

Abstract
Although agranulocytosis as a side effect of clozapine is well known, there is scarcity of data with regard to thrombocytopenia associated with clozapine. In this report we describe a case of clozapine induced thrombocytopenia and review the existing literature. A 22 year old female patient developed thrombocytopenia while on clozapine 187.5 mg/day for 17 weeks. Thrombocytopenia persisted for 24 weeks even after reduction in the dose of clozapine and ultimately clozapine had to be stopped, which led to resolution of thrombocytopenia. Clozapine-induced thrombocytopenia is a less well-known, but potentially serious, adverse effect that should be screened for in practice. The case highlights the fact that besides monitoring the leucocyte count, platelet count of patients receiving clozapine should also be monitored.
Keywords: Clozapine, thrombocytopenia, platelet
INTRODUCTION
Clozapine has been known to cause haematological side effects like agranulocytosis, neutropenia, leucocytosis, eosinophilia and thrombocytopenia. Although some data is available with regard to leucopenia, data for thrombocytopenia is limited. In this report we present the case of a patient who developed thrombocytopenia with clozapine and review the existing literature.
CASE REPORT
A woman aged 22, suffering from paranoid schizophrenia (as diagnosed by DSM-IV) for the past three years, presented with an acute episode. She had received adequate trials of olanzapine, risperidone and quetiapine along with electroconvulsive therapy. There was history of severe extrapyramidal side effects with risperidone. Taking this into account she was started on clozapine. Prior to starting of clozapine her hemogram including platelet count did not reveal any abnormality. For the management of acute symptoms in view of the suicidal risk, she was treated with electroconvulsive therapy, lorazepam up to 4 mg/day and was started on clozapine and the dose was gradually increased to 187.5 mg/day over the period of four weeks because of side effects of hypersalivation and constipation. While clozapine was increased, leucocyte count and platelet counts were monitored regularly on weekly basis and serial monitoring did not reveal any abnormality. With this she achieved symptomatic remission following which lorazepam was stopped. While on clozapine 187.5 mg/day, low platelet count (101,000 and 98,000/μL on two occasions) was noted for the first time after 17 weeks of continuation of clozapine at the above said dose without reduction in the leucocyte count or haemoglobin levels. Following this monitoring was increased and platelet count kept on fluctuating between 1,20,000/μL to 1,35,000/μL. Over the period, platelet count started dropping. By another 24 weeks of clozapine therapy, the platelet count dropped to 60,000/μL without any reduction in the leucocyte count and the haemoglobin levels. The drop occurred despite reduction in the dose of clozapine upto 125 mg/day. Clozapine was stopped completely as a result. Throughout this period she never had any fever, skin rash, purpura, excessive menstrual bleeding or bleeding from any other source, arthritis, arthralgia, muscle pain and muscle weakness. Her investigations in the form of serum electrolytes, liver function test, renal function test, prothrombin time, bleeding time, clotting time and ultrasound abdomen and pelvis did not reveal any abnormality. She was also evaluated by physician and the opinion was that the low platelet count may be related to clozapine.
Within a week of stopping clozapine platelet counts started improving and by six weeks her platelet count was 1,80,000/μL. In the meanwhile, with stoppage of clozapine, she had relapse of symptoms and required inpatient care, was treated with electroconvulsive therapy, lorazepam and chlorpromazine, with which she achieved remission. During this period her platelet count remained within the normal range.
DISCUSSION
Thrombocytopenia is defined as platelet count of less than 100 × 109/L. Only two studies[1,2] and a small case series[3] have reported incidence of thrombocytopenia associated with clozapine and only few case reports have focused on this association.[4–10] The findings are summarized in Table 1.
Table 1.
