

Abstract
OBJECTIVE
Associations between HbA1c and cardiovascular diseases (CVD) have been reported mainly in Western countries. It is not clear whether HbA1c measurements are useful for assessing CVD mortality risk in East Asian populations.
RESEARCH DESIGN AND METHODS
The risk for cardiovascular death was evaluated in a large cohort of participants selected randomly from the overall Japanese population. A total of 7,120 participants (2,962 men and 4,158 women; mean age 52.3 years) free of previous CVD were followed for 15 years. Adjusted hazard ratios (HRs) and 95% CIs among categories of HbA1c (<5.0%, 5.0–5.4%, 5.5–5.9%, 6.0–6.4%, and ≥6.5%) for participants without treatment for diabetes and HRs for participants with diabetes were calculated using a Cox proportional hazards model.
RESULTS
During the study, there were 1,104 deaths, including 304 from CVD, 61 from coronary heart disease, and 127 from stroke (78 from cerebral infarction, 25 from cerebral hemorrhage, and 24 from unclassified stroke). Relations to HbA1c with all-cause mortality and CVD death were graded and continuous, and multivariate-adjusted HRs for CVD death in participants with HbA1c 6.0–6.4% and ≥6.5% were 2.18 (95% CI 1.22–3.87) and 2.75 (1.43–5.28), respectively, compared with participants with HbA1c <5.0%. Similar associations were observed between HbA1c and death from coronary heart disease and death from cerebral infarction.
CONCLUSIONS
High HbA1c levels were associated with increased risk for all-cause mortality and death from CVD, coronary heart disease, and cerebral infarction in general East Asian populations, as in Western populations.
Since the association between HbA1c and microangiopathy was established in patients with diabetes, HbA1c has been used for not only the determination of glucose control among patients with diabetes but also the diagnosis of diabetes (1). Measurement of HbA1c is also recommended for cardiovascular risk assessment in asymptomatic adults without a diagnosis of diabetes (2) because the association between HbA1c and the risk for cardiovascular disease (CVD) in general populations has been reported, mainly from Western countries (3–10).
There have been only a few studies regarding the associations between HbA1c and CVD in Asian populations (11–13). Furthermore, these studies were from Japan, and HbA1c measurements were expressed mainly using Japan Diabetes Society (JDS) values rather than National Glycohemoglobin Standardization Program (NGSP) values; thus, we cannot compare these results with those from Western countries. Recently, the JDS provided an equation for the conversion from HbA1c (JDS) to HbA1c (NGSP) units (14), which allows a comparison of the results from Japanese studies and previous studies from Western countries.
CVD in East Asian people is characterized by a higher rate of stroke and lower rate of coronary heart disease compared with CVD in Western populations (15). In one previous study evaluating the association between HbA1c and incidence of stroke in Japan, ischemic stroke, but not hemorrhagic stroke, was associated with HbA1c in Asian populations (12). Other studies from Japan (11,13) showed a significant association between HbA1c and CVD; however, the number of participants and CVD events were too small to calculate the risk by subtype of CVD, such as coronary heart disease, stroke, cerebral infarction, and cerebral hemorrhage.
The current study was performed to examine the association between HbA1c using NGSP values and the risks for death from all causes and from CVD (coronary heart disease, cerebral infarction, and cerebral hemorrhage) in a 15-year cohort study of representative Japanese men and women randomly selected from the overall Japanese population.
RESEARCH DESIGN AND METHODS
NIPPON DATA (National Integrated Project for Prospective Observation of Noncommunicable Disease And its Trends in the Aged) is a cohort study of participants in the National Survey on Circulatory Disorders of Japan, which has been conducted by the Ministry of Health, Labor and Welfare of Japan. NIPPON DATA includes two cohort studies in which the baseline data were surveyed in 1980 (NIPPON DATA80) and in 1990 (NIPPON DATA90); the details of the studies have previously been described (16–21). Here, we investigated the data from NIPPON DATA90 because HbA1c was not measured in the NIPPON DATA80 baseline survey.
