

Abstract
Background
Metabolic functions typically increase with human activity, but optimal methods to characterize activity levels for real-time predictions of ventilation volume (l/min) during exposure assessments have not been available. Could tiny, triaxial accelerometers be incorporated into personal level monitors to define periods of acceptable wearing compliance, and allow the exposures (μg/m3) to be extended to potential doses in μg/min/kg of body weight?
Objectives
In a pilot effort, we tested: 1) whether appropriately-processed accelerometer data could be utilized to predict compliance and in linear regressions to predict ventilation volumes in real time as an on-board component of personal level exposure sensor systems, and 2) whether locating the exposure monitors on the chest in the breathing zone, provided comparable accelerometric data to other locations more typically utilized (waist, thigh, wrist, etc.).
Methods
Prototype exposure monitors from RTI International and Columbia University were worn on the chest by a pilot cohort of adults while conducting an array of scripted activities (all <10 METS), spanning common recumbent, sedentary, and ambulatory activity categories. Referee Wocket accelerometers that were placed at various body locations allowed comparison with the chest-located exposure sensor accelerometers. An Oxycon Mobile mask was used to measure oral-nasal ventilation volumes in-situ. For the subset of participants with complete data (n= 22), linear regressions were constructed (processed accelerometric variable versus ventilation rate) for each participant and exposure monitor type, and Pearson correlations computed to compare across scenarios.
Results
Triaxial accelerometer data were demonstrated to be adequately sensitive indicators for predicting exposure monitor wearing compliance. Strong linear correlations (R values from 0.77 to 0.99) were observed for all participants for both exposure sensor accelerometer variables against ventilation volume for recumbent, sedentary, and ambulatory activities with MET values ~<6. The RTI monitors mean R value of 0.91 was slightly higher than the Columbia monitors mean of 0.86 due to utilizing a 20 Hz data rate instead of a slower 1 Hz rate. A nominal mean regression slope was computed for the RTI system across participants and showed a modest RSD of +/−36.6%. Comparison of the correlation values of the exposure monitors with the Wocket accelerometers at various body locations showed statistically identical regressions for all sensors at alternate hip, ankle, upper arm, thigh, and pocket locations, but not for the Wocket accelerometer located at the dominant-side wrist location (R=0.57; p=0.016).
Conclusions
Even with a modest number of adult volunteers, the consistency and linearity of regression slopes for all subjects were very good with excellent within-person Pearson correlations for the accelerometer versus ventilation volume data. Computing accelerometric standard deviations allowed good sensitivity for compliance assessments even for sedentary activities. These pilot findings supported the hypothesis that a common linear regression is likely to be usable for a wider range of adults to predict ventilation volumes from accelerometry data over a range of low to moderate energy level activities. The predicted volumes would then allow real-time estimates of potential dose, enabling more robust panel studies. The poorer correlation in predicting ventilation rate for an accelerometer located on the wrist suggested that this location should not be considered for predictions of ventilation volume.
Keywords: Ventilation volume, personal exposure, potential dose, triaxial accelerometry, adults, wearing compliance
1. BACKGROUND
The National Research Council (NRC, 2004) noted that reducing the uncertainties associated with characterizing individual and population exposures to particulate matter (PM) was a critically-important area of research needed to improve the establishment of linkages between exposures to sized particles and adverse health effects. A meta-analysis by Avery et al. (2010) reviewed 567 epidemiologic and toxicology studies during the prior decade and concluded that substantial progress has been made in understanding exposure biases such as misclassification error research progress is still needed to strengthen analyses attempting to utilize ambient air toxics concentration data as a surrogate for true personal exposures. Brook et al. (2010) noted that the strongest associations between vascular diseases and fine particles resulted from the use of personal level exposure assessments that applied approaches to identify measurement confounders such as second hand smoke and poor sensor wearing compliance and adjust accordingly. Fajardo and Rojas (2012) reported that utilizing individual exposure characterizations of bicycling near roadways that did not account for breathing rates, could significantly underestimate health risk levels. Especially in cases where spatial and temporal PM gradients are produced by strong sources such as roadways, linking localized exposure levels with respiratory effects would provide the most robust associations (McCreanor et al., 2007). Historically, the methodologies to characterize exposure levels for sized particles at the personal level have been cumbersome (Rodes and Thornburg, 2005), but technological advances are allowing smaller and lighter exposure monitors. If a comparably-low-burden approach were utilized to simultaneously monitor exposure study participant breathing rates with personal level PM concentrations, estimates of personal dose would be possible in real-time. Associating potential doses with potential sources and adverse outcomes, rather than more simplistic concentration data, should strengthen observed associative levels, thereby minimizing misclassification error. If such strengthening could be achieved, it would ultimately enhance the exposure/dose metric, thereby potentially reducing the sizes of cohorts and/or the numbers of participant-days needed to achieve acceptable statistical significance levels in epidemiologic analyses.
Vries et al. (2006) had investigated in a clinimetric review the validity, reliability and reproducibility of various accelerometer-based activity sensors in children. They concluded that the inherent and acceptable levels of (accelerometric) reproducibility, validity, and application feasibility strongly merited further study. Similarly, Pober et al. (2006) described the utility of triaxial accelerometers to define activity levels and potentially identify activities by some level of pattern recognition. They also concluded the accelerometers were indeed promising for activity studies focusing on energy expenditure and provided several recommendations for future work, including collecting better participant descriptive variables during baseline enrollments to better examine factors such as age, fitness level, and handedness. Initial testing at RTI with accelerometric data produced from components embedded within the main circuit board of the MicroPEM™ personal level exposure monitor worn in the breathing zone provided comparable and encouraging results to that of Pober et al. (2006). These tests bolstered the case that properly collected and processed accelerometric data (designated ACCEL here) had the potential to correlate strongly with estimations of pulmonary ventilation while monitoring PM exposure levels. Successful predictions of ventilation (breathing) volume in liters/minute, designated here as V, would enable concentration data to be transposed in either real-time or post-processing into potential inhalation-based dose. While ventilation volumes could be determined by wearing a mask during exposure assessments (Panis et al., 2010), masks can hinder breathing patterns and are too cumbersome for large cohort applications. Additionally, they could alter the rates particles enter the respiratory system.
Prior accelerometers have been modestly-robust single axis sensors, typically placed at convenient body locations to provide specific information about activity levels and estimated activity energy expenditure (Trost, 2001; Puyau et al., 2002; Mathie et al., 2002; Welk et al., 2006). The potential of using 3-axis accelerometry to predict selected metabolic functions and provide metrics inherently having more information content was suggested as early as 1997 by Bouten et al. (1997) and Mathie et al. (2002). New systems, such as the Wockets used by Albinali et al., (2010) permit comfortable, long-term wearability to support human activity studies for a range of health-based applications. The most common body location for measuring physical activity has been the hip. The preferred location for monitoring sleeping has been the wrist. As noted by Liu et al. (2010), defining bodily movement produced by skeletal muscles provides valuable insights into behavior patterns and the associated energy expenditures. Vries et al. (2006) surveyed childrens’ accelerometric activity research and characterized the quality of the data for clinimetric applications. The relationships between activity level and the physiological responses that alter metabolic rates and impact obesity levels are summarized by Bouchard et al. (2007). Bates et al. (2010) and Albinali et al. (2010) describe some benefits for activity type and energy expenditure detection of using 3 spatial axes and high-sampling rate data with pattern recognition algorithms. They also noted that the current tiny device packages offered by MEMS manufacturers should broaden the potential applications and enhance the potential for estimating ventilation and a range of metabolic rates in transparent manners from relatively simplistic motion sensing. As mentioned by Albinali et al., (2010) and Liu et al. (2009; 2010), locating wearable accelerometric sensors on the body and wearing them for extended periods can be significantly less obtrusive compared with piezoelectric chest straps that must necessarily be worn invasively adjacent to the skin and under the clothing.
Although ventilation volume data have been linked to exposures (Beals et al., 1996), data were not available to suggest: 1) whether simple to apply on-board predictive linear regression forms were applicable, nor how broadly the regression data for a single participant was likely to be applicable to broader cohorts - representing both adult men and women, over a reasonable age range, and 2) whether the wearing location of the accelerometer on the body might affect the strengths of the developed regressions. While personal level exposure monitors are preferentially worn in the breathing zone, accelerometer data have been historically collected at hip or wrist locations. For a range of scripted mild to moderate activities, we tested the accelerometer-enabled prototype personal exposure sensors of RTI and Columbia worn in participant breathing zones with accelerometer data collected at several other locations on the body simultaneously with sensors specifically designed for monitoring physiologic metrics (including ventilation rate and volume, heart rate, skin temperature, etc.).
