

Abstract
It is nowadays accepted that, independently of methodological issues, women commit fewer suicides than men but make more frequent attempts. Yet, female suicidal risk varies greatly along the lifetime and is linked to the most significant moments in it. A wide analysis of the existing literature was performed to provide a narrative description on the evolution of female suicidal rates from childhood to old age, considering the milestones in their life history. A detailed analysis of gender differences in suicidal behavior is key to establish preventive measures and priorities. More specific studies are needed to adapt future interventions on female suicide.
1. Introduction
A vast majority of epidemiological studies performed in diverse cultures and countries show gender differences in suicidal behavior. In developed countries, the completed suicides are 2 to 4-fold more frequent among men [1–3], while suicide attempts are 2 to 3-fold more frequent among women [4–6]. However, suicide rates vary significantly between regions and countries. In Europe, northern countries report higher suicide rates [7]. Developed countries have higher male to female ratios than Asian countries [8, 9], although the estimated global male/female suicide ratio is 1.67 to 1 and not 3 to 1 [10]. Young women may be particularly exposed to suicidal risk [6, 11]. For instance, during 2005 suicide was the fourth cause of death in the United States (US) among women aged 15–44 years [12]. The rates of suicidal ideation and attempts among females are notably increased after puberty [13]. It has been calculated that in the US a woman attempts suicide every 78 seconds and dies of it every 90 minutes [14].
The higher frequency of completed suicides among men and suicide attempts among women is called the gender paradox and has been reported on many different countries. This paradox is absent in India and China where women and men present similar suicide rates [10, 15] due to the high rates of completed suicide among rural young women [16, 17]. In addition, suicide among Indian and Chinese women may be favored by the use of lethal methods such as self-burning in India and pesticides in China [17–19]. It is of note that female suicide rates in South Korea have increased from 1.1 (1986) to 4.2 (2005) per 100.000 [20]. The limitations to obtain national suicide data from undeveloped countries remark the presumed importance of cultural dimensions. It must be remembered that WHO counts with trustworthy information on death causes covering about 13% of the world population and actualized mortality data on 25% of the world population is lacking [21].
Not considered to be a methodological artifact [4], a lack of agreement on the origin of the gender paradox persists. Proposed explanations are based on the differential suicidal methods, which may condition lethality, disposal, and cultural acceptance [3, 22]. Usually, males use methods such as shooting by firearm, hanging, or suffocation, while females attempt poisoning, wrist cutting, or falling from heights [2]. Durkheim [23] suggested that suicide is influenced by individual traits but also by the characteristics and changes of the society. Males appear to be more affected by external factors, such as economic crisis, than females [24–27].
The study of sexual dimorphism is constraint by the variations of risk factors between generations. For example, McIntosh [28] analyzed the rates of suicide between baby-boomers (born in the 1943–1960 period) and the 13th generation (born in the 1961–1981 period) in the US. Following his results, the suicidal risk is increased among subjects of the 13th generation when considering the same chronological age. Some authors have informed as well on a reduction in the global rates of suicide in recent years, especially among aged women and despite a subtle increase among young men [29]. The WHO/EURO multicentre study [30] reported that suicide rates had diminished by 17% among men and 14% among women from 1989 to 1992. Others point out that the gender rate of completed suicide in the USA has remained stable around 2.5 : 1 (2.5 fold more frequent completed suicides among men) from 1930 to 1971, but has increased ever since reaching a proportion of 4.4 : 1 in the last decade of the nineties [14]. Nevertheless, studies analyzing different time periods in developed countries found that the suicide rate in women has increased over time [31, 32].
Besides, global ratios may conceal bigger differences among gender during the vital cycle. Hawton and Harriss [33] analyzed a large sample of self-aggressions admitted to the hospital in a 10-year interval. Gender ratio was globally close to 1.5 women for each man. However, this coefficient varied greatly between age groups and decreased with advancing age, from 8:1 among the younger (10–14 years of age) to 0.8:1 among the elder (>50 years of age).
The present study is focused on the longitudinal evolution of the suicidal behavior in women and particularly at some significant moments of women's lifetime: childhood/adolescence, reproductive cycle/pregnancy, middle-aged/marital status, and old age (see Figure 1 and Table 1).
Figure 1.
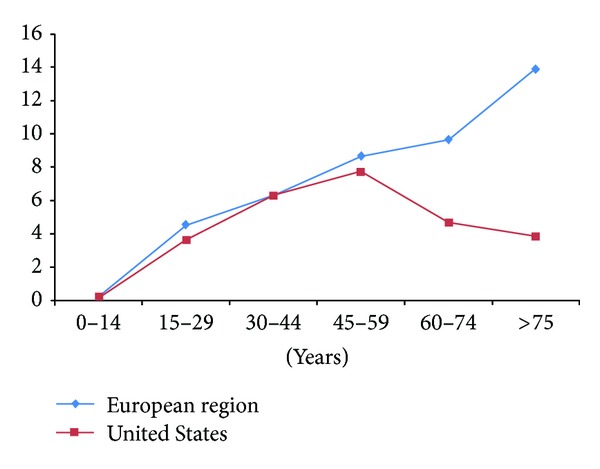
Evolution of female suicide rates in Europe and the United States 1999–2010 (Source: http://data.euro.who.int/hfamdb/, http://webappa.cdc.gov/sasweb/ncipc/mortrate10_us.html)
Table 1.
Female suicide across the life cycle: main studies.
