

Abstract
Based on molecular aberrations, in particular the NPM1 mutation (NPM1mut) and the FLT3 internal tandem duplication (Flt3-ITD), prognostic subgroups have been defined among patients with acute myeloid leukemia with normal karyotype. Whereas these subgroups are known to play an important role in outcome in first complete remission, and also in the indication for allogeneic stem cell transplantation, data are limited on their role after transplantation in advanced disease. To evaluate the role of molecular subgroups of acute myeloid leukemia with normal karyotype after allogeneic stem cell transplantation beyond first complete remission, we analyzed the data from 141 consecutive adults (median age: 51.0 years, range 18.4-69.3 years) who had received an allogeneic transplant either in primary induction failure or beyond first complete remission. A sequential regimen of cytoreductive chemotherapy (fludarabine, high-dose AraC, amsacrine) followed by reduced intensity conditioning (FLAMSA-RIC), was uniformly used for conditioning. After a median follow up of three years, overall survival from transplantation was 64±4%, 53±4% and 44±5% at one, two and four years, respectively. Forty patients transplanted in primary induction failure achieved an encouraging 2-year survival of 69%. Among 101 patients transplanted beyond first complete remission, 2-year survival was 81% among patients with the NPM1mut/FLT3wt genotype in contrast to 43% in other genotypes. Higher numbers of transfused CD34+ cells (hazard ratio 2.155, 95% confidence interval 0.263-0.964, P=0.039) and favorable genotype (hazard ratio 0.142, 95% confidence interval: 0.19-0.898, P=0.048) were associated with superior overall survival in multivariate analysis. In conclusion, patients with acute myeloid leukemia with normal karyotype can frequently be rescued after primary induction failure by allogeneic transplantation following FLAMSA-RIC. The prognostic role of NPM1mut/FLT3-ITD based subgroups was carried through after allogeneic stem cell transplantation beyond first complete remission.
Introduction
Acute myeloid leukemia with normal cytogenetics (CN-AML) is diagnosed in more than 40% of AML patients. Over recent years, a variety of gene mutations and deregulated expression of genes and microRNA have been described, providing insight into leukemogenesis and allowing for the definition of distinct subgroups of CN-AML with different sensitivity to treatment and prognosis.1 Among the numerous aberrations described, three somatically acquired mutations are currently recommended for analysis in clinical trials and routine practice: mutations in the nucleophosmin 1 gene (NPM1mut, affecting 45-54% of CN-AML), mutations in the myeloid transcription factor CEBPA (affecting 10-18% of CN-AML), and internal tandem duplications of the fmsrelated tyrosine kinase 3 gene (FLT3-ITD, observed in 28-34% of CN-AML).2 Patients combining NPM1mut and wild type of FLT3wt, and patients with a biallelic CEBPA mutation have a better prognosis. In contrast, CN-AML with FLT3-ITD, or with negativity for both FLT3-ITD and NPM1mut represent unfavorable subgroups with poorer outcome.3,4
Allogeneic transplantation of hematopoietic stem cells (alloHSCT) has been evaluated as consolidation therapy in first complete remission (CR1) for molecularly defined sub-entities of CN-AML. Recently, the European Bone Marrow Transplantation Group (EBMT) has shown a negative influence of FLT3-ITD after related and unrelated alloHSCT in CR1.5 In a large German study4 the availability of a related donor for alloHSCT was associated with improved overall survival (OS) in CR1 in patients with an unfavorable (high-risk) genotype (FLT3-ITD with or without NPM1mut, or NPM1wt/FLT3wt), but not in patients with favorable genotype (the role of CEBPA was not evaluated due to limited numbers). Similar results had been reported by others6 although the issue remains controversial.7
In contrast to CR1, few studies have addressed the role of molecular markers in relapsed patients or patients with primary induction failure (PIF), although the cumulative incidence (CI) of PIF and relapse in CN-AML is around 15% and 44%, respectively.4 Recently, the favorable genotype was shown to maintain a good prognosis in relapsed and refractory AML after gemtuzumab-ozogamicin based therapy,8 whereas FLT3-ITD retained its negative prognostic value in two series of relapsed patients which both included a limited number of patients receiving salvage alloHSCT.9,10 Here, we present the results of a large cohort of patients who had all received the FLAMSA-RIC regimen before alloHSCT for CN-AML, either in PIF or beyond CR1. The study aimed to further evaluate the role of the most common molecular aberrations in this setting, and to determine the efficacy of FLAMSA-RIC based alloHSCT in clinically and molecularly defined patient subgroups.
Design and Methods
Patients
In 1999, a preparative regimen for alloHSCT in high-risk AML, comprised of a sequence of cytoreductive chemotherapy [fludarabine, high-dose AraC (HiDAC), and amsacrine, (FLAMSA)] and reduced intensity conditioning (RIC) was introduced.11 Over the following years, a registry was established for patients receiving FLAMSA-RIC to allow for specific analysis against the background of a uniform conditioning. So far, more than 700 patients have been reported by 16 centers where this protocol was used for all consecutive patients with high-risk AML. For the present analysis, all consecutive patients who had undergone alloHSCT for advanced CN-AML and had information on mutational status of FLT3 and NPM1 at time of diagnosis available, were selected from the database. As in other studies,4,10 the number of patients with the CEBPAmut genotype was low, which is why the role of this favorable subgroup could not be evaluated. No other selection criteria were used. The outcome of 18 previously published patients12 was updated as of October 15, 2011. Review of submitted data, personal contact with the treating physicians, and repeated visits in the reporting centers guaranteed quality of data.
