

Abstract
The stress of co-infection with HIV and Human Papillomavirus (HPV), in race/ethnic minority women, may increase depression and immune decrements. Compromised immunity in HIV+ HPV+ women may increase the odds of cervical dysplasia. Thus we tested the efficacy of a 10-wk cognitive behavioral stress management (CBSM) group intervention and hypothesized that CBSM would decrease depression and improve immune status (CD4+ T-cells, natural killer [NK] cells). HIV+HPV+ women (n=71) completed the Beck Depression Inventory (BDI) and provided blood samples, were randomized to CBSM or a control condition, and were re-assessed post-intervention. Women in CBSM revealed less depression, greater NK cells, and marginally greater CD4+ T-cells post-intervention vs. controls. Stress management may improve mood and immunity in HIV+HPV+ lower income minority women.
Introduction
The incidence of Human Immunodeficiency Virus (HIV) infection and Acquired Immunodeficiency Syndrome (AIDS) in the United States is increasing more rapidly among women, specifically in women of color, than in any other defined population at risk for HIV infection (CDC, 2007). Recent studies have found that women infected with HIV have increased prevalence, incidence, and persistence rates of human papillomavirus (HPV) infection, cervical neoplasia and invasive cervical cancer (Hankins et al., 1999; Massad et al., 1999). Approximately 40% of women with HIV may develop a neoplastic lesion (Goedert, 1998), which can then lead to cervical cancer (Tachezy, 2003). Even with standard treatment, recurrence of cervical intraepithelial neoplasia (CIN) persists in women who have HIV, and studies show that the severity of cervical lesions are inversely correlated with immune function (Boccalon, Tirelli, Sopracoredevoli, & Vaccher, 1996). Moreover, research examining cellular immune activity in progression of CIN shows that regressors (individuals with baseline gynecological abnormalities that regressed to normal results by follow-up) show an increase of CD4+ T-cell counts at follow-up (Moore et al., 2002). Other studies have found that HPV recurrence is associated with decreased Natural Killer (NK) cell count (Stentella et al., 1998), and that patients with spontaneous regression of cervical dysplasia show higher levels of NK cell activity (Garzetti et al., 1995).
Individual differences in psychological variables such as depression have been related to health status in HIV-infected persons (Leserman, 2008). Studies examining the psychosocial impact of an HIV+HPV+ diagnosis have found increased stress reports and depression rates when compared with women with neither diagnosis (McCaffery, Waller, Nazroo, & Wardle, 2006; Clarke, Ebel, Catotti, & Stewart, 1996; Kabbash, El-Gueneidy, Sharaf, Hassan, & Al-Nawawy, 2008; Siegel & Schrimshaw, 2005). One meta-analysis reported that depression rates in persons with HIV are twice those of HIV seronegative individuals (Ciesla & Roberts, 2001). We also know that people with HIV who report lower life stress and fewer depressive symptoms show less declines in CD4+ T-cell percentages at 6 month follow-up (Patterson et al., 1995). Depression has been associated with enumerative immune measures (e.g. lower CD4+ T-cells) that hastened disease progression in HIV+ persons (Leserman, 2008). Furthermore, studies have shown a relationship between both depression and severe stress with lower NK cells (Evans et al., 1995; Alciati, Gallo, Monforte, Brambilla, & Mellado, 2007).
Given the evidence, it appears that HIV+HPV+ women, especially those from race/ethnic minority groups, are particularly vulnerable to experiencing a variety of psychological stressors that may exacerbate depressive symptoms, which can then influence immune system functioning and susceptibility to disease progression. As mentioned previously, HIV+HPV+ women experience higher rates of depressive symptoms than women with neither diagnosis. These psychosocial factors have been associated with immunological changes, which in turn have been shown to play a role in HIV disease progression and HPV-associated neoplasias (Massad et al., 1999; Palefsky, 2003; Harris et al., 2005; Bonneau, 1994; Ho et al., 1995; Grinsztejn et al., 2008). It would be plausible to suggest then that this population, who is dealing with considerable amounts of challenges, would benefit from behavioral interventions designed to lower stress, such as those that teach cognitive behavioral techniques that help individuals cope and manage their distress.
Currently, there is growing evidence that stress management interventions are effective and beneficial to distressed medical populations. The literature on HIV has shown that stress management interventions can buffer declines of CD4+ T-cells, decrease depressed mood, and elevate quality of life (Creswell, Myers, Cole, &Irwin, 2009; Chan et al., 2004; Crepaz et al., 2008). One intervention in particular, group-based Cognitive Behavioral Stress Management (CBSM) intervention has received much attention due to its effectiveness in improving adjustment and physical health indicators in populations that are HIV+ (Carrico & Antoni, 2008). CBSM has been shown to improve depression and anxiety in a sample of homosexual men awaiting HIV status notification (Antoni et al., 1991), and in minority women living with HIV (Laperriere et al., 2005; Lechner et al., 2003). In one study of homosexual men awaiting HIV status notification, those receiving CBSM showed increases in helper CD4+ T-cells, NK cell counts, and NKCC compared to controls pre to post-intervention (Antoni et al., 1991). Other studies have replicated these CBSM findings on depressed mood, anxiety, and distress in gay men with symptomatic HIV (Antoni et al., 1991, Carrico, Antoni, Weaver, Lechner, & Schneiderman, 2005). Finally, prior studies of women with both HIV and HPV have shown that CBSM appears to lower the odds of persistent cervical neoplasia (Antoni et al., 2008).
The present study conducted secondary analysis on data collected in the latter trial (Antoni et al., 2008). Specifically, we examined whether CBSM influences aspects of depression and immune status in lower income race/ethnic minority HIV+HPV+ women. We hypothesized that women receiving a CBSM intervention would show a decrease in depression symptoms and improvements in immune status (i.e., increased CD4+ T-cells and NK cells) from baseline to post-intervention. We also hypothesized that CBSM effects on immune variables would be largest in women showing the greatest decreases in depression. Finally we examined which of the targets of this intervention (e.g., perceived relaxation skills, improved interpersonal skills etc.) are associated with improvements in depression.
Methods
Participants and Procedures
Participants were recruited from the Special Immunology Clinic at the Department of Obstetrics and Gynecology at the University of Miami/Jackson Memorial Hospitals, where patients received routine gynecological, prenatal, postpartum, family planning, and primary care. Women eligible to participate in the study were co-infected with HIV and HPV, between the ages of 18 to 60, had a history of Papanicolaou smears indicating low-grade squamous intraepithelial lesions (LGSIL) or at least two cervical biopsies indicating atypical cells of undetermined significance (ASCUS) in the two years prior to baseline entry, had a CD4+CD3+ cell count above 200 cells/mm3, and were fluent in English. Exclusion criteria included two or more negative Papanicolaou smears in the two years prior to baseline entry; a history of high-grade SIL diagnosis, or invasive cervical cancer; being on immunotherapy; pregnant or postpartum less than six weeks. Women were also required to have a 6th grade reading and writing level, and not be experiencing any major psychiatric illnesses, substance abuse or suicidality.