| Authors | Population | Main results |
|---|---|---|
| Childhood, adolescence, and youth women | ||
|
| ||
| Biddle et al., [50] | England and Wales, 1968–2005. Men and women aged 15–34 years | Suicide rates stability over time. In the 21st century recording lowest rate |
| Grøholt et al., [41] | Norway, 1990–1992. All suicide in people under 20 years | Teenage girls suicide victims died mainly by hanging. They were more often affected by problems with parents, wrote farewell note, and had previous suicide attempts |
| Eaton et al., [37] | Youth Risk Behavior Surveillance System (YRBSS) USA, 2007. 1268 primary students | Adolescent women from 13 years of age show an abrupt increase of suicidal ideation, plans, and attempts |
| Gunnell et al., [48] | Mortality data England and Wales, 1950–1998 | Suicide rates decreases in women aged over 45 years. Risk greater in women aged 25–34 years associated to participation in the workforce |
| Lewinsohn et al., [43] | USA (Western Oregon), 1987–1989. 1709 adolescents (aged 14–18) | Suicide attempts hazard rate in female adolescents greater than males adolescents. Adolescent suicidal behavior predicted suicide attempts during young adulthood for females |
|
| ||
| Role of reproductive cycle and maternity | ||
|
| ||
| Appleby, [61] | England and Wales, 1973–1984. Women aged 15–44 years committed suicide in the year after childbirth or during pregnancy | Women in the first year after childbirth or during pregnancy have a low-risk suicide despite their high rate of psychiatry morbidity women who committed suicide after childbirth most often did at the first month |
| Czeizel, [71] | Budapest, 1960–1993. 1044 pregnant women aged 14–44 years | Maximum number of suicide attempts in pregnant women occurs in the group from 18 to 20 years. Most unplanned pregnancies and main method used poisoning |
| Da silva et al., [65] | Brazil, 2006–2008. 1414 women pregnant treated in the public health system | There is greater suicidality in pregnant women who have depressive and anxiety symptoms |
| Gissler et al., [68] | Finland, 1987–1994. 1347 women aged 15–49 years that committed suicide | The risk of suicide was at its highest during the first two months after the end of pregnancy and mainly in the age group 35–39 years |
| Samandari et al., [85] | North Carolina surveillance and vital statistics data from 2004–2006. Women reproductive age, 14–44 years | Greater percentages of pregnant/postpartum suicide victims never married compared to no pregnant/no postpartum suicide victims |
|
| ||
| Middle-aged women | ||
|
| ||
| Burrows et al., [31] | Canada (Québec), 1990–2005. People 10 years and older | Suicide mortality in women increases in the time. Rate suicide is highest between 25 and 44 years (2002–2005) |
| Bramness et al., [87] | Norwegian, 1994–2007. 131362 people (69774 women) aged 39–44 years | More self-report mental health problems among females than males. Increased risk of suicide with higher self-report depressive and anxiety symptoms |
| Cutright et al., [88] | Suicide rates of married and not married females in 12 developed countries, 1960 | The suicide rate is higher in not married females mainly age group 35–44 years. Being married is a protective factor. |
| Karch et al., [2] | United States, 2009. National Violent Death Reporting System (NVDRS). 15981 fatal incidents (60.6% suicides) | Females among ages 35 and 64 years accounted for 64.8% of suicides. Rates suicide for females peaked at 9.1 per 100,000 among those aged 45–54 years |
| White and Holmes, [89] | Mortality database WHO, men and women aged 15–44 years across 44 countries | Suicide rate in women increases with age. Group 15–24 years (14.1), group 25–34 years (21.7), and group 35–44 years (23.8) |
|
| ||
| Oldest women | ||
|
| ||
| Erlangsen et al., [90] | Danish population, 1994–1998. People 50 years or above | During first year of widowhood the suicide risk increases in ages over 80 years. The highest rate of suicide is reached in the group 65–79 years and then declines over 80 years |
| Klein et al., [53] | Switzerland (Canton), 1995–2007. 3431 cases of suicide | Suicide risk increases with age. Women's group of the 50–89 years rates the highest. Main methods used poisoning, hanging, and firearm |
| Pridemore and Spivak, [27] | Mortality date Russian, 1965–1999 | Suicide rates increased about 17% in the last three decades. Suicide rate in women increases with age reaching its peak over 80 years. Risk factor in females that reside alone |
| Wanta et al., [91] | Wisconsin's. USA, 2001–2006. People over 65 years | The suicide rates in women decrease with age. Protective factor is being married. |
| Zeppegno et al., [92] | Date on suicide in Italy (Novara and Verbania), 1990–2000. People 65 and older years | Suicide rates in women increase over 74 years. Greater risk of suicide in divorced, widowed, and single |
2. Suicidal Behavior in Childhood, Adolescence, and Youth
Infantile suicide is an unusual occurrence. However, the number of suicides among children and adolescents till 14 years of age appears to be increasing in several countries. Rates are varying from 0 to 3.1/100000 between countries with an estimated 0.6/100000 global rate and a 2 : 1 male/female coefficient [34]. These rates rise towards adolescence due to a greater planning and more lethal suicide attempts, and together with a higher prevalence of mental disorders and substance abuse [35, 36].
Some studies observed the gender paradox among subjects aged 10–19 years. Adolescent women from 13 years of age show an abrupt increase of suicidal ideation, plans, and attempts [37]. The rates of suicidal ideation and attempts are consistently increased after puberty among females when compared to male adolescents [13, 38]. The highest rates of suicide attempts [39] or parasuicides [40] appear earlier in adolescent women compared to men, with a time gap of about 3 years [39]. In addition, teenage girls that committed suicide more often had previous attempts and conflicts with their parents and left a note than male groups [41, 42]. Suicidal behavior among female adolescents should be a worrying problem for institutions and researchers [43].
Suicide is the third leading cause of death for persons aged 10–14 years and 15–24 years, the second leading cause for persons aged 25–34 years in the US [2], and the second cause of mortality after accidental deaths in Europe [44]. According to a recent study on 14738 suicides committed in 15 European countries among youths aged 15–24 years, men had a 3.7-fold higher risk of completed suicide than women [3]. Some authors have suggested that this difference between male and female adolescents is due to methodological issues, such as an overrepresentation of male subjects in the group of suicides aged 15–19 years [45]. However, gender differences could be explained by greater levels of aggression, more frequent substance use disorders, and more lethal methods in males than females [35, 46]. This situation changes when considering Asian countries, for instance in Hong Kong the suicide rates (per 100000) among persons aged 15–19 were 5.1 for males and 5.2 for females [47]. Gunnell et al. [48] showed that although the suicide rate in England and Wales is still higher in men, the difference in recent years has decreased compared to women (1950–1998). Suicide is also the world leading cause of death in women aged 15–24 years, mainly in low-income and middle-income countries, according to Patton et al. [49]. In addition, suicides by hanging/suffocation may be augmenting among U.S. women aged 15–34 years [50] and 10–19 years [51]. Åsgård et al. [52] analyzed the causes of death in Sweden from 1952 to 1981, finding a tendency towards lower ages and higher female suicidal risk along this period.