Treatment
Salvage treatment for relapse or PIF was at the respective centers' discretion. The FLAMSA-RIC regimen has been described previously.11 In brief, fludarabine (30 mg/m2), HiDAC (2 g/m2), and amsacrine (100 mg/m2) were applied from Day -12 to Day -9. After three days of rest, 4 Gy total body irradiation (TBI) on Day -5, cyclophosphamide (40 mg/kg for related, 60 mg/kg for unrelated or mismatched transplants) on Days -4 and -3, and rabbit anti-thymococyte globulin (ATG Fresenius; 10 mg/kg for related, 20 mg/kg for unrelated or mismatched transplants) from Day -4 to Day -2 were given. Intravenous (iv) busulfan (8 × 0.8 mg/kg) was substituted for TBI in patients not eligible for TBI. For transplantation, G-CSF mobilized peripheral blood stem cells (PBSC) were preferred; bone marrow (BM) was also accepted. Graft-versus-host disease (GvHD) prophylaxis consisted of cyclosporine and mycophenolate mofetil (2 × 15 mg/kg). Rapamycin could be substituted for cyclosporine according to the centers' preference. Supportive medication followed local standards. From Day +120, prophylactic transfusion of donor lymphocytes (pDLT) was recommended in patients in remission, without infection, and free of GvHD after 30 days off immunosuppression. The initial cell dose was 1×106 CD3 cells/kg; in the absence of GvHD, pDLT was repeated up to 3 times, with 5- to 10-fold increase in cell dose per transfusion.
Evaluation and definition
Disease response,2,13 HSCT-related risk,14 and GvHD15 were classified as recommended. As proposed by Schlenk and co-workers,4,10 molecular subgroups were defined on the basis of the mutational status of NPM1 and the presence or absence of FLT3-ITD and CEBPAmut: The favorable group was defined by presence of an NPM1 mutation in absence of FLT3-ITD. As described above, the CEBPAmut genotype was not observed in enough patients to include this subgroup into the analysis. Conversely, the unfavorable genotype was defined by absence of CEBPAmut and either NPM1mut/FLT3-ITD, NPM1wt/FLT3-ITD, or NPM1wt/FLT3wt. As suggested, primary induction failure was defined as persistence of more than 5% blasts in BM or detection of circulating blasts, following either two courses of conventional induction chemotherapy, or induction chemotherapy including at least one course of HiDAC (i.e. >1 g/m2/d) with or without a second course of conventional or HiDAC-based chemotherapy.2,13,16-19 Relapse was defined by reappearance of blasts in peripheral blood (PB), by any leukemia infiltration outside the hematopoietic system, or by BM infiltration of more than 5% blasts. Refractory relapse was defined by circulating blasts or more than 5% BM blasts following at least one course of salvage chemotherapy.
Date of neutrophil engraftment was defined as the first of two consecutive days with a PB neutrophil count over 0.5 × 109/L. Date of platelet engraftment was defined as the first of three consecutive days with a platelet count over 20 × 109/L without transfusion. Disease response and chimerism were assessed by Day +30. Since platelet regeneration could be postponed by factors other than leukemia and cytotoxic therapy (i.e. GvHD, drugs, viral infection), CR after transplantation was defined by less than 5% blasts without evidence of dysplasia in BM, and more than 1500 neutrophils/μL in PB. Non-relapse mortality (NRM) after HSCT was defined as death from any reason in the absence of leukemia, whereas death with persisting leukemia after alloHSCT or after post transplant relapse was classified as leukemia-associated death (LAD).
Cytogenetics and molecular genetic analysis
Chromosome analysis was performed using short-term cultures following standard protocols.20 The chromosomes were interpreted according to the International System for Human Cytogenetic Nomenclature.21
Molecular analyses were performed according to the local standard at each center following published protocols.4,22-24
Statistical analysis
Cumulative incidence of LAD and NRM after HSCT were simultaneously calculated, accounting for competing risks. Overall survival (OS) was calculated from day of transplant to day of death or last follow up. Leukemia free survival (LFS) was calculated from day of transplant to day of relapse or death in remission. OS and LFS were estimated using the Kaplan-Meier method. The log rank test and a Cox's model were used for analysis of risk factors for time-to-event variables. Hazard ratio (HR) and 95% confidence interval (CI) were reported. R version 2.14.1 and SPSS version 18 (SPSS Inc., Chicago, IL, USA) software were used.
Study conduct
The study was performed according to the modified Declaration of Helsinki, and was approved by the local institutional review board. Written informed consent for inclusion of data into national and international registries was obtained from all patients.
Results
We analyzed 141 consecutive patients (median age 51.0 years, range 18.4-69.3 years) transplanted in primary induction failure (PIF, n=40), or beyond CR1 (untreated first relapse, n=51; refractory first relapse, n=39, CR2, n=11). Fourteen had a favorable and 127 an unfavorable genotype. Patients' characteristics are shown in Table 1.
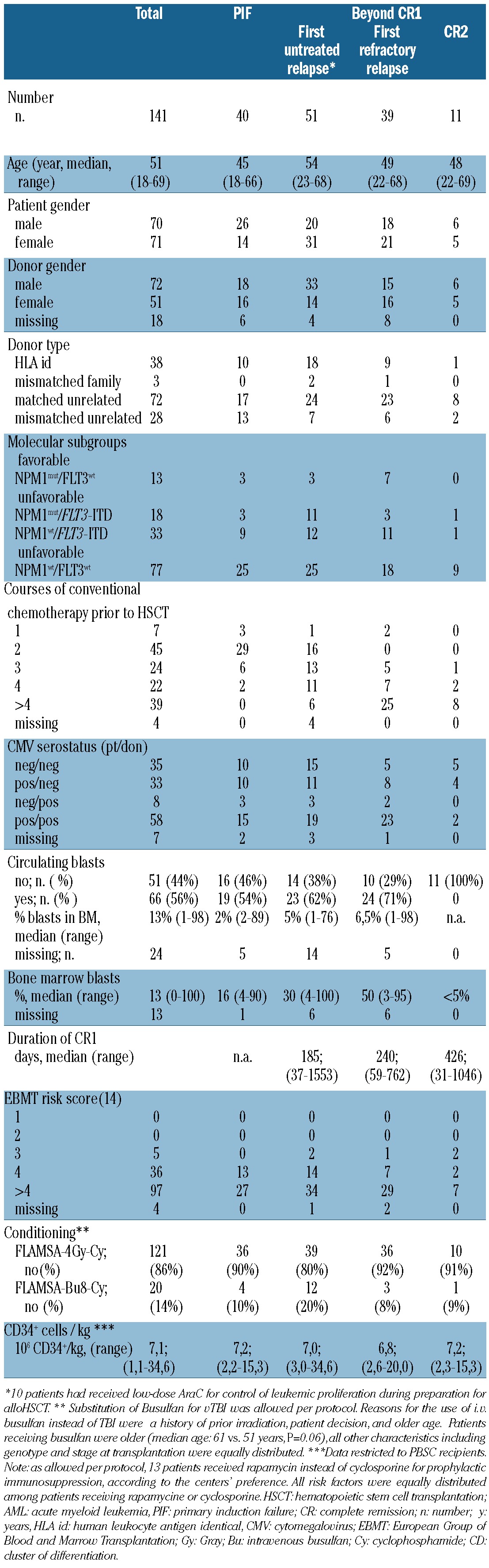
Table 1.
