

Abstract
With the aim of reviewing critical concepts and producing recommendations for the management of chronic myelomonocytic leukemia, key questions were selected according to the criterion of clinical relevance. Recommendations were produced using a Delphi process and four consensus conferences involving a panel of experts appointed by the Italian Society of Hematology and affiliated societies. This report presents the final statements and recommendations, covering patient evaluation at diagnosis, diagnostic criteria, risk classification, first-line therapy, monitoring, second-line therapy and allogeneic stem cell transplantation. For the first-line therapy, the panel recommended that patients with myelodysplastic-type chronic myelomonocytic leukemia and less than 10% blasts in bone marrow should be managed with supportive therapy aimed at correcting cytopenias. In patients with myelodysplastic-type chronic myelomonocytic leukemia with a high number of blasts in bone marrow (≥10%), supportive therapy should be integrated with the use of 5-azacytidine. Patients with myeloproliferative-type chronic myelomonocytic leukemia with a low number of blasts (<10%) should be treated with cytoreductive therapy. Hydroxyurea is the drug of choice to control cell proliferation and to reduce organomegaly. Patients with myeloproliferative-type chronic myelomonocytic leukemia, and a high number of blasts should receive polychemotherapy. Both in myelodysplastic-type and myeloproliferative-type chronic myelomonocytic leukemia, allogeneic stem cell transplantation should be offered within clinical trials in selected patients.
Introduction
Chronic myelomonocytic leukemia (CMML) is classified by the WHO as a clonal hematopoietic malignancy characterized by features of both a myeloproliferative neoplasm and a myelodysplastic syndrome.1 CMML accounts for 10% of all cases of myelodysplastic syndromes;2,3 affected patients are diagnosed at a median age of 65–75 years, and there is a 2 to 1 male predominance.3 The most common symptoms of CMML are a reflection of the underlying cytopenia, hyper-catabolic syndrome, splenomegaly, or organ infiltration of monocytes. The disease presents with variable clinical phenotypes, the prognosis is generally poor, and effective therapies are limited.2 In recent years, array and sequencing technologies have provided new insights into the molecular pathogenesis of CMML.2 Molecular discoveries, however, have not yet been translated into changes in disease management. Therefore, therapy for CMML remains a challenge. For this reason, the Italian Society of Hematology (SIE) and affiliated Societies (the Italian Society of Experimental Hematology, SIES, and the Italian Group for Bone Marrow Transplantation, GITMO) decided to review recent data regarding diagnostic criteria, evaluation needs at diagnosis, assessment of prognostic risk, and determinants of therapeutic intervention, in order to produce recommendations aimed at helping to optimize and standardize CMML clinical management.
Methods
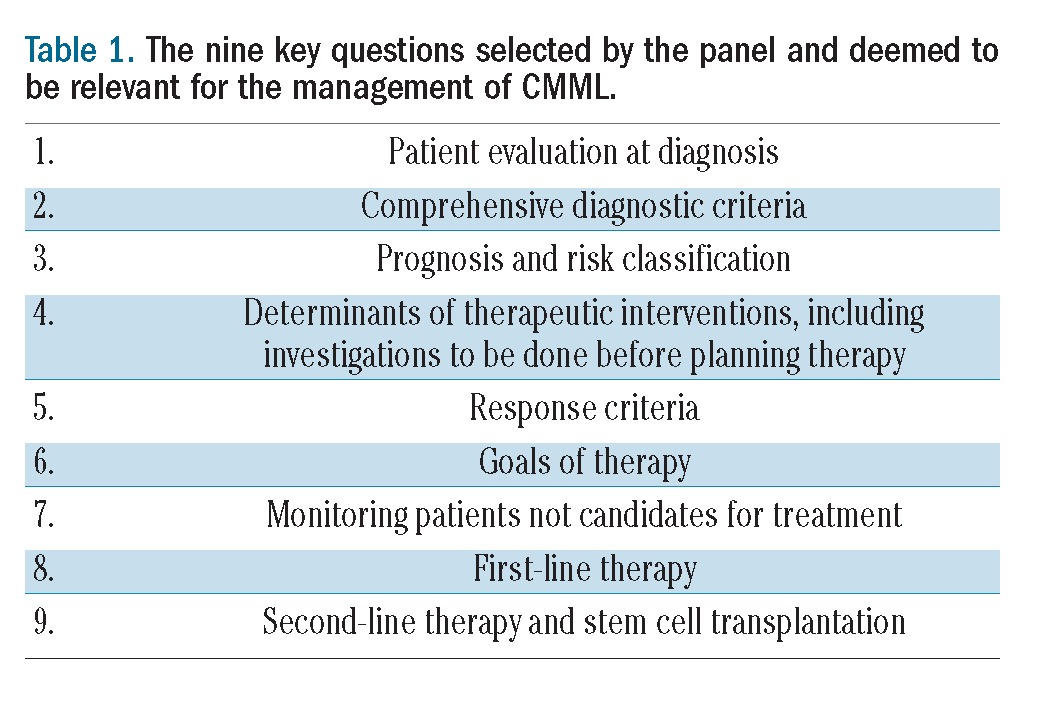
An expert panel of 8 hematologists with a long experience and scientific interest in CMML was selected. During an initial meeting on December 2011, the areas of major concern in the management of CMML were identified. Clinical key-questions were generated and rank-ordered using the criterion of clinical relevance (Table 1).
Table 1.
The nine key questions selected by the panel and deemed to be relevant for the management of CMML.
Each panelist drafted statements that addressed the key questions, and the remaining panelists scored their agreement with those statements providing suggestions for re-phrasing. To exploit this phase of the process, the Delphi questionnaire method was used.4 Finally, the panel met three times in Bologna, Italy, for consensus conferences. The nominal group technique5 was used according to which participants were first asked to comment in round-robin fashion on their preliminary votes and then to propose a new vote.
Results
Patient evaluation at diagnosis
The diagnosis of CMML relies largely on findings of bone marrow (BM) morphological dysplasia or clonal genetic abnormalities in patients with persistent peripheral blood monocytosis. Conventional cytogenetic analysis can allow clonal abnormalities to be indentifed, even if most patients with CMML exhibit a normal karyotype.6 The most frequent abnormalities involve chromosome 7, mostly consisting of monosomy, trisomy 8, and a complex karyotype involving 3 or more abnormalities.7
Several molecular gene mutations have been found in CMML.8–10 These mutations affect different cellular targets and processes, like RUNX19,11,12 (transcription regulation), isocitrate dehydrogenases IDH1/IDH213 (metabolism), KRAS, NRAS, CBL, and JAK29,14–17 (tyrosine-signaling pathways), TET2, DNMT3A, ASXL1, UTX, EZH28,18–21 (epigenetic regulatory mechanism), and SRSF222 (splicing regulation). Mutations involving the NRAS, KRAS, TET2, CBL and SRSF2 genes, and JAK2 V617F mutations are the most frequently reported.22 A comprehensive mutation analysis revealed that 93% of all CMML patients carried at least one somatic mutation in 9 recurrently mutated genes.22
Flow cytometry immunophenotyping may detect aberrancies in the monocytic lineage, including abnormal CD11b/HLA-DR, CD36/CD14, abnormal intensity of CD13, CD14, CD16, CD33, CD36, CD64, expression of CD34 and lineage infidelity markers, and overexpression of CD56.23–25 None of these aberrancies are specific for CMML.