Brent et al. [35] have compared several studies on psychological autopsies among adolescents with their own sample. They found that females used generally less lethal means, such as self-poisoning by overdose, with a more frequent prevalence of affective disorders and previous attempts. However, adolescent women who commit suicide may use increasingly violent methods such as shooting by firearms or hanging [41]. Klein et al. [53] found that the method most commonly used in the 10–19 years group was jumping form a height, while the 20–49 age group used other methods such as poisoning, hanging, strangulation, suffocation, or drowning. Other studies in western populations found that the most common suicidal methods in women aged 10–24 years were hanging/suffocation, drug poisoning, and jumping [3, 54]. Thus, if women used more lethal means the gender difference in suicide rates could be reduced [55]. However, the highest suicidal risk among female adolescents precede 2-3 years that of male adolescents, and by 19 years of age the risk is similar [43]. Saunders and Hawton [56] suggested that the initiation of menarche is the moment when gender differences in the ratios of affective disorders and suicide behavior move apart.
3. Role of Reproductive Cycle and Maternity
Consistent evidence of an association between menstrual phase and completed suicide has not been found [56]. Non-fatal suicidal behavior and suicidal ideation seem to be more frequent when estrogen levels are lowest during the menstrual cycle, in particular the late luteal and follicular phases [56–58]. Besides, suicide attempters have shown higher prevalence of premenstrual symptoms and premenstrual dysphoric disorder than the general population [57].
Several studies seem to confirm that maternity plays a more important role than marriage in the decreased risk for completed suicide among middle-aged women when compared to men. Actually, mothers having more children show an enhanced protection [59]. Being pregnant [33] and having a child of less than two years of age [60] have also been associated with lower suicidal risk. Moreover, as the age of the youngest child diminishes, suicide risk is reduced to a greater extent [59]. Women living with a partner and children that changed to living with only a partner were overrepresented among parasuicidal women in the WHO study [30].
Different authors support the idea that the birth of a child is a protective factor against fatal and non-fatal self-harm, especially in the first year after delivery [59, 61, 62]. However, this protective function differs in pregnant women with psychiatric disorders. Between 10–25% of pregnant and postpartum women experience depressive disorders [63, 64] or anxiety disorders [65, 66]. These women are more likely to complete suicide, especially within the two first months of the postpartum [67, 68]. In addition, pregnant teens represent a high risk group, with an estimated 16–44% prevalence rate of depression [69, 70]. Teen mothers are more likely to present suicidal thoughts, or attempts especially if it is the first pregnancy or if the pregnancy is unplanned [71–74].
Suicide is the fourth cause of maternal deaths in the world [75] and the leading cause of death in first-year postpartum women in the United Kingdom [76, 77]. The risk of suicide was calculated to be 70 times higher in women with psychiatric disorders during the first year after childbirth compared to the general female population [78]. In the same vein, Gissler et al. [68] reported a suicide rate of 11 per 100.000 in a large sample of Finnish postpartum women. In this study, suicide rates associated with childbirth were close to half of those among non-pregnant women aged 15–49 years, but adolescent mothers were three times more likely to commit suicide than other females in their age group.
Suicidal behavior and suicide rates may be increased after an abortion, particularly when induced [79, 80]. In fact, induced abortion may increase suicidal risk in relation with the impact of the decision itself, because prior to the abortion no difference in suicidal risk was found with women completing their pregnancy [81]. However, findings on mental health consequences of abortion have been contested, and the recent literature review limited the validity of studies to date [82].
Miscarriage has also been linked to an increased maternal suicide risk [68, 81]. Other factors associated with an increased risk of suicide in pregnant women and after childbirth were single, unmarried, or divorced marital status, low income, having thoughts about abortion, unemployment, occupational instability, and poor social support [65, 83–85]. Finally, another dimension associated with female suicide but less studied is infertility. Kjaer et al. [86] found in a sample of 51221 Danish women, that those who succeeded in the treatment of infertility had half the risk of suicide than the unsuccessful ones.
4. Suicide in Middle-Aged Women, Marriage, and Divorce
In the US, female suicide is concentrated in the 35–64 years age group (64.8%), with a 9.1/100000 peak between those aged 45–54 years [2]. Similar results have been reported for England and Wales [25]. Societal changes lead many women in this age group to become economically active, maybe increasing the risk of suicide among them [48, 93] as well as the mental health problems [87]. From 50 years of age, the suicide rates among women tend to diminish progressively [4, 94] till old age, when rates start increasing again (Figure 1). White and Holmes [89] found that suicide rate in women increases with age reaching its peak at 35–44 years. Yet, depression and suicide ideation have been associated with the perimenopause phase in women when compared to premenopausal and postmenopausal [95].
According to the exist literature, married women are less prone to suicide than single, divorced, and widowed women [88]. Never-married, divorced, or widowed women conduct most suicides (60.4%) in the US [2]. Cutright et al. [88] analyzed retrospective data from 12 developed countries to explain the differences in suicide between married and non-married women. They concluded that the compatibility of marital status with the corresponding age group was the best explanation of these differences, but the results were limited by not considering the influence of maternity. Divorce affects in a singular way the risk of suicide among women. They present lower suicide rates after divorce than men, but the gender protection seems to decrease with advancing age [96].
5. Suicidal Behavior among the Oldest Women: Death of Partner or Child
Advanced age seems to increase the divergence between sexes in the rate of completed suicide among the elder [22]. Whereas suicide attempt rates diminish with age independently of gender [97], the rates of completed suicide augment with age [92]. This increase is particularly prominent among men [53] reaching 6–12 times higher rates than women in western countries [98]. This important difference has been attributed to a better planning, fewer warnings of suicidal intent, and the use of more lethal methods, mainly firearms and hanging/suffocation [91, 98–100]. However, the male to female suicide ratio did not change in Eastern Europe or South America in the group aged over 65 years [101], and it even decreased in the US [6].
Female suicide rates in western countries increase with advancing age until they reach a peak around menopause. However, the evolution of suicide rates among older women may vary greatly depending on the country. In Europe they appear to continue their growth at a lower pace but sustainable increased in the oldest age groups (Figure 1) [53, 102], and similar results have been reported in Russia [27], Korea [103], and China [104]. The Centers for Disease Control and Prevention (CDC) report a declining trend in the US, 5.8 for those aged 60–69 years, 4.2 for those aged 70–79 years, and 2.7 for those aged over 80 years [2]. The largest differences between Europe and the US with regards to female suicide rates are seen in this group of age (Figure 1), although longitudinal trends show an approximation in the rates of both regions in recent years (Figure 2).
Figure 2.