Robust estimates of potential dose rather than more simplistic personal level exposure characterizations more accurately reflect true body burden and hence should provide stronger association with adverse biological and health outcomes. Importantly, if reasonably-robust predictive regressions are possible, could a single regression then be used for all adults over a reasonable range of activity levels, body types and fitness levels? Data from Bennett and Zeman (2004) had already shown that BMI was moderately correlated (R=0.46) with ventilation rate in children measured on a per minute basis. If such strengthening could be achieved, it would ultimately enhance the exposure/dose metric, thereby potentially reducing the sizes of cohorts and the numbers of participant-days needed to achieve acceptable statistical significance levels in epidemiologic analyses. The primary goal of this paper was to explore the applicability of the ventilation rate estimation process using accelerometry for application to exposure panel studies attempting to characterize general population adult cohorts.
2. OBJECTIVES
Determine whether linear regression fits between ACCEL and V have reasonable predictive power for adult cohorts over a range of scripted activities, thereby reducing the complexity of applying the predictions in near-real-time, i.e. V = m x ACCEL + b where m=slope and b= intercept ]
Determine whether accelerometric measurements (ACCEL) made by an exposure sensor system worn on the chest or other locations near the breathing zone could be used to develop regressions to predict ventilation rates (V’s) for each participant over a representative array of scripted activity tests representing typical daily, low-energy activities.
3. MATERIALS AND METHODS
The participants were recruited, representative activities selected, followed by participants outfitted with a range of accelerometers, exposure sensors, and metabolic function monitors, (see below), and asked to perform a range of scripted activities according to a standardized protocol. Normalized comparisons across body locations were facilitated by collocations of small wireless 3-axis accelerometers (Wockets) developed at MIT1. These sensors can be used with pattern recognition algorithms to detect activity type and intensity, with one recent paper showing improvement in activity energy estimation during a variety of activities by incorporating activity type detection (Albinali et al., 2010). The pilot cohort size of recruited and successfully tested adults that underwent the preset list of scripted activities was n = 22.
3.1 Personal Exposure Sensors/Samplers
Two prototype personal exposure sensor platforms developed by RTI International and Columbia University containing embedded 3-axis accelerometer devices were used in this research. Due to the timing of the experiments, both the systems used were early prototype versions of what each group was ultimately aiming to produce (i.e. with limited sensor functionality) but the tri-axial accelerometer chip used by each group has not changed as their platform has evolved. The prototype RTI MicroPEM™ system used here weighs under 300g, has a volume of 510 cm3 and fits into a shirt pocket (see photos in Figure 1). Key capabilities of the system include: a) providing both integrated PM samples on a 25 mm OD Teflon filter, and real-time PM data by nephelometry at 780 nm for periods as short as 1s, b) collecting QC data such as flowrate, filter pressure drop, battery voltage, temperature, relative humidity, and wearing compliance level on-board to subsequently validate the PM data, and c) allowing fully programmable operational control and timing that permits a one-button starting procedure by the participant. The on-board 3-axis accelerometer device is an Okidata 8953 component with a +/−3g range, whose size (25 mm2) and weight (<1g) are typical of triaxial accelerometers (see Section 1.1 of Supplemental Material). The on-board software was set to sample the accelerometer’s x, y, and z output data at 20 Hz, with the resultant data integrated over 1s intervals (see Section 3.9) for comparison with all other accelerometers. The nominal resolution provided by the manufacturers for each accelerometric axis (RTI or Columbia) is 0.02 gravity units.
Figure 1.
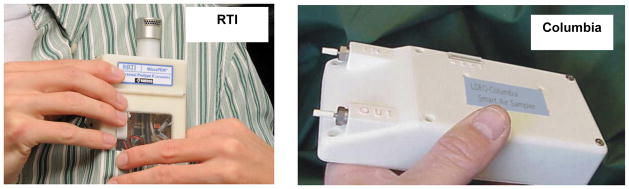
Prototype RTI MicroPEM™ (v2.7) and Columbia Black Carbon monitors worn in shirt pocket locations
The early Columbia prototype system tested here was an integrated sampler collecting filters for laboratory analysis only while logging location and compliance information, though the current model also provides real-time optical measurements for particulate matter components such as black carbon. The system weighed just over 300g and had a volume of ca. 310 cm3 allowing it to be worn in a vest pocket. At the time of the experiments, the accelerometer was limited by the software to collect data at a slower 1 Hz rate for the tests reported here.
3.2 Accelerometry for Wearing Compliance and Activity Level Prediction
Accelerometers can be used to characterize both wearing compliance (Rodes et al., 2010) for exposure monitors and to characterize human activity levels and patterns. Quantifying wearing compliance is extremely important in minimizing exposure misclassification, and refinements to the approach reported by Rodes et al. (2010) were developed as part of the present research. Additional background information on why protocol compliance is important is provided in Section 1 of the Supplemental material.
The ability to distinguish periods when the exposure systems are unworn requires that adequate accelerometric sensitivity is available to effectively set a threshold that can identify significant differences in the signal between when the system is unworn compared with worn during very low energy activities, such as working at a computer. Since it is nearly impossible for a participant to remain as motionless as an unworn system, a representative variability level was determined from an unworn unit and used to set a threshold compliance level. The composite arithmetic standard deviation of the AUC variable across all three axes, x, y, and z, (Sx,y,z) was determined for the RTI system for an unworn (stationary) RTI MicroPEM™ (Okidata 8953 accelerometer) unit and found to be 0.0078 G (gravity units). Table 1S in the supplementary material provides additional Sx,y,z values determined by activity type for participant #30. This threshold value was then compared across activities for all worn activities having a higher composite standard deviation by at least a factor of two. From these data, a modestly-conservative 20% higher threshold activity level variability of Sx,y,z = 0.0100 G was selected to account for likely between-accelerometer differences, above which the unit was presumed to be worn. The level of resolution was readily facilitated by the excellent sensitivity of current-technology triaxial devices combined with the digital sampling resolutions designed into the data capture electronics (typical analog-to-digital resolution 4,096 steps; see also Liu et al., 2010). The lowest standard deviation for all tested low energy activities while awake with the unit worn was Sitting at a Computer with a composite Sx,y,z of 0.0129 G, which was 65% greater than the threshold level. Since exposure monitoring protocols do not typically require them to be worn while sleeping, this mode was not evaluated.
3.3 Wocket Activity Monitor System
The Wocket system uses common mobile phones and multiple miniature sensors that transmit motion data to the phones using the Bluetooth wireless protocol. Each sensor, called a Wocket, has a 3-axis, Freescale Semiconductor model MMA7331LT-ND −4 to +4G accelerometer. The system is described in the web address given in Footnote 1. Each Wocket’s small (43mm × 30mm × 7mm with a small connector in a microSD form factor) to be placed comfortably and inconspicuously at various locations on the body in thin bands. The Wocket has limited on-board memory, but transmits collected data wirelessly to a nearby cellphone-based receiver unit. 3-axis accelerometer data can be saved to the phone for later processing or processed immediately given the phones microprocessor. In this paper we report data from Wockets worn at the wrist, ankle, chest, waist, pocket, and thigh.
3.4 Other Accelerometers
Comparison testing also included two additional commercially available 3-axis accelerometers These were the Actigraph model 7164 (Actigraph, Pensacola FL) and the accelerometer built into the Zephyr PSM Bioharness, (Zephyr Technology, Annapolis, MD, +/− 3G range) The Actigraph unit was worn at the waist attached to a belt (dominant hand side), while the Bioharness strap was worn under the clothing around the chest. The accelerometer on the Bioharness was located on the midline of the chest. Both the Actigraph and the Bioharness record and store data in on-board memory which then is downloaded to a computer following the test session.
3.6 Recruitment and Enrollment of Study Cohort
After development of a Consent Form and proposed test methodologies, the Institutional Review Boards at both Stanford University and RTI International provided reviews of the Consent Form and study design, with the Stanford IRB providing the primary approval. Recruitment for this pilot effort was conducted primarily from the campus community at Stanford University. Cohort data collection included age, sex, body weight and height, and self- reported habitual physical activity using the Stanford Brief Activity Survey, or SBAS (Taylor-Piliae, 2006). For this report data analyses were conducted on test data from 22 adult participants. The characteristics of this cohort are shown in Table 1. The cohort recruitment criteria considered only healthy, non-smoking adults who were sufficiently ambulatory to perform the range of selected activities, including bicycling. Since the recruitment was conducted on the Stanford campus, most participants were either students or university employees. Handedness was included in this table and exposure monitor placement in Table 4 for completeness as vigorous single hand activities such as painting are suspected to disproportionately shake a monitor worn on that side. However, no formal analysis to identify whether handedness was important are reported here.
Table 1.