Of the 142 women screened for the study, 53 did not meet study criteria, 17 were unwilling to participate, and 2 were missing data on variables of interest. The final sample consisted of 71 participants; 46 were randomized to the CBSM condition and 25 to the control group. A Consort Flow Diagram is shown on Figure 1. Data from baseline and post-intervention (3 month after baseline) were utilized for this study. Characteristics by group are shown in Table 1. Additionally, psychosocial and immunological outcomes by group at baseline and post-intervention are shown in Table 2. At baseline, participants completed an informed consent, medical history interview, underwent a colposcopy, provided a cervical swab for HPV testing, and provided morning peripheral venous blood samples (between 8:00am – 12:00pm). Gynecological history and chart review were used to establish eligibility criteria of a history of papanicolaou smears indicating LGSIL or at least two cervical biopsies indicating ASCUS in the two years prior to study entry. An in-person psychosocial assessment interview was also conducted at baseline and included a well-validated measure of depression (e.g. Beck Depression Inventory; Beck, Ward, Mendelson, Mock, & Erbaugh, 1961). After the psychosocial assessment interview, participants were randomized to CBSM or to the control condition. A 2:1 ratio procedure was implemented as it allowed randomization of six participants to the CBSM condition per cohort, which has been found to be an appropriate size to conduct a CBSM group (Antoni, Ironson, & Schneiderman, 2007). Furthermore, a 2:1 procedure enhanced recruitment among women potentially reluctant to enroll in the study. This provided a greater chance of being assigned to the experimental condition and allowed more individuals to receive the intervention.
Figure 1.
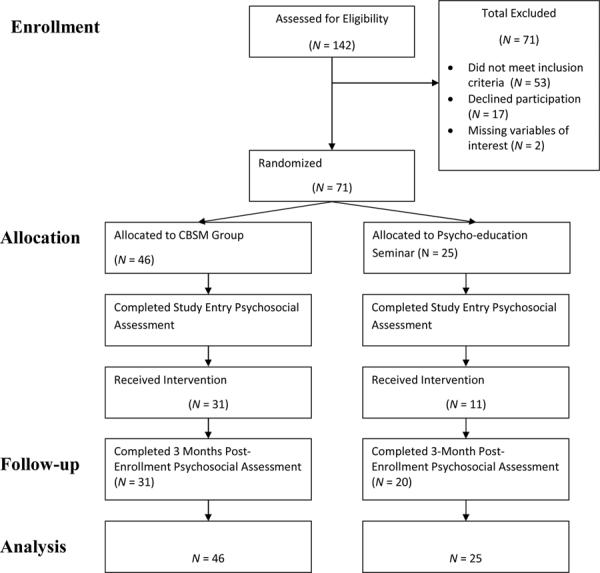
Participant flow diagram for the present randomized clinical trial.
*Only data from pre-post intervention was utilized for this study.
Table 1.
Characteristics of Sample.
| Variables | CBSM | Control |
|---|---|---|
| Demographics | ||
| Mean Age | 31.89(SD=8.45) | 30.19(SD=8.41) |
| Ethnicity | 62.2% Black 17.8% Black Other 11.2% Latina 4.4% Caribbean 2.2% Caucasian 2.2% Asian |
73.1% Black 15.4% Latina 7.1% Caribbean 2.2% Caucasian 2.2% Asian |
| Marital Status | 55.6% Single 22.1% Married 8.9% Divorced 6.7% Separated 6.7% Widowed |
50.1% Single 19.2% Married 15.4% Separated 11.5% Divorced 3.8% Widowed |
| Number of Children | 1.73(SD=1.33) | 1.88(SD=1.42) |
| Mean years of Education | 11.69(SD=1.74) | 11.32(SD=1.35) |
| Job Status | 60% Full Time 26.7% Part Time 6.7% Disability 6.7% Student |
75% Full Time 12.5% Student 6.3% Part Time 6.3% Disability |
| Average Yearly Income | $11, 957.82(SD=8,642.50) | $11,070.00(SD-8,290.95) |
| HIV History and Treatment | ||
| Mean Months Since Diagnosis | 72.69(49.30) | 84.04(47.15) |
| HIV Medications: NNRTI |
Yes 10.5% No 89.5% |
Yes 22.7% No 77.3% |
| NRTI | Yes 76% No 24% |
Yes 70.6% No 29.4% |
| MCC | Yes 18% No 82% |
Yes 13.0% No 87.0% |
| Protease Inhibitor | Yes 23.7% No 76.3% |
Yes 26.1% No 73.9% |
| OB/GYN | ||
| Cervical Dysplasia at study entry | Yes 79.5% No 20.5% |
Yes 88.5% No 11.5% |
| History of Syphilis | Yes 22.7% No 77.3% Unknown 2.3% |
Yes 26.9% No 65.4% Unknown 7.7% |
| History of Chlamydia | Yes 34.1% No 65.9% |
Yes 23.1% No 69.2% Unknown 7.7% |
| History of Genital Herpes | Yes 27.3% No 70.5% Unknown 2.3% |
Yes 30.8% No 61.5% Unknown 7.7% |
| Leukoplakia in Cervix | Yes 2.3% No 97.7% |
Yes 7.7% No 92.3% |
SD= Standard Deviation; NNRTI= Non-nucleoside reverse transcriptase inhibitor; NRTI= Nucleoside reverse transcriptase inhibitor; MCC= Multi-Class combination;
Table 2.
Psychosocial and immunological outcome variables at baseline (T1) and post-intervention (T2).
| CBSM | CONTROL | |||
|---|---|---|---|---|
| MEAN | SD | MEAN | SD | |
| Outcome Variables | ||||
| BDI-Total |
T1: 8.98(10.08) T2: 6.91(10.07) |
T1: 10(9.61) T2: 10.38(2.26) |
||
| BDI-Cognitive Affective |
T1: 5.86(7.43) T2: 6.91(10.07) |
T1: 7.68(7.88) T2: 10.38(2.26) |
||
| BDI-Somatic |
T1: 3.04(3.34) T2: 2.31(3.08) |
T1: 2.32(2.19) T2: 3.43(3.01) |
||
| CD4 cells/mm3 |
T1: 422.21(266.17) T2: 442.61(306.33) |
T1: 462.56(327.46) T2: 386.50(249.80) |
||
| NK cells/mm3 |
T1: 97.71(60.26) T2: 88.33(54.28) |
T1: 102.32(126.55) T2: 62.11(41.44) |
||
| Viral Load copies/mm3 |
T1: 29, 513.48 (117,239.784) T2: 12,462.90 (28,331.98) |
T1: 21, 358.16 (37,221.72) T2: 16,911.06 (24,196.618) |
||
SD= Standard Deviation
CBSM intervention
The CBSM condition comprised ten group-based 2.5 hour weekly sessions consisting of relaxation training (e.g. progressive muscle relaxation, diaphragmatic breathing, autogenics and mindfulness meditation), and a didactic cognitive behavioral component (cognitive restructuring, coping effectiveness training, assertion training, anger management and social support building techniques). The intervention employed a similar format as previous CBSM studies conducted with HIV+ women and men (Pereira, 2002), but included modifications designed to make the intervention more applicable for low-income minority women who were HIV+HPV+ (Antoni et al., 2008). These changes included education on cervical health, overcoming barriers for gynecological treatment, and utilizing intrapersonal, spiritual, and social resources to negotiate safer sex. Sessions were conducted according to a training manual by a post-doctoral associate and advanced clinical psychology graduate students.