Characteristics of 141 patients undergoing allogeneic HSCT for advanced AML.
Response and outcome
After alloHSCT, 127 patients (90%) achieved CR, with no differences with respect to genotype or stage at HSCT. Seven patients (5%) each died in aplasia or showed refractory disease after HSCT. Median time to engraftment of both neutrophils and platelets was 16 days. Median follow up among 67 survivors was 36 months. OS at one, two and four years was 64±4%, 53±4% and 44±5%, respectively; the respective LFS was 58±4%, 48±4% and 40±4%. OS and LFS were superior after alloHSCT in PIF, as compared to transplantation beyond CR1 (P=0.013, HR=2.097, 95%CI: 1.17-3.759 for OS, P=0.017, HR 1.997, 95%CI: 1.131-3.525 for LFS, Figure 1). Forty-three patients (34% of responders) relapsed. Cumulative incidence of LAD and NRM was 5±2% and 8±2% at Day 100, and 28±4% and 18±3% at two years (Figure 2). Causes of NRM were infections (n=16), acute or chronic GvHD (n=5), GvHD + infection (n=4), and other reasons (n=6). AGvHD grades I, II, III and IV occurred in 30%, 16%, 8% and 6% of patients at risk, respectively, aGvHD of grade III/IV was associated with higher NRM (P=0.011) and inferior OS (P=0.004). Twenty-four percent and 22% of patients alive by Day 100 developed limited and extensive cGvHD, respectively. CGvHD was associated with lower incidence of relapse (P=0.034) and LAD (P=0.001), and superior OS (P=0.01). Effects of both aGvHD and cGvHD were observed without significant differences across all disease stages and molecular subgroups.
Figure 1.
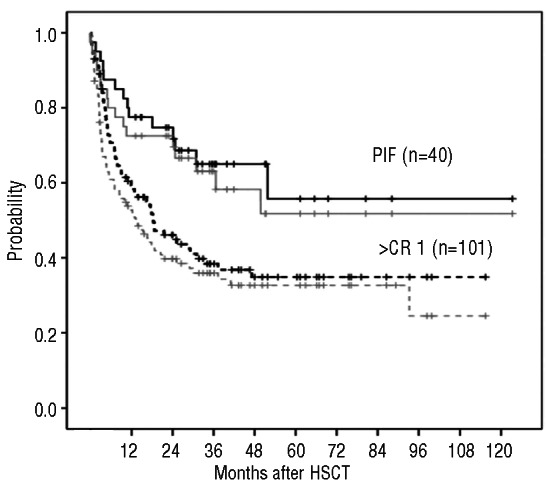
Overall survival (in black) and leukemia free survival (in gray) after allogeneic HSCT for 141 patients with CN-AML as of stage at transplantation. Patients transplanted in primary induction failure (PIF, solid curves) achieved superior OS (P=0.013) and LFS (P=0.017) as compared to patients transplanted beyond CR1 (dashed curves).
Figure 2.
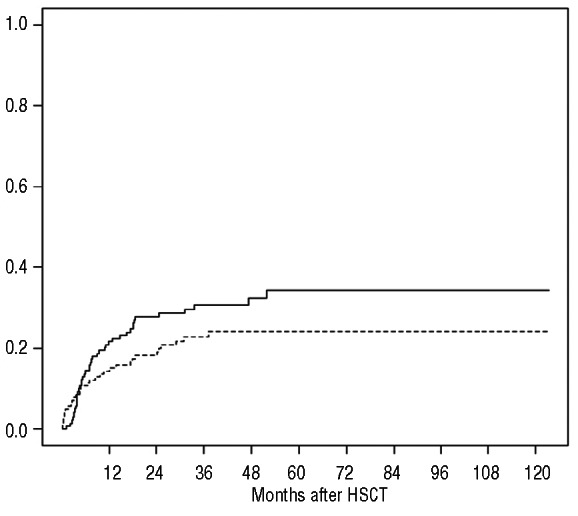
Cumulative incidence of leukemia-associated death (solid curve) and non-relapse mortality (dashed curve) among 141 patients transplanted for advanced CN-AML.
Thirty-four patients (24% of the entire cohort) fulfilled the criteria for pDLT and received one (n=13), 2 (n=6) and 3 (n=15) transfusions. Development of GvHD and relapse were reasons for giving less than 3 transfusions.
Transplantation in primary induction failure
Among 40 patients fulfilling the definition of primary induction failure (PIF), 8 had received two cycles of conventional induction, 3 had received one course of HiDAC-based chemotherapy, and 29 had received more than one course, including at least one HiDAC-based course. A median of two cycles was given before FLAMSA-RIC. At start of FLAMSA, 59% of patients had circulating blasts (median 22%, range 2-89%), median percentage of blast in BM was 15.5% (range 4-90%). Following alloHSCT, one patient each died in aplasia and from persisting AML; 38 achieved CR. Relapse occurred in 8 responders at a median of 7.8 (range 1.9-49.8) months from transplantation. OS/LFS at two and four years were 69%±7%/63±8%, and 68±7%/58±9%, respectively (Figure 1). Two-year cumulative incidence of both LAD (15±6%) and NRM (10±5%) were low. Thirteen patients had received pDLT; only one of them relapsed.
Only 3 of 40 patients had a favorable genotype, precluding the analysis of the role of the predefined molecular subgroups after alloHSCT for CN-AML in PIF. There was a trend for superior outcome in patients without an FLT3-ITD (2-year OS: 80+/-9% vs. 56+/-15% in patients with an FLT3-ITD, P=0.093, HR: 2.552, 95%CI: 0.821-7.923) and in patients without circulating blasts at start of conditioning (2-year OS: 97% vs. 61%, P=0.085, HR=3.848, 95% CI: 0.8294-17.874). The following factors had no influence on outcome: gender and age of patient and donor, type of donor, use of HiDAC prior to conditioning, CMV status, the EBMT risk score,14 percentage of blasts in BM before conditioning, type of conditioning (4Gy TBI/Cy vs. busulfan/Cy) and CD34+ cell counts in the transplant.