Adult Participant Characteristics, indicating the number of scripted activities included for each participant.
| Participant # | Age | Sex | Weight, kg | Height, cm | BMI | SBAS Cat. | Dom. Hand | scripted activities n |
|---|---|---|---|---|---|---|---|---|
| 6 | 31 | F | 59.9 | 163 | 22.5 | 4 | R | 12 |
| 15 | 36 | F | 58.1 | 162.6 | 22.00 | 4 | R | 11 |
| 16 | 23 | M | 71.4 | 183.3 | 21.30 | 4 | R | 8 |
| 17 | 21 | M | 64.7 | 174.2 | 21.30 | 3 | R | 9 |
| 18 | 18 | F | 61.0 | 156.3 | 25.00 | 5 | R | 8 |
| 19 | 30 | M | 95.3 | 185.4 | 27.70 | 4 | L | 13 |
| 20 | 45 | F | 61.3 | 170.2 | 21.20 | 5 | R | 9 |
| 21 | 53 | F | 71.7 | 170.2 | 27.10 | 5 | R | 12 |
| 22 | 43 | F | 82.2 | 162.6 | 31.10 | 3 | R | 14 |
| 23 | 29 | F | 63.1 | 162.6 | 23.90 | 5 | R | 12 |
| 24 | 75 | M | 79.1 | 176.6 | 25.40 | 5 | R | 12 |
| 25 | 42 | F | 70.4 | 170.2 | 24.30 | 5 | R | 13 |
| 26 | 19 | M | 65.8 | 175.3 | 21.40 | 5 | R | 14 |
| 27 | 56 | M | 82.6 | 180.3 | 25.40 | 5 | R | 13 |
| 29 | 26 | F | 62.7 | 152.4 | 27.00 | 3 | R | 15 |
| 30 | 26 | M | 93.0 | 190.5 | 25.60 | 4 | R | 13 |
| 31 | 21 | M | 111.2 | 175.3 | 36.20 | 4 | R | 13 |
| 32 | 21 | F | 63.6 | 170.2 | 22.00 | 3 | R | 13 |
| 33 | 19 | M | 77.2 | 167.6 | 27.50 | 3 | L | 11 |
| 34 | 19 | F | 55.5 | 163.0 | 20.90 | 3 | R | 12 |
| 35 | 48 | F | 71.3 | 174.4 | 23.40 | 5 | R | 12 |
| 36 | 72 | M | 97.0 | 185.4 | 28.20 | 3 | L | 14 |
| n | 22 | |||||||
| SUMMARY: median | 29.0 | 71.3 | 170.2 | 25.0 | 4.0 | |||
| mean | 35.3 | 74.2 | 171.8 | 25.1 | 4.1 | |||
| std dev | 17.1 | 14.7 | 9.8 | 3.8 | 0.9 | |||
| min | 18 | 55.5 | 152.4 | 20.9 | 3 | |||
| max | 75 | 111.2 | 190.5 | 36.2 | 5 | |||
| MEN: n | 10 | 10 | 10 | 10 | 10 | |||
| median | 24.5 | 80.9 | 178.5 | 25.5 | 4.0 | |||
| average | 36.2 | 83.7 | 179.4 | 26.0 | 4.0 | |||
| WOMEN: n | 12 | 12 | 12 | 12 | 12 | |||
| median | 33.5 | 62.9 | 163.0 | 23.7 | 4.5 | |||
| average | 34.3 | 65.1 | 164.8 | 24.2 | 4.2 |
Table note: for SBAS categories, see Taylor-Piliae et al. (2006)
Table 4.
Linear Regression Statistics for RTI Exposure Monitor accelerometer variable against the Oxycon Ventilation volume for activities 1 through 16
| 95% Confidence Intervals | 95% Confidence Intervals | |||||||
|---|---|---|---|---|---|---|---|---|
| Part. # | exposure monitor side | activities n | Slope | Slope − | Slope + | Intercept | Intercept − | Intercept + |
| 6 | na | 12 | 1.19 | 0.77 | 1.62 | 6.91 | 4.74 | 9.08 |
| 15 | L | 11 | 1.76 | 1.11 | 2.42 | 10.70 | 5.87 | 15.50 |
| 16 | L | 8 | 1.27 | 0.66 | 1.87 | 7.74 | 3.00 | 12.50 |
| 17 | L | 9 | 1.24 | 0.84 | 1.64 | 5.83 | 3.28 | 8.40 |
| 18 | L | 8 | 1.24 | 1.10 | 1.38 | 9.64 | 8.48 | 10.80 |
| 19 | L | 13 | 1.75 | 1.13 | 2.38 | 10.70 | 5.18 | 16.20 |
| 20 | L | 9 | 1.41 | 0.99 | 1.84 | 11.30 | 8.42 | 14.10 |
| 21 | R | 12 | 1.25 | 0.93 | 1.57 | 8.86 | 6.70 | 11.00 |
| 22 | R | 14 | 1.94 | 1.63 | 2.24 | 10.71 | 8.43 | 12.98 |
| 23 | R | 12 | 1.18 | 0.74 | 1.62 | 11.30 | 8.50 | 14.10 |
| 24 | R | 12 | 1.84 | 1.64 | 2.05 | 12.17 | 10.66 | 13.69 |
| 25 | R | 13 | 1.27 | 0.79 | 1.27 | 7.48 | 4.36 | 10.60 |
| 26 | R | 14 | 1.11 | 0.92 | 1.31 | 12.19 | 10.37 | 14.01 |
| 27 | R | 13 | 1.80 | 1.61 | 1.98 | 9.09 | 7.99 | 10.20 |
| 29 | R | 15 | 1.20 | 1.03 | 1.38 | 10.90 | 9.10 | 12.80 |
| 30 | R | 13 | 1.53 | 1.30 | 1.75 | 9.32 | 7.82 | 10.83 |
| 31 | R | 13 | 2.36 | 2.11 | 2.60 | 9.94 | 8.20 | 11.67 |
| 32 | R | 13 | 1.43 | 1.16 | 1.71 | 11.93 | 10.08 | 13.79 |
| 33 | R | 11 | 1.51 | 1.25 | 1.76 | 12.32 | 10.46 | 14.17 |
| 34 | R | 12 | 1.06 | 0.78 | 1.34 | 8.78 | 6.82 | 10.73 |
| 35 | R | 12 | 1.66 | 1.50 | 1.82 | 8.71 | 7.57 | 9.85 |
| 36 | R | 14 | 3.75 | 2.58 | 4.93 | 15.00 | 8.83 | 21.20 |
| ALL DATA: | ||||||||
| n | 22 | 22 | 22 | 22 | 22 | 22 | 22 | |
| median | 12.0 | 1.43 | 1.11 | 1.76 | 10.70 | 8.20 | 12.80 | |
| average | 12.0 | 1.60 | 1.23 | 1.95 | 10.22 | 7.62 | 12.82 | |
| std dev | 0.58 | 0.48 | 0.77 | 2.11 | 2.26 | 2.83 | ||
| RSD % | 36.6 | 38.9 | 39.4 | 20.6 | 29.6 | 22.1 | ||
| min | 8 | 1.06 | 0.66 | 1.27 | 5.83 | 3.00 | 8.40 | |
| max | 15 | 3.75 | 2.58 | 4.93 | 15.00 | 10.66 | 21.20 | |
Note: F-tests showed a 99% confidence level for goodness of fit to a linear model for all tests, except Part. #16, which was significant at 95% level.
3.7 Scripted Activity Selection and Testing
A limited panel of physical activities was selected that could easily be conducted in a 2 hour session and which were not physically demanding for generally healthy adults 18 to 75 years with no medical or functional limitations. The activities, listed in Table 2 range up to 8 METS (8 times resting energy expenditure - for MET classifications see Ainsworth et al., (2011). The activities were performed for 2 to 3 min, or long enough for each activity so participants reached “steady state” for heart rate, pulmonary ventilation and oxygen uptake. Note that activities #14 and #15 typically were much shorter than 2 minutes, and were not included in the present analysis for consistency with the 2 to 3 min. criterion. To minimize the effects of fatigue, the panel was selected so that they all could be completed in less than 120 minutes of actual testing. Activity selection (range of types and intensities) was based in part on the recommendations from previous and on-going research (Lyden et al., 2011; Kozey-Keadle et al., 2011; Sasaki et al., 2011), an NIH-sponsored workshop on the Objective Measurement of Physical Activity (Freedson, 2009), and review of reports on how American adults spend their time (American Time Use Survey), and a report on those activities that contribute the most to the daily energy expenditure of American adults (Dong et al., 2004). Since resources were limited and this work considered a demonstration pilot, some compromises were made including not being able to include all of the most common activities, such as commuting. The latter was logistically complicated to include in a 2 hour suite of activities, and while important, had to be relegated to subsequent testing. Some activities such as stationary biking were selected because of strong staff familiarity with these activities in prior and on-going programs, simplifying the setup times. Some participant fatigue may have occurred toward the end of the 120 minute test period, but if so, those fatigued periods couldn’t be identified separately by our methodology. Future work on that aspect is warranted.
Table 2.