Literature reporting clozapine associated thrombocytopenia
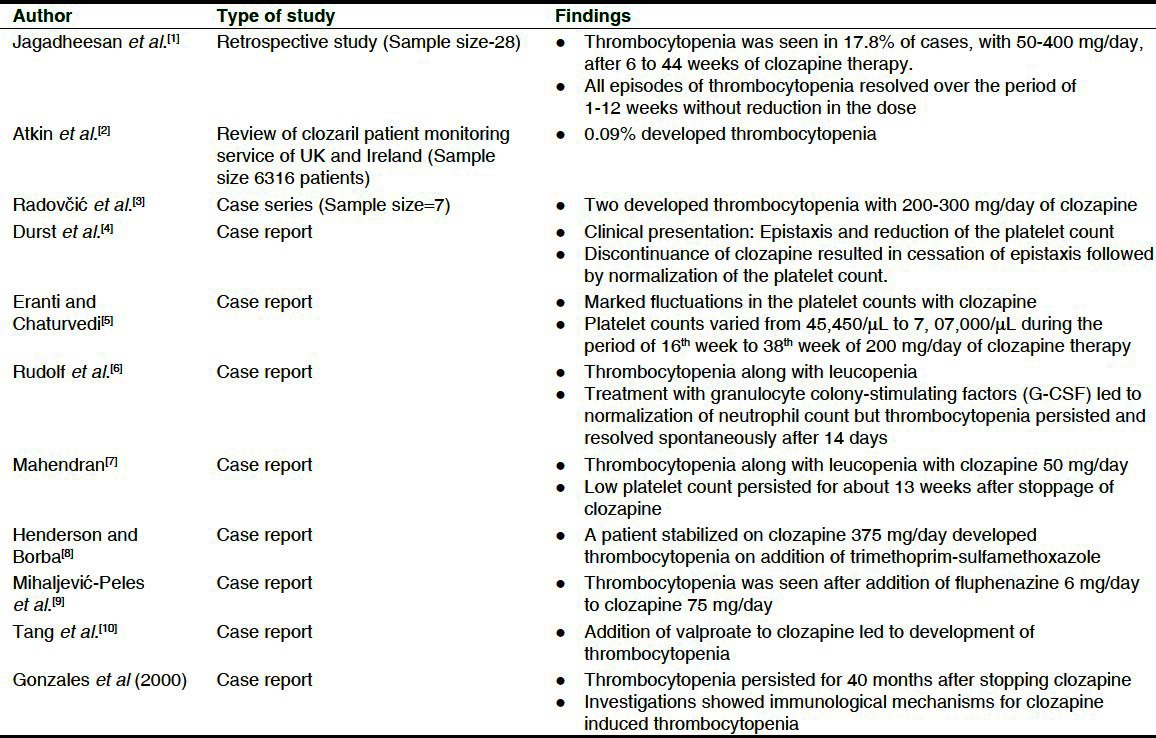
Although in most of the literature thrombocytopenia associated with clozapine has been reported to be transitory to at best last for 13 weeks, in a case report thrombocytopenia persisted for 40 months after stopping clozapine.[11] There are also few case reports of clozapine associated thrombocytosis.[12,13] In one of this case reports thrombocytosis was seen in a patient treated with granulocyte colony stimulating factor for clozapine associated agranulocytosis.[13] As with thrombocytopenia, an immunological mechanism is also suggested for development of thrombocytosis.
In the index case, thrombocytopenia was noted for the first time after 17 weeks of stable dose of clozapine, which kept on worsening with continuation of clozapine, even on the lower dose and subsided only after stoppage of clozapine and normalization of platelet count required six weeks. This clinical picture is consistent with the available literature in many aspects. However, in contrast to some of the reports, in the index case, platelet count kept on falling consistently with continuation of clozapine and improved only after stoppage of clozapine, suggesting that in certain cases the side effects may be transitory and can lead to fatal outcome.
From the above literature it can be concluded that there is a wide variation in the incidence of thrombocytopenia with clozapine, which possibly is influenced by the sample size studied. There is lack of consensus with regard to resolution, with some reports suggesting that resolution requires stoppage of clozapine, as was seen in the index case too; whereas others suggest that thrombocytopenia resolves on its own. Most of the available literature is silent about the possible mechanism, except for one report which demonstrated underlying immunological mechanism in a case of persistent thrombocytopenia even after stopping clozapine. Other authors have also suggested immunological mechanism for both thrombocytopenia and thrombocytosis with clozapine.[14]
Considering the fact that the thrombocytopenia may be transitory as suggested in some of the case reports, an informed decision about rechallenge must be made after weighing the risk and benefits.