Transplantation beyond CR1
Among 101 patients undergoing alloHSCT beyond first remission, CR was achieved after alloHSCT in 92%, 82%, and 91% of patients transplanted in untreated relapse, refractory relapse or CR2, respectively (P=0.42). OS/LFS from transplantation of the entire cohort was 45±5%/40±5% at two years, and 36±5%/33±5% at four years (Figure 1). In comparison to HSCT in PIF, both increased rates of LAD (41±6%) and NRM (33±6) were responsible for treatment failure. Patients in CR2 achieved an OS of 73%, whereas outcome of patients in both untreated and refractory relapse was inferior (P=0.07, HR 2.927, 95% CI: 0.941-9.371; Figure 3A).
Figure 3.
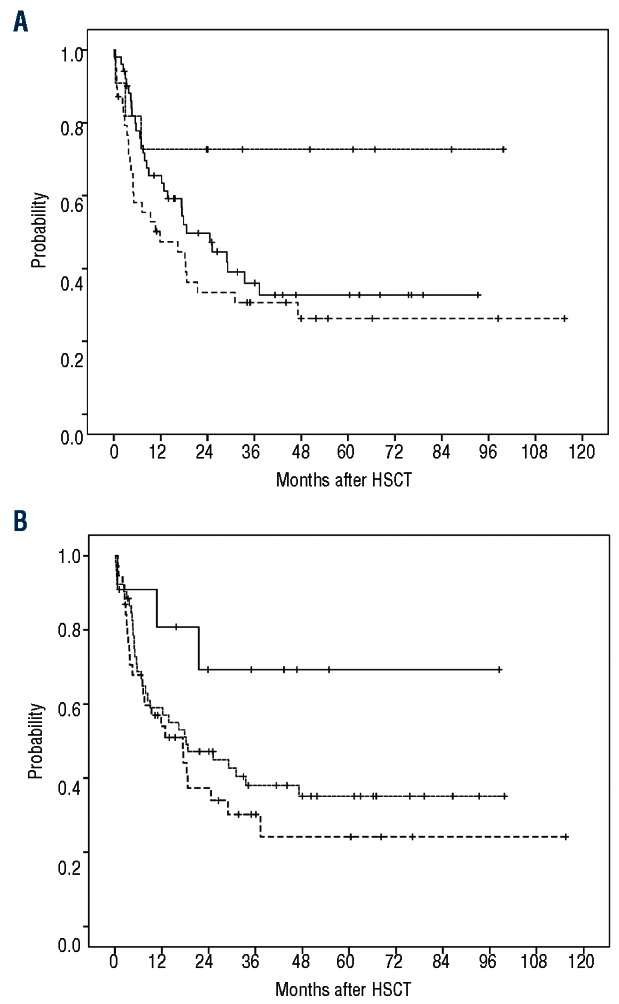
Overall survival from HSCT in 101 patients transplanted beyond CR1. (A) OS as of stage at HSCT [CR2 (dotted curve), untreated relapse (solid curve) and refractory relapse (dashed curve)]. (B) OS as of molecular subgroups [favorable genotype (NPM1mut/FLT3wt, solid curve), versus unfavorable genotypes (NPM1wt/FLT3wt, dotted curve, or FLT3-ITD with or without NPM1mut, dashed curve)]
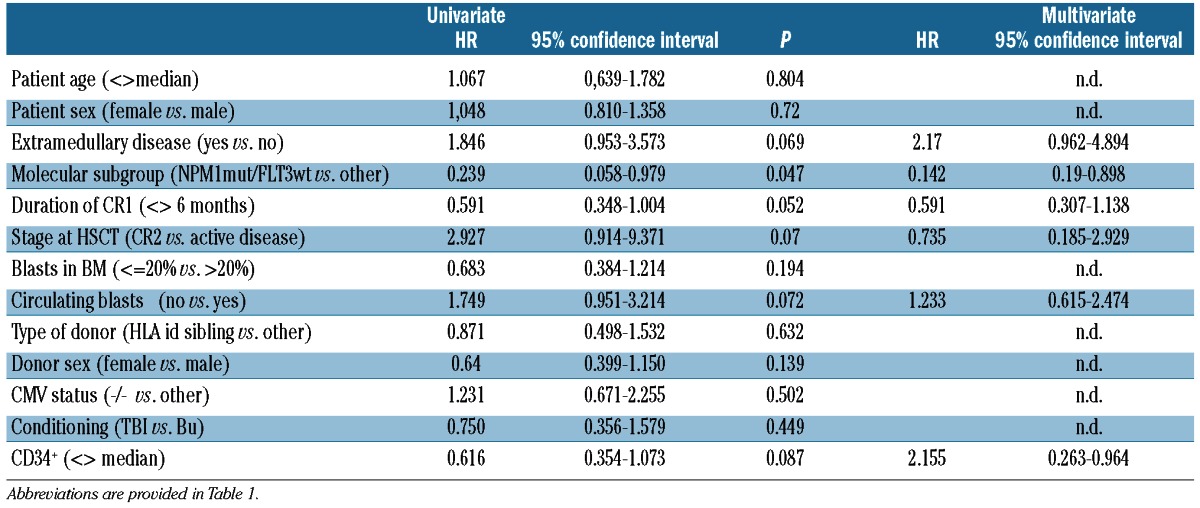
At start of conditioning, there was a significant difference in patients' characteristics among the molecular subgroups (Table 2). Patients with a favorable genotype had experienced a longer remission (P<0.001) and presented with less circulating blasts (P<0.001) and lower blast counts in BM (P=0.032). Differences were most pronounced in comparison to patients with an FLT3-ITD, regardless of the presence or absence of NMP1mut. With respect to OS from HSCT, patients with a favorable genotype achieved a superior outcome in comparison to all other genotypes (2-year OS: 80.8% vs. 41.9%; Figure 3B). Outcome was comparable among the double negative patients (NPM1wt/FLT3wt) and those with an FLT3-ITD (with or without NMP1mut; P=0.360). In a multivariate Cox's model for OS from alloHSCT, a CD34+ cell content in the graft above the median of 6.8 × 106/kg (HR: 2.155, 95% CI: 0.263-0.964, P=0.039), the molecular subgroup (favorable vs. unfavorable, HR: 0.142, 95%CI: 0.19-0,898, P=0.048) and presence of extramedullary manifestation of AML (HR=2.17, 95%CI: 0.96-2.4.894, P=0.062) were the most important variables (Table 3). pDLT could be given to 22 patients (22%), with no difference between molecular subgroups. Among pDLT recipients, 8 patients relapsed at a median of 23 months from alloHSCT.
