. doi: 10.1111/j.1572-0241.2006.00941.x. [DOI] [PubMed] [Google Scholar]
- 25.Hartmann D, Schmidt H, Bolz G, et al. A prospective two-center study comparing wireless capsule endoscopy with intraoperative enteroscopy in patients with obscure GI bleeding. Gastrointest Endosc. 2005;61:826–832. doi: 10.1016/s0016-5107(05)00372-x. [DOI] [PubMed] [Google Scholar]
- 26.Li X, Chen H, Dai J, Gao Y, Ge Z. Predictive role of capsule endoscopy on the insertion route of double-balloon enteroscopy. Endoscopy. 2009;41:762–766. doi: 10.1055/s-0029-1215009. [DOI] [PubMed] [Google Scholar]
- 27.Iddan G, Meron G, Glukhovsky A, Swain P. Wireless capsule endoscopy. Nature. 2000;405:417. doi: 10.1038/35013140. [DOI] [PubMed] [Google Scholar]
- 28.Pasha SF, Leighton JA, Das A, et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin Gastroenterol Hepatol. 2008;6:671–676. doi: 10.1016/j.cgh.2008.01.005. [DOI] [PubMed] [Google Scholar]
- 29.Chen X, Ran ZH, Tong JL. A meta-analysis of the yield of capsule endoscopy compared to double-balloon enteroscopy in patients with small bowel diseases. World J Gastroenterol. 2007;13:4372–4378. doi: 10.3748/wjg.v13.i32.4372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Nakamura M, Niwa Y, Ohmiya N, et al. Preliminary comparison of capsule endoscopy and double-balloon enteroscopy in patients with suspected small-bowel bleeding. Endoscopy. 2006;38:59–66. doi: 10.1055/s-2005-870446. [DOI] [PubMed] [Google Scholar]
- 31.Fujimori S, Seo T, Gudis K, et al. Diagnosis and treatment of obscure gastrointestinal bleeding using combined capsule endoscopy and double balloon endoscopy: 1-year follow-up study. Endoscopy. 2007;39:1053–1058. doi: 10.1055/s-2007-967014. [DOI] [PubMed] [Google Scholar]
- 32.Kameda N, Higuchi K, Shiba M, et al. A prospective, single-blind trial comparing wireless capsule endoscopy and double-balloon enteroscopy in patients with obscure gastrointestinal bleeding. J Gastroenterol. 2008;43:434–440. doi: 10.1007/s00535-008-2182-9. [DOI] [PubMed] [Google Scholar]
- 33.Marmo R, Rotondano G, Casetti T, et al. Degree of concordance between double-balloon enteroscopy and capsule endoscopy in obscure gastrointestinal bleeding: a multicenter study. Endoscopy. 2009;41:587–592. doi: 10.1055/s-0029-1214896. [DOI] [PubMed] [Google Scholar]
- 34.Matsumoto T, Esaki M, Moriyama T, Nakamura S, Iida M. Comparison of capsule endoscopy and enteroscopy with the double-balloon method in patients with obscure bleeding and polyposis. Endoscopy. 2005;37:827–832. doi: 10.1055/s-2005-870207. [DOI] [PubMed] [Google Scholar]
- 35.Hadithi M, Heine GD, Jacobs MA, van Bodegraven AA, Mulder CJ. A prospective study comparing video capsule endoscopy with double-balloon enteroscopy in patients with obscure gastrointestinal bleeding. Am J Gastroenterol. 2006;101:52–57. doi: 10.1111/j.1572-0241.2005.00346.x. [DOI] [PubMed] [Google Scholar]
- 36.Mehdizadeh S, Ross A, Gerson L, et al. What is the learning curve associated with double-balloon enteroscopy? Technical details and early experience in 6 U.S. tertiary care centers. Gastrointest Endosc. 2006;64:740–750. doi: 10.1016/j.gie.2006.05.022. [DOI] [PubMed] [Google Scholar]
- 37.Ohmiya N, Yano T, Yamamoto H, et al. Diagnosis and treatment of obscure GI bleeding at double balloon endoscopy. Gastrointest Endosc. 2007;66(3 Suppl):S72–S77. doi: 10.1016/j.gie.2007.05.041. [DOI] [PubMed] [Google Scholar]
- 38.Arakawa D, Ohmiya N, Nakamura M, et al. Outcome after enteroscopy for patients with obscure GI bleeding: diagnostic comparison between double-balloon endoscopy and videocapsule endoscopy. Gastrointest Endosc. 2009;69:866–874. doi: 10.1016/j.gie.2008.06.008. [DOI] [PubMed] [Google Scholar]
- 39.Gerson L, Kamal A. Cost-effectiveness analysis of management strategies for obscure GI bleeding. Gastrointest Endosc. 2008;68:920–936. doi: 10.1016/j.gie.2008.01.035. [DOI] [PubMed] [Google Scholar]
- 40.Somsouk M, Gralnek IM, Inadomi JM. Management of obscure occult gastrointestinal bleeding: a cost-minimization analysis. Clin Gastroenterol Hepatol. 2008;6:661–670. doi: 10.1016/j.cgh.2008.02.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ladas SD, Triantafyllou K, Spada C, et al. European Society of Gastrointestinal Endoscopy (ESGE): recommendations (2009) on clinical use of video capsule endoscopy to investigate small-bowel, esophageal and colonic diseases. Endoscopy. 2010;42:220–227. doi: 10.1055/s-0029-1243968. [DOI] [PubMed] [Google Scholar]