Psycho-education control
Women who were randomized to the control condition were invited to attend a one-day seminar where they received a summary of general health information and stress management in a group setting. The control condition differed from the intervention in having less contact hours, lack of structured group interactions, and absence of homework or assigned home based practice. It can be conceptualized as a minimal contact educational control focusing on assorted self-help topics relevant to stress, coping, and health in HIV.
Measures
Beck depression inventory (BDI)
(Beck, Ward, Mendelson, & Erbaugh, 1961). The BDI is a widely used 21 item multiple choice self report measure designed to assess symptoms of depression. The measure is designed for individuals 13 or older, and is composed of items asking about hopelessness, weight loss, fatigue, guilt etc. in order to assess severity of depression. The BDI produces a total score and cognitive-affective and somatic subscale scores. The BDI has a split half Spearman-Brown reliability of .93 for psychiatric patients (Beck, 1970), and a mean alpha coefficient of .81 for non-psychiatric patients (Beck, Steer, & Garbin, 1988). The BDI correlates highly with alternative depression measures such as the Hamilton Rating Scale for Depression (mean= .73 in psychiatric samples) and the Zung Self Reported Depression Scale (mean= .76 in psychiatric samples) and discriminates well between several different groups of both psychiatric and non-psychiatric populations (Beck, Steer, & Garbin, 1988). The BDI has been used frequently with individuals infected with HIV and has been shown to improve over the course of the 10 week CBSM intervention in men with HIV (Lutgendorf et al., 1997; Lutgendorf et al., 1998). The mean BDI for the participants was 9.34 (SD= 12.80; range = 0 – 44, α= .92).
Immunologic Measures
Immune measures utilized in this study included HIV viral load, T-helper cells (CD4+), and NK cells (CD56+). Blood draws were performed by a trained phlebotomist at the Women's Health Initiative Program (WHI) at the UM/JMH campus and were taken to the E.M. Papper Clinical Immunology Laboratory within two hours of draw. Enumeration of lymphocyte subpopulations was determined by flow cytometry and 4-color direct immunofluorescence as outlined by Ironson et al. (1997). HIV viral load was determined through an ultrasensitive in vitro reverse transcriptase polymerase chain reaction assay (AMPLICOR, Roche Laboratories, US #83088) with a lower limit of 50 copies/ml.
Statistical Analyses
Hierarchical multiple regression analyses tested for group differences (CBSM vs. control) in post-intervention depression while controlling for baseline levels in addition to putative confounding variables. To determine potential confounders, we ran independent t-tests and chi square tests comparing the CBSM vs. control group on a set of sociodemographic and health variables at baseline. Candidate covariates included HIV medications, such as highly active antiretroviral therapy, sleep quality, adherence to medications, illicit drug use, number of cigarettes smoked, caffeine, alcohol, antihistamines, and nicotine use, as they have been shown to contribute to mood, hormonal and immunologic changes (Kuhn, 1989; Sellmeyer & Grunfeld, 1996). None of these measures differed by group assignment. However, we decided to control for sleep quality via the Pittsburgh Sleep Quality Index (PSQI; Buysse, Reynolds, Monk, Berman, & Kupfer, 1995) as it was correlated with depression symptoms at study entry.
We also examined associations between the immune measures, CD4+ cell and NK cell counts, and multiple demographic, health behaviors, medications, and medical co-morbidities that could affect the immune system (see Table 3). As can be seen, there were very few associations between these patient characteristics and immune measures. Less education, greater time since diagnosis, and being on a Nucleoside Reverse Transcriptase Inhibitor (NRTI) medication regimen were associated with lower CD4+ cell counts at study entry, while greater age related to lower NK cell counts. However, all of these factors were equally balanced between CBSM and controls. There were no associations between immune measures and health behaviors (e.g., unsafe sex, tobacco, alcohol, or substance use), medical co-morbidities, or gynecological health history. Therefore we did not control for any of these variables in our analyses.
Table 3.
Correlations between CD4+ cells/Natural killer cells and demographics, HIV histor and treatment regimen, health behaviors, and ob/gyn variables at study entry.
| CD4 Cells | NK Cells | |
|---|---|---|
| Demographics | ||
| Age | r=−.15 | r=.30* |
| Yearly Income | r=−.08 | r=−.07 |
| Education | r=−.23* | r=−.05 |
| Living Status | r=−.07 | r=.05 |
| HIV History and Treatment | ||
| Months Since Dx | r=−.30* | r=.07 |
| NNRTI | r=−.13 | r=−.15 |
| NRTI | r=−.34* | r=.06 |
| MCC | r=−.11 | r=−.03 |
| Protease Inhibitor | r=.01 | r=.04 |
| Health Behaviors | ||
| Recent # Unsafe Sexual Behaviors | r=.02 | r=−.13 |
| Recent Alcohol Use | r=.09 | r=−.18 |
| # Smoking Packs per day | r=−.08 | r=−.08 |
| Marijuana | r=−.03 | r=−.13 |
| Coffee | r=.12 | r=−.02 |
| Vigorous Physical Activity | r=−.05 | r=.03 |
| Sleep Quality | r=.11 | r=.09 |
| Co-Morbidity | ||
| Arthritis | r=−.23 | r=−.00 |
| Cancer | r=−.12 | r=−.02 |
| Asthma | r=.14 | r=.24 |
| Hepatitis | r=.13 | r=.09 |
| OB/GYN | ||
| Cervical Dysplasia at study entry | r=−.15 | r=.07 |
| History of Syphilis | r=−.14 | r=−.13 |
| History of Chlamydia | r=−.01 | r=−.12 |
| History of Genital Herpes | r=−.04 | r=.18 |
| History of Genital Warts | r=.00 | r=−.03 |
| Leukoplakia in Cervix | r=.13 | r=−.11 |
p ≤.05; NNRTI= Non-nucleoside reverse transcriptase inhibitor; NRTI= Nucleoside reverse transcriptase inhibitor; MCC= Multi-Class combination
Fifty-three percent of participants reported taking highly active antiretroviral therapy (HAART) medications at study entry, and 51% of individuals on HAART with complete self-reported adherence data reported 100% adherence to their regimen in the four days prior to study entry. For this sample, baseline self-reported adherence was not significantly correlated with depression (r=−0.16, p=.92), CD4 cells (r=0.10, p=.53), NK cells (r=0.17, p=.30), or HIV viral load (r=−0.30, p=.19) at post-intervention. There was a 50% mean attendance rate for women in the one day seminar condition and a 45% attendance rate for women in the CBSM condition. Attendance rate was not significantly correlated with outcomes for either group (all p's= ns).
