

Abstract
Rapid pull-through pressure profiles of the normal human upper esophageal sphincter (UES) were simultaneously studied with a conventional three-orifice Honeywell solid-state probe, an eight lumen radially perfused (RP) probe, and a circumferentially sensitive (CS) probe designed to measure UES pressure (UESP) without regard to probe orientation. Pressure curves were digitized and analyzed by computer. The Honeywell probe recorded significantly lower peak pressures than the other two methods, and had wide intrasubject pressure variations (average coefficient of variation, 53%). In contrast, UESP measured with the CS probe was constant for each subject (mean peak UESP, 121 mm Hg; average coefficient of variation, 15%). Anteroposterior RP probe UESP were identical to CS probe pressures. Thus, peak perfused anteroposterior UESP correlates with circumferentially measured sphincter squeeze.
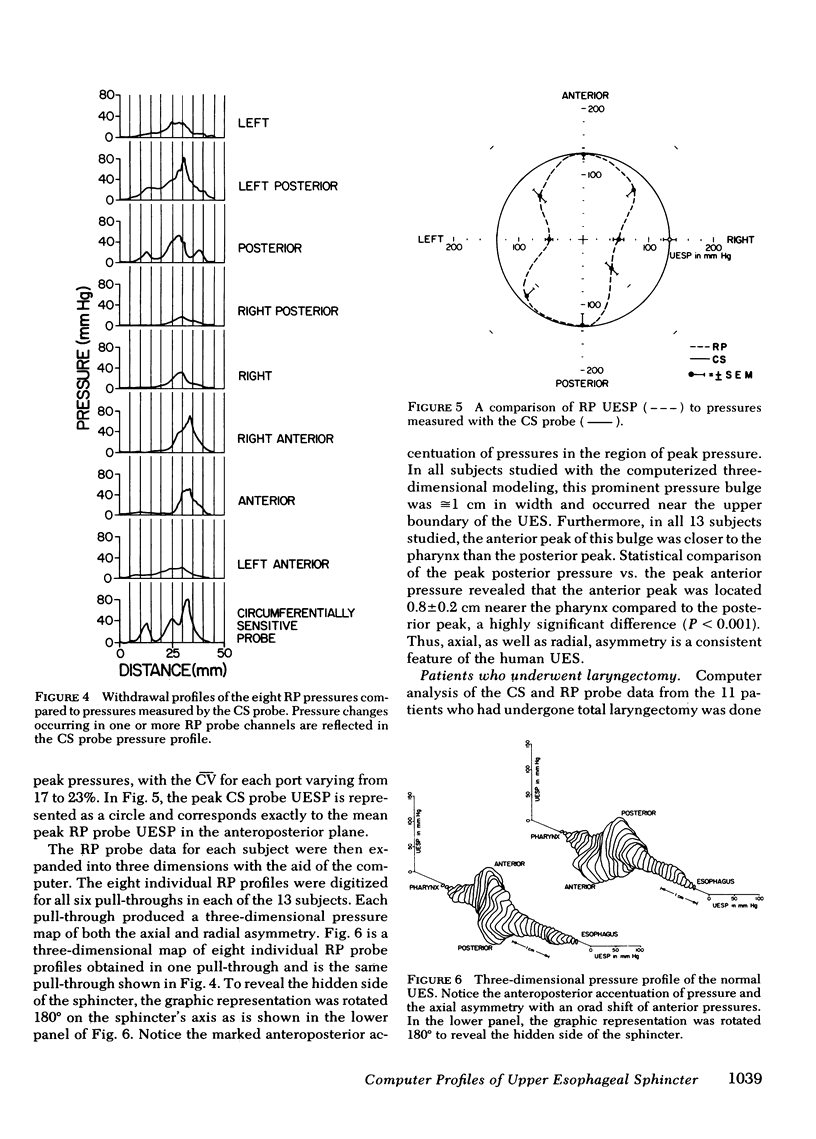
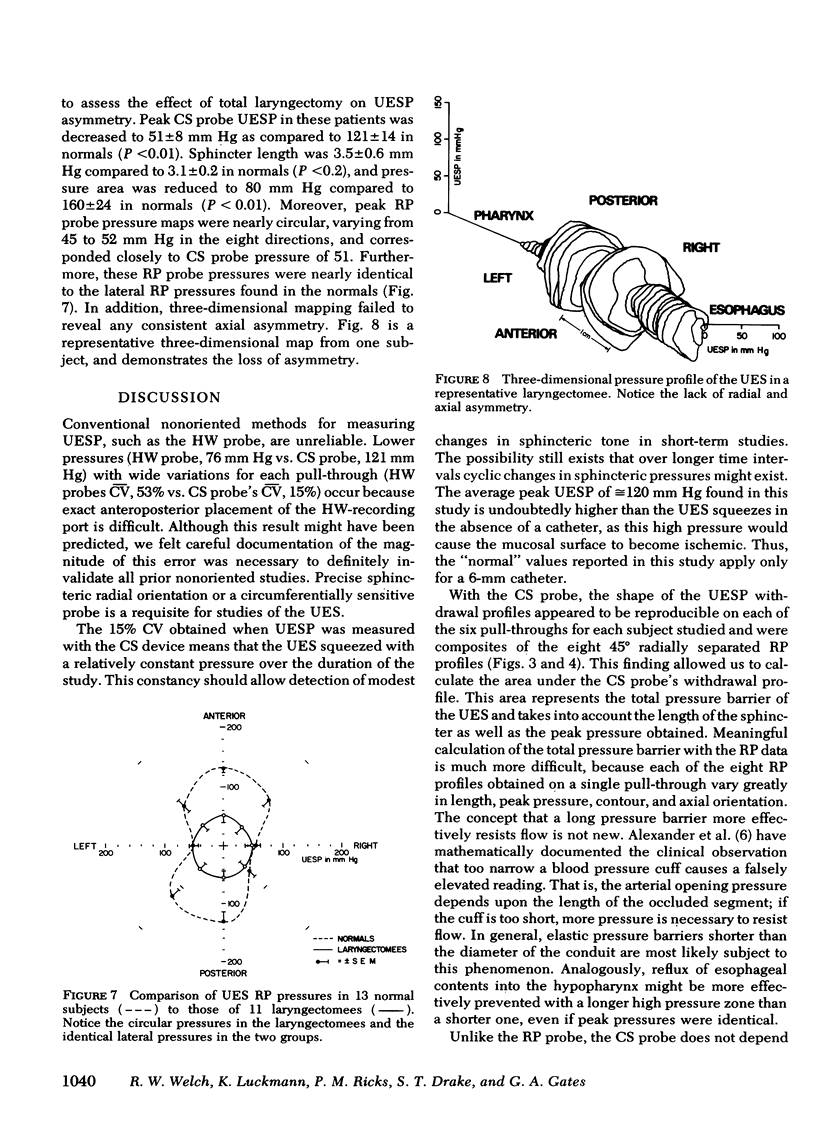
Computer programs were written that allowed RP probe pressures to be mapped in three dimensions. Normal three-dimensional maps were characterized by anteroposterior accentuation of peak pressures and also by consistent axial asymmetry with anterior peak pressures occurring 0.8±0.2 cm closer to the pharynx.
