

Abstract
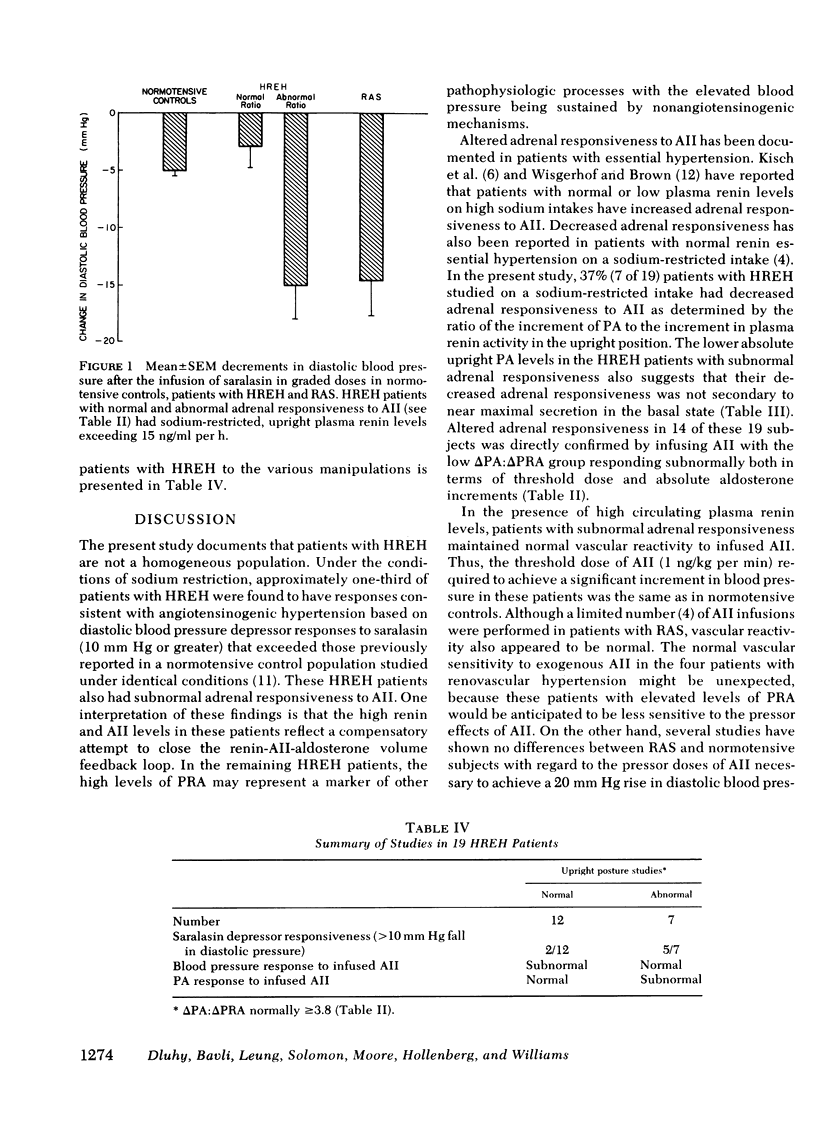
Adrenal responsiveness to angiotensin II (AII) and the diastolic blood pressure responses to saralasin were studied in 19 patients with high renin essential hypertension (HREH) on a 10-meq Na+/100 meq K+ diet. The increment in plasma renin activity (PRA) between supine and upright positions was used as an estimate of the acute stimulation of the adrenal gland by endogenous AII; the normal increment in plasma aldosterone divided by the increment in PRA was >3.8. 7 of 19 had abnormal upright posture responses with significantly greater mean PRA increments (24±6 ng/ml per h) and significantly smaller plasma aldosterone increments 47 ± 16 ng/dl) (P < 0.036) compared to the increments observed in HREH patients with normal adrenal responsiveness (PRA = 15 ± 1 ng/ml per h; plasma aldosterone = 87 ± 17 ng/dl). When AII was infused at doses of 0.1-3 ng/kg per min, only patients with normal posture responses had normal plasma aldosterone increments; plasma aldosterone levels failed to significantly increase even at the highest infusion rate in the patients with the abnormal upright posture responses. The AII competitive inhibitor, saralasin (0.3-30 μg/kg per min) was then infused to study the occurrence of angiotensinogenic hypertension in both HREH subgroups. The mean decline in diastolic blood pressure to saralasin in the subnormal adrenal responsive patients (−15 ± 3 mm Hg) was significantly greater than in the normal adrenal responsive group (−3 ± 2 mm Hg) (P < 0.02).