A total of 8,383 residents (3,503 men and 4,880 women, aged ≥30 years) from 300 randomly selected districts from all over Japan participated in the baseline survey and were followed until November 2005. The participation rate in this survey was 76.5%. Of the 8,383 participants, 1,263 were excluded because of a history of coronary heart disease or stroke (n = 358), missing information in the baseline survey (n = 649), or incomplete residential access information (n = 256). The remaining 7,120 participants (2,962 men and 4,158 women) were analyzed in the current study. The institutional review board of Shiga University of Medical Science (no. 12-18, 2000) approved this study.
Baseline examination
BMI was calculated as weight in kilograms divided by the square of height in meters. Trained observers measured baseline blood pressure using a standard mercury sphygmomanometer on the right arm of seated participants. Nonfasting blood samples were obtained at the baseline survey. Serum was separated by centrifugation soon after blood coagulation. Plasma samples were collected into siliconized tubes containing sodium fluoride and shipped to a central laboratory (SRL, Tokyo, Japan) for blood measurements. HbA1c was measured using the high-performance liquid chromatography method. The range of coefficient of variance of HbA1c measurement in this laboratory was 1.19–1.79% intra-assay and 0.24–0.45% interassay in the 1990s. HbA1c (JDS) values were converted to HbA1c (NGSP) values using the conversion formula provided by JDS: HbA1c NGSP value (%) = 1.02 × JDS value (%) + 0.25 (14). All present analyses adopted the HbA1c values of the NGSP method. Serum total cholesterol (milligrams per deciliter) was measured using an enzymatic method, and HDL cholesterol was measured after heparin-calcium precipitation (22). Public health nurses collected the information about smoking, alcohol consumption, habitual exercise, and medical history. Treatment for diabetes was self-reported, which included diet, exercise, and medication with regular visits to hospitals.
End points
We reported previously that participants who had died in each area were confirmed by computer matching with data from the National Vital Statistics database, using area, sex, date of birth, and death as key codes (16,23). The underlying causes of death in the National Vital Statistics were coded according to the ICD-9 until 1994 and according to the ICD-10 from 1995. Details of these classifications have previously been described (16,17,20,23). Deaths coded were defined as follows: CVD, from 393 to 459 (ICD-9) and from I00 to I99 (ICD-10); coronary heart disease, from 410 to 414 (ICD-9) and from I20 to I25 (ICD-10); stroke, from 430 to 438 (ICD-9) and from I60 to I69 (ICD-10); cerebral infarction, 433, 434, 437.8a, and 437.8b (ICD-9) and I63 and I69–3 (ICD-10); cerebral hemorrhage, from 431 to 432 (ICD-9) and I61 and I69.1 (ICD-10).
Statistical analysis
Participants were divided into six groups; five groups of participants without treatment for diabetes according to HbA1c level, <5.0% (31 mmol/mol), 5.0–5.4% (31–36 mmol/mol), 5.5–5.9% (37–41 mmol/mol), 6.0–6.4% (42–47 mmol/mol), and ≥6.5% (48 mmol/mol), and one group for participants with treatment for diabetes. One-way ANOVA or the χ2 test was used to compare characteristics of participants at baseline according to HbA1c categories. We calculated crude mortality and hazard ratios (HRs) for death due to all causes, CVD, coronary heart disease, stroke, cerebral infarction, and cerebral hemorrhage according to the six categories. The Cox proportional hazards model was used to calculate adjusted HRs. Adjustment for possible confounders was performed sequentially: for age and sex (age- and sex-adjusted model), then plus BMI, smoking habit (non-, ex-, or current smoker), drinking habit (non-, ex-, or daily drinker), habitual exercise (yes or no), systolic blood pressure, total cholesterol, HDL cholesterol, and medical treatment for hypertension and dyslipidemia (multivariate-adjusted model). HRs for death associated with a 1% increment in HbA1c were calculated for participants without treatment for diabetes. HRs were also calculated separately for each sex, and the interaction between sex and HbA1c on the mortality from each cause of death was calculated. As HbA1c was affected by anemia (24), we evaluated the HRs for participants without anemia (n = 5,978) for sensitivity analyses. Anemia was defined as hemoglobin concentration <13.5 g/dL for men and <12.0 g/dL for women. The statistical analysis package SPSS 17.0 for Windows (SPSS, Chicago, IL) was used for all statistical analyses. All probability values were two tailed, and the significance level was set at P < 0.05.