Recommendations
The diagnostic workup of a suspected CMML should include: patient’s history aimed at excluding reactive causes of monocytosis (in particular, infectious diseases and solid tumors); physical examination (in particular, assessment of spleen size and search for cutaneous lesions); complete blood count and peripheral blood smear examination with differential leukocyte count; bone marrow aspiration and biopsy; conventional cytogenetic analysis; molecular assays to exclude bcr/abl fusion gene and rearrangement of PDGFRA and PDGFRB; any investigation necessary to exclude infectious diseases with monocytosis. A sample of bone marrow cells should be stored for possible further molecular analysis in centers where a certified tissue bank is available.
Useful diagnostic information gained from peripheral blood smear examination includes: monocyte count; presence of dysgranulopoiesis; presence of promonocytes, blasts, and neutrophil precursors. Useful diagnostic information from bone marrow aspiration is: presence of dysplasia in one or more myeloid lineages; granulocytic hyperplasia; percentage of blasts, that should include myeloblasts, monoblasts and promonocytes.
Staining of bone marrow biopsy sections should include hematoxylin-eosin or equivalent, immunostaining for CD34+ and monocytic cells (CD68R and CD163), and Gomori’s silver impregnation for fibrosis. Useful diagnostic information from BM biopsy is: marrow cellularity; dysplasia and hyperplasia of megakaryocyte compartment; blast count; and bone marrow fibrosis.
Conventional cytogenetic analysis should allow acquired clonal chromosomal abnormalities to be detected and t(9;22) and t(5;12) translocations excluded that are characteristic for chronic myeloid leukemia and MDS/MPN with eosinophilia, respectively.
In patients with negative t(9;22), bcr/abl fusion gene molecular assay should be performed to definitively exclude chronic myeloid leukemia. In the case of eosinophilia and negative t(5;12), the PDGFRA and PDGFRB rearrangement molecular assay should be performed in order to exclude MDS/MPN with eosinophilia.
The panel agreed that validation of potential diagnostic molecular biomarkers, like SRSF2, TET2, JAK2 or RAS mutations, and a better knowledge of their specificity is needed before they can be indicated for routine assessment in CMML patients at diagnosis.
Comprehensive diagnostic criteria
Diagnostic criteria proposed by the FAB group in the 1980s included: blood monocytes > 1×109/L; bone marrow blasts <20%, associated with dysplasia in erythroid, granulocytic, or megakaryocytic lineages; peripheral blasts < 5%; and absence of Auer rods in myeloid cells.26 Due to the variability of this presentation, in 1994 the FAB group distinguished “dysplastic” (MD-CMML) and “proliferative” (MP-CMML) variants, considering a white blood cell (WBC) count of 13×109/L as a cut-off point.27 In most of the studies investigating the prognostic significance of such a subdivision,28–34 median survival of patients with the MP-CMML turned out to be shorter than that of patients with the MD-variant, even though the observed differences were hardly ever statistically significant. On the contrary, the probability of transformation to acute myeloid leukemia (AML) was generally similar between the two subtypes of CMML.
In 2001, the WHO classification definitively separated CMML from MDS.35 A new group of diseases with both myelodysplastic and myeloproliferative features was established, named “myelodysplastic/myeloproliferative diseases” including CMML, atypical CMML, and juvenile CMML. WHO committees chose not to maintain the distinction between MD and MP CMML, but to divide CMML into two prognostic categories based on blast number: CMML-1 (blasts < 5% in blood and < 10% in BM) and CMML-2 (blasts 5–19% in blood and/or 10–19% in BM). A diagnostic sub-category of “CMML with eosinophilia” was recommended in cases where peripheral eosinophil counts resulted over 1.5×109/L.
The WHO classification was reviewed in 20081 and “myelodysplastic/myeloproliferative diseases” were renamed “myelodysplastic/myeloproliferative neoplasms”. A new subgroup, “myeloid and lymphoid neoplasm with eosinophilia and abnormalities of PDGRFA, PDGRFB and FGFR1”, was added. “CMML with eosinophilia” harboring PDGRFA or PDGRFB rearrangement was included in this new entity.
Recommendations
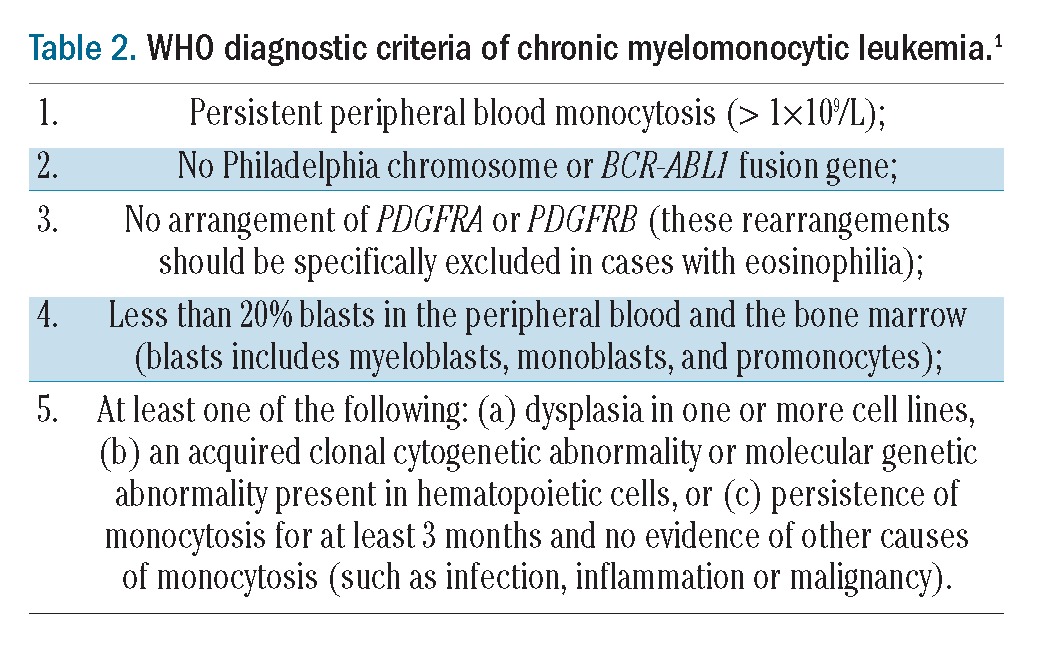
Diagnostic criteria for CMML are clearly set out in the WHO 2008 classification and their use is recommended (Table 2). We suggest that the distinction of CMML into MP- and MD-variants should be maintained in the diagnostic workup, since it retains importance due to the different therapeutic options that this may involve. For the time being, although arbitrary, a white blood cell count of 13×109/L is considered an appropriate cut-off point for this distinction.
Table 2.