Table 2.
Characteristics at time of relapse and transplantation among 101 patients with different molecular subtypes transplanted beyond CR1.
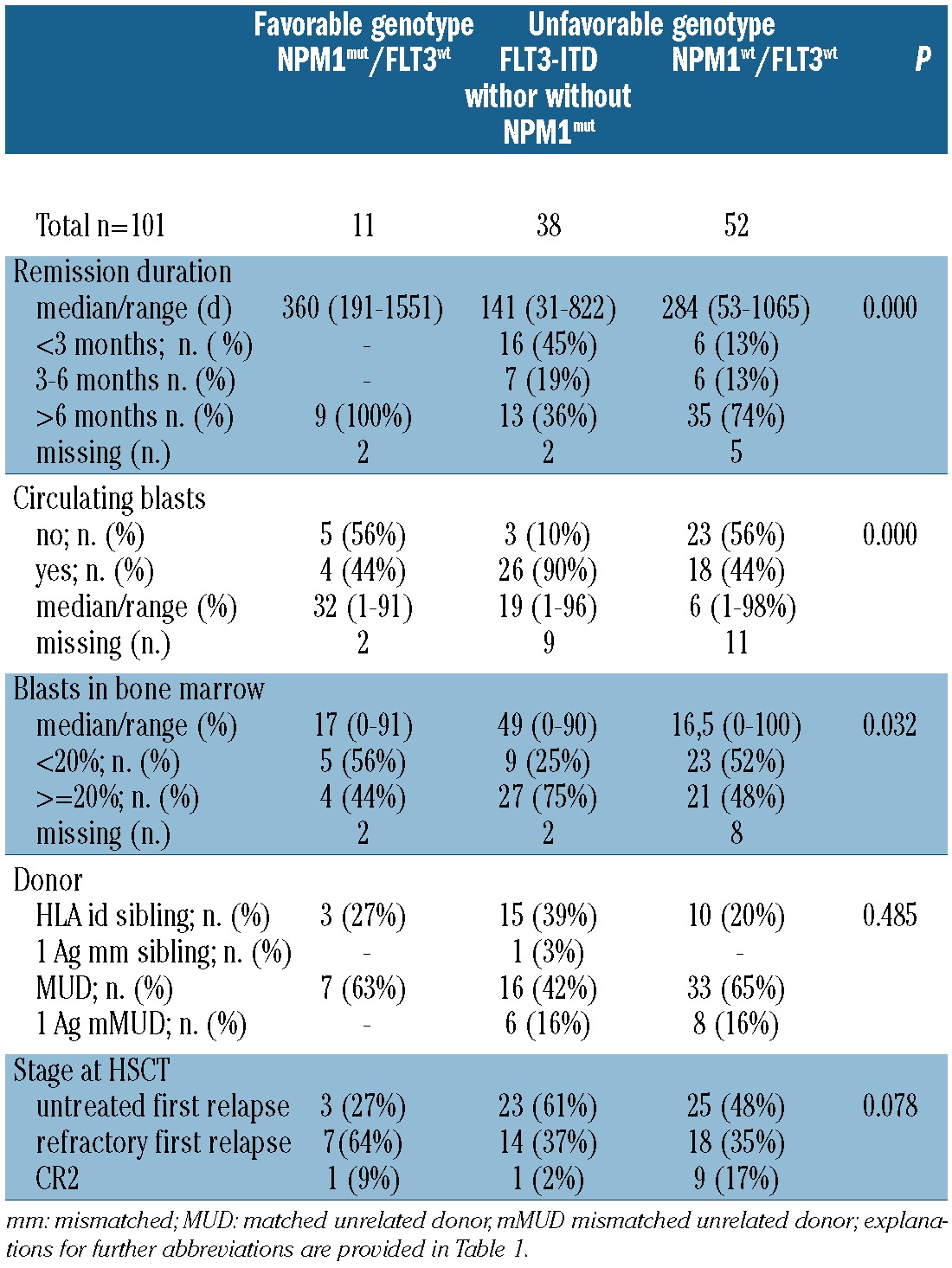
Table 3.
Analysis of risk factors for overall survival among 101 patients transplanted for CN-AML beyond CR1.
Discussion
This study analyzed the efficacy of the FLAMSA-RIC regimen and the role of molecular subgroups for outcome after allogeneic HSCT in advanced CN-AML. Promising results were observed after transplantation in PIF. In patients transplanted beyond CR1, the prognostic significance of molecular subgroups, originally developed to estimate the individual prognosis at time of diagnosis,4 was confirmed, as shown both by the different patients' characteristics at relapse and transplantation, and by the differences in outcome among patients with various genotypes. Similar data have been reported in a smaller cohort of patients with FLT3-ITD,9 but so far not in patients with double negative (NPM1wt/FLT3wt) CN-AML.
Considering the intrinsic limitations of a retrospective analysis, several steps have been taken to assure data quality: i) the uniform use of FLAMSA-RIC as standard regimen for all consecutive patients with advanced AML in the participating centers excluded a frequent bias of retrospective studies in HSCT, in which non-myeloablative, RIC, and standard regimen are often mixed; ii) a strict definition for PIF according to published guidelines2,13,18 was applied, assuring a homogeneous cohort that had failed double induction and/or HiDAC-based chemotherapy; iii) median follow up was three years from HSCT in all subgroups, covering the vast majority of expected events, which in advanced AML are usually seen within two years;25 iv) repeated questionnaires were completed, personal visits were made to centers, and direct contact with the treating physicians was maintained.