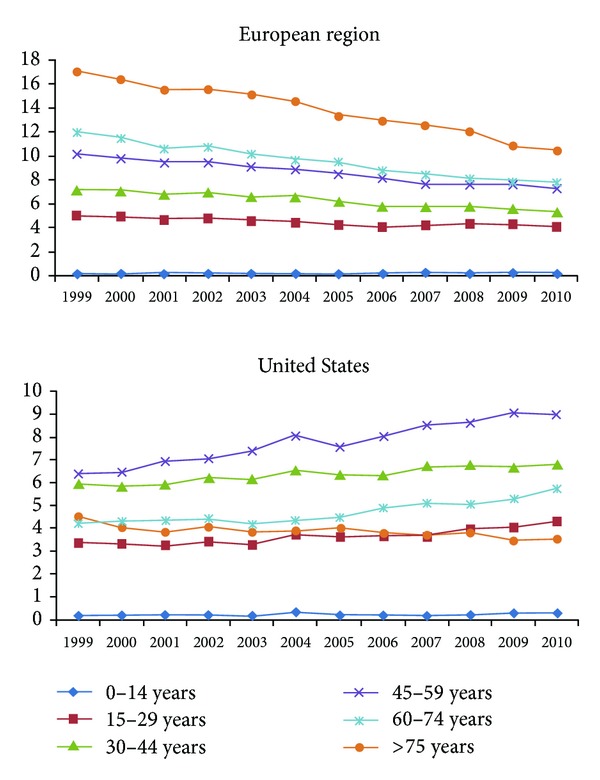
Comparison of longitudinal trends in female suicide rates between Europe and the United States 1999–2010. Source: http://data.euro.who.int/hfamdb/, http://webappa.cdc.gov/sasweb/ncipc/dataRestriction_inj.html.
Widowed, divorced, and never married old women are at greater risk of completing suicide [91, 92]. The death of the partner occupies a prominent place to explain the high rates of suicide they present. Following the work by Erlangsen et al. [90] old persons present a 15-fold higher risk of suicide after the loss of their partner than middle-aged persons. Though women are also affected, suicide rates and time needed for recovery are particularly increased among men. In an interesting study by Agerbo [105], conjugal bereavement was found to raise spousal suicide risk, and especially when death had been the result of a suicide. He also found that suicide risk when other causes produced the death of the partner was three-fold higher among men than among their feminine counterpart. Some studies found that the main methods used to completed suicide by this age group are poisoning and firearms [53, 98].
Parental suicide risk is highly influenced by the loss of a child [59]. Risk is enhanced in the first month after the death, with younger age of the child or if result of a suicide [59]. The increased risk of suicide is independent of gender, but having another child constitutes a protective factor for the mother [105].
6. Conclusions
Suicidal behavior presents important differences between men and women. Men are more prone to completed suicide but women have more frequent suicide attempts. It is nowadays accepted that this fact is independent of methodological issues. Several hypotheses have been proposed to explain this difference; some of them underline biological aspects, while others focus mainly on the feminine role and psychosocial aspects of gender. In any case, gender is one of the most frequently replicated predictors of suicide, and a detailed analysis of gender differences in suicidal behavior is important to establish preventive measures and priorities. Besides, suicide risk is not regular along the female lifecycle and the literature revision revealed large cross-national differences. Intervention on suicide must therefore be adapted specifically to the different populations. Studies analyzing the evolution of suicidal behavior in women and associated factors in the most significant milestones of their life history are needed.
The evolution of female suicide rates in Europe and the United States diverges in the 1999–2010 period. Suicide rates increase in the old age among European women, while an opposite trend for that age period is seen in the U.S. (Figure 1). Consequently, the longitudinal trends show the highest suicide rates in European women over 75 years, while the highest rates in the US correspond to women of 45–59 years of age (Figure 2). These differences demonstrate the importance of cultural and sociodemographic variables in the analysis and should be considered for the development and implementation of prevention programs.
Conflict of Interests
The authors declares no conflict of interests.
Acknowledgment
J. Lopez-Castroman was supported by a Fundamental Foundation research grant for this study.
References
- 1.Denney JT, Rogers RG, Krueger PM, Wadsworth T. Adult suicide mortality in the United States: marital status, family size, socioeconomic status, and differences by sex. Social Science Quarterly. 2009;90(5):1167–1185. doi: 10.1111/j.1540-6237.2009.00652.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Karch DL, Logan J, McDaniel D, Parks S, Patel N. Surveillance for violent deaths—National Violent Death Reporting System, 16 states, 2009. Morbidity and Mortality Weekly Report. Surveillance Summaries. 2008;61(6):1–43. [PubMed] [Google Scholar]
- 3.Värnik A, Kõlves K, Allik J, et al. Gender issues in suicide rates, trends and methods among youths aged 15–24 in 15 European countries. Journal of Affective Disorders. 2009;113(3):216–226. doi: 10.1016/j.jad.2008.06.004. [DOI] [PubMed] [Google Scholar]
- 4.Canetto SS, Sakinofsky I. The gender paradox in suicide. Suicide & Life-Threatening Behavior. 1998;28(1):1–23. [PubMed] [Google Scholar]
- 5.Bertolote JM, Fleischmann A, De Leo D, et al. Suicide attempts, plans, and ideation in culturally diverse sites: the WHO SUPRE-MISS community survey. Psychological Medicine. 2005;35(10):1457–1465. doi: 10.1017/S0033291705005404. [DOI] [PubMed] [Google Scholar]
- 6.Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, Lee S. Suicide and suicidal behavior. Epidemiologic Reviews. 2008;30(1):133–154. doi: 10.1093/epirev/mxn002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hawton K, van Heeringen K. Suicide. The Lancet. 2009;373(9672):1372–1381. doi: 10.1016/S0140-6736(09)60372-X. [DOI] [PubMed] [Google Scholar]
- 8.World Health Organization. World Report on Violence and Health. Geneva, Switzerland: World Health Organization; 2012. http://www.who.int/violence_injury_prevention/violence/world_report/chapters/en/index.html. [Google Scholar]
- 9.Yip PSF. Suicide in Asia. Causes and Prevention. Hong Kong: Hong Kong University Press; 2008. [Google Scholar]
- 10.Phillips MR, Cheng HG. The changing global face of suicide. The Lancet. 2012;379(9834):2318–2319. doi: 10.1016/S0140-6736(12)60913-1. [DOI] [PubMed] [Google Scholar]
- 11.Baca-Garcia E, Perez-Rodriguez MM, Keyes KM, et al. Suicidal ideation and suicide attempts in the United States: 1991-1992 and 2001-2002. Molecular Psychiatry. 2010;15(3):250–259. doi: 10.1038/mp.2008.98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Centers for Disease Control and Prevention (CDC) Web-based injury statistics query and reporting system. 2009, http://www.cdc.gov/injury/wisqars/index.html.