WHO diagnostic criteria of chronic myelomonocytic leukemia.1
Prognosis and risk classification
In the past, patients with CMML were usually assessed for risk using scoring systems developed for MDS.36 In 2002, a specific prognostic scoring system was developed at the University of Texas MD Anderson Cancer Center (MDACC).37 This study identified a hemoglobin level (<12 vs. ≥12 g/dL), absolute number of lymphocytes (>2.5 vs. ≤2.5×109/L), the presence of immature myeloid cells (IMC) in the peripheral blood and marrow blast percentage (≥10 vs. <10%) as the variables independently associated to prognosis that could identify four subgroups of patients (low, intermediate-1, intermediate-2, and high risk, with median survival times of 26, 14, 9, and 5 months, respectively) showing significantly different life expectations (MDAPS). The association of higher lymphocyte counts with shorter survival has been confirmed by the MDS Düsseldorf Registry.38 A few years later, a slight modification of the MDAPS was proposed (MDAPS M1) replacing BM blasts with LDH, which allowed a slightly better stratification in four risk groups to be obtained in comparison to the original MDAPS.39
The presence of cytogenetic aberrations has been associated to shorter survival in CMML,37 in particular in patients with high-risk disease.39 A recent multivariate analysis of 414 CMML patients included in the Spanish MDS Registry confirmed the independent association of an abnormal karyotype (reported in 27% of patients) with poorer overall survival and a higher risk of AML evolution.40
Independent associations of molecular abnormalities with prognosis have been recently identified.14 Indeed, the presence of RAS point mutations appears to be significantly higher in MP-CMML than in MD-CMML (40% vs. 20%).41 The presence of EZH2 implies an unfavorable prognosis8 while mutation of ASXL1 correlates with evolution to AML and a shorter overall survival.18 The impact of TET2 mutations remains controversial.9,42 No impact of SRSF2 mutation on survival was observed.22 However, in the RUNX1 mutated sub-cohort, SRSF2 Pro95His had a favorable impact on overall survival.22 Most important, a recently concluded phase II trial in which 39 CMML patients were treated with decitabine suggested that lower CJUN and CMYB gene expression levels were independently associated with an improved overall outcome and survival.43 However, the value of somatic gene mutations in the prognosis of CMML has not been validated and no scoring system including such molecular aberrations has been developed.
Recommendations
Because life expectancy is so heterogeneous in CMML, risk assessment is highly recommended for clinical decision making in individual patients.
The CMML-1 and CMML-2 WHO classification is recommended for prognostic implications but it should not be considered sufficient on its own to discriminate between low- and high-risk patients. Additional clinical criteria should be taken into account to decide the timing and modalities of therapeutic interventions.
At present, there is no universally used validated CMML-specific risk classification system. The use of CMML specific risk-oriented systems (i.e. MDAPS, MDAPS-M1, Düsseldorf or Spanish Registry scores) for individual patient risk assessment is recommended, in particular for patients who are candidates for allogeneic HSCT or enrolled in clinical trials.
Determinants of therapeutic intervention
Although criteria for starting therapy in CMML have not yet been fully established, the panel reasoned that clinical relevance should be considered when deciding the criteria for starting therapy. Thus empirical values were selected for the severity of anemia, thrombocytopenia, percentage of blasts and immature myeloid cells. The panel agreed on the following recommendations.
Recommendations
Therapy should be started when the disease is symptomatic or progressive, and, in particular, when one of these events occurs: a) severe anemia (Hb less than 10 g/dL); b) percentage of blasts in peripheral blood >5% (including myeloblasts, monoblasts and promonocytes;) c) platelet count ≤ 50×109/L; d) WBC count ≥ 30×109/L; e) immature granulocytes ≥ 10% in peripheral blood; f) extramedullary manifestations of the disease, such as cutaneous or lymphnodal; g) symptomatic splenomegaly.
Response criteria and definition of resistance
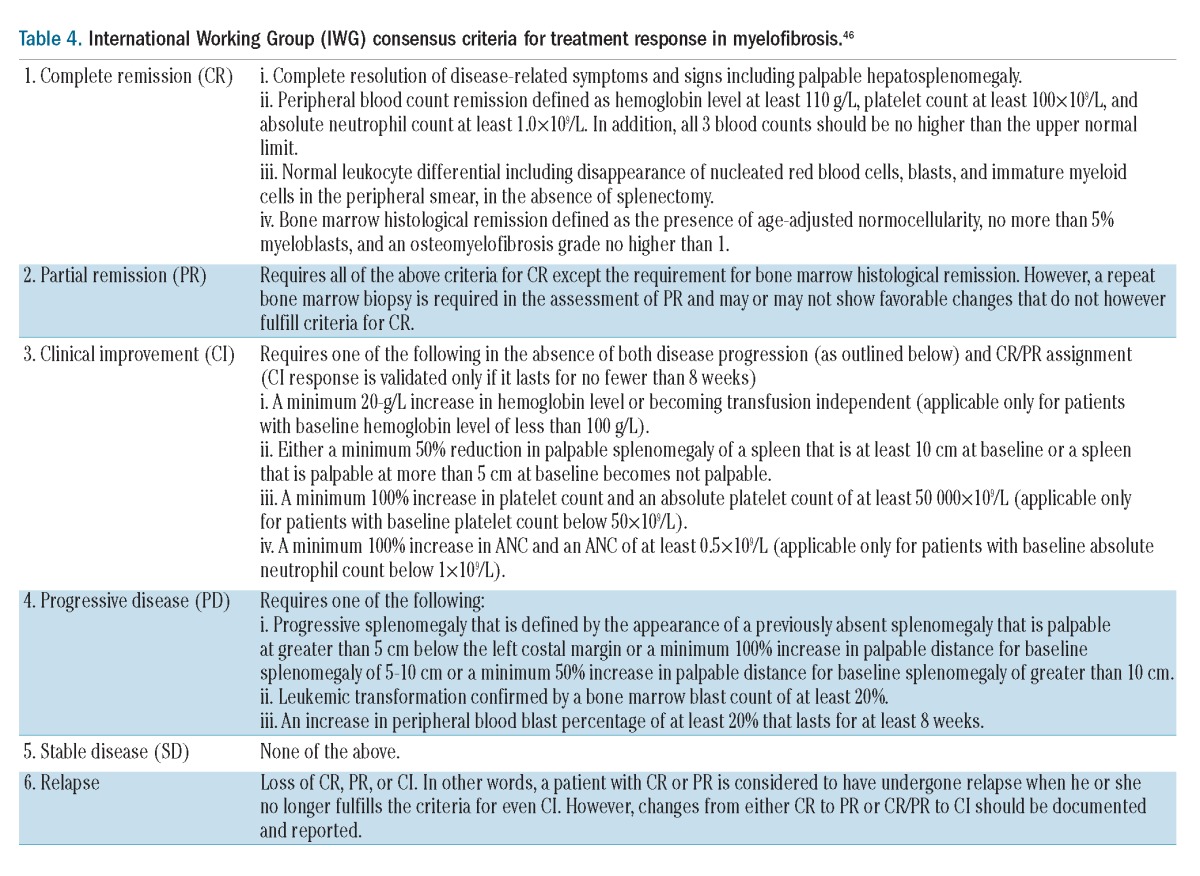
In 1996, Wattel et al. proposed five grades of response (clinical remission, good response, minor response, progression and stable disease) based on blood count, bone marrow aspirate and biopsy, and karyotype. However, these criteria were not used thereafter.44 Stressing the need for response criteria that are specific for CMML, the panel concluded that, at present, either the IWG 2006 response criteria for MDS or the IWG response criteria for myelofibrosis are appropriate for CMML in the myelodysplastic and myeloproliferative variants, respectively45,46 (Tables 3 and 4). There is no universally applied standardized definition of resistance/intolerance to first-line therapy (either hydroxyurea or 5-azacytidine) in CMML.
Table 3.