Adult Scripted Activities by Number. Recumbent, sedentary and low-energy activities 1 through 16 all had METS values <6.0. Cycling and single-arm dominant activities not used in linear regression modeling had METS values from 1.8 to 8.0. see also, Ainsworth et al. (2011).
| # | Description | METS Values, mean (std dev) |
|---|---|---|
| Recumbent, Sedentary, or Lower-Energy Ambulatory | ||
| 1 | lying on back | 1.1 (0.24) |
| 2 | sitting | 1.0 (na) |
| 3 | sitting, computer search | 1.3 (0.27) |
| 4 | sitting, writing | 1.1 (0.27) |
| 5 | sitting, sorting files | 1.2 (0.33) |
| 6 | sitting, reading | 1.2 (0.39) |
| 7 | indoor treadmill, 2 mph, 0% | 2.8 (0.57) |
| 8 | indoor treadmill, 4 mph, 0% | 5.0 (1.04) |
| 9 | indoor treadmill, 3 mph, 6% incline | 4.7 (1.04) |
| 10 | indoor treadmill, 3 mph, 9% incline | 5.6 (1.24) |
| 11 | walking outside naturally | 2.8 (0.83) |
| 12 | standing | 1.3 (na) |
| 13 | indoors, carrying load | 3.2 (0.74) |
| 14 | indoors, stairs, down | nd |
| 15 | indoors, stairs, up | nd |
| 16 | sweeping with broom | nd |
| Cycling or Single Arm Dominant | ||
| 17 | indoor painting, roller | 2.0 (0.41) |
| 18 | indoor painting, brush | 1.8 (0.36) |
| 19 | indoor, stationary bike | 4.0 (0.82) |
| 20 | outdoor, bicycling | 5.5 (0.95) |
| 21 | outdoor, bicycling, downhill | 4.1 (na) |
| 22 | outdoor, bicycling, uphill | 8.0 (na) |
na - not available; nd - not determined
The panel of activities included activities performed by many members of the target population such as different postures (lying, sitting, standing), ambulation at different speeds (on the level and up or down various gradients) and at least partially representative forms of occupational transportation and home care activities. While vehicle driving is likely a scenario with high particle exposures (Panis et al., 2010; Dons et al., 2011), we simply didn’t have the resources to include that activity in these pilot tests. The activities spanned the intensity range from sedentary activities to medium-vigorous intensity (≥ ~8.0 METS). Activities were included that require use of lower body, upper body, and upper plus lower body combined. Activities were also included where the increase in energy expenditure was due to an increase in speed or frequency of movement and where the increase in energy expenditure was due to an increase in resistance or weight. Weight bearing and non-weight bearing activities were also included. A photo of a simulated participant wearing the array of sensors is shown in Figure 2, while additional photos of testing indoor and outdoor cycling are shown in supplemental Figure 2S.
Figure 2.
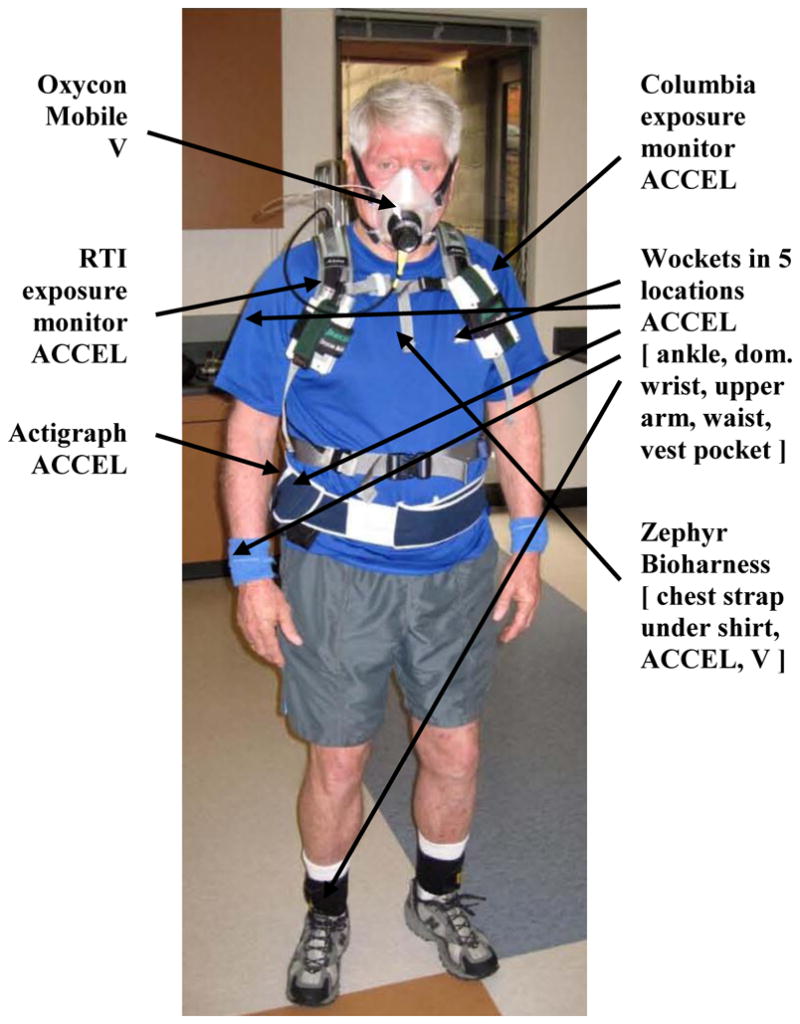
Placement of exposure and accelerometric sensors on an adult during scripted testing, with the Oxycon Mobile face mask for characterizing ventilation volume (V). Not shown is the backpack containing data logging modules.
3.8 Metabolic Data Collection
The pulmonary ventilation data collected for the present analyses were obtained using an Oxycon Mobile metabolic measurement system (Carefusion, Yorba Linda, CA). This is a lightweight (950 g.) portable unit that is worn by the subject and consists of a face mask that contains a flat fan for measuring pulmonary ventilation volume and an air sampling port that directs expired air through tubing to oxygen and carbon dioxide measurement devices. Data from expired air volume and the measures of oxygen and carbon dioxide concentrations are stored by unit and used to calculate a number of metabolic variables. After a testing session, the data on the memory card are downloaded to a computer for analysis using software provided by the company. The Oxycon Mobile1 and its supporting software have been shown to provide accurate ventilation and oxygen uptake data on subjects performing a wide variety of physical activities (Carter and Jeukendrup, 2002). For measurement of pulmonary ventilation, the reported range of the Oxycon unit is 0–300 l/min with an accuracy of ± 3%
3.9 Data Processing, Data Base Development and Validation
The ability to time synchronize data across sensors was important, and great care was taken to develop data collection procedures and software that would seamlessly allow temporal synchronization to nominally 1s across all accelerometric and metabolic sensors. A common laptop computer time was identified as the time-keeping referee against which all sensor clocks were synchronized prior to each participant test.
Data from 3-axis accelerometers were sampled at 40 Hz on the Wockets, 20 Hz for the RTI MicroPEM™ and 1 Hz for the Columbia sensor. To isolate the dynamic component of motion and get rid of the static component (due to gravity and changes in the orientation of the sensor), a moving average filter calculated over the previous 5s was applied to each raw acceleration stream (x, y and z) to remove high frequency components of the signal. The resulting smoothened signal was then integrated using the Trapezoidal Rule to compute the area under the curve (AUC) for each axis at 1s intervals. The integrated results from each axis were then summed into a single composite activity count that represents an orientation independent measure of movement intensity. Thus, for the RTI sensor, the AUC data were computed from the individual x, y, and z directions (Xauc, Yauc, and Zauc) and these three components totaled to provide a single XYZauc value for each second. A moving-time-base 5 second average of the prior 1s values was computed and subtracted from each 1s value in an effort to remove the impact of gravity on the individual readings for each accelerometer type. These 1s AUC difference values were also utilized for the ACCEL variable (see supplemental material) to establish threshold response levels above which indicated that the exposure monitors were actually being worn. A rapid scanning viewer procedure was developed to intercom pare the accelerometer data across all sensors for comparability as part of the review and validation process. An example output of this viewer is shown in supplemental Figure 2S.
On-board programming restrictions for the Columbia prototype necessarily limited its data collection to 1 Hz for these tests. The Wocket units served as the “referee” units against which the informational content losses of the slower RTI and Columbia sampling rates could be gauged. All Wocket, RTI, and Columbia accelerometry data were processed in the same manner, differing only by the hardware producing the signal, and the data sampling rates. Note that while slower data rates were thought to be usable for V rate prediction, data rates as high as 40 Hz are likely to be required only if categorical identifications by pattern recognition of activity type are considered, as was done in Albinali et al. (2010). This type of pattern recognition was not a goal of the current analyses but the developed data bases should allow these analyses in the future.