RESULTS
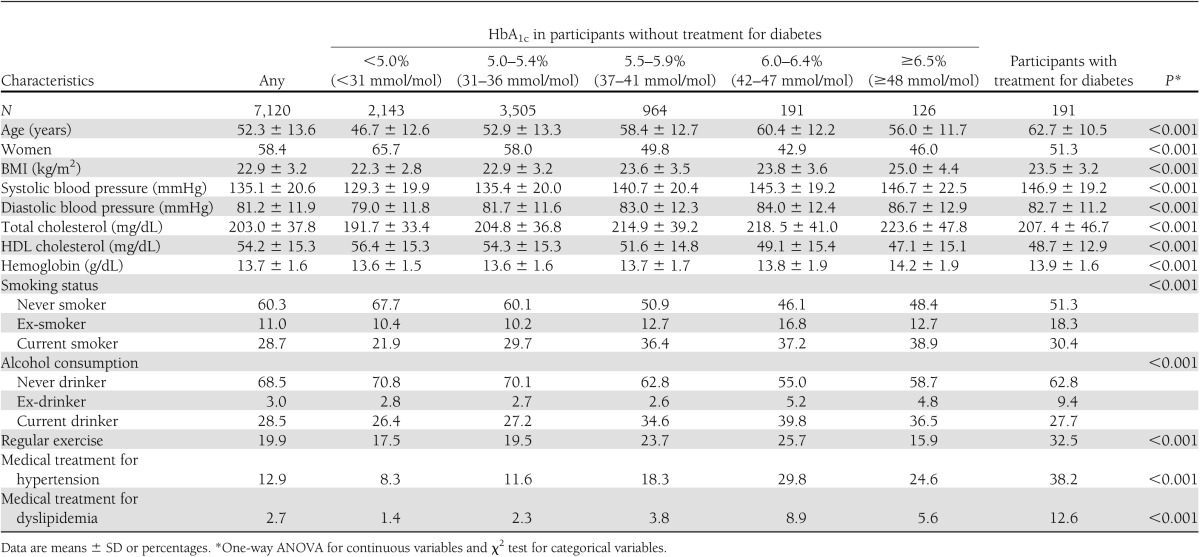
The baseline characteristics of study participants are shown in Table 1. The mean age at baseline was 52.3 years, and the mean BMI was 22.9 kg/m2. The mean HbA1c level was 5.3% (34 mmol/mol). Participants with higher HbA1c levels were older and had higher values for BMI, systolic and diastolic blood pressure, and serum total cholesterol; lower HDL cholesterol levels; and higher smoking rates.
Table 1.
Baseline characteristics of study participants according to HbA1c levels at baseline: NIPPON DATA90
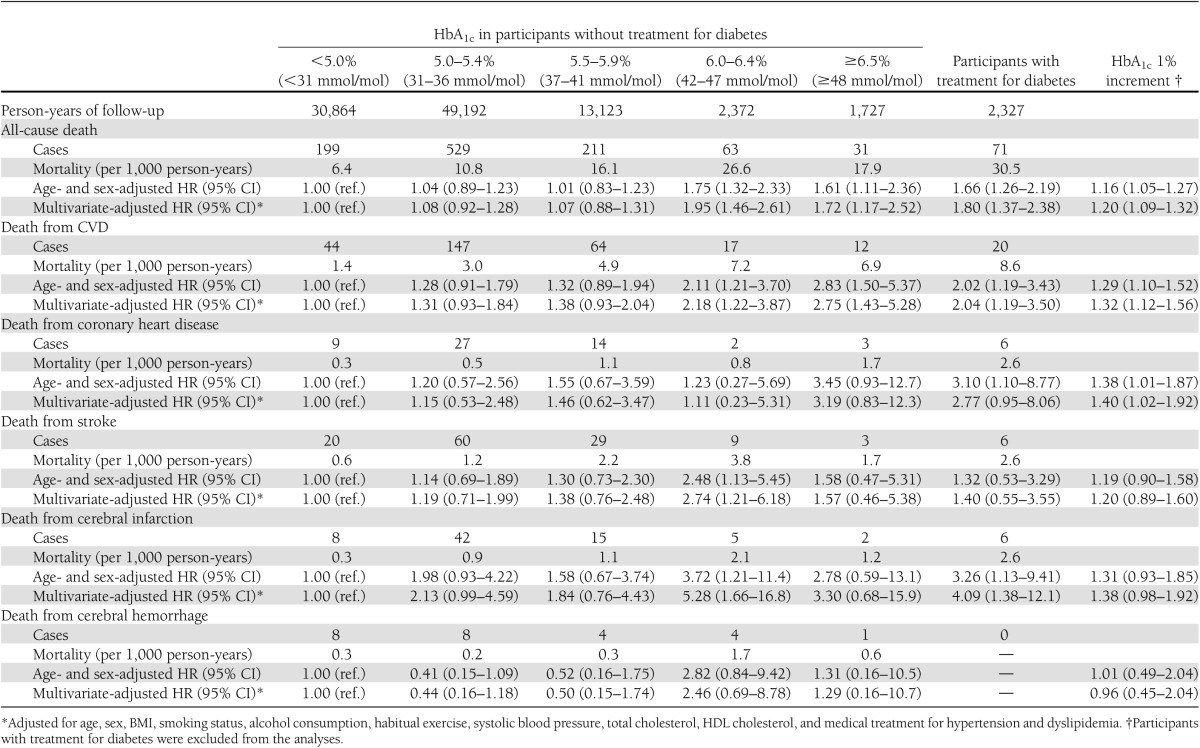
There were 99,605 person-years of follow-up for the 7,120 participants. Among all of the participants, there were 1,104 deaths, including 304 deaths from CVD, 61 from coronary heart disease, and 127 from stroke (78 from cerebral infarction, 25 from cerebral hemorrhage, and 24 from unclassified stroke).
Mortality and adjusted HRs according to HbA1c categories are shown in Table 2. The multivariate-adjusted HR for CVD death associated with a 1% increment in HbA1c was 1.32. Relations to HbA1c with CVD death