Nevertheless, the study still has some limitations. First, the molecular status was analyzed as determined at diagnosis rather than at relapse. However, NPM1 has been shown to be relatively stable during the course of AML, and can reliably be used as a marker for minimal residual disease (MRD) and relapse.26-28FLT3-ITD is less stable and is more difficult to monitor, but de novo acquisition at a later stage is rare.26,29,30 Second, the mutant/wild-type ratio and the FLT3-ITD insertion site were not systematically determined. Both parameters have been shown to influence outcome after conventional chemotherapy and alloHSCT in CR1.24,31 Although there are no published data addressing their role in advanced disease, integration into the regular monitoring might be useful. Restriction to the analysis of NPM1mut and FLT3-ITD is another limitation. However, these are the two most common and most intensively studied markers, and are both recommended for routine clinical practice.2 In contrast, the clinical relevance and mutual interaction of a variety of mutations (NRAS, IDH1/2, TET2, DNMT3A) or altered gene expression levels (BAALC, WT1, ERG, EVI1) is not completely clear, meaning these markers still only have investigational status.1,32 Furthermore, in a recently published multivariable scoring system for CN-AML,33 92% of the patients classified as high-risk could be identified by a high-risk NPM1/FLT3-ITD status.
According to our data, CN-AML patients in PIF have a relatively favorable prognosis following FLAMSA-RIC and alloHSCT, with 69% being alive at two years from alloHSCT. A better outcome after transplantation in PIF as compared to early relapse has been observed in a large CIBMTR study;25 this difference might be more pronounced in CN-AML. High-risk clinical characteristics (80% of patients resistant to HiDAC, circulating blasts at start of conditioning in 59%, EBMT risk score >3 in 100%) argue against a selection bias in this cohort transplanted in PIF. Unfortunately, limited numbers precluded a meaningful analysis of risk factors after alloHSCT in PIF. Since 37 of 40 patients showed a genotype other than the favorable NPM1mut/FLT3wt, the role of the predefined molecular subgroups could not be evaluated either. Among the unfavorable genotypes, patients with NPM1wt/FLT3wt achieved an OS of 80% at two years from alloHSCT in PIF, whereas OS was 56% in patients with FLT3-ITD. Nevertheless, these results still compare favorably to published data in refractory FLT3-ITD+ AML. A median of two chemotherapy cycles was given prior to FLAMSA-RIC. Results after alloHSCT were identical, whether or not the patients had received HiDAC-based induction or salvage. Hence, the sequence of initial cytoreduction applied by FLAMSA, followed by an allogeneic graft-versus-leukemia reaction applied by the graft, can be effective even in CN-AML not achieving CR after HiDAC-based chemotherapy alone. Furthermore, early transplantation instead of repeated attempts for remission induction might improve the results of alloHSCT, once the definition of PIF is fulfilled.12,17 Repeated courses of chemotherapy have even been suggested to promote relapse or more aggressive disease in FLT3-ITD+ CN-AML.34
In patients transplanted beyond CR1, the different biology of the molecular subgroups was reflected by significant differences in characteristics at relapse and start of conditioning (Table 2). Within the favorable subgroup, patients' characteristics (longer CR1, lower numbers of blasts in BM and PB) indicated a less aggressive disease in spite of having relapsed. In contrast, patients with an unfavorable genotype showed a significantly shorter CR, including a remission of less than six months in 39% of patients who would have been regarded as primary refractory by many groups.10,35,36 Moreover, the FLT3-ITD+ subgroup was characterized by a higher number of patients with circulating blasts, and a higher leukemia burden in BM. As compared to the favorable genotype, OS and LFS after HSCT beyond CR1 were clearly inferior among patients showing an unfavorable genotype at time of diagnosis. No significant differences were observed among patients with double negative genotype and those harboring an FLT3-ITD. Consequently, the genotype at diagnosis was a decisive factor for OS after alloHSCT beyond CR1 in a multivariate analysis. Similarly, a higher CD34+ cell content in the graft was advantageous for OS, as it has been shown previously in advanced AML.12,37 No single explanation could be found within our data. However, higher CD34+ cell counts showed a trend for association with more cGvHD (cumulative incidence 38% vs. 20%, P=0.17).
In summary, these data show the efficacy of the FLAM-SA-RIC regimen for alloHSCT in advanced CN-AML. Patients with PIF had a promising outcome. In relapsed CN-AML, results after alloHSCT compared favorably to published data,8,9,25,38-40 although the prognostic significance of NPM1mut and FLT3-ITD was carried through. Confirmation of these findings in a larger cohort, and integration with other genetic aberrations and leukemogenic mechanisms are warranted for a more precise estimation of individual prognosis.41 Innovative strategies, such as integration of FLT3-specific thyrosine kinase inhibitors42 or novel cytotoxic drugs such as clofarabine43 into pre- and post HSCT treatment may be used to improve the results in patients with an unfavorable genotype.
Supplementary Material
Acknowledgments
The authors wish to thank all the nurses and physicians at the respective transplant units for their dedicated work. The help of the following data managers is also highly appreciated: Elke Dammann (Hannover), Karin David, (Wiesbaden), A. Franke, C. Lallinger and M. Rothmeyer (Munich) and A. Bader (Augsburg).
Funding: There is no specific funding to be reported in relation to the present study.