3.10 Data Treatments and Statistical Analyses
The total number of participants enrolled for testing was 36, but data from only 22 participants were deemed usable for this analysis, such that all participants could be compared across the same suite of tests with identical levels of data completeness for each participant by metric. The logistical complexity of the effort (since a longer suite of metabolic function data were also being collected, but are not reported here) resulted in identification of early stage testing functional and logistics problems. Only 7 of the first 20 participants enrolled provided complete data for the current analyses (<40% data capture) due primarily to early exposure sensor prototype system failures. This shortfall necessarily limited the number (n) of scripted low-energy (defined here as recumbent, sedentary, and ambulatory <4 mph) activities validated for these seven ranged from 8 to 13. For the last 16 participants tested, data from only 2 participants were lost, resulting in a much improved 88% data capture. The activity n-values for the last 15 participants ranged from 11 to 14. As noted previously, hardware and software glitches (e.g. intermittent failures of the Oxycon ventilation channel) with the exposure and metabolic function monitors proved to be the most troublesome and caused the greatest number of invalid participant days. The number of scripted activities investigated for each participant were not the same across participants. The number of higher-energy activities exhibiting valid data captures was also limited for the first 7 participants, with the number of activities ranging from 1 to 4 for this early group. The final 15 participants were more comprehensively tested, with the number of higher energy activities ranging from 4 to 5.
The statistical testing reported here consists of standard linear regression fit testing (Kleinbaum et al., 1988), with computations conducted primarily within Excel (v2003; Microsoft, Corp.). Goodness of fit (ACCEL versus V) to a linear model was characterized by the square of the Pearson correlation, with a two-way analysis of variance F test applied to test the degree of linearity of each regression for either the 95% or 99% confidence level. Comparability of Pearson correlation for a candidate accelerometer at a given body location against the data provide by a referee accelerometer located on the dominant side hip (Wocket 00; see location codes at the top of Table 3) was determined from associated Z and P-statistics for the 95% confidence level. Additionally, 95% confidence limits were computed for both the slope and intercept for each of the 22 participants to determine how appropriately a single median value could be applied (overlapping confidence limits) for the recruited cohort.
Table 3.
Pearson Coefficients of Determination (R2) for ACCEL vs V; activities 1 through 16 only
| Body location --> | Rt chest | Lf chest | hip | ankle | upper arm | wrist | thigh | chest | |
|---|---|---|---|---|---|---|---|---|---|
| Sensor type --> | RTI | Columbia | W00 | W01 | W02 | W03 | W04 | W05 | Zephyr |
| Participant # | R2 Oxycon | R2 Oxycon | R2 Oxycon | R2 Oxycon | R2 Oxycon | R2 Oxycon | R2 Oxycon | R2 Oxycon | R2 Oxycon |
| 6 | 0.80 | 0.79 | na | 0.77 | 0.77 | 0.77 | 0.41 | 0.76 | 0.80 |
| 15 | 0.80 | 0.58 | 0.78 | na | na | na | 0.72 | 0.84 | 0.83 |
| 16 | 0.81 | 0.89 | na | na | 0.86 | na | na | 0.87 | 0.82 |
| 17 | 0.85 | 0.40 | 0.94 | na | 0.76 | na | 0.96 | 0.95 | na |
| 18 | 0.99 | 0.96 | 0.98 | 0.94 | 0.96 | na | 0.95 | 0.97 | 0.99 |
| 19 | 0.78 | 0.72 | 0.74 | 0.74 | 0.74 | na | 0.69 | 0.71 | 0.81 |
| 20 | 0.90 | 0.94 | 0.90 | 0.94 | 0.96 | 0.86 | 0.92 | 0.86 | 0.92 |
| 21 | 0.88 | 0.87 | na | na | na | na | na | 0.85 | 0.87 |
| 22 | 0.94 | 0.89 | 0.93 | na | 0.91 | 0.20 | 0.91 | 0.91 | 0.97 |
| 23 | 0.80 | 0.62 | 0.80 | na | 0.81 | 0.44 | 0.81 | 0.84 | 0.80 |
| 24 | 0.98 | 0.83 | 0.98 | 0.97 | 0.94 | 0.56 | 0.97 | 0.97 | 0.98 |
| 25 | 0.77 | 0.86 | 0.87 | 0.88 | 0.78 | 0.27 | 0.88 | 0.86 | 0.84 |
| 26 | 0.93 | 0.92 | 0.93 | 0.93 | 0.89 | 0.77 | 0.95 | 0.94 | 0.94 |
| 27 | 0.98 | 0.94 | 0.97 | 0.95 | 0.91 | 0.51 | 0.95 | 0.95 | 0.97 |
| 29 | 0.94 | 0.49 | na | 0.91 | na | na | na | na | 0.93 |
| 30 | 0.95 | 0.89 | na | 0.92 | 0.90 | 0.64 | 0.91 | 0.90 | 0.94 |
| 31 | 0.98 | 0.86 | 0.95 | 0.93 | 0.97 | 0.67 | 0.94 | 0.93 | 0.98 |
| 32 | 0.92 | 0.90 | na | na | 0.87 | 0.58 | na | na | 0.90 |
| 33 | 0.95 | 0.84 | 0.91 | 0.89 | 0.90 | 0.44 | 0.90 | 0.88 | 0.93 |
| 34 | 0.88 | na | na | 0.86 | 0.83 | 0.34 | 0.87 | 0.85 | 0.87 |
| 35 | 0.98 | 0.92 | 0.97 | 0.97 | 0.96 | 0.75 | 0.96 | 0.96 | 0.97 |
| 36 | 0.80 | 0.79 | na | na | na | na | na | 0.87 | 0.80 |
| n | 22 | 21 | 14 | 14 | 18 | 14 | 17 | 20 | 21 |
| ALL DATA: median | 0.91 | 0.86 | 0.93 | 0.93 | 0.90 | 0.57 | 0.91 | 0.88 | 0.92 |
| average | 0.89 | 0.80 | 0.90 | 0.90 | 0.87 | 0.56 | 0.86 | 0.88 | 0.90 |
| std dev | 0.077 | 0.156 | 0.078 | 0.069 | 0.075 | 0.201 | 0.143 | 0.068 | 0.069 |
| min | 0.77 | 0.40 | 0.74 | 0.74 | 0.74 | 0.20 | 0.41 | 0.71 | 0.80 |
| max | 0.99 | 0.96 | 0.98 | 0.97 | 0.97 | 0.86 | 0.97 | 0.97 | 0.99 |
| R2 differ from hip 95% level? | NO | NO | na | NO | NO | YES | NO | NO | NO |
| p value: | NO | 0.342 | --- | 0.465 | 0.734 | 0.016 | 0.749 | 0.734 | 0.857 |
4. RESULTS
4.1 Recruited Adult Cohort Characteristics
Data from a final total of 22 adults were deemed to be acceptable for these analyses, having no missing data for each participant-day for the full suite of exposure monitors, referee Wockets, and metabolic sensors. The distribution of ages shown in Table 1 was no doubt impacted by the proximity of the Stanford university community for recruitment. The mean/median SBAS physical activity score was 4.2/4.5 indicating a generally physically active population. The sample was somewhat leaner than the general US adult population in which about two-thirds have a BMI above 25 compared to 45% in this sample.
4.2 Predictive Model Development
The mean, steady-state AUC data as the ACCEL dependent variable for all activities were initially regressed against the mean minute ventilation rate (V) data for all scripted activities to test the simple linear regression form V = m x ACCEL + b, where m = slope and b = intercept. Applying the linear model to data with METS levels less than or equal to that of walking on a level treadmill at 4 mph, resulted in the majority of coefficients of determination (R2) exceeding a nominal level of 0.85. These lower-energy activities correspond to the activities numbered 1 through 16 in Table 2. Including activities 17 through 22 in the regressions substantially reduced the observed correlation levels. This resulted from either higher METS level activities such as cycling, or single arm dominant activities such as brush painting which disproportionately jostled the chest accelerometers relative to the true METS levels. Since activities from 17 to 22 tended to produce significantly higher ventilations compared with simple linear predictions for the same accelerometer value, they were excluded from the linear modeling. It became clear that as the testing progressed that the higher energy activities, and especially cycling, merited a separate focus and warranted appending even high level activities such as jogging to better understand and define the breakpoint between linear and non-linear modeling. Figure 3s in the Supplemental material shows how including elevation in the treadmill to increase the METS level, began to shift these points from the linear model. Subsequently, the initially planned modeling was divided into low and higher energy activity levels, nominally at the 6 MET level. Thus, the subsequent ACCEL versus V regression analyses for the current analyses reported here cover only those lower-energy scripted activities with numbers from 1 thru 16. Higher METS modeling will be reported in a subsequent analysis.