were graded and continuous, and the multivariate-adjusted HR for CVD death in participants with HbA1c 6.0–6.4% (42–47 mmol/mol) was 2.18 (95% CI 1.22–3.87), and that in participants with HbA1c ≥6.5% (48 mmol/mol) was 2.75 (1.43–5.28); both HRs were significantly higher than that in participants with HbA1c <5.0% (31 mmol/mol). Similarly, HR for CVD death in participants with treatment for diabetes was 2.04 (1.19–3.50) and was significantly higher than that in participants with HbA1c <5.0% (31 mmol/mol). Similar associations were observed between HbA1c and death from coronary heart disease and death from cerebral infarction. On the other hand, cerebral hemorrhage was not significantly associated with HbA1c.
Table 2.
Risk of death according to the baseline HbA1c levels in 7,120 participants: NIPPON DATA90, 1990–2005
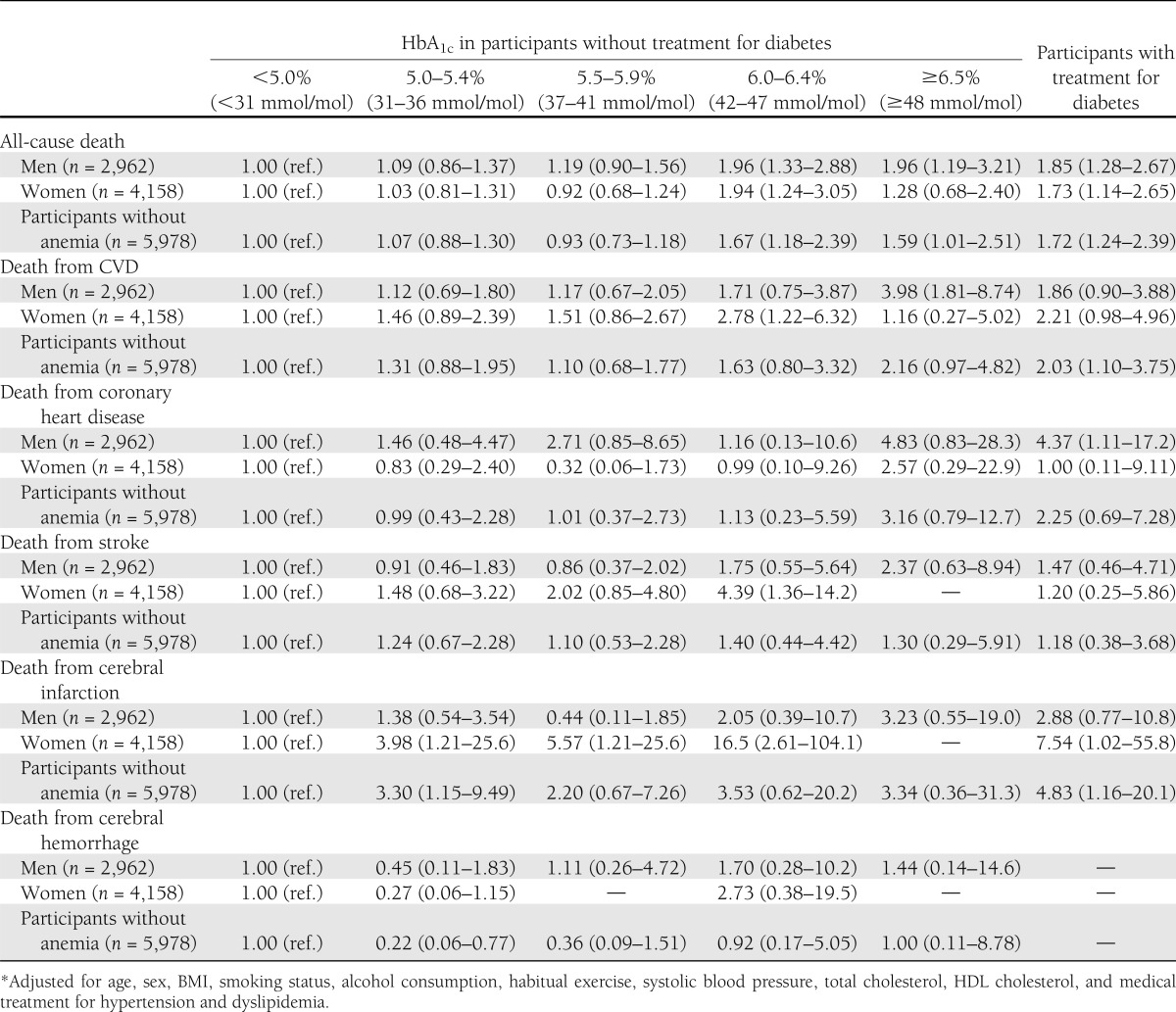
When the association was evaluated separately by sex (Table 3), the results were similar between men and women, and no interaction was observed between sex and HbA1c with regard to the association with all-cause death or death from any CVD (P for interactions: 0.283 for all-cause death, 0.405 for CVD death, 0.119 for death from coronary heart disease, 0.709 for death from stroke, 0.880 for death from cerebral infarction, and 0.390 for death from cerebral hemorrhage). The results were similar when the associations were evaluated after excluding those with anemia (Table 3).
Table 3.
Multivariate-adjusted HR* of death according to the baseline HbA1c levels in men, women, and participants without anemia: sensitivity analyses, NIPPON DATA90, 1990–2005
CONCLUSIONS
In the present prospective, community-based study in Japan, the HbA1c level in individuals without treatment for diabetes was significantly and positively associated with an increased risk for all-cause mortality and death from CVD. Among CVDs, coronary heart disease and cerebral infarction were associated with HbA1c levels. The multivariate-adjusted HR for death from CVD was significantly higher for the participants with HbA1c >6.0% (42 mmol/mol) compared with HbA1c <5.0% (31 mmol/mol), even though they were not diagnosed as having diabetes based on HbA1c levels.