To examine whether CBSM-associated changes in immune system indicators paralleled the magnitude of reductions in depressive symptoms the bootstrap method was used to test mediation, to estimate direct and indirect effects, and estimate confidence intervals. Bootstrapping is the preferred method for testing mediation and is recommended for small sample sizes as it provides a more precise estimate of indirect effects (Preacher & Hayes, 2008). The SPSS default bootstrap command was utilized which requests 1,000 bootstrap re-samples.
Missing follow-up data was imputed in the present study by utilizing a linear interpolation method (Little & Rubin, 1987). This method is an improvement over mean substitution in that the value substituted is predicted from variables within the same scale of the same person (Norazian, Ahmad Shukri, Ramli, & Mohd Mustafa, 2007). Linear interpolation links the observed values before and after the missing value, such that the missing value at x=x is imputed by the mean value at x=x−1 and x=x+1. The amount of missing values in the present data ranged from 1–18 values for the BDI, and 4–18 values for immune variables. The majority of missing data for outcome measures was found at post-intervention. Furthermore, psychosocial and immunological data was indicated to be missing completely at random as shown by Little's MCAR test (X2= 9.68, DF= 11, p= .560).
Results
Mood effects
Assignment to the CBSM group significantly predicted decreases in BDI somatic subscale scores at post-intervention (ΔR2= .05, p < .05) but did not affect BDI total or BDI cognitive-affective subscale scores (p's > .05). To determine whether CBSM effects on depression were independent of changes in sleep quality we re-ran regression analyses controlling for sleep quality as a covariate. Significant effects of decreases in the BDI somatic subscale remained even after including sleep quality as a control variable (ΔR2= .07, p < .03). Because of the significant CBSM effect on depression, exploratory analyses looking at anxiety and confidence in using relaxation as outcomes were also conducted to investigate if women showed parallel changes in these psychological variables during the intervention. Assignment to CBSM did not predict differences in anxiety at post-intervention (p = ns). However, assignment to CBSM significantly predicted greater confidence in using relaxation techniques (ΔR2= .08, p < .04) as measured by the Measure of Current Status scale (MOCS; Carver, 2006). Increases in relaxation confidence for women in CBSM were, in turn, significantly correlated with reductions in BDI somatic scores (r=−.37, p=.007).
Immune effects
To examine whether assignment to CBSM predicted improved immune status at post-intervention and whether CBSM-associated changes in immune system indicators paralleled the magnitude of reductions in somatic depressive symptoms, bootstrapping analyses were performed on CD4+ T-cell counts and somatic depression scores at post-intervention. Bootstrapping results revealed that assignment to CBSM was marginally significantly associated with greater CD4+ T-cells (b = 106.27, SE = 56.89, t(66) = 1.87, p = .06) as shown in Table 4. Assignment to CBSM was also significantly associated with lower BDI somatic subscale scores (b = −1.29, SE = .67, t(66) = −1.93, p < .05). The BDI somatic subscale (b = −21.39, SE = 10.12, t(66) = −2.11, p = .04), in turn, was inversely associated with post-intervention CD4+T-cell counts. The direct effect of assignment to CBSM on CD4+ T-cells with the BDI somatic subscale in the equation was reduced to b = 78.69, SE = 56.98 (t(66) = 1.38, ns) suggesting that reductions in BDI somatic depression accounted, in part, for the effects of the intervention on CD4+ T-cells. Furthermore, the indirect effect of assignment to CBSM on CD4+ T-cells through the BDI somatic subscale was significant (bootstrap estimated indirect effect =25.92, CI= 3.77, 74.35, p < .001). The total amount of variance accounted by for the complete model was 34% (Adj. R2 = .34, p < .001). These results support the hypothesis that a CBSM intervention may increase CD4+ T-cell count in HIV+HIV+ women, an effect that is paralleled by reductions in BDI somatic depression scores. Given the association between sleep quality and depression, bootstrapping analyses controlling for sleep quality were also tested. Findings remained significant with inclusion of sleep quality as a covariate, supporting a depression mediation model.
Table 4.
Bootstrapping results for the influence of BDI somatic (BDI-S) scores on the relationship between assignment to CBSM and (a) CD4+ T-cells and (b) CD56+ NK cells.
| OUTCOME | DIRECT EFFECTS | INDIRECT EFFECTS | |
|---|---|---|---|
|
| |||
| Predictor/Mediator | b (SE)1 | Estimate2 | TIbootstrap3 |
|
|
|||
| (a) CD4+ T cells | |||
| CBSM | 106.27(56.89) | ||
| BDI-S | −21.39(10.12) | 25.93 | (3.77, 74.35) |
|
|
|||
| (b) CD56+ NK cells | |||
| CBSM | 24.12(11.72) | ||
| BDI-S | −.44(1.92) | .28 | (−1.66,7.06) |
|
|
|||
Predictor to outcome with mediators.
Bootstrapped estimates of indirect effects.
Bias-corrected confidence intervals.
Bootstrapping results also revealed that assignment to CBSM was significantly associated with greater NK cells at post-intervention (b = 24.44, SE = 11.56, t(66) = 2.12, p = .04). However, the BDI somatic subscale was not significantly associated with higher NK cell counts (b = −.91, SE = 1.95, t(66) = 1.31, p = .64), suggesting that reductions in depressive symptoms did not explain the effects of CBSM on NK cells. (See table 4). Lastly, results revealed that group assignment did not significantly predict post-intervention variance in viral load. See figure 2 for CBSM and control condition effects on BDI somatic, NK cells, and CD4+ cells.
Figure 2.