Footnotes
Authorship and Disclosures: Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Marcucci G, Haferlach T, Dohner H. Molecular genetics of adult acute myeloid leukemia: prognostic and therapeutic implications. J Clin Oncol. 2011;29(5):475-86 [DOI] [PubMed] [Google Scholar]
- 2.Dohner H, Estey E, Amadori S, Appelbaum F, Buchner T, Burnett A, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood. 2010; 115(3):453-74 [DOI] [PubMed] [Google Scholar]
- 3.Mrozek K, Marcucci G, Paschka P, Whitman SP, Bloomfield C. Clinical relevance of mutations and gene-expression changes in adult AML with normal cytogenetics: are we ready for a prognostically prioritized molecular classification? Blood.2007;109(2):431-48 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Schlenk R, Döhner K, Krauter J, Fröhling S, Corbacioglu A, Bullinger L, et al. Mutations and Treatment Outcome in Cytigenetically Normal Acute Myeloid Leukemia. N Engl J Med. 2008;358(18):1909-18 [DOI] [PubMed] [Google Scholar]
- 5.Brunet S, Labopin M, Esteve J, Cornelissen J, Socie G, Iori AP, et al. Impact of FLT3 Internal Tandem Duplication on the Outcome of Related and Unrelated Hematopoietic Transplantation for Adult Acute Myeloid Leukemia in First Remission: A Retrospective Analysis. J Clin Oncol. 2012;30(7):735-41 [DOI] [PubMed] [Google Scholar]
- 6.Bornhauser M, Illmer T, Schaich M, Soucek S, Ehninger G, Thiede C. Improved outcome after stem-cell transplantation in Flt3/ITD-positive AML. Blood. 2007;109(5):2264-5 [DOI] [PubMed] [Google Scholar]
- 7.Gale RE, Hills R, Kottaridis PD, Srirangan S, Wheatley K, Burnett A, et al. No evidence that Flt3 status should be considered as an indication for transplantation in Acute Myeloid Leukemia (AML): An analysis of 1135 patients excluiding APL from the UK MRC AML 10 and 12 trials. Blood. 2005;106:3658-65 [DOI] [PubMed] [Google Scholar]
- 8.Chevallier P, Prebet T, Pigneux A, Hunault M, Delaunay J, Perry F, et al. Influence of NPM1 and FLT3-ITD status on outcome in relapsed/refractory AML patients receiving salvage therapy including gemtuzumab ozogamicin. Leukemia. 2010;24(2):467-9 [DOI] [PubMed] [Google Scholar]
- 9.Wagner K, Damm F, Thol F, Gohring G, Gorlich K, Heuser M, et al. FLT3-internal tandem duplication and age are the major prognostic factors in patients with relapsed acute myeloid leukemia with normal karyotype. Haematologica. 2011;96(5):681-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chevallier P, Labopin M, Turlure P, Prebet T, Pigneux A, Hunault M, et al. A new Leukemia Prognostic Scoring System for refractory/relapsed adult acute myelogeneous leukaemia patients: a GOELAMS study. Leukemia. 2011;25(6):939-44 [DOI] [PubMed] [Google Scholar]
- 11.Schmid C, Schleuning M, Ledderose G, Tischer J, Kolb HJ. Sequential regimen of chemotherapy, reduced-intensity conditioning for allogeneic stem-cell transplantation, and prophylactic donor lymphocyte transfusion in high-risk acute myeloid leukemia and myelodysplastic syndrome. J Clin Oncol. 2005;23(24):5675-87 [DOI] [PubMed] [Google Scholar]
- 12.Schmid C, Schleuning M, Schwerdtfeger R, Hertenstein B, Mischak-Weissinger E, Bunjes D, et al. Long term survival in refractory acute myeloid leukemia after sequential treatment with chemotherapy and reduced intensity conditioning for allogeneic stem cell transplantation. Blood. 2006;108(3):1092-9 [DOI] [PubMed] [Google Scholar]
- 13.Cheson B, Benet JM, Kopecky KJ, Büchner T, Willman CL, Estey E, et al. Revised Recommendations of the International Working Group for Diagnostics, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J Clin Oncol. 2003;21(24):4642-9 [DOI] [PubMed] [Google Scholar]
- 14.Gratwohl A, Stern M, Brand R, Apperley J, Baldomero H, de Witte T, et al. Risk score for outcome after allogeneic hematopoietic stem cell transplantation: a retrospective analysis. Cancer. 2009;115(20):4715-26 [DOI] [PubMed] [Google Scholar]
- 15.Sullivan KM. Graft-versus-host-disease. In “Hematopoietic Cell Transplantation”. Thomas E, Blume K, Forman SJ, editors. 2nd, 515-536 1999. Boston,Blackwell Science; Ref Type: Serial (Book, Monograph) [Google Scholar]
- 16.Kern W, Schoch C, Haferlach T, Braess J, Unterhalt M, Wormann B, et al. Multivariate analysis of prognostic factors in patients with refractory and relapsed acute myeloid leukemia undergoing sequential high-dose cytosine arabinoside and mitoxantrone (S-HAM) salvage therapy: relevance of cytogenetic abnormalities. Leukemia 2000;14(2):226-31 [DOI] [PubMed] [Google Scholar]
- 17.Craddock C, Labopin M, Pillai S, Finke J, Bunjes D, Greinix H, et al. Factors predicting outcome after unrelated donor stem cell transplantation in primary refractory acute myeloid leukaemia. Leukemia. 2011;25(5):808-13 [DOI] [PubMed] [Google Scholar]
- 18.Ravandi F, Cortes J, Faderl S, O'Brien S, Garcia-Manero G, Verstovsek S, et al. Characteristics and outcome of patients with acute myeloid leukemia refractory to 1 cycle of high-dose cytarabine-based induction chemotherapy. Blood. 2010;116(26):5818-23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Estey E. Treatment of refractory AML. Leukemia. 1996;10(6):932-6 [PubMed] [Google Scholar]
- 20.Schoch C, Schnittger S, Bursch S, Gerstner D, Hochhaus A, Berger U, et al. Comparison of chromosome banding analysis, interphase- and hypermetaphase-FISH, qualitative and quantitative PCR for diagnosis and for follow-up in chronic myeloid leukemia: A study on 350 cases. Leukemia. 2002;53-9 [DOI] [PubMed] [Google Scholar]
- 21.Shaffer L, Slovak M, Campbell LJ, ISCN An international System for Human Cytogenetic Nomenclature. S. Karger, Basel, Switzerland, 2009 [Google Scholar]
- 22.Schnittger S, Schoch C, Dugas M, Kern W, Staib P, Wuchter C, et al. Analysis of FLT3 length mutations in 1003 patients with acute myeloid leukemia: correlation to cytogenetics, FAB subtype, and prognosis in the AMLCG study and usefulness as a marker for the detection of minimal residual disease. Blood. 2002;100(1):59-66 [DOI] [PubMed] [Google Scholar]