Since the association between HbA1c and microangiopathy in patients with diabetes was established, HbA1c has been used for not only the determination of glucose control among patients with diabetes but also the diagnosis of diabetes (1). Macrovascular complications are not specific to diabetes, and the association between HbA1c and the risk for CVD has been reported in the general population (3–13) as well as patients with diabetes (25–28). Recent American College of Cardiology Foundation and American Heart Association guidelines indicate that measurement of HbA1c may be reasonable for cardiovascular risk assessment in asymptomatic adults without a diagnosis of diabetes (2). However, the association between HbA1c and the risk for CVD has been reported mainly from Western countries. A recent study in Japan found a significant association between HbA1c and the incidence of CVD (13), although the number of participants was small (n = 1,607) and no association between HbA1c and the incidence of myocardial infarction was shown owing to the small number of cases. Our results demonstrate that HbA1c was significantly associated with not only all-cause mortality and death from CVD but also death from coronary heart disease in a Japanese population. The Atherosclerosis Risk in Communities Study showed that multivariate-adjusted HRs in participants with HbA1c 6.0–6.4% and ≥6.5% were 1.88 (95% CI 1.55–2.28) and 2.46 (1.84–3.28) for the incidence of coronary heart disease and 2.19 (1.58–3.05) and 2.96 (1.87–4.67) for ischemic stroke, respectively, compared with participants with HbA1c 5.0–5.5% (10). The European Prospective Investigation into Cancer (EPIC)-Norfolk study also evaluated the HbA1c categories and CVD death, and relative risk of the participants with HbA1c 5.5–6.9% was ~2.5 compared with the participants with HbA1c <5.0% (3). Thus, the relative strength of the association of HbA1c with CVD risk in Japanese people was similar to that in Western individuals.
Previous studies in Western countries indicated increased cardiovascular risk with an increase in HbA1c within the nondiabetic range (3–8,10,29). In the current study, participants with HbA1c 6.0–6.4% (42–47 mmol/mol) had a significantly increased risk of death from CVD and cerebral infarction. HbA1c values were more closely related to postprandial hyperglycemia than to fasting glucose levels (30). High-normal HbA1c levels, even within the nondiabetic range, may reflect the presence of impaired glucose tolerance and postprandial hyperglycemia, which are important risk factors for CVD (31). Individuals with an HbA1c level of 6.0–6.4% (42–47 mmol/mol) are at high risk for progression to diabetes (1) as well as high risk for CVD. Future public health campaigns targeting CVD and type 2 diabetes should focus on lifestyle and other risk factors in these high-risk individuals.
Significant linear associations between HbA1c and all-cause death and death from CVD were observed in our study. Recently, a J-shape relationship between HbA1c and all-cause mortality was reported in a study of the New Zealand general population (8). Participants with HbA1c <4.0% (20 mmol/mol) had the highest mortality rates of those without diabetes, and the HR was 2.90 compared with participants with an HbA1c of 4.0–4.9% (20–30 mmol/mol). As discussed by the authors, it was difficult to determine whether the increased risk of mortality for participants with very low HbA1c levels was causal or merely a result of reserve causation due to preexisting disease. In our study, the number of participants with HbA1c <4.0% (20 mmol/mol) was too small (n = 15) to evaluate the risk of death.
The association between the incidence of hemorrhagic stroke and diabetes is controversial. Studies have indicated an increased risk for hemorrhagic stroke in individuals with diabetes diagnosed by fasting glucose levels (32); a decreased risk in individuals with overt diabetes (33); or no association in individuals with overt diabetes (34) or with diabetes defined by fasting (35), 1-h (36), or 2-h post–glucose load measurements (35). Similar to our results, those of one previous study showed no association between hemorrhagic stroke and HbA1c level (12). The etiology and pathophysiology of ischemic and hemorrhagic stroke are different (37), which may also indicate different risk factors for the two stroke subtypes.
The strength of the current study was that these data were from a large, nationally representative cohort, and thus our findings can be generalized to the whole Japanese population. Another strength lies in the large sample size and long-term follow-up period compared with those in other Asian studies. Therefore, we could evaluate the associations separately for subtypes of CVD. Third, most previous studies in Asian countries were from Japan and used JDS values for HbA1c, whereas our analyses used NGSP values for HbA1c, allowing our data to be compared with those from Western countries. The main limitation of this study was that because fasting glucose was not measured in all participants, analyses on fasting glucose could not performed. It is difficult to obtain fasting blood samples at a mass health check-up. However, fasting is not necessary for assessment of HbA1c, and our data suggested that HbA1c would facilitate assessment of CVD risk associated with glucose metabolism at mass health check-ups, even if a fasting blood sample is not obtained. Another limitation was that deaths from stroke, especially hemorrhagic stroke, were too few to detect any significant relationship. Similarly, the number of participants with very low HbA1c levels was too few to allow evaluation of the mortality risk in these individuals. Another limitation was that we did not have data for some CVD risk factors associated with glucose metabolism, such as waist circumference and fasting triglycerides levels. A further limitation was that we used a single measurement of HbA1c at baseline, which might have underestimated the relationship owing to regression dilution bias (38), and changes in HbA1c during the 15-year follow-up period were not taken into account.