- 13.Grunbaum JA, Kann L, Kinchen S, et al. Youth risk behavior surveillance—United States, 2003. Morbidity and Mortality Weekly Report. Surveillance Summaries. 2004;53(2):1–96. [PubMed] [Google Scholar]
- 14.American Foundation for Suicide Prevention (AFSP) Facts and Figures about Suicide. 1998, http://www.afsp.org/
- 15.Soman CR, Safraj S, Kutty V, Vijayakumar K, Ajayan K. Suicide in South India: a community-based study in Kerala. Indian Journal of Psychiatry. 2009;51(4):261–264. doi: 10.4103/0019-5545.58290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sudhir Kumar CT, Mohan R, Ranjith G, Chandrasekaran R. Gender differences in medically serious suicide attempts: a study from South India. Psychiatry Research. 2006;144(1):79–86. doi: 10.1016/j.psychres.2005.11.012. [DOI] [PubMed] [Google Scholar]
- 17.Yip PSF, Liu KY. The ecological fallacy and the gender ratio of suicide in China. The British Journal of Psychiatry. 2006;189:465–466. doi: 10.1192/bjp.bp.106.021816. [DOI] [PubMed] [Google Scholar]
- 18.Gunnell D, Eddleston M, Phillips MR, Konradsen F. The global distribution of fatal pesticide self-poisoning: systematic review. BMC Public Health. 2007;7, article 357 doi: 10.1186/1471-2458-7-357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kumar V. Burnt wives—a study of suicides. Burns. 2003;29(1):31–35. doi: 10.1016/s0305-4179(02)00235-8. [DOI] [PubMed] [Google Scholar]
- 20.Kwon JW, Chun H, Cho SI. A closer look at the increase in suicide rates in South Korea from 1986–2005. BMC Public Health. 2009;9, article 72 doi: 10.1186/1471-2458-9-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.World Health Organization. Quality of cause-of-death information: a challenge in large part of the world. 2007, http://www.who.int/research/cod_info_quality_20071005.pdf.
- 22.Canetto SS. Women and suicidal behavior: a cultural analysis. American Journal of Orthopsychiatry. 2008;78(2):259–266. doi: 10.1037/a0013973. [DOI] [PubMed] [Google Scholar]
- 23.Durkheim E. Suicide. New York, NY, USA: Free Press; 1897. [Google Scholar]
- 24.Chung A. Gender difference in suicide, household production and unemployment. Applied Economics. 2009;41(19):2495–2504. [Google Scholar]
- 25.Thomas K, Gunnell D. Suicide in England and Wales 1861—2007: a time-trends analysis. International Journal of Epidemiology. 2010;39(6):1464–1475. doi: 10.1093/ije/dyq094. [DOI] [PubMed] [Google Scholar]
- 26.McPhedran S, Baker J. Recent Australian suicide trends for males and females at the national level: has the rate of decline differed? Health Policy. 2008;87(3):350–358. doi: 10.1016/j.healthpol.2008.01.009. [DOI] [PubMed] [Google Scholar]
- 27.Pridemore WA, Spivak AL. Patterns of suicide mortality in Russia. Suicide & Life-Threatening Behavior. 2003;33(2):132–150. doi: 10.1521/suli.33.2.132.22771. [DOI] [PubMed] [Google Scholar]
- 28.McIntosh JL. Generational analyses of suicide: baby Boomers and 13ers. Suicide & Life-Threatening Behavior. 1994;24(4):334–342. [PubMed] [Google Scholar]
- 29.Fekete S, Voros V, Osvath P. Gender differences in suicide attempters in Hungary: retrospective epidemiological study. Croatian Medical Journal. 2005;46(2):288–293. [PubMed] [Google Scholar]
- 30.Schmidtke A, Bille-Brahe U, DeLeo D, et al. Attempted suicide in Europe: rates, trends and sociodemographic characteristics of suicide attempters during the period 1989-1992. Results of the WHO/EURO Multicentre Study on Parasuicide. Acta Psychiatrica Scandinavica. 1996;93(5):327–338. doi: 10.1111/j.1600-0447.1996.tb10656.x. [DOI] [PubMed] [Google Scholar]
- 31.Burrows S, Auger N, Roy M, Alix C. Socio-economic inequalities in suicide attempts and suicide mortality in Québec, Canada, 1990–2005. Public Health. 2010;124(2):78–85. doi: 10.1016/j.puhe.2010.01.008. [DOI] [PubMed] [Google Scholar]
- 32.Hansen L, Pritchard C. Consistency in suicide rates in twenty-two developed countries by gender over time 1874–78, 1974–76, and 1998–2000. Archives of Suicide Research. 2008;12(3):251–262. doi: 10.1080/13811110802101153. [DOI] [PubMed] [Google Scholar]
- 33.Hawton K, Harriss L. The changing gender ratio in occurrence of deliberate self-harm across the lifecycle. Crisis. 2008;29(1):4–10. doi: 10.1027/0227-5910.29.1.4. [DOI] [PubMed] [Google Scholar]
- 34.Dervic K, Brent DA, Oquendo MA. Completed suicide in childhood. Psychiatric Clinics of North America. 2008;31(2):271–291. doi: 10.1016/j.psc.2008.01.006. [DOI] [PubMed] [Google Scholar]
- 35.Brent DA, Baugher M, Bridge J, Chen T, Chiappetta L. Age- and sex-related risk factors for adolescent suicide. Journal of the American Academy of Child & Adolescent Psychiatry. 1999;38(12):1497–1505. doi: 10.1097/00004583-199912000-00010. [DOI] [PubMed] [Google Scholar]
- 36.Grøholt B, Ekeberg Ø, Wichstrøm L, Haldorsen T. Suicide among children and younger and older adolescents in Norway: a comparative study. Journal of the American Academy of Child & Adolescent Psychiatry. 1998;37(5):473–487. doi: 10.1097/00004583-199805000-00008. [DOI] [PubMed] [Google Scholar]
- 37.Eaton DK, Kann L, Kinchen S, et al. Youth risk behavior surveillance—United States, 2007. Morbidity and Mortality Weekly Report. Surveillance Summaries. 2008;57(4):1–131. [PubMed] [Google Scholar]
- 38.Eaton DK, Kann L, Kinchen S, et al. Youth risk behavior surveillance—United States, 2005. Journal of School Health. 2006;76(7):353–372. doi: 10.1111/j.1746-1561.2006.00127.x. [DOI] [PubMed] [Google Scholar]