Modified IWG response criteria in myelodysplasia.45
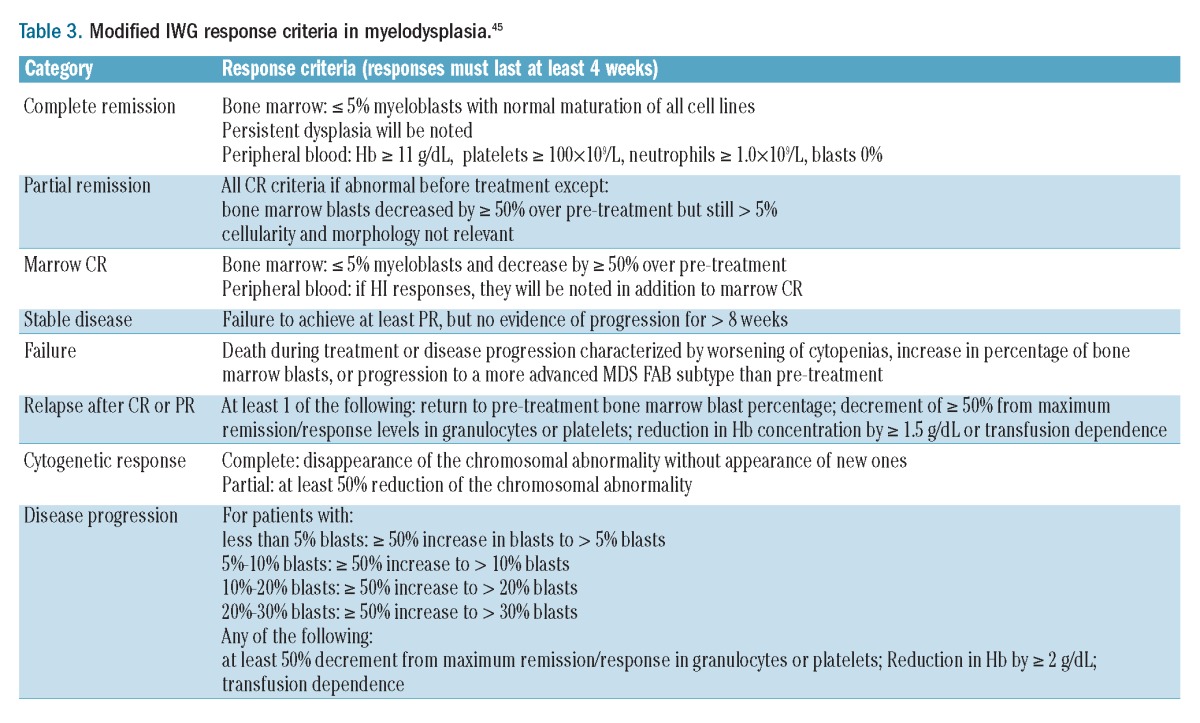
Table 4.
International Working Group (IWG) consensus criteria for treatment response in myelofibrosis.46
Recommendations
Response to treatment should be assessed according to the MD- and MP-disease classification at the time of treatment. For patients with MD-CMML, the IWG 2006 criteria for MDS (Table 3) should be applied. For patients with MP-CMML, the same set of IWG criteria of response used for primary myelofibrosis should be applied (IWG 2009 - Table 4). In both variants of the disease, the distinction of patients according to the WHO classification (CMML-1 vs. CMML-2) does not imply modifications of response criteria.
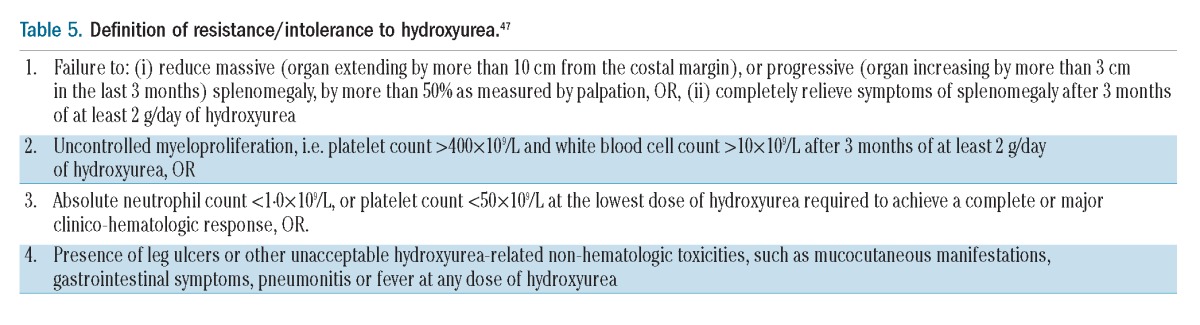
In MD-CMML, the absence of hematologic improvement after at least six cycles of 5-azacytidine and without progression of the disease should be defined as resistance. In MP-CMML, the same criteria used for defining resistance to hydroxyurea in myelofibrosis may be used47 (Table 5).
Table 5.
Definition of resistance/intolerance to hydroxyurea.47
Monitoring patients not candidates for treatment
The frequency of clinical and laboratory monitoring in patients who are not candidates for treatment should be initially set according to the individual disease characteristics and then adjusted depending on the natural clinical course.
Recommendations
Patients with MD-CMML who are not candidates for treatment should be monitored with a full blood count one month after diagnosis to assess the hematologic stability. These patients should then be monitored by full blood count and clinical examination every three months.
Patients with MP-CMML at diagnosis or evolving from an MD-CMML and not candidates for treatment, should be monitored monthly by full blood count for the first three months from diagnosis to exclude a rapid rise in WBC count or significant changes in other hematologic parameters, then by complete whole blood count and clinical examination every three months. Clinical examination should aim to evaluate spleen size, and the appearance of lymphoadenomegalies or extra-hematologic involvement (e.g. skin).
In cases of disease evolution from MD- to MP-CMML, as well as in cases of a significant increase in WBC count or a considerable spleen size enlargement in patients with a previously stable MP-CMML, hematologic and cytogenetic re-evaluation is recommended. Molecular evaluation should be considered, storing marrow cell DNA for further studies.
In patients not candidates for stem cell transplantation or any other possible experimental treatment, BM examination for blast count and cytogenetics should be performed once a year and in cases of relevant hematologic changes.
First-line therapy
Management of CMML is usually focused on supportive care and cytoreductive therapy, depending on the characteristics of individual patient’s disease (MD- vs. MP-CMML). Wattel et al. compared 1,000 mg/day of oral hydroxyurea (HU) to 150 mg/week of oral etoposide in 105 patients.44 After a median follow up of 11 months, 60% of patients in the HU arm responded compared with 36% in the etoposide arm. Median overall survival (OS) was statistically superior in the UH arm leading to the trial ending early.