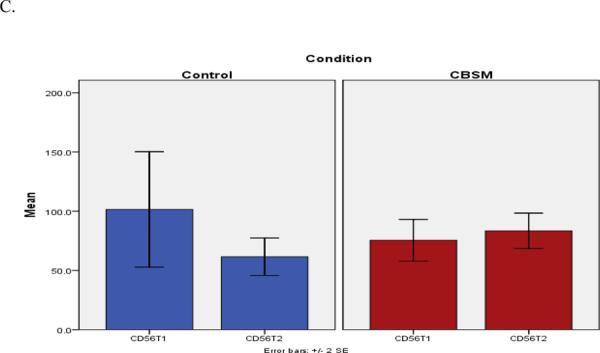
CBSM and control condition effects on BDI somatic (A), CD4+ cells/mm3 (B), and Natural killer (NK) cells/mm3 (C), from baseline (T1) to post-intervention (T2).
Discussion
The present study was based upon secondary analyses of the effects of a group-based CBSM intervention designed to help lower income racial/ethnic minority women living with HIV to cope with the stress of their illness. Because of the added vulnerability to HPV infection that many lower-income race/ethnic minority women with HIV suffer (Andrasik, Rose, Pereira, & Antoni, 2008), we recruited a sample of low-income minority women co-infected with HIV and HPV and tested the ability of a CBSM intervention that had been tailored for this group. Primary outcomes for this intervention can be found in Antoni et al., 2008. Results of the present secondary analyses revealed that women assigned to CBSM reported lower post-intervention somatic depression symptoms and increased perceived relaxation skills, as well as showing significantly increased CD56+ NK cells and marginally increased CD4+ T-cells compared to controls. These findings are important for the present population given the established relationship between CD4+ T-cells and HIV progression (Bonneau, 1994; Ho et al., 1995) and the role of CD56+ NK and CD4+ T-cells in helping the immune system successfully control the HPV virus (Garcia-Iglesias et al. 2009, Moore et al., 2002; Harris et al., 2005, Woo et al., 2008). It was also revealed that perceived relaxation skills correlated significantly with BDI somatic scores, which may point to a treatment component that is effective in reducing depression. These results are in accordance with previous studies showing that CBSM attenuates depressive symptoms in heterosexual and homosexual men and minority women infected with HIV (Antoni et al., 1991; Laperriere et al., 2005; Lechner et al., 2003; Lutgendorf et al., 1997; Carrico, Antoni, Weaver, Lechner & Schneiderman, 2005; Carrico & Antoni, 2008). In this particular study CBSM effects were found for somatic depressive symptoms, which may be due to differences in reports of depression symptoms found in ethnically and culturally diverse populations. Indeed, some studies have demonstrated differences in expressions of distress, with immigrant or minority populations expressing physical symptoms or somatization more often than their more westernized counterparts (Kirmayer, 2001; Baarnhielm & Ekblad, 2000).
Results also supported a model relating somatic depression changes during CBSM with immunological changes. Specifically, bootstrapping analyses showed that the effects of CBSM on CD4+ cells over time were explained, in part, by women's greater decreases in somatic depression symptoms. Findings provide further support to previous CBSM studies demonstrating a relationship between reductions in depressive symptoms and improvement in immune indices (Antoni et al., 1991; Antoni et al., 2005). This appears to be a consistent finding even in a relatively small and diverse sample as presented here. Since our outcome measurements of psychological and immunological variables occurred at post-intervention concurrently, there is a possibility that the relationship between depression and immune changes may be bi-directional. However, there is longitudinal research supporting a sequential relationship of depressive symptoms and immune changes in persons with HIV/AIDS (Leserman et al., 1997; Antoni et al., 2006; Laperriere et al., 2005). Interestingly, while CBSM was associated with increases in NK cell counts these changes were not accounted for by changes in somatic depression suggesting that other psychological changes potentially occurring during CBSM (e.g., social support, coping) may be more closely aligned with NK cell changes.
Overall, results suggest that CBSM is beneficial in reducing somatic depression and preserving immunological status in a vulnerable minority population dealing with HIV and HPV co-infection who are at risk for negative health outcomes such as cervical cancer. Given the dearth of research in this area, there is a need for future research investigating similar biobehavioral relationships and their influence on disease outcomes in HIV+HPV+ women (Andrasik, Rose, Pereira, & Antoni, 2008).
As with all studies utilizing small samples with missing data, interpretation of results should be made with caution due to limitations in power and biases introduced by missing data estimation techniques. Specifically, significant indirect effects may not be as stable due to the small sample size. The control group used in the present study did not match equivalence of patient contact between groups, creating a marked difference in attention time between conditions. Also, information on whether women were on hormonal treatment or if they were post-menopausal was unavailable. The generalizability of results is limited to low-income ethnically diverse women. Furthermore, due to the lack of data at longer-term follow-up it was not feasible to test longer-term effects to determine if immune improvements were maintained. Future work with a larger sample and longer follow-up period is indicated.
Future studies should pay particular attention to alternative psychological and ecological processes that may be quite relevant to low-income minority women co-infected with HIV and HPV. Inclusion of spiritually and culturally pertinent factors may provide researchers with a better understanding of the experiences of minority women dealing with deteriorating health and a lack of basic resources. For instance, the importance of spirituality and social support in health and healing in minority cultural groups has been well established (Brome, Owens, Allen, & Vevaina, 2000; Potts, 1996; Hodge et al., 2000), with particular medical populations, such as those living with HIV and cancer, also gaining benefits (Galvan, David, Banks, & Bing, 2008; Crawford, Allison, Zamboni, & Soto, 2002; Lagos et al., 2008; Avants & Margolin, 2004; Yanez et al., 2009). Other relevant work has shown the importance of maintaining a sense of ethnic identity in managing stress levels among lower income minority women with HIV (Lopez, Antoni, Fekete, & Penedo, 2012).
In conclusion, the present work identifies CBSM effects on depressive symptoms and immune status in a sample of lower income racial/ethnic minority women living with HIV and HPV infection. Our results suggested that CBSM was beneficial in ameliorating somatic symptoms of depression and preserving immune status evidenced by CD4+ and NK cells. A biobehavioral model was supported where the effects of CBSM on psychological changes may have contributed to immunological status found at post-intervention. However, this model must be viewed as tentative until a larger sample can be collected that can fully elucidate the trajectories of disease over longer time periods.
Declaration of Interest and acknowledgements
This work was supported by an NIH grant (5 P50 CA84944) to MA. Dr. Antoni reports receiving royalties form a book based on stress management techniques similar to those tested in the present study.