- 23.Schnittger S, Schoch C, Kern W, Mecucci C, Tschulik C, Martelli MF, et al. Nucleophosmin gene mutations are predictors of favorable prognosis in acute myelogenous leukemia with a normal karyotype. Blood. 2005;106(12):3733-9 [DOI] [PubMed] [Google Scholar]
- 24.Baldus CD, Thiede C, Soucek S, Bloomfield CD, Thiel E, Ehninger G. BAALC expression and FLT3 internal tandem duplication mutations in acute myeloid leukemia patients with normal cytogenetics: prognostic implications. J Clin Oncol. 2006;24(5):790-7 [DOI] [PubMed] [Google Scholar]
- 25.Duval M, Klein JP, He W, Cahn JY, Cairo M, Camitta BM, et al. Hematopoietic stem-cell transplantation for acute leukemia in relapse or primary induction failure. J Clin Oncol. 2010;28(23):3730-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Palmisano M, Grafone T, Ottaviani E, Testoni N, Baccarani M, Martinelli G. NPM1 mutations are more stable than FLT3 mutations during the course of disease in patients with acute myeloid leukemia. Haematologica. 2007;92(9):1268-9 [DOI] [PubMed] [Google Scholar]
- 27.Schnittger S, Kern W, Tschulik C, Weiss T, Dicker F, Falini B, et al. Minimal residual disease levels assessed by NPM1 mutation-specific RQ-PCR provide important prognostic information in AML. Blood. 2009;114(11):2220-31 [DOI] [PubMed] [Google Scholar]
- 28.Kronke J, Schlenk RF, Jensen KO, Tschurtz F, Corbacioglu A, Gaidzik VI, et al. Monitoring of minimal residual disease in NPM1-mutated acute myeloid leukemia: a study from the German-Austrian acute myeloid leukemia study group. J Clin Oncol. 2011;29(19):2709-16 [DOI] [PubMed] [Google Scholar]
- 29.Cloos J, Goemans B F,, Hess CJ, van Oostveen JW, Waisfisz Q, Corthals S, et al. Stability and prognostic influence of FLT3 mutations in paired initial and relapsed AML samples. Leukemia. 2006;20(7):1217-20 [DOI] [PubMed] [Google Scholar]
- 30.Bacher U, Haferlach C, Schnittger S, Kern W, Kroeger N, Zander AR, et al. Interactive diagnostics in the indication to allogeneic SCT in AML. Bone Marrow Transplant. 2009;43:745-56 [DOI] [PubMed] [Google Scholar]
- 31.Kayser S, Schlenk R F,, Londono MC, Breitenbuecher F, Wittke K, Du J, et al. Insertion of FLT3 internal tandem duplication in the tyrosine kinase domain-1 is associated with resistance to chemotherapy and inferior outcome. Blood. 2009;114(12):2386-92 [DOI] [PubMed] [Google Scholar]
- 32.Foran JM. New prognostic markers in acute myeloid leukemia: perspective from the clinic. Hematology Am Soc Hematol Educ Program. 2010:47-55 [DOI] [PubMed] [Google Scholar]
- 33.Damm F, Heuser M, Morgan M, Wagner K, Gorlich K, Grosshennig A, et al. Integrative prognostic risk score in acute myeloid leukemia with normal karyotype. Blood 2011;117(17):4561-8 [DOI] [PubMed] [Google Scholar]
- 34.Levis M. FLT3/ITD AML and the law of unintended consequences. Blood. 2011;117(26):6987-90 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Chevallier P, Delaunay J, Turlure P, Pigneux A, Hunault M, Garand R, et al. Long-term disease-free survival after gemtuzumab, intermediate-dose cytarabine, and mitoxantrone in patients with CD33(+) primary resistant or relapsed acute myeloid leukemia. J Clin Oncol. 2008;26(32):5192-7 [DOI] [PubMed] [Google Scholar]
- 36.Gupta V, Tallman MS, Weisdorf DJ. Allogeneic hematopoietic cell transplantation for adults with acute myeloid leukemia: myths, controversies, and unknowns. Blood. 2011;117(8):2307-18 [DOI] [PubMed] [Google Scholar]
- 37.Gorin NC, Labopin M, Boiron JM, Theorin N, Littlewood T, Slavin S, et al. Results of genoidentical hemopoietic stem cell transplantation with reduced intensity conditioning for acute myelocytic leukemia: higher doses of stem cells infused benefit patients receiving transplants in second remission or beyond--the Acute Leukemia Working Party of the European Cooperative Group for Blood and Marrow Transplantation. J Clin Oncol. 2006;24(24): 3959-66 [DOI] [PubMed] [Google Scholar]
- 38.Boissel N, Cayuela JM, Preudhomme C, Thomas X, Grardel N, Fund X, et al. Prognostic significance of FLT3 internal tandem repeat in patients with de novo acute myeloid leukemia treated with reinforced courses of chemotherapy. Leukemia. 2002;16(9):1699-704 [DOI] [PubMed] [Google Scholar]
- 39.Levis M, Ravandi F, Wang ES, Baer MR, Perl A, Coutre S, et al. Results from a randomized trial of salvage chemotherapy followed by lestaurtinib for patients with FLT3 mutant AML in first relapse. Blood. 2011;117(12):3294-301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kurosawa S, Yamaguchi T, Miyawaki S, Uchida N, Sakura T, Kanamori H, et al. Prognostic factors and outcomes of adult patients with acute myeloid leukemia after first relapse. Haematologica. 2010;95(11):1857-64 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Walker A, Marcucci G. Impact of molecular prognostic factors in cytogenetically normal acute myeloid leukemia at diagnosis and relapse. Haematologica. 2011;96(5): 640-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Metzelder S, Wang Y, Wollmer E, Wanzel M, Teichler S, Chaturvedi A, et al. Compassionate use of sorafenib in FLT3-ITD-positive acute myeloid leukemia: sustained regression before and after allogeneic stem cell transplantation. Blood. 2009;113(26):6567-71 [DOI] [PubMed] [Google Scholar]
- 43.Buchholz S, Dammann E, Stadler M, Krauter J, Beutel G, Trummer A, et al. Cytoreductive treatment with clofarabine/ara-C combined with reduced-intensity conditioning and allogeneic stem cell transplantation in patients with high-risk, relapsed, or refractory acute myeloid leukemia and advanced myelodysplastic syndrome. Eur J Haematol. 2012;88(1):52-60 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.