It is concluded that patients with HREH are not a homogeneous population; approximately one-third have AII-dependent hypertension. In these patients, the mechanism responsible for the elevated renin and blood pressure could be a compensatory increase secondary to decreased adrenal responsiveness to AII. In the remainder, the high PRA levels have little, if any, causal role in the pathogenesis of the hypertension but could reflect a marker of other pathophysiologic processes.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- AMES R. P., BORKOWSKI A. J., SICINSKI A. M., LARAGH J. H. PROLONGED INFUSIONS OF ANGIOTENSIN II AND NOREPINEPHRINE AND BLOOD PRESSURE, ELECTROLYTE BALANCE, AND ALDOSTERONE AND CORTISOL SECRETION IN NORMAL MAN AND IN CIRRHOSIS WITH ASCITES. J Clin Invest. 1965 Jul;44:1171–1186. doi: 10.1172/JCI105224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Case D. B., Wallace J. M., Keim H. J., Sealey J. E., Laragh J. H. Usefulness and limitations of saralasin, a partial competitive agonist of angioten II, for evaluating the renin and sodium factors in hypertensive patients. Am J Med. 1976 May 31;60(6):825–836. doi: 10.1016/0002-9343(76)90903-7. [DOI] [PubMed] [Google Scholar]
- Dustan H. P., Tarazi R. C., Frohlich E. D. Functional correlates of plasma renin activity in hypertensive patients. Circulation. 1970 Mar;41(3):555–567. doi: 10.1161/01.cir.41.3.555. [DOI] [PubMed] [Google Scholar]
- Emanuel R. L., Cain J. P., Williams G. H. Double antibody radioimmunoassay of renin activity and angiotensin II in human peripheral plasma. J Lab Clin Med. 1973 Apr;81(4):632–640. [PubMed] [Google Scholar]
- Esler M., Julius S., Zweifler A., Randall O., Harburg E., Gardiner H., DeQuattro V. Mild high-renin essential hypertension. Neurogenic human hypertension? N Engl J Med. 1977 Feb 24;296(8):405–411. doi: 10.1056/NEJM197702242960801. [DOI] [PubMed] [Google Scholar]
- Esler M., Zweifler A., Randall O., Julius S., DeQuattro V. The determinants of plasma-renin activity in essential hypertension. Ann Intern Med. 1978 Jun;88(6):746–752. doi: 10.7326/0003-4819-88-6-746. [DOI] [PubMed] [Google Scholar]
- Frohlich E. D., Kozul V. J., Tarazi R. C., Dustan H. P. Physiological comparison of labile and essential hypertension. Circ Res. 1970 Jul;27(1 Suppl 1):55–69. [PubMed] [Google Scholar]
- Hollenberg N. K., Chenitz W. R., Adams D. F., Williams G. H. Reciprocal influence of salt intake on adrenal glomerulosa and renal vascular responses to angiotensin II in normal man. J Clin Invest. 1974 Jul;54(1):34–42. doi: 10.1172/JCI107748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hollenberg N. K., Williams G. H., Adams D. F., Moore T., Brown C., Borucki L. J., Leung F., Bavli S., Solomon H. S., Passan D. Response to saralasin and angiotensin's role in essential and renal hypertension. Medicine (Baltimore) 1979 Mar;58(2):115–127. doi: 10.1097/00005792-197903000-00001. [DOI] [PubMed] [Google Scholar]
- Hollenberg N. K., Williams G. H., Burger B., Chenitz W., Hoosmand I., Adams D. F. Renal blood flow and its response to angiotensin II. An interaction between oral contraceptive agents, sodium intake, and the renin-angiotensin system in healthy young women. Circ Res. 1976 Jan;38(1):35–40. doi: 10.1161/01.res.38.1.35. [DOI] [PubMed] [Google Scholar]
- KAPLAN N. M., SILAH J. G. THE EFFECT OF ANGIOTENSIN II ON THE BLOOD PRESSURE IN HUMANS WITH HYPERTENSIVE DISEASE. J Clin Invest. 1964 Apr;43:659–669. doi: 10.1172/JCI104951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kisch E. S., Dluhy R. G., Williams G. H. Enhanced aldosterone response to angiotensin II in human hypertension. Circ Res. 1976 Jun;38(6):502–505. doi: 10.1161/01.res.38.6.502. [DOI] [PubMed] [Google Scholar]
- Moore T. J., Williams G. H., Dluhy R. G., Bavli S. Z., Himathongkam T., Greenfield M. Altered renin-angiotensin-aldosterone relationships in normal renin essential hypertension. Circ Res. 1977 Aug;41(2):167–171. doi: 10.1161/01.res.41.2.167. [DOI] [PubMed] [Google Scholar]
- Streeten D. H., Anderson G. H., Jr, Dalakos T. H. Angiotensin blockade: its clinical significance. Am J Med. 1976 May 31;60(6):817–824. doi: 10.1016/0002-9343(76)90894-9. [DOI] [PubMed] [Google Scholar]
- Tuck M. L., Williams G. H., Cain J. P., Sullivan J. M., Dluhy R. G. Relation of age, diastolic pressure and known duration of hypertension to presence of low renin essential hypertension. Am J Cardiol. 1973 Oct;32(5):637–642. doi: 10.1016/s0002-9149(73)80056-6. [DOI] [PubMed] [Google Scholar]
- Underwood R. H., Williams G. H. The simultaneous measurement of aldosterone, cortisol, and corticosterone in human peripheral plasma by displacement analysis. J Lab Clin Med. 1972 May;79(5):848–862. [PubMed] [Google Scholar]
- Williams G. H., Hollenberg N. K., Moore T. J., Swartz S. L., Dluhy R. G. The adrenal receptor for angiotensin II is altered in essential hypertension. J Clin Invest. 1979 Mar;63(3):419–427. doi: 10.1172/JCI109318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wisgerhof M., Brown R. D. Increased adrenal sensitivity to angiotensin II in low-renin essential hypertension. J Clin Invest. 1978 Jun;61(6):1456–1462. doi: 10.1172/JCI109065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yamamoto Y. Effect of pressor agents on blood pressure, plasma renin activity and plasma aldosterone concentration in essential hypertension. Jpn Heart J. 1975 Jul;16(4):404–420. doi: 10.1536/ihj.16.404. [DOI] [PubMed] [Google Scholar]