References
- Abbas A, Lichtman A, Pober J. Cellular and molecular immunology. Saunders; Philadelphia: 1991. [Google Scholar]
- Alciati A, Gallo L, Monforte AD, Brambilla F, Mellado C. Major depression-related immunological changes and combination antiretroviral therapy in HIV-seropositive patients. Human Psychopharmacology. 2007;22:33–40. doi: 10.1002/hup.813. doi:10.1002/hup.81315. [DOI] [PubMed] [Google Scholar]
- Antoni MH, Goodkin K. Host moderator variables in the promotion of cervical neoplasia. II. Dimensions of life stress. Journal of Psychosomatic Research. 1989;33:457–67. doi: 10.1016/0022-3999(89)90007-x. [DOI] [PubMed] [Google Scholar]
- Andrasik MD, Rose R, Pereira D, Antoni M. Barriers to cervical screening among low-income HIV positive African American women. Journal of Health Care for the Poor and Undeserved. 2008;19:912–925. doi: 10.1353/hpu.0.0037. [DOI] [PubMed] [Google Scholar]
- Antoni MH, Baggett L, Ironson G, August S, LaPerriere A, Klimas N, Fletcher MA. Cognitive behavioral stress management intervention buffers distress responses and immunologic changes following notification of HIV-1 seropositivity. Journal of Consulting and Clinical Psychology. 1991;59:906–915. doi: 10.1037//0022-006x.59.6.906. [DOI] [PubMed] [Google Scholar]
- Antoni MH, Cruess D, Klimas N, Maher K, Cruess S, Lechner S, Schneiderman N. Increases in a marker of immune system reconstitution are predated by decreases in 24-hour urinary cortisol output and depressed mood during a 10-week stress management intervention in symptomatic gay men. Journal of Psychosomatic Research. 2005;58:3–13. doi: 10.1016/j.jpsychores.2004.05.010. [DOI] [PubMed] [Google Scholar]
- Antoni MH, Ironson G, Schneiderman N. Stress Management for Persons with HIV Infection. Oxford University Press; New York: 2007. [Google Scholar]
- Antoni MH, Lutgendorf S, Cole S, Dhabhar F, Sephton S, McDonald P, Sood A. The influence of biobehavioral factors on tumor biology, pathways and mechanisms. Nature Reviews Cancer. 2006;6:240–248. doi: 10.1038/nrc1820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Antoni MH, Pereira DB, Marion I, Ennis N, Andrasik MP, Rose R, O'Sullivan MJ. Stress management effects on perceived stress and cervical neoplasia in low-income HIV-infected women. Journal of Psychosomatic Research. 2008;4:389–401. doi: 10.1016/j.jpsychores.2008.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Avants S, Margolin A. Development of spiritual self-Schema (3-S) therapy for the treatment of addictive and HIV risk behavior: A convergence of cognitive and buddhist psychology. Journal of Psychotherapy Integration. 2004;14(3):253–289. [Google Scholar]
- Bäärnhielm S, Ekblad S. Turkish migrant women encountering health care in Stockholm: a qualitiative study of somatization and illness meaning. Culture, Medicine and Psychiatry. 2000;24:431–452. doi: 10.1023/a:1005671732703. [DOI] [PubMed] [Google Scholar]
- Baron G, Klimas N, Fischl M, Fletcher MA. Decreased natural cell mediated cytotoxicity per effector cell in acquired immunodeficiency syndrome. Diagnostic Immunology. 1985;3:97–202. [PubMed] [Google Scholar]
- Beck A. Depression: Causes and Treatment. University of Pennsylvania Press; Philadelphia, PA: 1970. [Google Scholar]
- Beck A, Steer R, Garbin M. Psychometric properties of the Beck Depression Inventory: Twenty five years of evaluation. Clinical Psychology Review. 1988;8:77–100. [Google Scholar]
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Archives of General Psychiatry. 1961;4:561–71. doi: 10.1001/archpsyc.1961.01710120031004. [DOI] [PubMed] [Google Scholar]
- Boccalon M, Tirelli U, Sopracordevole F, Vaccher E. Intra-epithelial and invasive cervical neoplasia during HIV infection. European Journal of Cancer. 1996;32:2212–2217. doi: 10.1016/s0959-8049(96)00416-9. [DOI] [PubMed] [Google Scholar]
- Bonneau RH. Experimental approaches to identify mechanisms of stress-induced modulation of immunity to herpes simplex virus infection. Academic Press; New York, NY US: 1994. Handbook of Human Stress and Immunity; pp. 125–160. [Google Scholar]
- Brome DR, Owens MD, Allen K, Vevaina T. An examination of Spirituality among African American Women in recovery from substance abuse. The Journal of Black Psychology. 2000;26(4):470–486. [Google Scholar]
- Burack JH, Barrett DC, Stall RD, Chesney MA, Ekstrand ML, Coates TJ. Depressive symptoms and CD4 lymphocyte decline among HIV-infected men. JAMA. 1993;270(21):2568–2573. [PubMed] [Google Scholar]
- Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index (PSQI): A new instrument for psychiatric research and practice. Psychiatry Research. 1989;28(2):193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC) CDC HIV/AIDS Statistics and Surveillance. 2007 http://www.cdc.gov/hiv/topics/surveillance/basic.htm#aidscases. Retrieved on 06-25-2009.
- Carrico A, Antoni MH. The Effects of Psychological Interventions on Neuroendocrine Hormone Regulation and Immune Status in HIV-Positive Persons: A Review of Randomized Controlled Trials. Psychosomatic Medicine. 2008;70:575–584. doi: 10.1097/PSY.0b013e31817a5d30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carrico AW, Antoni MH, Weaver KE, Lechner SC, Schneiderman N. Cognitive-behavioural stress management with HIV-positive homosexual men: mechanisms of sustained reductions in depressive symptoms. Chronic Illness. 2005;1:207–15. doi: 10.1177/17423953050010030401. [DOI] [PubMed] [Google Scholar]
- Carver CS. Measure of Current Status. 2006 http://www.psy.miami.edu/faculty/ccarver/sclMOCS.html Retrieved on 11-01-11.