4.3 V Measurements by Sensor Type
The assessment of V in l/min for each participant was made simultaneously by an Oxycon Mobile system using an adult ventilation face mask, and Zephyr Bioharness (the latter providing respiration rates in breaths/minute using a chest strap positioned sensor, but not true V). The ACCEL versus V regressions for the RTI system were constructed separately using ACCEL data from both types of monitors. Comparisons between the Pearson R2 coefficients of determination by V monitor type are presented in Table 3 across all participants for all ACCEL data for the two exposure monitors, all Wockets, the Zephyr Bioharness and the Actigraph accelerometers. The mean/median correlations developed by the RTI unit across all participants with the Oxycon Mobile were 0.89/0.92. The correlations of the MicroPEM™ (and other accelerometers) was substantially poorer as expected when the Zephyr breathing rate (min1) data were used as a marker variable for V (e.g. mean/media values of 0.65/0.70 for the MicroPEM™ for the same participants and activities), see data column 9 in Table 3.
In general the R2 data for all accelerometers at their tested locations were excellent, except for the Wocket data from the dominant side wrist location. This location gave consistently poorer correlations than any other location. Using the waist Wocket (00) as the “referee” location, correlations from all other sensors and locations were found to be statistically identical at the 95% CI, except for the dominant side wrist location (p=0.016). The latter mean/median R2 values were 0.56/0.57, respectively.
4.4 RTI and Columbia Regression Data, Chest Locations
The slopes and intercepts, and respective 95% confidence intervals for the linear regressions with the RTI and Columbia systems worn at chest locations (Rodes and Thornburg, 2005) were determined for activities 1 through 16. The RTI data regression summary by participant is provided in Table 4, while the comparable Columbia unit results are provided in Table 2S of the supplemental data. The numbers of scripted activities available for each regression gradually increased over the testing, reflecting improvements in the prototype exposure sensor hardware and software, as well as refinement of the complex matrix of scripted activity test procedures and metrics. The n for both exposure systems ranged from a low of 8 to a high of 15 (of 16 possible) activity types.
The slope and intercept data for the RTI and Columbia units cannot be directly compared due to the differences in internal scaling utilized by each approach in determining the ACCEL variable. However the composite relative standard deviations for the regression slopes and intercepts by unit types showed the RTI RSD’s to be 36.6% and 21.5% for the slope and intercept composites across all participants, while the comparable RSD’s for the Columbia unit were indistinguishable at 35.1% and 22.0% for the slopes and intercepts, respectively. The fractional magnitude of the mean 95% CI’s of the mean slope for the RTI units was 45%, while the same fractional CI for the Columbia mean slope was much larger at 66.0%. The fraction of the mean 95% CI for the RTI intercept was 50.9%, compared with 66.0% for the Columbia unit.
Graphical comparison across participants by Participant ID # for the slopes and their 95% CI’s for the RTI unit are shown in Figure 3. Comparable intercept data comparisons are shown in supplemental Figure S4. Also provided at the top of these graphs are the ages and BMI values for each participant. The mean slope value is indicated by the dashed line across all participants. Comparable slope and intercept data for the Columbia unit are provided in Table 2S of the supplemental material, and are very similar to the RTI, except exhibiting slightly lower Pearson correlations and larger confidence intervals for the slopes and intercept values. This performance deficit was attributed to the slower data collection rate for the Columbia prototype.
Figure 3.

RTI Composite Regression Slopes (ACCEL versus V by Oxycon); activities 1 through 16, showing the median value of 1.43. Highlighted age and BMI values reflect participants over 70 years of age, and outside a BMI range of 20 to 30, respectively.
4.5 ACCEL versus V for Cycling
Both indoor stationary cycling and outdoor bicycling provided linear regression relationships, but with slopes that are substantially different from the lower energy activities 1 through 16. The plot in Figure 4 compares the low energy regression for participant #30 with the linear regression for cycling activities. Note that both regressions had excellent R2 values exceeding 0.9, but had slopes differing by a factor of four. Including cycling and the higher energy activities (roller and brush painting) 17 and 18, resulted in substantial correlation weakening, with an all-activity R2 reduced to only 0.32.
Figure 4.

Example regression plots for Participant #30 comparing including only low-energy activities 1 to 16 (
 ), with cycling (
), with cycling (
 ) indoor (and outdoor) regressions to illustrate the dramatic slope change. R2 data are provided (but not plotted) for a regression merging low and high METS activities (1 to 22), showing the much poorer correlation, but similar slope.
) indoor (and outdoor) regressions to illustrate the dramatic slope change. R2 data are provided (but not plotted) for a regression merging low and high METS activities (1 to 22), showing the much poorer correlation, but similar slope.
Attempting to utilize the low-energy activity regression across all activities for this participant to predict a cycling event could lead to large biases. On the presumption that subsequent analyses of the higher data rate sampling will support at least categorical identification of higher energy activities such as cycling, an example prediction was undertaken for Participant 16 with and without the knowledge of a cycling component. Figure 5 plots both the ACCEL and V time series data across a suite of tested activities, highlighting the indoor (Activity 19) and outdoor (Activity 20) events. Utilizing the low energy regression across the cycling events (+ data), shows excellent tracking of the ventilation rate for all other activities, but is biased substantially low for cycling events by factors of 2 to 5. An a priori categorical identification of the cycling events (Δ) would have dramatically improved the predictive power for these events. Examples of some distinctive activity patterns at 20 Hz are shown in supplemental Figure 5S.
Figure 5.
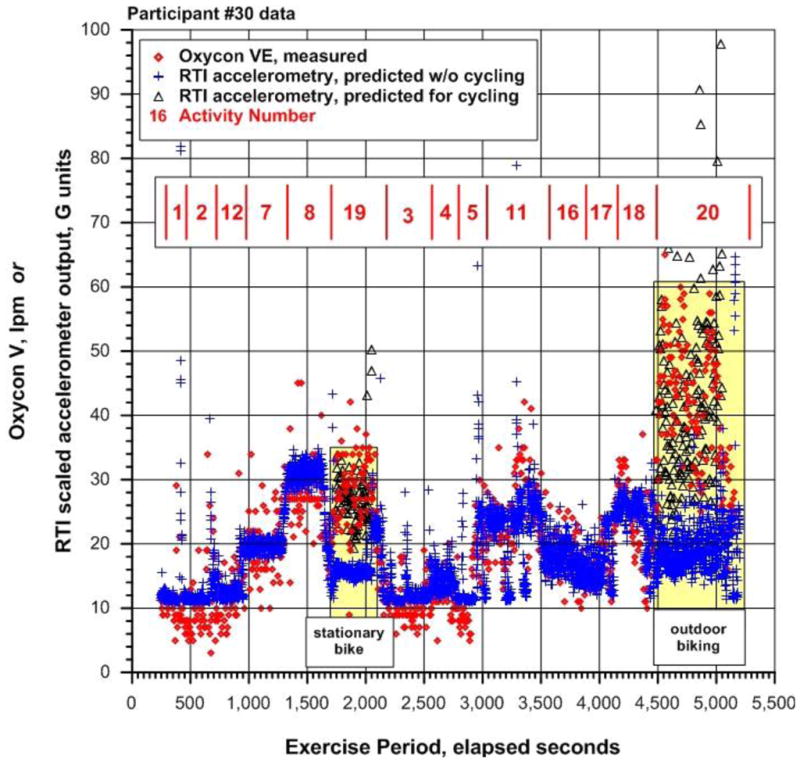
Example of Measured V for Participant #30 across selected scripted activities, illustrating the consistency of the ACCEL variable in predicting ventilation volume, and the potential biases if cycling was (black △) or was not (blue
 ; see color in online version only) identified a prior to define the appropriate regression to characterize the actual, measured V (
; see color in online version only) identified a prior to define the appropriate regression to characterize the actual, measured V (
 ).
).
5. DISCUSSION
Even as a pilot effort with a limited adult cohort size, the results presented here are encouraging. The data strongly support the application of utilizing on-board accelerometry in exposure sensors to predict ventilation rates for adults for a fairly wide range of typical adult daily activities. The strengths of the correlations across a wide array of triaxial accelerometer types and locations show that any of the tested triaxial devices and all but one body location (the wrist) would have provided equally robust data.
Note that the ACCEL metric utilized here was not the conventional vector composite of the x, y, and z components, but an area-under-the-curve (AUC) summation metric that was observed to be more reflective of subtle changes that might lead to increased energy expenditure and strong impacts on metabolic functioning. The AUC metric also proved more sensitive for identifying whether the exposure monitors were being worn across all tested activities. Also, it was clear that the importance of examining data for higher energy activities, as well as a small, parallel childrens’ cohort with child-appropriate activities evaluated will be extremely interesting (manuscripts in preparation).
5.1 Predictive Power Versus Data Collection Rate
The referee Wocket accelerometers sampled and recorded motion at a rate of 40 Hz, while the RTI accelerometer collected data at 20 Hz, and the Columbia accelerometer sampled at only 1 Hz. While it is likely true that predictions of activity type may indeed require data rates approaching 40 Hz, the strengths of prediction between the Wocket and RTI devices at the same chest location were indistinguishable when AUC 1s summary values are used. If activity predictions are not needed, the slower 1 Hz data rate would provide a 40× reduction in required on-board memory and substantially speed data downloading. The slower 1 Hz rate used by the Columbia system provided acceptably strong correlations, but exhibited much wider error bars around the regression slopes for nearly all participants tested. This strongly suggests that such a low data rate is unreasonably slow, and a rate approaching or equaling the 20 Hz rate is far more robust and accurate. Since the data can be processed and stored in 1 sec increments or longer- the 20 Hz rate does not take any additional memory or energy.