- 39.Levinson D, Haklai Z, Stein N, Gordon ES. Suicide attempts in Israel: age by gender analysis of a national emergency departments database. Suicide & Life-Threatening Behavior. 2006;36(1):97–102. doi: 10.1521/suli.2006.36.1.97. [DOI] [PubMed] [Google Scholar]
- 40.Welch SS. A review of the literature on the epidemiology of parasuicide in the general population. Psychiatric Services. 2001;52(3):368–375. doi: 10.1176/appi.ps.52.3.368. [DOI] [PubMed] [Google Scholar]
- 41.Grøholt B, Ekeberg Ø, Wichstrøm L, Haldorsen T. Sex differences in adolescent suicides in Norway, 1990–1992. Suicide & Life-Threatening Behavior. 1999;29(4):295–308. [PubMed] [Google Scholar]
- 42.Shaffer D, Garland A, Gould M, Fisher P, Trautman P. Preventing teenage suicide: a critical review. Journal of the American Academy of Child & Adolescent Psychiatry. 1988;27(6):675–687. doi: 10.1097/00004583-198811000-00001. [DOI] [PubMed] [Google Scholar]
- 43.Lewinsohn PM, Rohde P, Seeley JR, Baldwin CL. Gender differences in suicide attempts from adolescence to young adulthood. Journal of the American Academy of Child & Adolescent Psychiatry. 2001;40(4):427–434. doi: 10.1097/00004583-200104000-00011. [DOI] [PubMed] [Google Scholar]
- 44.Blum RW, Nelson-Mmari K. The health of young people in a global context. Journal of Adolescent Health. 2004;35(5):402–418. doi: 10.1016/j.jadohealth.2003.10.007. [DOI] [PubMed] [Google Scholar]
- 45.Centers for Disease Control and prevention and prevention (CDC) Suicide Trends Among Youths and Young Adults Aged 10–24 Years—United States, 1990–2004. 2007, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5635a2.htm. [PubMed]
- 46.Hawton K, Hall S, Simkin S, et al. Deliberate self-harm in adolescents: a study of characteristics and trends in Oxford, 1990–2000. Journal of Child Psychology and Psychiatry and Allied Disciplines. 2003;44(8):1191–1198. doi: 10.1111/1469-7610.00200. [DOI] [PubMed] [Google Scholar]
- 47.WHO Statistical Information System. WHO mortality database. 2005, http://www.who.int/whosis/en/
- 48.Gunnell D, Middleton N, Whitley E, Dorling D, Frankel S. Why are suicide rates rising in young men but falling in the elderly? A time-series analysis of trends in England and Wales 1950–1998. Social Science & Medicine. 2003;57(4):595–611. doi: 10.1016/s0277-9536(02)00408-2. [DOI] [PubMed] [Google Scholar]
- 49.Patton GC, Coffey C, Sawyer SM, et al. Global patterns of mortality in young people: a systematic analysis of population health data. The Lancet. 2009;374(9693):881–892. doi: 10.1016/S0140-6736(09)60741-8. [DOI] [PubMed] [Google Scholar]
- 50.Biddle L, Brock A, Brookes ST, Gunnell D. Suicide rates in young men in England and Wales in the 21st century: time trend study. British Medical Journal. 2008;336(7643):539–542. doi: 10.1136/bmj.39475.603935.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Lubell KM, Kegler SR, Crosby AE, Karch D. Suicide trends among youths and young adults aged 10–24 years—United States, 1990–2004. Morbidity and Mortality Weekly Report. 2007;56(35):905–908. [PubMed] [Google Scholar]
- 52.Åsgård U, Nordström P, Råbäck G. Birth cohort analysis of changing suicide risk by sex and age in Sweden 1952 to 1981. Acta Psychiatrica Scandinavica. 1987;76(4):456–463. doi: 10.1111/j.1600-0447.1987.tb05631.x. [DOI] [PubMed] [Google Scholar]
- 53.Klein SD, Bischoff C, Schweitzer W. Suicides in the Canton of Zurich. Swiss Medical Weekly. 2010;140(NOVEMBER):p. 35. doi: 10.4414/smw.2010.13102. [DOI] [PubMed] [Google Scholar]
- 54.Bridge JA, Greenhouse JB, Sheftall AH, Fabio A, Campo JV, Kelleher KJ. Changes in suicide rates by hanging and/or suffocation and firearms among young persons aged 10–24 years in the United States: 1992–2006. Journal of Adolescent Health. 2010;46(5):503–505. doi: 10.1016/j.jadohealth.2009.11.206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Beautrais AL. Suicide and serious suicide attempts in youth: a multiple-group comparison study. The American Journal of Psychiatry. 2003;160(6):1093–1099. doi: 10.1176/appi.ajp.160.6.1093. [DOI] [PubMed] [Google Scholar]
- 56.Saunders KEA, Hawton K. Suicidal behaviour and the menstrual cycle. Psychological Medicine. 2006;36(7):901–912. doi: 10.1017/S0033291706007392. [DOI] [PubMed] [Google Scholar]
- 57.Baca-Garcia E, Diaz-Sastre C, Ceverino A, et al. Premenstrual symptoms and luteal suicide attempts. European Archives of Psychiatry and Clinical Neuroscience. 2004;254(5):326–329. doi: 10.1007/s00406-004-0506-1. [DOI] [PubMed] [Google Scholar]
- 58.Baca-García E, Diaz-Sastre C, Ceverino A, Saiz-Ruiz J, Diaz FJ, De Leon J. Association between the menses and suicide attempts: a replication study. Psychosomatic Medicine. 2003;65(2):237–244. doi: 10.1097/01.psy.0000058375.50240.f6. [DOI] [PubMed] [Google Scholar]
- 59.Qin P, Mortensen PB. The impact of parental status on the risk of completed suicide. Archives of General Psychiatry. 2003;60(8):797–802. doi: 10.1001/archpsyc.60.8.797. [DOI] [PubMed] [Google Scholar]
- 60.Qin P, Agerbo E, Westergard-Nielsen N, Eriksson T, Mortensen PB. Gender differences in risk factors for suicide in Denmark. The British Journal of Psychiatry. 2000;177:546–550. doi: 10.1192/bjp.177.6.546. [DOI] [PubMed] [Google Scholar]
- 61.Appleby L. Suicide during pregnancy and in the first postnatal year. British Medical Journal. 1991;302(6769):137–140. doi: 10.1136/bmj.302.6769.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Appleby L, Turnbull G. Parasuicide in the frrst postnatal year. Psychological Medicine. 1995;25(5):1087–1090. doi: 10.1017/s0033291700037570. [DOI] [PubMed] [Google Scholar]