Two randomized studies established the efficacy and safety of hypomethylating agents (5-azacitidine and decitabine) in a total of 361 patients with MDS.48,49 However, only 14 patients with CMML were enrolled in each of these studies. Although the responses for CMML patients were not reported separately in the trials, it was reported that there were no significant differences in response rates among patients with refractory anemia as compared to CMML. Only one out of the 7 CMML patients randomized to the decitabine arm had a response. 5-azacitidine and decitabine have been approved by the US FDA for the treatment of CMML. More restricted approval was given by the EMA who indicated 5-azacitidine for the treatment of CMML-2 in absence of myeloproliferative aspects (<13×109/L WBC) therefore allowing a treatment indication only in 10–20% of patients. Recently, Costa et al. retrospectively reviewed 38 CMML patients treated with two different schedules of 5-azacytidine and reported a 39% overall response rate (ORR) and a significantly improved survival in responders versus non-responders.50 In a retrospective study, clinical data of 31 patients with CMML consecutively treated with 5-azacitidine were collected.51 5-azacitidine was administered at 75 mg/m2 or 50 mg/m2 daily for 7 days, or at 100 mg daily for 5 or 7 days, every 4 weeks. Overall, 51% of the patients responded to the drug, with a high rate of complete remissions (CR), while hematologic improvement (HI) was obtained in 2 patients. The disease remained stable in 7 patients (SD, 23%) while 8 patients (26%) were resistant to the drug. Patients responding to 5-azacitidine had a better survival than those with SD or progression. The use of 5-azacytidine in MP-CMML is debated because at low doses the drug primarily acts as a demethylating agent, with minimal cytotoxicity that is unable to control high proliferation rates.52 In contrast to this observation, a recent study on a small group of 10 CMML patients treated with 5-azacytidine reported an ORR of 60%. Response was increased in proliferative CMML, with good control of leukocytosis and achievement of transfusion independence in 66% of the patients.53
Phase II studies using decitabine showed ORRs ranging from 38% to 70%.54,55 A recent trial of decitabine 20 mg/m2/day for 5 days carried out on a median of 10 cycles in CMML patients with advanced myeloproliferative or myelodysplastic features indicated an ORR of 38% and suggested that a lower CJUN and CMYB expression could be predictive of response.43
Intensive chemotherapy with intermediate doses of Ara-C and topotecan was investigated in a phase II trial in CMML, obtaining a CR rate of 44%, with a median remission duration of 33 weeks and a median survival of 41 weeks.56 Therapy with topotecan as single agent induced CR in 28% of CMML patients, with a median survival time of 10.5 months, and a median CR duration of 7.5 months.57 In a more recent trial in 90 patients with MDS and CMML treated with oral topotecan following 2 different schedules, the response rate in CMML patients was 50%, but no CR was reached.58
As CMML, especially in its proliferative variant, has the highest frequency of N- and K-RAS mutations among hematologic malignancies, farnesyl transferase inhibitors were considered potential effective drugs. Tipifarnib and lonafarnib were the most closely studied: unfortunately, both drugs, as single agents, were effective in only a few patients, resulting in limited disease control and leading to sporadic CR.59,60
In a pilot study, bendamustine was utilized in 15 pre-treated elderly patients with AML or high-risk MDS.61
Recommendations
Patients who start therapy later than three months from the diagnosis should have a pre-treatment re-evaluation, including BM aspiration, BM biopsy, and cytogenetic analysis. HLA typing is recommended for patients aged under 65 years. Serum erythropoietin should be determined in all patients with severe anemia (Hb ≤ 10 g/dL).
The treatment strategy should be decided first according to the disease hematologic phenotype, in particular whether it is an MP or MD phenotype, and to the number of blasts in BM.
Patients with MD-CMML and less than 10% blasts in BM should be managed with supportive therapy aimed at correcting cytopenias. Patients with severe anemia (Hb ≤ 10g/dL and with serum erythropoietin ≤ 500 mU/dL) should be treated with erythropoietic stimulating agents. Myeloid growth factors may be considered only for patients with febrile severe neutropenia.
In patients with MD-CMML with high number of blasts (≥10% in BM, ≥5% in the blood), the supportive therapy should be integrated with the use of hypomethylating agents (5-azacytidine or decitabine). In selected patients, allo-SCT may be offered within clinical trials.
Patients with MP-CMML with a low number of blasts should be treated with cytoreductive therapy. Hydroxyurea is the drug of choice to control proliferative myelomonocytic cells and to reduce organomegaly.
Patients with MP-CMML and a high number of blasts should receive blastolytic therapy with polychemotherapy followed, when possible, by allo-SCT.
If allo-SCT is not a possible option, patients should be informed that, although not curative, chemotherapy is recommended to maintain Quality of Life.
Second-line treatment
In the absence of any scientific evidence that could address the decision on second-line therapy in patients refractory or intolerant to first-line treatment, the panel approved the following recommendations.
Recommendations
Patients with MD-CMML with a high number of blasts, resistant or intolerant to 5-azacitidine, and not eligible for transplant, should be treated with supportive therapy and enrolled in experimental therapeutic studies.
In patients with MP-CMML and resistant or intolerant to hydroxyurea (Table 5) without blasts (<10%), cytolytic therapy should be given to control the disease and avoid a rapid increase in WBC count. VP16, low-dose ARA-C, thioguanine as single agents are reported to be efficacious. Hypomethylating agents should be used in the context of clinical trials. Patients with MP-CMML with a high blast count resistant to conventional blastolytic therapies should be treated with new and experimental therapies. Topoisomerase I inhibitors, farnesyl-transferase inhibitors or other drugs like bendamustine seem to have little effect as single agents.
Hematopoietic stem cell transplantation
Allo-SCT is the only strategy that may lead to cure in patients with CMML. However, due to the advanced age of the vast majority of patients, this treatment option is rarely feasible. Recently,62 a literature search was performed and data from adult CMML patients undergoing allo-SCT were reviewed. In all, 197 patients from eight studies63–70 met the final inclusion criteria. All studies were retrospective, 6 out of 8 (71%) being single institution experiences. The overall results of allogeneic SCT following myeloablative conditioning in CMML patients were disappointing, indicating a manifest excess mortality. The overall survival (OS) at 2–10 years ranged from 18% to 75% for all studies: relapse-free survival (RFS) ranged from 18% to 67%. Reduced intensity conditioning (RIC) transplant improved non-relapse mortality, OS and RFS without increasing the relapse rate.
Recommendations
The panel agreed that allo-SCT should be considered a therapeutic option in CMML for fit patients aged under 60 years with high-risk CMML requiring treatment. Its use should be considered experimental under a controlled strategy that investigates new pre-transplant therapies and transplant protocols. In MP-CMML and a high number of blasts, allo-SCT should be preceded by polychemotherapy, whereas in MD-CMML, 5-azacytidine may be considered before enrolling patients in a program of allo-SCT.
Discussion
Few recommendations in this work were grounded on strong scientific evidence, thus most of them reflect the uncertainty surrounding many issues in CMML. A critical issue in the disease assessment derives from recent comprehensive studies of somatic gene mutations. In these analyses, more than 80% of patients were found to have gene aberrations, and it has been hypothesized that such mutations, especially in the SRSF2, TET2, ASXL genes, represent disease-associated diagnostic markers. The panel concluded that these aberrancies must be validated before entering clinical practice. The hope is that integrating genetic lesions with traditional prognostic markers could lead to a better definition of risk classes, improving the indications for different therapeutic strategies.
The second issue is reflected in the recently revised WHO classification of CMML, which specifies hematologic, morphological and molecular parameters distinguishing two clinical CMML types on the basis of the number of blasts. However, the experts in this work considered that this distinction is not fully exploitable in therapeutic decision making. They believe that the previously reported distinction between myelodysplastic and myeloproliferative characteristics retains a clinical relevance in therapeutic decision making and that a validation of this distinction and correlation with genetic or molecular characteristics of the disease could improve patients’ stratification for therapy.
A difficult therapeutic decision is that of advising patients about allo-SCT. The panel recommended that allo-SCT should be performed as an experimental procedure. Nevertheless, by significantly reducing toxicities and extending the allo-SCT option to older patients, approaches based on reduced intensity conditioning transplant are definitely worth investigating in CMML.