In conclusion, HbA1c was significantly and positively associated with an increased risk for all-cause mortality and mortality from CVD and coronary heart disease in this long-term cohort from a representative Japanese population. A higher risk of CVD was observed even in participants with HbA1c levels of 6.0–6.4% (42–47 mmol/mol), which are below the threshold for diabetes. HbA1c is a useful marker of glucose metabolism for mass screening because fasting is not required for its assessment. Our results showed that HbA1c was associated with CVD death in general East Asian populations, as in Western populations. Further study is needed to establish whether the measurement of HbA1c is useful for cardiovascular risk assessment in general East Asian populations.
Supplementary Material
Acknowledgments
This study was supported by a grant-in-aid from the Ministry of Health, Labor and Welfare under the auspices of the Japanese Association for Cerebro-cardiovascular Disease Control; a Research Grant for Cardiovascular Diseases (7A-2) from the Ministry of Health, Labor and Welfare; and a Health and Labor Sciences Research Grant, Japan (Comprehensive Research on Aging and Health [H11-Chouju-046, H14-Chouju-003, H17-Chouju-012, and H19-Chouju-Ippan-014], and Comprehensive Research on Life-Style Related Diseases including Cardiovascular Diseases and Diabetes Mellitus [H22-Jyunkankitou-Seisyu-Sitei-017]).
No potential conflicts of interest relevant to this article were reported.
M.S. performed the analysis, wrote the manuscript, and approved the final version of the manuscript. S.S. collected data, performed the analysis, wrote the manuscript, and approved the final version of the manuscript. K.M. and H.N. collected data, contributed to discussion, reviewed and edited the manuscript, and approved the final version of the manuscript. H.O. and H.A. contributed to discussion, reviewed and edited the manuscript, and approved the final version of the manuscript. A.K., Y.K., T.H., T.Ohk., A.O., T.Oka., and H.U. collected data, contributed to the discussion, reviewed and edited the manuscript, and approved the final version of the manuscript. K.M. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc12-2412/-/DC1.
A complete list of members of the NIPPON DATA Research Group can be found in Supplementary Data online.
References
- 1.International Expert Committee International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 2009;32:1327–1334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Greenland P, Alpert JS, Beller GA, et al. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2010;122:2748–2764 [DOI] [PubMed] [Google Scholar]
- 3.Khaw KT, Wareham N, Luben R, et al. Glycated haemoglobin, diabetes, and mortality in men in Norfolk cohort of European Prospective Investigation of Cancer and Nutrition (EPIC-Norfolk). BMJ 2001;322:15–18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Blake GJ, Pradhan AD, Manson JE, et al. Hemoglobin A1c level and future cardiovascular events among women. Arch Intern Med 2004;164:757–761 [DOI] [PubMed] [Google Scholar]
- 5.Selvin E, Coresh J, Shahar E, Zhang L, Steffes M, Sharrett AR. Glycaemia (haemoglobin A1c) and incident ischaemic stroke: the Atherosclerosis Risk in Communities (ARIC) Study. Lancet Neurol 2005;4:821–826 [DOI] [PubMed] [Google Scholar]
- 6.Selvin E, Coresh J, Golden SH, Brancati FL, Folsom AR, Steffes MW. Glycemic control and coronary heart disease risk in persons with and without diabetes: the atherosclerosis risk in communities study. Arch Intern Med 2005;165:1910–1916 [DOI] [PubMed] [Google Scholar]
- 7.Myint PK, Sinha S, Wareham NJ, et al. Glycated hemoglobin and risk of stroke in people without known diabetes in the European Prospective Investigation into Cancer (EPIC)-Norfolk prospective population study: a threshold relationship? Stroke 2007;38:271–275 [DOI] [PubMed] [Google Scholar]
- 8.Brewer N, Wright CS, Travier N, et al. A New Zealand linkage study examining the associations between A1C concentration and mortality. Diabetes Care 2008;31:1144–1149 [DOI] [PubMed] [Google Scholar]