- 63.Andersson L, Sundström-Poromaa I, Bixo M, Wulff M, Bondestam K, Åström M. Point prevalence of psychiatric disorders during the second trimester of pregnancy: a population-based study. American Journal of Obstetrics and Gynecology. 2003;189(1):148–154. doi: 10.1067/mob.2003.336. [DOI] [PubMed] [Google Scholar]
- 64.Melville JL, Gavin A, Guo Y, Fan MY, Katon WJ. Depressive disorders during pregnancy: prevalence and risk factors in a large urban sample. Obstetrics and Gynecology. 2010;116(5):1064–1070. doi: 10.1097/AOG.0b013e3181f60b0a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.da Silva R, da Costa Ores L, Jansen K, et al. Suicidality and associated factors in pregnant women in Brazil. Community Mental Health Journal. 2012;48(3):392–395. doi: 10.1007/s10597-012-9495-0. [DOI] [PubMed] [Google Scholar]
- 66.Reck C, Struben K, Backenstrass M, et al. Prevalence, onset and comorbidity of postpartum anxiety and depressive disorders. Acta Psychiatrica Scandinavica. 2008;118(6):459–468. doi: 10.1111/j.1600-0447.2008.01264.x. [DOI] [PubMed] [Google Scholar]
- 67.Frautschi S, Cerulli A, Maine D. Suicide during pregnancy and its neglect as a component of maternal mortality. International Journal of Gynecology & Obstetrics. 1994;47(3):275–284. doi: 10.1016/0020-7292(94)90574-6. [DOI] [PubMed] [Google Scholar]
- 68.Gissler M, Hemminki E, Lönnqvist J. Suicides after pregnancy in Finland, 1987–94: register linkage study. British Medical Journal. 1996;313(7070):1431–1434. doi: 10.1136/bmj.313.7070.1431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Lewinsohn PM, Hops H, Roberts RE, Seeley JR, Andrews JA. Adolescent psychopathology: I. prevalence and incidence of depression and other DSM-III-R disorders in high school students. Journal of Abnormal Psychology. 1993;102(1):133–144. doi: 10.1037//0021-843x.102.1.133. [DOI] [PubMed] [Google Scholar]
- 70.Schoenbach VJ, Garrison CZ, Kaplan BH. Epidemiology of adolescent depression. Public Health Reviews. 1984;12(2):159–189. [PubMed] [Google Scholar]
- 71.Czeizel AE. Attempted suicide and pregnancy. Journal of Injury and Violence Research. 2011;3(1):45–54. doi: 10.5249/jivr.v3i1.77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Howard LM, Flach C, Mehay A, Sharp D, Tylee A. The prevalence of suicidal ideation identified by the Edinburgh postnatal depression scale in postpartum women in primary care: findings from the RESPOND trial. BMC Pregnancy and Childbirth. 2011:p. 57. doi: 10.1186/1471-2393-11-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Mauri M, Oppo A, Borri C, Banti S. SUICIDALITY in the perinatal period: comparison of two self-report instruments. results from PND-ReScU. Archives of Women's Mental Health. 2012;15(1):39–47. doi: 10.1007/s00737-011-0246-y. [DOI] [PubMed] [Google Scholar]
- 74.Pinheiro RT, da Cunha Coelho FM, da Silva RA, et al. Suicidal behavior in pregnant teenagers in southern Brazil: social, obstetric and psychiatric correlates. Journal of Affective Disorders. 2012;136(3):520–525. doi: 10.1016/j.jad.2011.10.037. [DOI] [PubMed] [Google Scholar]
- 75.Lindahl V, Pearson JL, Colpe L. Prevalence of suicidality during pregnancy and the postpartum. Archives of Women’s Mental Health. 2005;8(2):77–87. doi: 10.1007/s00737-005-0080-1. [DOI] [PubMed] [Google Scholar]
- 76.Henshaw C. Maternal suicide. In: Cockburn J, Pawson M, editors. Psychological Challenges in Obstetrics and Gynecology: The Clinical Management. New York, NY, USA: Springer; 2007. pp. 157–164. [Google Scholar]
- 77.Brettingham M. Depression and obesity are major causes of maternal death in Britain. BMJ. 2004;329(7476):p. 1205. doi: 10.1136/bmj.329.7476.1205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Appleby L, Mortensen PB, Faragher EB. Suicide and other causes of mortality after post-partum psychiatric admission. The British Journal of Psychiatry. 1998;173:209–211. doi: 10.1192/bjp.173.3.209. [DOI] [PubMed] [Google Scholar]
- 79.Gissler M, Berg C, Bouvier-Colle MH, Buekens P. Injury deaths, suicides and homicides associated with pregnancy, Finland 1987–2000. European Journal of Public Health. 2005;15(5):459–463. doi: 10.1093/eurpub/cki042. [DOI] [PubMed] [Google Scholar]
- 80.Steinberg JR, Becker D, Henderson JT. Does the outcome of a first pregnancy predict depression, suicidal ideation, or lower self-esteem? Data from the national comorbidity survey. American Journal of Orthopsychiatry. 2011;81(2):193–201. doi: 10.1111/j.1939-0025.2011.01088.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Morgan CL, Evans M, Peters JR. Suicides after pregnancy. Mental health may deteriorate as a direct effect of induced abortion. BMJ. 1997;314(7084):902–903. [PMC free article] [PubMed] [Google Scholar]
- 82.Charles VE, Polis CB, Sridhara SK, Blum RW. Abortion and long-term mental health outcomes: a systematic review of the evidence. Contraception. 2008;78(6):436–450. doi: 10.1016/j.contraception.2008.07.005. [DOI] [PubMed] [Google Scholar]
- 83.Palladino CL, Singh V, Campbell J, Flynn H, Gold KJMSW. Homicide and suicide during the perinatal period: findings from the national violent death reporting system. Obstetrics & Gynecology. 2011;118(5):1056–1063. doi: 10.1097/AOG.0b013e31823294da. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Murray D, Cox JL, Chapman G, Jones P. Childbirth: life event or start of a long-term difficulty? further data from the stoke-on-trent controlled study of postnatal depression. The British Journal of Psychiatry. 1995;166:595–600. doi: 10.1192/bjp.166.5.595. [DOI] [PubMed] [Google Scholar]