Last-minute addendum
Since submission of the paper, a new CMML-specific prognostic scoring system (CPSS) has been published by Such et al.71 The most relevant variables for overall survival and evolution to acute myeloblastic leukemia were FAB and WHO CMML subtypes, CMML-specific cytogenetic risk classification, and RBC transfusion dependency. CPSS was able to segregate patients into four clearly different risk groups for OS and risk of AML evolution.
Acknowledgment
Authorship contribution: GB and ST designed the research. FO, GL, LM, EM, VS, GS and ST formed the panel of experts who produced recommendations. FO and GB wrote the preliminary version of the paper. All authors participated in writing significant sections of the paper.
Footnotes
Funding
Funding of the project was provided by SIE, SIES, and GITMO societies. The SIE administered all aspects of the meetings.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. (eds.): WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. IARC: Lyon, 2008 [Google Scholar]
- 2.Parikh SA, Tefferi A. Chronic myelomonocytic leukemia: 2012 update on diagnosis, risk stratification, and management. Am J Hematol. 2012;87(6):610–9 [DOI] [PubMed] [Google Scholar]
- 3.Beran M. Chronic myelomonocytic leukemia. Cancer Treat Res. 2008;142:107–32 [DOI] [PubMed] [Google Scholar]
- 4.Williams PL, Webb C. The Delphi technique: a methodological discussion. J Adv Nurs. 1994;19(1):180–6 [DOI] [PubMed] [Google Scholar]
- 5.Delbecq AL, van de Ven AH, Gustafson DH. Group Techniques for Program Planning: A guide to nominal group and Delphi processes. Scott, Foresman and Co; Glenview, IL, USA: 1975 [Google Scholar]
- 6.Bacher U, Haferlach T, Kern W, Hiddemann W, Schnittger S, Schoch C. Conventional cytogenetics of myeloproliferative diseases other than CML contribute valid information. Ann Hematol. 2005;84 (4):250–7 [DOI] [PubMed] [Google Scholar]
- 7.Haase D, Germing U, Schanz J, Pfeilstöcker M, Nösslinger T, Hildebrandt B, et al. New insights into the prognostic impact of the karyotype in MDS and correlation with subtypes: Evidence from a core dataset of 2124 patients. Blood. 2007;110(13):4385–95 [DOI] [PubMed] [Google Scholar]
- 8.Grossmann V, Kohlmann A, Eder C, Haferlach C, Kern W, Cross NC, et al. Molecular profiling of chronic myelomonocytic leukemia reveals diverse mutations in >80% of patients with TET2 and EZH2 being of high prognostic relevance. Leukemia. 2011;25(5):877–9 [DOI] [PubMed] [Google Scholar]
- 9.Kohlmann A, Grossmann V, Klein HU, Schindela S, Weiss T, Kazak B, et al. Next-generation sequencing technology reveals a characteristic pattern of molecular mutations in 72.8% of chronic myelomonocytic leukemia by detecting frequent alterations in TET2, CBL, RAS, and RUNX1. J Clin Oncol. 2010;28(24):3858–65 [DOI] [PubMed] [Google Scholar]
- 10.Jankowska AM, Makishima H, Tiu RV, Szpurka H, Huang Y, Traina F, et al. Mutational spectrum analysis of chronic myelomonocytic leukemia includes genes associated with epigenetic regulation: UTX, EZH2, and DNMT3A. Blood. 2011; 118(14):3932–41 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Asou N. The role of a Runt domain transcription factor AML1/RUNX1 in leukemogenesis and its clinical implications. Crit Rev Oncol Hematol. 2003;45(12):129–50 [DOI] [PubMed] [Google Scholar]
- 12.Kuo MC, Liang DC, Huang CF, Shih YS, Wu JH, Lin TL, et al. RUNX1 mutations are frequent in chronic myelomonocytic leukemia and mutations at the C-terminal region might predict acute myeloid leukemia transformation. Leukemia. 2009; 23(8):1426–31 [DOI] [PubMed] [Google Scholar]
- 13.Ward PS, Patel J, Wise DR, Abdel-Wahab O, Bennett BD, Coller HA, et al. The common feature of leukemia-associated IDH1 and IDH2 mutations is a neomorphic enzyme activity converting alpha-ketoglutarate to 2-hydroxyglutarate. Cancer Cell. 2010;17(3):225–34 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gelsi-Boyer V, Trouplin V, Adélaïde J, Aceto N, Remy V, Pinson S, et al. Genome profiling of chronic myelomonocytic leukemia: Frequent alterations of RAS and RUNX1 genes. BMC Cancer. 2008;8:299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ricci C, Fermo E, Corti S, Molteni M, Faricciotti A, Cortelezzi A, et al. RAS mutations contribute to evolution of chronic myelomonocytic leukemia to the proliferative variant. Clin Cancer Res. 2010;16(18): 2246–56 [DOI] [PubMed] [Google Scholar]
- 16.Pich A, Riera L, Sismondi F, Godio L, Davico Bonino L, Marmont F, et al. JAK2V617F activating mutation is associated with the myeloproliferative type of chronic myelomonocytic leukaemia. J Clin Pathol. 2009;62(9):798–801 [DOI] [PubMed] [Google Scholar]
- 17.Grand FH, Hidalgo-Curtis CE, Ernst T, Zoi K, Zoi C, McGuire C, et al. Frequent CBL mutations associated with 11q acquired uniparental disomy in myeloproliferative neoplasms. Blood. 2009;113(24):6182–92 [DOI] [PubMed] [Google Scholar]
- 18.Gelsi-Boyer V, Trouplin V, Adélaïde J, Bonansea J, Cervera N, Carbuccia N, et al. Mutations of polycomb-associated gene ASXL1 in myelodysplastic syndromes and chronic myelomonocytic leukaemia. Br J Haematol. 2009;145(6):788–800 [DOI] [PubMed] [Google Scholar]
- 19.Abdel-Wahab O, Pardanani A, Patel J, Wadleigh M, Lasho T, Heguy A, et al. Concomitant analysis of EZH2 and ASXL1 mutations in myelofibrosis, chronic myelomonocytic leukemia and blast-phase myeloproliferative neoplasms. Leukemia 2011;25(7):1200–2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tefferi A, Lim KH, Abdel-Wahab O, Lasho TL, Patel J, Patnaik MM, et al. Detection of mutant TET2 in myeloid malignancies other than myeloproliferative neoplasms: CMML, MDS, MDS/MPN and AML. Leukemia. 2009;23(7):1343–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jankowska AM, Szpurka H, Tiu RV, Makishima H, Afable M, Huh J, et al. Loss of heterozygosity 4q24 and TET2 mutations associated with myelodysplastic/myeloproliferative neoplasms. Blood. 2009;113(25):6403–10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Meggendorfer M, Roller A, Haferlach T, Eder C, Dicker F, Grossmann V, et al. SRSF2 mutations in 275 cases with chronic myelomonocytic leukemia (CMML). Blood. 2012;120(15):3080–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Rashidi HH, Xu X, Wang HY, Shafi NQ, Rameshkumar K, Messer K, et al. Utility of peripheral blood flow cytometry in differentiating low grade versus high grade myelodysplastic syndromes (MDS) and in the evaluation of cytopenias. Int J Clin Exp Pathol. 2012;5(3):224–30 [PMC free article] [PubMed] [Google Scholar]