5.2 Wearing Tightness Importance
Attaching accelerometers (or exposure sensing systems) tightly to the body undoubtedly results in the recorded motion patterns most closely resembling the correct activity magnitudes and pattern across a study period. However, tightly worn sensors may be perceived as somewhat invasive and uncomfortable over time, and looser sensor attachments are preferred if they don’t degrade the predictive power. At least for low energy activities represented by Activities 1 through 16, wearing tightness appeared not to be a factor, but no systematic focus on evaluating the impact of wearing tightness was conducted. Wocket 05 was loosely contained in a chest shirt pocket and provided equally strong associations with V as tight ankle, thigh, hip, and upper arm locations. This ability to provide strong associations may change significantly with higher energy activities where a loosely attached sensor would begin to bounce from its own inertia. Further investigation of the impact of wearing tightness on ventilation rate prediction for these higher energy activities is warranted.
5.3 Expanding Real-Time Exposure Data to Predict Potential Dose
The ability to robustly predict V data in real-time opens the door to predicting potential dose levels (μg/min/kg) instead of the more commonly collected exposures (μg/m3). This could result in significant strengthening of associations between exposures to aerosol toxicants and adverse health effects in situations where the aerosol concentrations are elevated simultaneously with the ventilation volume. For example, walking events on residential carpeting can readily increase the vertical gradients within a room by factors of two to more between breathing zone levels and other room heights (Rosati et al., 2008). Re-suspended dusts in the breathing zone have been associated with increased exposures to endotoxin (Rabinovitch et al., 2005) during walking events. During these walking events, typical adult ventilation volumes increased from sedentary activities to walking at 4 mph (Activity 8 in Figure 4) by roughly a factor of three. Thus, modeling potential dose estimates with concentrations measured at a fixed location and using a constant ventilation rate rather than applying a measured and varying V, could mis-characterize the peak respiratory burdens by a factor of 6 or more for the most active participants. This important point is supported by the conclusions of Panis et al. (2010) who reported that concentrations unadjusted for ventilation volumes under-estimated respiratory burden by a factor of 4.3 for a bicyclist.
While the single activity impacts on dose can be substantial, they have to be placed in context with the amount of time each day that a participant actually is walking on an aerosol sink such as carpeting that would produce such extremes in peak concentrations and potential doses. The critical importance of time-activity patterns in elevating particle exposures is also highlighted by Dons et al. (2011). Additionally, while the correlation for the ACCEL versus V regression is strong for a given participant, attempting to utilize composite regression statistics to represent a larger cohort of adults (per Table 4) will overlay the additional uncertainties posed by the reported confidence limits for both the slope and intercept. The impacts of these empirical confidence limits on the overall uncertainties in potential dose prediction remain to be identified.
System modules to compute both real-time exposures and potential dose estimates simultaneously have now been appended to the RTI MicroPEM™ on-board system software. Examples of those exposure and potential dose graphical interfaces can be found in Figure 6S of the supplemental materials.
5.4 Role of Participant BMI and Age Characteristics
Review of the data presented here strongly suggests that extremes in BMI (e.g. those above 30) and age (those over age 70) may deviate significantly from an adult general population regression to predict V from ACCEL data. For example, BMI was moderately correlated with the slope of the regression between V and ACCEL, with coefficients of determination of 0.30, but increasing to 0.50 if one elderly outlier was removed. A cursory breakdown of the data here with only 10 men and 22 women suggests that sex is also an important factor. Further testing with larger cohorts would be needed to prove that these surmises are correct. However, it is also clear that at rest V data from each recruited participant could be collected with minimal difficulty during enrollment and Consent Form processing to improve the predictive power of the regression. The at-rest V would then become the intercept term for that participant in place of a general adult regression value. This approach also merits further testing to demonstrate whether this surmise is correct.
5.5 Pattern Recognition is Possible and Important
Even with no formal pattern recognition analyses, the data collected here tended to show dramatically different triaxial magnitudes and patterns for the AUC ACCEL data across activity types. Example patterns are provided in the Supplemental material in Figure 5S. Future analyses will determine whether such identification is possible for at least a limited suite of the most common adult activities. Not only would this greatly strengthen the predictive accuracy, but peak values in the real-time exposure data would be simpler to interpret if categorical activity types could be identified transparently to the participant (no time-activity logging required).
6. FUTURE DIRECTIONS
Even as a modest effort with adults exhibiting a limited range of BMI’s, the results presented here are very encouraging, and strongly suggest that including small-footprint, low power triaxial accelerometers within personal exposure systems supporting health studies is very advantageous from perspectives of both wearing compliance determination and predicting potential doses. The surprisingly linear and consistent ACCEL versus V relationships for the limited range of adults tested, greatly simplifies the on-board data processing needed and encourages broader examinations as to how accelerometric data could enhance the robustness of panel study data. The significant slopes differences for the two oldest participants and the two with BMI’s greater than 30, clearly suggests that the limitations in the applicability of the approach need to be established from further testing. Until further analyses are undertaken, it is not clear whether the prediction of other metabolic variables such as pulse rate will show similar patterns.
A large experimental database still remains to be analyzed, including a limited cohort of 20 youth age 11–15 years who participated in scripted juvenile activity testing very similar to the adult testing reported here. Additional, data are still under review for higher intensity (e.g. jogging) adult scripted activities with METS >10 to more readily clarify when and how nonlinearities become apparent. A range of additional physiological data were collected simultaneously with the ventilation volume data, including pulse rate, skin temperature, and breath oxygen and have not yet been analyzed to determine whether the ACCEL variable would provide comparable predictive power.
Confirmatory data are needed across larger and more diverse cohorts, especially to examine distinctions between low and higher-energy activities, males and females, and to cover a wider range of participant BMI’s and ages. Additional analyses should also be considered as to whether other physical characteristics such as body height or weight (alone) might prove to be more robust predictors than BMI or age.
Supplementary Material
Acknowledgments
NIH GEI2 grant awards were made in 2007 to research groups at both RTI International (Engineering Technology Unit) and Columbia University (Lamont-Doherty Earth Observatory) to develop personal level PM exposure monitoring systems (Weis et al., 2005) that were robust but low burden. The RTI International NIEHS grant (U01ES016093) was entitled “Personal Aerosol Sensor Platform to Link Children’s Exposures to Asthma Severity,” to monitor sized (PM2.5 or PM10) particle mass in both integrated and real-time modes simultaneously. The Columbia University NIEHS grant (U01ES016110) entitled “Smart Miniaturized Personal Monitors for Black Carbon and Multiple Air Pollutants,” had the ultimate goal of making real-time measurements of black carbon and a tracer gas while collecting different filters for laboratory analysis for key locations (home vs away from home) and also logging location and compliance information. An NIEHS competitive supplemental Opportunity Fund grant award was also made to both RTI (Engineering Technology Unit) and Columbia (Lamont-Doherty Earth Observatory) allowing them to team with other GEI research groups, including Stanford University (Prevention Research Center) and MIT (House_n Research Group) to extend the utility and versatility of the accelerometric data (NIEHS grant U01HL091737). Additional support is acknowledged by Dr. Chillrud from NIEHS (ES009089). We are also grateful to Dr. David Balshaw and Dr. Daniel Schaughnessy NIH/NIEHS who provided guidance on technical integration and NIH Gene and Environment Initiative coordination.