- Chan I, Kong P, Leung P, Au A, Li P, Chung R, Yu P. Cognitive-behavioral group program for Chinese heterosexual HIV-infected men in Hong Kong. Patient Education and Counseling. 2004;56:78–84. doi: 10.1016/j.pec.2003.12.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ciesla JA, Roberts JE. A meta-analysis of risk for Major Depressive Disorder among HIV-positive individuals. American Journal of Psychiatry. 2001;158:725–730. doi: 10.1176/appi.ajp.158.5.725. [DOI] [PubMed] [Google Scholar]
- Clarke P, Ebel C, Catotti DN, Stewart S. The psychosocial impact of human papillomavirus infection: implications for health care providers. Journal of STDS and AIDS. 1996;3:197–200. doi: 10.1258/0956462961917618. [DOI] [PubMed] [Google Scholar]
- Crawford I, Allison KW, Zamboni BD, Soto T. The influence of dual-identity development on the psychosocial functioning of African-American gay and bisexual men. Journal of Sex Research. 2002;3:179–89. doi: 10.1080/00224490209552140. [DOI] [PubMed] [Google Scholar]
- Crepaz N, Passin WF, J.H. H, Rama SM, Malow RM, Purcell DW, Wolitski RJ, Team HAPRSP. Meta-analysis of cognitive-behavioral interventions on HIV-positive persons' mental health and immune functioning. Health Psychology. 2008;27:4–14. doi: 10.1037/0278-6133.27.1.4. [DOI] [PubMed] [Google Scholar]
- Creswell JD, Myers HF, Cole SW, Irwin MR. Mindfulness meditation training effects on CD4+ T lymphocytes in HIV-1 infected adults: a small randomized controlled trial. Brain Behavior and Immunology. 2009;23:184–188. doi: 10.1016/j.bbi.2008.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evans DL, Leserman J, Perkins DO, Stern RA, Murphy C, Tamul K, Petitto JM. Stress-associated reductions of cytotoxic T lymphocytes and natural killer cells in asymptomatic HIV infection. American Journal of Psychiatry. 1995;152(4):543–550. doi: 10.1176/ajp.152.4.543. [DOI] [PubMed] [Google Scholar]
- Fletcher MA, Baron G, Ashman M, Fischl M, Klimas N. Use of whole blood methods in assessment of immune parameters n immunodeficiency states. Diagnostic and Clinical Immunology. 1987;5:69–81. [PubMed] [Google Scholar]
- Galvan F, Davis EM, Banks D, Bing EG. HIV stigma and social support among African Americans. AIDS Patient Care and STD's. 2008;22:423–436. doi: 10.1089/apc.2007.0169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garcia-Iglesias T, Del Toro-Arreola A, Albarran-Somoza B, Del Toro-Arreola S, Sanchez-Hernandez PE, Ramirez-Dueñas MG, Daneri-Navarro A. Low NKp30, NKp46 and NKG2D expression and reduced cytotoxic activity on NK cells in cervical cancer and precursor lesions. BMC Cancer. 2009;9:186. doi: 10.1186/1471-2407-9-186. doi:10.1186/1471-2407-9-186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garzetti GG, Ciavattini A, Provinciali M, Muzziolo M, Di Stefano G, Fabrins N. Natural killer cell activity in stage III and IV endometriosis: impaired cytotoxicity and retained lymphokine responsiveness of natural killer cells. Gynecological endocrinology. 1995;9:125–130. doi: 10.3109/09513599509160201. [DOI] [PubMed] [Google Scholar]
- Goedert JJ, Cote TR, Virgo P, Scoppa SM, Kingma DW, Gail MH, Biggar RJ. Spectrum of AIDS-associated malignant disorders. Lancet. 1998;351:1833–1839. doi: 10.1016/s0140-6736(97)09028-4. [DOI] [PubMed] [Google Scholar]
- Grinsztejn B, Veloso VG, Levi JE, Velasquez L, Luz PM, Friedman, Palefsky J. Factors associated with increased prevalence of human papillomavirus infection in a cohort of HIV-infected Brazilian women. International Journal of Infectious Diseases. 2008;13:72–80. doi: 10.1016/j.ijid.2008.03.031. [DOI] [PubMed] [Google Scholar]
- Hankins C, Coutlee F, Lapointe N, Simard P, Tran T, Samson J, Hum L. Prevalence of risk factors associated with human papillomavirus infection in women living with HIV. Canadian Women's HIV Study Group. 1999;160:185–91. [PMC free article] [PubMed] [Google Scholar]
- Harris TG, Burk RD, Palefsky JM, Massad LS, Bang JY, Anastos K, Strickler HD. Incidence of cervical squamous intraepithelial lesions associated with HIV serostatus, CD4 cell counts, and human papillomavirus results. Journal of the American Medical Association. 2005;292(12):1471–1476. doi: 10.1001/jama.293.12.1471. [DOI] [PubMed] [Google Scholar]
- Herbert TB, Cohen S. Depression and immunity: a meta-analytic review. Psychology Bulletin. 1993a;113:472–486. doi: 10.1037/0033-2909.113.3.472. [DOI] [PubMed] [Google Scholar]
- Herbert TB, Cohen S. Stress and immunity in humans: a meta-analytic review. Psychosomatic Medicine. 1993b;55:364–379. doi: 10.1097/00006842-199307000-00004. [DOI] [PubMed] [Google Scholar]
- Ho DD, Neumann AU, Perelson AS, Chen W, Leonard JM, Markowitz M. Rapid turnover of plasma virions and CD 4 lymphocytes in HIV-1 infection. Nature. 1995;373:123–126. doi: 10.1038/373123a0. [DOI] [PubMed] [Google Scholar]
- Hodge SCD, Headen SW, Skelly AH, Ingram AF, Keyserling TC, Jackson EJ, Elasy TA. Influences on day-to-day self-management of type 2 diabetes among African-American women: spirituality, the multi caregiver role, and other social context factors. Diabetes Care. 2000;23:928–33. doi: 10.2337/diacare.23.7.928. [DOI] [PubMed] [Google Scholar]
- Ironson G, Wynings C, Schneiderman N, Baum A, Rodriguez M, Greenwood D, Fletcher MA. Posttraumatic stress symptoms, intrusive thoughts, loss, and immune function after Hurricane Andrew. Psychosomatic Medicine. 1997;59:128–141. doi: 10.1097/00006842-199703000-00003. [DOI] [PubMed] [Google Scholar]
- Kabbash IA, El-Gueneidy M, Sharaf AY, Hassan NM, Al-Nawawy N. Needs assessment and coping strategies of persons infected with HIV in Egypt. Eastern Mediterranean Health Journal. 2008;6:1308–20. [PubMed] [Google Scholar]
- Kirmayer LJ. Cultural variations in the clinical presentation of depression and anxiety: implications for diagnosis and treatment. Journal of Clinical Psychiatry. 2001;62:22–28. [PubMed] [Google Scholar]
- Kuhn C. In: Adrenocortical and gonadal steroids in behavioral cardiovascular medicine. Schneiderman N, Kauffman P, editors. Handbook of Cardiovascular Methods; Plenum: 1989. pp. 185–204. [Google Scholar]
- Lagos VI, Perez MA, Ricker CN, Blazer KR, Santiago NM, Feldman N, Weitzel JN. Social-cognitive aspects of underserved Latinas preparing to undergo genetic cancer risk assessment for hereditary breast and ovarian cancer. Psychooncology. 2008;17:774–782. doi: 10.1002/pon.1358. [DOI] [PubMed] [Google Scholar]