- 24.Bellos F, Alpermann T, Gouberman E, Haferlach C, Schnittger S, Haferlach T, et al. Evaluation of flow cytometric assessment of myeloid nuclear differentiation antigen expression as a diagnostic marker for myelodysplastic syndromes in a series of 269 patients. Cytometry B Clin Cytom. Cytometry B Clin Cytom. 2012;82 (15):295–304 [DOI] [PubMed] [Google Scholar]
- 25.Rollins-Raval MA, Roth CG. The value of immunohistochemistry for CD14, CD123, CD33, myeloperoxidase and CD68R in the diagnosis of acute and chronic myelomonocytic leukaemias. Histopathology. 2012;60 (6):933–42 [DOI] [PubMed] [Google Scholar]
- 26.Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton DA, Gralnick HR, et al. Proposals for the classification of the myelodysplastic syndromes. Br J Haematol. 1982;51(2):189–99 [PubMed] [Google Scholar]
- 27.Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton DA, Gralnick H, et al. The chronic myeloid leukaemias: guidelines for distinguishing chronic granulocytic, atypical chronic myeloid, and chronic myelomonocytic leukaemia. Proposals by the French–American–British Cooperative Leukaemia Group. Br J Haematol. 1994;87 (4):746–54 [DOI] [PubMed] [Google Scholar]
- 28.Germing U, Gattermann N, Minning H, Heyll A, Aul C. Problems in the classification of LMMC--dysplastic versus proliferative type. Leuk Res. 1998;22(10):871–8 [DOI] [PubMed] [Google Scholar]
- 29.Voglová J, Chrobák L, Neuwirtová R, Malasková V, Straka L. Myelodysplastic and myeloproliferative type of chronic myelomonocytic leukemia - distinct subgroups or two stages of the same disease? Leuk Res. 2001;25(6):493–9 [DOI] [PubMed] [Google Scholar]
- 30.Nösslinger T, Reisner R, Grüner H, Tüchler H, Nowotny H, Pittermann E, et al. Dysplastic versus proliferative LMMC - a retrospective analysis of 91 patients from a single institution. Leuk Res. 2001;25 (9):741–7 [DOI] [PubMed] [Google Scholar]
- 31.Onida F, Kantarjian H, Ball G, Estey E, Keating MJ, Glassman A, et al. The dysplastic versus proliferative classification dilemma of chronic myelomonocytic leukemia: a retrospective single institution analysis of 273 patients. Blood. 2001, 98;11 (1 Suppl): 622A–623A [Google Scholar]
- 32.Cervera J, Sanz GF, Vallespi T, del Cañizo MC, Irriguible D, Löpez F, et al. Does WBC count really define two different subtypes of chronic myelomonocytic leukemia (LMMC)? Analysis of a series of 119 patients. Leuk Res. 1997;21(4):S7 [Google Scholar]
- 33.González-Medina I, Bueno J, Torre-quebrada A, López A, Vallespí T, Massagué I, et al. Two groups of chronic myelomonocytic leukaemia: myelodysplastic and myeloproliferative. Prognostic implications in a series of a single center. Leuk Res. 2002;26(9):821–4 [DOI] [PubMed] [Google Scholar]
- 34.Breccia M, Cannella L, Frustaci A, Stefanizzi C, D’Elia GM, Alimena G, et al. Chronic myelomonocytic leukemia with antecedent refractory anemia with excess blasts: further evidence for the arbitrary nature of current classification systems. Leuk Lymphoma. 2008;49(7):1292–6 [DOI] [PubMed] [Google Scholar]
- 35.Jaffe E, Harris NL, Stein HS, Vardiman JW. (eds.). Pathology and genetics of tumours of haematopoietic and lymphoid tissue. World Health Organization classification of tumours. Lyon: IARC Press, 2001, pp. 35–38 [Google Scholar]
- 36.Greenberg P, Cox C, LeBeau MM, Fenaux P, Morel P, Sanz G, et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood. 1997;89(6):2079–88 [PubMed] [Google Scholar]
- 37.Onida F, Kantarjian HM, Smith TL, Ball G, Keating MJ, Estey EH, et al. Prognostic factors and scoring systems in chronic myelomonocytic leukemia: a retrospective analysis of 213 patients. Blood. 2002;99 (3):840–9 [DOI] [PubMed] [Google Scholar]
- 38.Germing U, Strupp C, Alvado M, Gattermann N. New Prognostic parameters for myelomonocytic leukemia. Blood. 2002;100(2):731–3 [DOI] [PubMed] [Google Scholar]
- 39.Beran M, Wen S, Shen Y, Onida F, Jelinek J, Cortes J, et al. Prognostic factors and risk assessment in chronic myelomonocytic leukemia: validation study of the M.D. Anderson Prognostic Scoring System. Leuk Lymphoma. 2007;48(6):1150–60 [DOI] [PubMed] [Google Scholar]
- 40.Such E, Cervera J, Costa D, Solé F, Vallespí T, Luño E, et al. Cytogenetic risk stratification in chronic myelomonocytic leukemia. Haematologica. 2011;96(3):375–83 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Onida F, Gatto S, Scappini B, Ricci C, Ball G, Cortes J, et al. Significance of Ras point mutations for prognosis and response to treatment in chronic myelomonocytic leukemia: analysis of 112 patients. Proc Am Soc Clin Oncol. 2002;21:263a(1048) [Google Scholar]
- 42.Kosmider O, Gelsi-Boyer V, Ciudad M, Racoeur C, Jooste V, Vey N, et al. TET2 gene mutation is a frequent and adverse event in chronic myelomonocytic leukemia. Haematologica. 2009;94(12): 1676–81 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Braun T, Itzykson R, Renneville A, de Renzis B, Dreyfus F, Laribi K, et al. Molecular predictors of response to decitabine in advanced chronic myelomonocytic leukemia: a phase 2 trial. Blood. 2011;118(14):3824–31 [DOI] [PubMed] [Google Scholar]
- 44.Wattel E, Guerci A, Hecquet B, Economopoulos T, Copplestone A, Mahé B, et al. A randomized trial of hydroxyurea versus VP16 in adult chronic myelomonocytic leukemia. Groupe Francais des Myelodysplasies and European CMML Group Blood. 1996;88(17):2480–7 [PubMed] [Google Scholar]
- 45.Cheson BD, Greenberg PL, Bennett JM, Lowenberg B, Wijermans PW, Nimer SD, et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood. 2006;108(2):419–25 [DOI] [PubMed] [Google Scholar]
- 46.Tefferi A, Barosi G, Mesa RA, Cervantes F, Deeg HJ, Reilly JT, et al. International Working Group (IWG) consensus criteria for treatment response in myelofibrosis with myeloid metaplasia, for the IWG for Myelofibrosis Research and Treatment (IWG-MRT). Blood. 2006;108(5):1497–503 [DOI] [PubMed] [Google Scholar]
- 47.Barosi G, Birgegard G, Finazzi G, Griesshammer M, Harrison C, Hasselbalch H, et al. A unified definition of clinical resistance and intolerance to hydroxycarbamide in polycythaemia vera and primary myelofibrosis: results of a European LeukemiaNet (ELN) consensus process. Br J Haematol. 2010;148(6):961–3 [DOI] [PubMed] [Google Scholar]