ABBREVIATIONS
- ACCEL
designation for the composite variable computed from the triaxial accelerometer
- AUC
Area Under the Curve
- b
linear regression intercept
- BMI
Body Mass Index
- Hz
hertz
- m
linear regression slope
- MEMS
Micro-Electro-Mechanical Systems
- METS
Metabolic Equivalent TaskS
- PM
particulate matter
- QC
quality control
- R
Pearson correlation coefficient
- R2
coefficient of determination
- RSD
relative standard deviation
- RTI
Research Triangle Institute
- SBAS
Stanford Brief Activity Survey
- V
ventilation volume (lpm)
Footnotes
References
- Albinali F, Intille S, Haskell W, Rosenberger M. Using wearable activity type detection to improve physical activity energy expenditure estimation. Proceedings of the 12th International Conference on Ubiquitous Computing; New York: ACM Press; 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ainsworth B, Haskell W, Herrmann S, Meckes N, Bassett D, Jr, Tudor-Locke C, Greer J, Vezina J, Whitt-Glover M, Leon S. Compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exercise. 2011 May;2011 doi: 10.1249/MSS.0b013e31821ece12. in press. [DOI] [PubMed] [Google Scholar]
- Avery C, Mills K, Williams R, McGraw K, Poole C, Smith R, Whitsel E. Estimating Error in Using Residential Outdoor PM2.5 Concentrations as Proxies for Personal Exposures: a Meta-Analysis. EHP. 2010;118(5):673–678. doi: 10.1289/ehp.0901158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bates A, Ling M, Mann J, Arvina D. Respiratory rate and flow waveform estimation from tri-axial accelerometer data. proceedings 2010 International Conference on Body Sensor Networks; Singapore. 2010. pp. 144–150. [Google Scholar]
- Beals J, Funk L, Fountain R, Sedman R. Quantifying the distribution of inhalation exposure in human populations: Distribution of minute volumes in adults and children. EHP. 1996;104(9):104–109. doi: 10.1289/ehp.96104974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bennett W, Zeman K. Effect of body size on breathing pattern and fine-particle deposition in children. J Appl Physiol. 2004;97:821–826. doi: 10.1152/japplphysiol.01403.2003. [DOI] [PubMed] [Google Scholar]
- Bouchard C, Blair S, Haskell W. Physical Activity and Health. Human Kinetics; Champaign, IL 61825: 2007. [Google Scholar]
- Bouten C, Koekkoek K, Verduin M, Kodde R, Janssen J. A triaxial accelerometer and portable data processing unit for the assessment of daily physical activity. IEEE Transactions on Biomedical Engineering. 1997;44(3):136–147. doi: 10.1109/10.554760. [DOI] [PubMed] [Google Scholar]
- Brook R, Bard R, Burnett R, Shin H, Vette A, Croghan C, Phillips M, Rodes C, Thornburg J, Williams R. Differences in Blood Pressure and Vascular Responses Associated with Ambient Fine Particulate Matter Exposures Measured at the Personal Versus Community Level. Occ Env Med. 2010;68:224–230. doi: 10.1136/oem.2009.053991. [DOI] [PubMed] [Google Scholar]
- Carter J, Jeukendrup A. Validity and reliability of three commercially available breath-by-breath respiratory systems. Eur J Appl Physiol. 2002;86(5):435–441. doi: 10.1007/s00421-001-0572-2. [DOI] [PubMed] [Google Scholar]
- Dong L, Block G, Mandel S. Activities contributing to total energy expenditure in the United States: results from the NHAPS study. International J of Behavioral Nutrition and Physical Activity. 2004;1(4):1–11. doi: 10.1186/1479-5868-1-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dons E, Panis L, Poppel M, Theunis J, Willems H, torfs R, Wets G. Impact of Time-Activity Patterns on Personal Exposure to Black Carbon. Atmos Env. 2011;45:3594–3602. [Google Scholar]
- Fajardo O, Rojas N. Particulate Matter Exposures of Bicycle Path Users in a High-Altitude City. Atmos Env. 2012;46:675–679. [Google Scholar]
- Freedson P. Objective measurement of physical activity (presentation), NIH Conference: Best Practices and Future Directions; Bethesda, MD. July 20–21, 2009.2009. [Google Scholar]
- Kleinbaum D, Kupper L, Muller K. Applied regression Analysis and other multivariable methods. PWS-Kent Publishing; Boston, MA: 1988. [Google Scholar]
- Kozey-Keadle S, Libertine A, Lyden K, Staudenmayer J, Freedson P. Validation of wearable monitors for assessing sedentary behavior. Med Sci Sports Exerc. 2011 Jan 12;2011 doi: 10.1249/MSS.0b013e31820ce174. (ahead of print) [DOI] [PubMed] [Google Scholar]
- Liu S, Gao R, He Q, Staudenmayer J, Freedson P. Development of statistical regression models for ventilation estimation, proceedings, 31st Annual Int. Conf of the IEEE EMBS; Minneapolis, MN. 2009. [DOI] [PubMed] [Google Scholar]
- Liu S, Gao R, Freedson P. Design of a wearable multi-sensor system for physical activity assessment, proceedings, IEEE/ASME Int. Conf. on Advanced Intelligent Mecatronics; Montreal, Quebec. 2010. [Google Scholar]
- Lyden K, Kozey S, Staudenmeyer J, Freedson P. A comprehensive evaluation of commonly used accelerometer energy expenditure and MET predicton equations. Eur J Appl Physiol. 2011;111(2):187–201. doi: 10.1007/s00421-010-1639-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mathie M, Lovell N, Coster A, Celler B. Determining activity using a triaxial accelerometer, proceedings. Second Joint EMBS/BMES Conference; October 23; Houston, TX. 2002. [Google Scholar]
- McCreanor J, Cullinan P, Nieuwenhuijsen M, Steward-Evans J, Malliarou E, Jarup L, Harrington R, Svartengren M, Han I, Ohman-Strickland P, Chung K, Zhang J. Respiratory Effects of Exposure to Diesel Traffic in Persons with Asthma. New England J Med. 2007;357:2348–2358. doi: 10.1056/NEJMoa071535. [DOI] [PubMed] [Google Scholar]
- National Research Council (NRC) Research Priorities for Airborne Particulate Matter. National Academies Press; Washington, D. C: 2004. Research Topic 1: Outdoor Measures Versus Actual Human Exposures. [Google Scholar]
- Panis L, Geus B, Vandenbulcke G, Willems H, Degraeuwe B, Bleux N, Mishra V, Thomas I, Meeusen R. Exposure to Particulate Matter in Traffic: A Comparison of Cyclists and Car Passengers. Atmos Env. 2010;44:2263–2270. [Google Scholar]
- Pober D, Staudenmayer J, Raphael C, Freedson P. Development of novel techniques to classify physical activity model using accelerometers. Med and Sci in Sports and Exercise. 2006;38(9):1626–1634. doi: 10.1249/01.mss.0000227542.43669.45. [DOI] [PubMed] [Google Scholar]
- Puyau M, Adolph A, Vohra F, Butte N. Validation and calibration of physical activity monitors in children. Obesity Res. 2002;10(3):150–157. doi: 10.1038/oby.2002.24. [DOI] [PubMed] [Google Scholar]
- Rabinovitch N, Liu A, Zhang L, Rodes C, Foarde K, Dutton S, Murphy J, Gelfand E. Importance of the personal endotoxin cloud in school-age children with asthma. Journal of Allergy and Clinical Immunology. 2005;116:1053–1057. doi: 10.1016/j.jaci.2005.08.045. [DOI] [PubMed] [Google Scholar]
- Rodes C, Thornburg J. Breathing zone exposure assessment. In: Ruzer L, Harley N, editors. Chapter 5 in Aerosols handbook: Measurement, dosimetry, and health effects. CRC Press; New York, NY: 2005. [Google Scholar]
- Rodes C, Lawless PA, Thornburg JW, Williams RW, Croghan C. DEARS Particulate Matter Relationships for Personal, Indoor, Outdoor, and Central Site Settings for a General Population. Atmos Env. 2010;44(11):1386–1399. [Google Scholar]
- Rosati J, Thornburg J, Rodes C. Resuspension of Particulate Matter from Carpeting Due to Human Activities. Aerosol Sci Tech. 2008;42:472–482. [Google Scholar]
- Sasaki J, John D, Freedson P. Validation and comparison of ActiGraph activity monitors. J Sci Med Sport. 2011 May 24;2011 doi: 10.1016/j.jsams.2011.04.003. (ahead of print) [DOI] [PubMed] [Google Scholar]
- Taylor-Piliae R, Norton L, Haskell W, Mahbouda M, Fair J, Iribarren C, Hlatky M, Go A, Fortmann S. Validation of a New Brief Physical Activity Survey among Men and Women, Aged 60–69 Years. American Journal of Epidemiology. 2006;164(6):598–606. doi: 10.1093/aje/kwj248. [DOI] [PubMed] [Google Scholar]
- Trost S. Objective measurement of physical activity in youth: current issues, future directions. Exercise Sport Sci Rev. 2001;29(1):32–36. doi: 10.1097/00003677-200101000-00007. [DOI] [PubMed] [Google Scholar]
- Vries S, Bakker I, Hopman-Rock M, Hirasing R, Mechelen W. Clinimetric review of motion sensor in children and adolescents. J Clin Epi. 2006;59:670–680. doi: 10.1016/j.jclinepi.2005.11.020. [DOI] [PubMed] [Google Scholar]
- Weis B, Balshaw D, Barr J, Brown D, Ellisman M, Lioy P, Omenn G, Potter J, Smith M, Sohn L, Suk W, Sumner S, Swenberg J, Walt D, Watkins S, Thompson C, Wilson S. Personalized exposure assessment: promising approaches for human environmental health research. EHP. 2005;113(7):840–848. doi: 10.1289/ehp.7651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Welk G, Corbin C, Dale D. Measurement issues in the assessment of physical activity in children. Res Quart Exercise Sports. 2006;71(2):59–73. doi: 10.1080/02701367.2000.11082788. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.