- 85.Samandari G, Martin SL, Kupper LL, Schiro S, Norwood T, Avery M. Are pregnant and postpartum women: at increased risk for violent death? Suicide and homicide findings from North Carolina. Maternal and Child Health Journal. 2011;15(5):660–669. doi: 10.1007/s10995-010-0623-6. [DOI] [PubMed] [Google Scholar]
- 86.Kjaer TK, Jensen A, Dalton SO, Johansen C, Schmiedel S, Kjaer SK. Suicide in Danish women evaluated for fertility problems. Human Reproduction. 2011;26(9):2401–2407. doi: 10.1093/humrep/der188. [DOI] [PubMed] [Google Scholar]
- 87.Bramness JG, Walby FA, Hjellvik V, Selmer R, Tverdal A. Self-reported mental health and its gender differences as a predictor of suicide in the middle-aged. American Journal of Epidemiology. 2010;172(2):160–166. doi: 10.1093/aje/kwq091. [DOI] [PubMed] [Google Scholar]
- 88.Cutright P, Stack S, Fernquist R. Marital status integration, suicide disapproval, and societal integration as explanations of marital status differences in female age-specific suicide rates. Suicide & Life-Threatening Behavior. 2007;37(6):715–724. doi: 10.1521/suli.2007.37.6.715. [DOI] [PubMed] [Google Scholar]
- 89.White A, Holmes M. Patterns of mortality across 44 countries among men and women aged 15–44 years. Journal of Men’s Health and Gender. 2006;3(2):139–151. [Google Scholar]
- 90.Erlangsen A, Jeune B, Bille-Brahe U, Vaupel JW. Loss of partment and suicide risks among oldest old: a population-based register study. Age and Ageing. 2004;33(4):378–383. doi: 10.1093/ageing/afh128. [DOI] [PubMed] [Google Scholar]
- 91.Wanta BT, Schlotthauer AE, Guse CE, Hargarten SW. The burden of suicide in Wisconsin’s older adult population. Wisconsin Medical Journal. 2009;108(2):87–93. [PubMed] [Google Scholar]
- 92.Zeppegno P, Manzetti E, Valsesia R, et al. Differences in suicide behaviour in the elderly: a study in two provinces of Northern Italy. International Journal of Geriatric Psychiatry. 2005;20(8):769–775. doi: 10.1002/gps.1354. [DOI] [PubMed] [Google Scholar]
- 93.Kuroki M. Suicide and unemployment in Japan: evidence from municipal level suicide rates and age-specific suicide rates. The Journal of Socio-Economics. 2010;39(6):683–691. [Google Scholar]
- 94.Centers for Disease Control and Prevention (CDC) Web-based Injury Statistics Query and Reporting System (WISQARS) 2007, http://www.cdc.gov/ncipc/wisqars/default.htm.
- 95.Usall J, Pinto-Meza A, Fernández A, et al. Suicide ideation across reproductive life cycle of women Results from a European epidemiological study. Journal of Affective Disorders. 2009;116(1-2):144–147. doi: 10.1016/j.jad.2008.12.006. [DOI] [PubMed] [Google Scholar]
- 96.Kposowa AJ. Marital status and suicide in the national longitudinal mortality study. Journal of Epidemiology and Community Health. 2000;54(4):254–261. doi: 10.1136/jech.54.4.254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.De Leo D, Padoani W, Scocco P, et al. Attempted and completed suicide in older subjects: results from the WHO/EURO Multicentre Study of Suicidal Behaviour. International Journal of Geriatric Psychiatry. 2001;16(3):300–310. doi: 10.1002/gps.337. [DOI] [PubMed] [Google Scholar]
- 98.Karch D. Sex differences in suicide incident characteristics and circumstances among older adults: surveillance data from the national violent death reporting system-17 U.S. states, 2007–2009. International Journal of Environmental Research and Public Health. 8(8):3479–3495. doi: 10.3390/ijerph8083479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Carney SS, Rich CL, Burke PA, Fowler RC. Suicide over 60: the San Diego study. Journal of the American Geriatrics Society. 1994;42(2):174–180. doi: 10.1111/j.1532-5415.1994.tb04948.x. [DOI] [PubMed] [Google Scholar]
- 100.Frierson RL. Suicide attempts by the old and the very old. Archives of Internal Medicine. 1991;151(1):141–144. [PubMed] [Google Scholar]
- 101.Shah A. The relationship between suicide rates and age: an analysis of multinational data from the World Health Organization. International Psychogeriatrics. 2007;19(6):1141–1152. doi: 10.1017/S1041610207005285. [DOI] [PubMed] [Google Scholar]
- 102.Snowdon J. Suicide rates and methods in different age groups: Australian data and perceptions. International Journal of Geriatric Psychiatry. 1997;12(2):253–258. doi: 10.1002/(sici)1099-1166(199702)12:2<253::aid-gps605>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 103.Cheong K, Choi M, Cho B, et al. Suicide rate differences by sex, age, and urbanicity, and related regional factors in Korea. Journal of Preventive Medicine and Public Health. 2012;45(2):70–77. doi: 10.3961/jpmph.2012.45.2.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Rebholz CM, Gu D, Yang W, et al. Mortality from suicide and other external cause injuries in China: a prospective cohort study. BMC Public Health. 2011;11, article 56 doi: 10.1186/1471-2458-11-56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Agerbo E. Midlife suicide risk, partner’s psychiatric illness, spouse and child bereavement by suicide or other modes of death: a gender specific study. Journal of Epidemiology and Community Health. 2005;59(5):407–412. doi: 10.1136/jech.2004.024950. [DOI] [PMC free article] [PubMed] [Google Scholar]