- 48.Silverman LR, Demakos EP, Peterson BL, Kornblith AB, Holland JC, Odchimar-Reissig R, et al. Randomized controlled trial of azacitidine inpatients with the myelodysplastic syndrome: a study of the cancer and leukemia group B. J Clin Oncol. 2002;20(10):2429–40 [DOI] [PubMed] [Google Scholar]
- 49.Kantarjian H, Issa JP, Rosenfeld CS, Bennett JM, Albitar M, DiPersio J, et al. Decitabine improves patient outcomes in myelodysplastic syndromes: results of a phase III randomized study. Cancer. 2006;106(8):1794–803 [DOI] [PubMed] [Google Scholar]
- 50.Costa R, Abdulhaq H, Haq B, Shadduck RK, Latsko J, Zenati M, et al. Activity of azacitidine in chronic myelomonocytic leukemia. Cancer. 2011;117(12):2690–6 [DOI] [PubMed] [Google Scholar]
- 51.Fianchi L, Criscuolo M, Breccia M, Maurillo L, Salvi F, Musto P, et al. High rate of remissions in chronic myelomonocytic leukemia treated with 5-azacytidine: results of an Italian retrospective study. Leuk Lymphoma. 2013;54(3):658–61 [DOI] [PubMed] [Google Scholar]
- 52.Tsai HC, Li H, Van Neste L, Cai Y, Robert C, Rassool FV, et al. Transient low doses of DNA-demethylating agents exert durable antitumor effects on hematological and epithelial tumor cells. Cancer Cell. 2012;21 (3):430–46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Thorpe M, Montalvão A, Pierdomenico F, Moita F, Almeida A. Treatment of chronic myelomonocytic leukemia with 5-Azacitidine: A case series and literature review. Leuk Res. 2012;36 (8):1071–3 [DOI] [PubMed] [Google Scholar]
- 54.Aribi A, Borthakur G, Ravandi F, Shan J, Davisson J, Cortes J, et al. Activity of decitabine, a hypomethylating agent, in chronic myelomonocytic leukemia. Cancer. 2007;109(4):713–7 [DOI] [PubMed] [Google Scholar]
- 55.Wijermans PW, Rüter B, Baer MR, Slack JL, Saba HI, Lübbert M. Efficacy of decitabine in the treatment of patients with chronic myelomonocytic leukemia (CMML). Leuk Res. 2008;32(4):587–91 [DOI] [PubMed] [Google Scholar]
- 56.Beran M, Estey E, O’Brien S, Cortes J, Koller CA, Giles FJ, et al. Topotecan and cytarabine is an active combination regimen in myelodysplastic syndromes and chronic myelomonocytic leukemia. J Clin Oncol. 1999;17(9):2819–30 [DOI] [PubMed] [Google Scholar]
- 57.Beran M, Estey E, O’Brien SM, Giles FJ, Koller CA, Kornblau S, et al. Results of topotecan single-agent therapy in patients with myelodysplastic syndromes and chronic myelomonocytic leukemia. Leuk Lymphoma. 1998;31(5–6):521–31 [DOI] [PubMed] [Google Scholar]
- 58.Grinblatt DL, Yu D, Hars V, Vardiman JW, Powell BL, Nattam S, et al. Treatment of myelodysplastic syndrome with 2 schedules and doses of oral topotecan: a randomized phase 2 trial by the Cancer and Leukemia Group B (CALGB 19803). Cancer. 2009;115(1):84–93 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Fenaux P, Raza A, Mufti GJ, Aul C, Germing U, Kantarjian H, et al. A multi-center phase 2 study of the farnesyltransferase inhibitor tipifarnib in intermediate-to high-risk myelodysplastic syndrome. Blood. 2007;109(10):4158–63 [DOI] [PubMed] [Google Scholar]
- 60.Feldman EJ, Cortes J, DeAngelo DJ, Holyoake T, Simonsson B, O’Brien SG, et al. On the use of lonafarnib in myelodysplastic syndrome and chronic myelomonocytic leukemia. Leukemia. 2008;22(9): 1707–11 [DOI] [PubMed] [Google Scholar]
- 61.Strupp C, Knipp S, Hartmann J, Gattermann N, Haas R, Germing U. A pilot study of bendamustine in elderly patients with high-risk MDS and AML. Leuk Lymphoma. 2007;48(6):1161–6 [DOI] [PubMed] [Google Scholar]
- 62.Cheng H, Kirtani VG, Gergis U. Current status of allogeneic HST for chronic myelomonocytic leukemia. Bone Marrow Transplant. 2012;47(4):535–41 [DOI] [PubMed] [Google Scholar]
- 63.Elliott MA, Tefferi A, Hogan WJ, Letendre L, Gastineau DA, Ansell SM, et al. Allogeneic stem cell transplantation and donor lymphocyte infusions for chronic myelomonocytic leukemia. Bone Marrow Transplant. 2006;37(11):1003–8 [DOI] [PubMed] [Google Scholar]
- 64.Kerbauy DM, Chyou F, Gooley T, Sorror ML, Scott B, Pagel JM, et al. Allogeneic hematopoietic cell transplantation for chronic myelomonocytic leukemia. Biol Blood Marrow Transplant. 2005;11(9):713–20 [DOI] [PubMed] [Google Scholar]
- 65.Krishnamurthy P, Lim ZY, Nagi W, Kenyon M, Mijovic A, Ireland R, et al. Allogeneic haematopoietic SCT for chronic myelomonocytic leukaemia: a single-centre experience. Bone Marrow Transplant. 2010;45(10):1502–7 [DOI] [PubMed] [Google Scholar]
- 66.Kroger N, Zabelina T, Guardiola P, Runde V, Sierra J, Van Biezen A, et al. Allogeneic stem cell transplantation of adult chronic myelomonocytic leukaemia. A report on behalf of the Chronic Leukaemia Working Party of the European Group for Blood and Marrow Transplantation (EBMT). Br J Haematol. 2002;118(1):67–73 [DOI] [PubMed] [Google Scholar]
- 67.Laport GG, Sandmaier BM, Storer BE, Scott BL, Stuart MJ, Lange T, et al. Reduced-intensity conditioning followed by allogeneic hematopoietic cell transplantation for adult patients with myelodysplastic syndrome and myeloproliferative disorders. Biol Blood Marrow Transplant. 2008;14(2):246–55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Mittal P, Saliba RM, Giralt SA, Shahjahan M, Cohen AI, Karandish S, et al. Allogeneic transplantation: a therapeutic option for myelofibrosis, chronic myelomonocytic leukemia and Philadelphia-negative/BCR-ABL-negative chronic myelogenous leukemia. Bone Marrow Transplant. 2004; 33(10):1005–9 [DOI] [PubMed] [Google Scholar]
- 69.Ocheni S, Kroger N, Zabelina T, Zander AR, Bacher U. Outcome of allo-SCT for chronic myelomonocytic leukemia. Bone Marrow Transplant. 2009;43(8):659–61 [DOI] [PubMed] [Google Scholar]
- 70.Eissa H, Gooley TA, Sorror ML, Nguyen F, Scott BL, Doney K, et al. Allogeneic hematopoietic cell transplantation for chronic myelomonocytic leukemia: relapse-free survival is determined by karyotype and comorbidities. Biol Blood Marrow Transplant. 2010;17(6):908–15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Such E, Germing U, Malcovati L, Cervera J, Kuendgen A, Della Porta MG, et al. Development and validation of a prognostic scoring system for patients with chronic myelomonocytic leukemia. Blood. 2013; 121(15):3005–15 [DOI] [PubMed] [Google Scholar]