From the above it can be concluded although rare, clozapine can lead to thrombocytopenia. Hence, besides monitoring the leucocyte count, platelet count of patients receiving clozapine should also be monitored.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Jagadheesan K, Agarwal SK, Nizamie SH. Clozapine-induced Thrombocytopenia: A Pilot Study. Hong Kong J Psychiatry. 2003;13:12–5. [Google Scholar]
- 2.Atkin K, Kendall F, Gould D, Freeman H, Licherman J, O’sullivan D. Neutropenia and agranulocytosis in patients receiving clozapine in the UK and Ireland. Br J Psychiatry. 1996;169:483–8. doi: 10.1192/bjp.169.4.483. [DOI] [PubMed] [Google Scholar]
- 3.Radovčić EP, Radeljak S, Palijan TZ, Sakic M, Kovac M. Clozapine induced thrombocytopenia: Clinical case report. Psychiatr Danub. 2009;21:140. [Google Scholar]
- 4.Durst R, Dorevitch A, Fraenkel Y. Platelet dysfunction associated with clozapine therapy. South Med J. 1993;86:1170–2. doi: 10.1097/00007611-199310000-00021. [DOI] [PubMed] [Google Scholar]
- 5.Savithasri Eranti V, Chaturvedi SK. Marked thrombocytopenia count variations without agranulocytosis due to clozapine. Indian J Psychiatry. 1998;40:300–2. [PMC free article] [PubMed] [Google Scholar]
- 6.Rudolf J, Grond M, Neveling M, Heiss WD. Clozapine-induced agranulocytosis and thrombopenia in a patient with dopaminergic psychosis. J Neural Transm. 1997;104:1305–11. doi: 10.1007/BF01294731. [DOI] [PubMed] [Google Scholar]
- 7.Mahendran R. Leucopenia and thrombocytopenia induced by clozapine. Hong Kong J Psychiatry. 2002;12:19–20. [Google Scholar]
- 8.Henderson DC, Borba CP. Trimethoprim-sulfamethoxazole and clozapine. Psychiatr Serv. 2001;52:111–2. doi: 10.1176/appi.ps.52.1.111. [DOI] [PubMed] [Google Scholar]
- 9.Mihaljević-Peles A, Jakovljevic M, Mrsic M, Sagud M. Thrombocytopenia associated with clozapine and fluphenazine. Nord J Psychiatry. 2001;55:449–50. [PubMed] [Google Scholar]
- 10.Tang C, Lee J, Hariram J. Thrombocytopenia with valproate and clozapine combination therapy. ASEAN J Psychiatry. 2011:12. [Google Scholar]
- 11.Gonzales MF, Elmore J, Luebbert C. Evidence for immune etiology in clozapine-induced thrombocytopenia of 40 months’ duration: A case report. CNS Spectr. 2000;5:17–8. doi: 10.1017/s1092852900007768. [DOI] [PubMed] [Google Scholar]
- 12.Hampson ME. Clozapine-induced thrombocytosis. Br J Psychiatry. 2000;176:400. doi: 10.1192/bjp.176.4.400-a. [DOI] [PubMed] [Google Scholar]
- 13.Dihingia S, Deka K, Bhuyan D, Mondal SK. Life-threatening thrombocytosis following GCSF treatment in a case of clozapine-induced agranulocytosis. Gen Hosp Psychiatry. 2012;34:320. doi: 10.1016/j.genhosppsych.2011.09.011. [DOI] [PubMed] [Google Scholar]
- 14.Marlowe K. Thrombocytosis due to clozapine treatment: Working towards an early marker for clozapine-induced agranulocytosis. Br J Psychiatry. 2000;177:372–3. doi: 10.1192/bjp.177.4.372-b. [DOI] [PubMed] [Google Scholar]