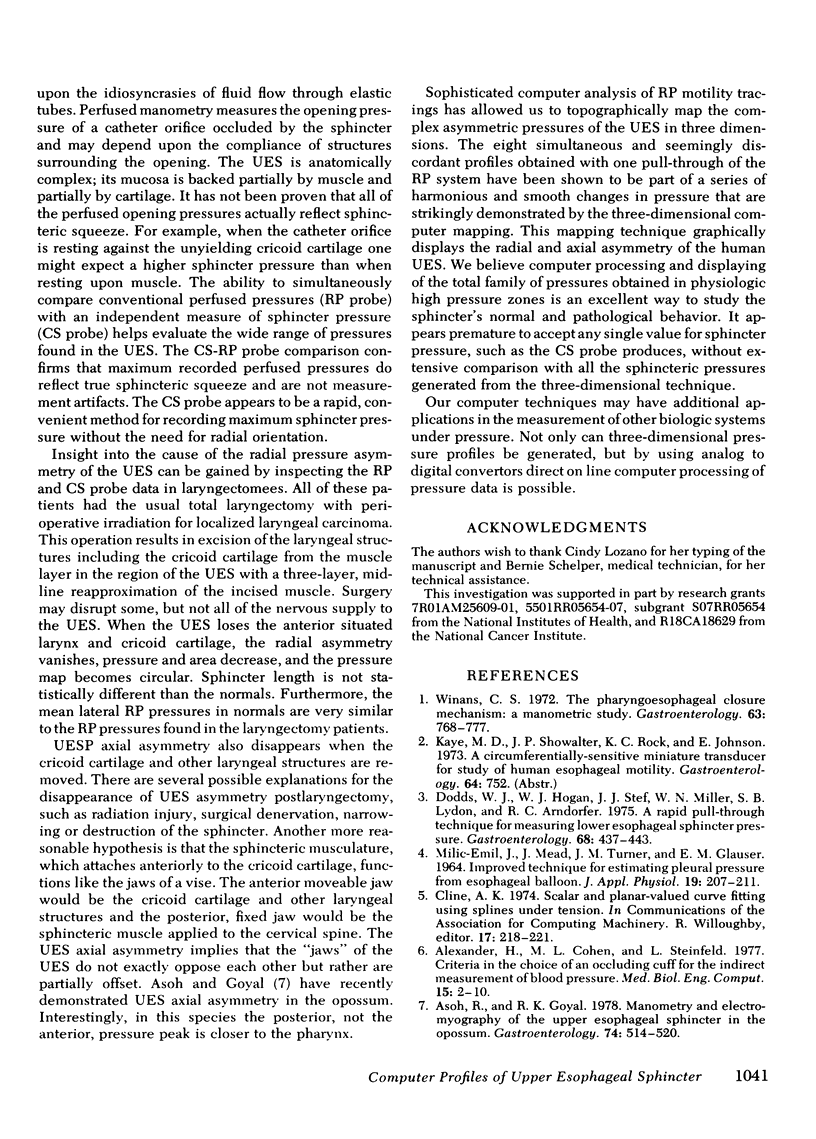
After defining the normal two- and three-dimensional UESP configuration, patients who had undergone laryngectomy were studied. Peak pressures measured with the RP probe decreased to ≅50 mm Hg and radial pressure asymmetry vanished. Like normals, CS probe pressures corresponded to peak RP probe pressures. UES length did not change significantly. Three-dimensional mapping showed that axial asymmetry also vanished. It therefore appears that the anatomic alterations produced by laryngectomy abolishes UESP asymmetry.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alexander H., Cohen M. L., Steinfeld L. Criteria in the choice of an occluding cuff for the indirect measurement blood pressure. Med Biol Eng Comput. 1977 Jan;15(1):2–10. doi: 10.1007/BF02441568. [DOI] [PubMed] [Google Scholar]
- Asoh R., Goyal R. K. Manometry and electromyography of the upper esophageal sphincter in the opossum. Gastroenterology. 1978 Mar;74(3):514–520. [PubMed] [Google Scholar]
- Dodds W. J., Hogan W. J., Stef J. J., Miller W. N., Lydon S. B., Arndorfer R. C. A rapid pull-through technique for measuring lower esophageal sphincter pressure. Gastroenterology. 1975 Mar;68(3):437–443. [PubMed] [Google Scholar]
- MILIC-EMILI J., MEAD J., TURNER J. M., GLAUSER E. M. IMPROVED TECHNIQUE FOR ESTIMATING PLEURAL PRESSURE FROM ESOPHAGEAL BALLOONS. J Appl Physiol. 1964 Mar;19:207–211. doi: 10.1152/jappl.1964.19.2.207. [DOI] [PubMed] [Google Scholar]
- Winans C. S. The pharyngoesophageal closure mechanism: a manometric study. Gastroenterology. 1972 Nov;63(5):768–777. [PubMed] [Google Scholar]