- Laperriere A, Ironson GH, Antoni MH, Pomm H, Jones D, Ishii M, Weiss SM. Decreased depression up to one year following CBSM+ intervention in depressed women with AIDS: the smart/EST women's project. Journal of Health Psychology. 2005;2:223–231. doi: 10.1177/1359105305049772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lechner S, Antoni M, Lydston D, LaPerriere A, Ishii M, Devieux J, Weiss S. Cognitive-behavioral interventions improve quality of life in women with AIDS. Journal of Psychosomatic Research. 2003;54(3):253–261. doi: 10.1016/s0022-3999(02)00480-4. [DOI] [PubMed] [Google Scholar]
- Leserman J. Role of depression, stress, and trauma in HIV disease progression. Psychosomatic Medicine. 2008;70(5):539–45. doi: 10.1097/PSY.0b013e3181777a5f. [DOI] [PubMed] [Google Scholar]
- Leserman J, Petitto JM, Perkins DO, Folds JD, Golden RN, Evans DL. Severe stress, depressive symptoms, and changes in lymphocyte subsets in human immunodeficiency virus infected men. Archives of General Psychiatry. 1997;54:79–285. doi: 10.1001/archpsyc.1997.01830150105015. [DOI] [PubMed] [Google Scholar]
- Little RJA, Rubin DB. Statistical Analysis with Missing Data. J. Wiley & Sons; New York: 1987. [Google Scholar]
- Lopez CR, Antoni MH, Fekete EM, Penedo FJ. Ethnic Identity and Perceived Stress in HIV+ Minority Women: The Role of Coping Self-Efficacy and Social Support. International Journal of Behavioral Medicine. 2012;19:23–28. doi: 10.1007/s12529-010-9121-x. [DOI] [PubMed] [Google Scholar]
- Lutgendorf SK, Antoni MH, Ironson G, Klimas N, Kumar M, Starr K, McCabe P. Cognitive behavioral stress management intervention decreases dysphoria and herpes simplex virus-type2 antibody titers in symptomatic HIV seropositive gay men. Journal of Consulting of Clinical Psychology. 1997;65:23–231. doi: 10.1037//0022-006x.65.1.31. [DOI] [PubMed] [Google Scholar]
- Lutgendorf SK, Antoni MH, Ironson G, Starr K, Costello N, Zuckerman, Schneiderman N. Changes in cognitive coping skills and social support during cognitive behavioral stress management intervention and distress outcomes in symptomatic human immunodeficiency virus-seropositive gay men. Psychosomatic Medicine. 1998;60:204–214. doi: 10.1097/00006842-199803000-00017. [DOI] [PubMed] [Google Scholar]
- Massad LS, Riester KA, Anastos KM, Frutcher RG, Palefsky JM, Miotti P. Prevalence and predictors of squamous cell abnormalities in Papanicolaou smears from women infected with HIV-1. Women's Interagency HIV Study Group. Journal of Acquired Immune Deficiency Syndrome. 1999;21:33–41. doi: 10.1097/00126334-199905010-00005. [DOI] [PubMed] [Google Scholar]
- McCaffery K, Waller J, Nazroo J, Wardle J. Social and psychological impact of HPV testing in cervical screening: a qualitative study. Sexually Transmitted Infections. 2006;82:169–174. doi: 10.1136/sti.2005.016436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore AL, Sabin CA, Madge S, Mocroft A, Reid W, Johnson MA. Highly active antiretroviral therapy and cervical intraepithelial neoplasia. AIDS. 2002;16(6):927–929. doi: 10.1097/00002030-200204120-00014. [DOI] [PubMed] [Google Scholar]
- Norazian MN, Ahmad Shukri Y, Ramli NA, Mustafa AA. Comparison of Linear Interpolation Method and Mean Method to Replace the Missing Values in Environmental Data Set. In Proceeding International Conference on Sustainable Management (ICOSM); Jun 9–11, 2007. ISBN 9789834235826. [Google Scholar]
- Palefsky JM. Cervical human papillomavirus infection and cervical intraepithelial neoplasia in women positive for human immunodeficiency virus in the era of highly active antiretroviral therapy. Current Opinion in Oncology. 2003;15:382–388. doi: 10.1097/00001622-200309000-00007. [DOI] [PubMed] [Google Scholar]
- Patterson TL, Semple SJ, Temoshok LR, Atkinson JH, McCutchan JA, Straits-Troster K, Grant I. Stress and depressive symptoms prospectively predict immune change among HIV-seropositive men. Psychiatry. 1995;58:299–312. doi: 10.1080/00332747.1995.11024735. [DOI] [PubMed] [Google Scholar]
- Pereira DB. Interventions for mothers during pregnancy and postpartum: behavioral and pharmacological approaches. In: Chesney M, Antoni MH MH, editors. Innovative approaches to health psychology: prevention and treatment—Lessons learned from AIDS. American Psychological Association Press; Washington, D.C.: 2002. [Google Scholar]
- Potts RG. Spirituality and the experience of cancer in an African-American community: Implications for psychosocial oncology. Journal of Psychosocial Oncology. 1996;14:1–17. [Google Scholar]
- Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in simple and multiple mediator models. Behavior Research Methods. 2008;40:1–51. 879–891. doi: 10.3758/brm.40.3.879. [DOI] [PubMed] [Google Scholar]
- Sellmeyer D, Grunfeld C. Endocrine and metabolic disturbances in human immunodeficiency virus infection and the acquired immune deficiency syndrome. Endocrine Reviews. 1996;17:518–532. doi: 10.1210/edrv-17-5-518. [DOI] [PubMed] [Google Scholar]
- Siegel K, Schrimshaw E. Stress, appraisal, and coping: A comparison of HIV-infected women in the pre-HAART and HAART eras. Journal of Psychosomatic Research. 2005;58:225–233. doi: 10.1016/j.jpsychores.2004.09.002. [DOI] [PubMed] [Google Scholar]
- Stentella P, Frega A, Ciccarone M, Cipriano L, Tinari A, Tzantzoglou S, Pachi A. HPV and intraepithelial neoplasia recurrent lesions of the lower genital tract: assessment of the immune system. European Journal of Gynecological Oncology. 1998;19:466–469. [PubMed] [Google Scholar]
- Tachezy R, Salakova M, Hamsikova E, Kanka J, Havrankova A, Vonka V. Prospective study on cervical neoplasia: presence of HPV DNA in cytological smears precedes the development of cervical neoplastic lesions. Sexually Transmitted Infection. 2003;79:191–196. doi: 10.1136/sti.79.3.191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woo YL, Sterling J, Damay I, Coleman N, Crawford R, Van der Burg SH, Stanley M. Characterising the local immune responses in cervical intraepithelial neoplasia: a cross-sectional and longitudinal analysis. British Journal of Obstetrics and Gynecology. 2008;115:1616–1621. doi: 10.1111/j.1471-0528.2008.01936.x. [DOI] [PubMed] [Google Scholar]
- Yanez B, Edmondson D, Stanton A, Park C, Kwan L, Ganz P, Blank TO. Facets of spirituality as predictors of adjustment to cancer: Relative contributions of having faith and finding meaning. Journal of Consulting and Clinical Psychology. 2009;77(4):730–741. doi: 10.1037/a0015820. [DOI] [PMC free article] [PubMed] [Google Scholar]