- 9.Adams RJ, Appleton SL, Hill CL, et al. Independent association of HbA(1c) and incident cardiovascular disease in people without diabetes. Obesity (Silver Spring) 2009;17:559–563 [DOI] [PubMed] [Google Scholar]
- 10.Selvin E, Steffes MW, Zhu H, et al. Glycated hemoglobin, diabetes, and cardiovascular risk in nondiabetic adults. N Engl J Med 2010;362:800–811 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Nakanishi S, Yamada M, Hattori N, Suzuki G. Relationship between HbA(1)c and mortality in a Japanese population. Diabetologia 2005;48:230–234 [DOI] [PubMed] [Google Scholar]
- 12.Sunaga K, Miura K, Naruse Y, et al. Glycated hemoglobin and risk of stroke, ischemic and hemorrhagic, in Japanese men and women. Cerebrovasc Dis 2008;26:310–316 [DOI] [PubMed] [Google Scholar]
- 13.Watanabe M, Kokubo Y, Higashiyama A, Ono Y, Okayama A, Okamura T. New diagnosis criteria for diabetes with hemoglobin A1c and risks of macro-vascular complications in an urban Japanese cohort: the Suita study. Diabetes Res Clin Pract 2010;88:e20–e23 [DOI] [PubMed] [Google Scholar]
- 14.Kashiwagi A, Kasuga M, Araki E, et al. Committee of the Standardization of Diabetes Mellitus-Related Laboratory Testing of Japan Diabetes Society International clinical harmonization of glycated hemoglobin in Japan: from Japan Diabetes Society to National Glycohemoglobin Standardization Program values. J Diabetes Invest 2012;3:39–40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ueshima H, Sekikawa A, Miura K, et al. Cardiovascular disease and risk factors in Asia: a selected review. Circulation 2008;118:2702–2709 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lida M, Ueda K, Okayama A, et al. Nippon Data 80 Research Group Impact of elevated blood pressure on mortality from all causes, cardiovascular diseases, heart disease and stroke among Japanese: 14 year follow-up of randomly selected population from Japanese -- Nippon data 80. J Hum Hypertens 2003;17:851–857 [DOI] [PubMed] [Google Scholar]
- 17.NIPPON DATA80 Research Group Risk assessment chart for death from cardiovascular disease based on a 19-year follow-up study of a Japanese representative population. Circ J 2006;70:1249–1255 [DOI] [PubMed] [Google Scholar]
- 18.Okamura T, Hayakawa T, Kadowaki T, Kita Y, Okayama A, Ueshima H, NIPPON DATA90 Research Group The inverse relationship between serum high-density lipoprotein cholesterol level and all-cause mortality in a 9.6-year follow-up study in the Japanese general population. Atherosclerosis 2006;184:143–150 [DOI] [PubMed] [Google Scholar]
- 19.Kadota A, Hozawa A, Okamura T, et al. NIPPON DATA Research Group Relationship between metabolic risk factor clustering and cardiovascular mortality stratified by high blood glucose and obesity: NIPPON DATA90, 1990-2000. Diabetes Care 2007;30:1533–1538 [DOI] [PubMed] [Google Scholar]
- 20.Okamura T, Tanaka H, Miyamatsu N, et al. NIPPON DATA80 Research Group The relationship between serum total cholesterol and all-cause or cause-specific mortality in a 17.3-year study of a Japanese cohort. Atherosclerosis 2007;190:216–223 [DOI] [PubMed] [Google Scholar]
- 21.Takashima N, Miura K, Hozawa A, et al. NIPPON DATA 90 Research Group Population attributable fraction of smoking and metabolic syndrome on cardiovascular disease mortality in Japan: a 15-year follow up of NIPPON DATA90. BMC Public Health 2010;10:306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nakamura M, Sato S, Shimamoto T. Improvement in Japanese clinical laboratory measurements of total cholesterol and HDL-cholesterol by the US Cholesterol Reference Method Laboratory Network. J Atheroscler Thromb 2003;10:145–153 [DOI] [PubMed] [Google Scholar]
- 23.Okamura T, Hayakawa T, Kadowaki T, et al. NIPPONDATA80 Research Group Resting heart rate and cause-specific death in a 16.5-year cohort study of the Japanese general population. Am Heart J 2004;147:1024–1032 [DOI] [PubMed] [Google Scholar]
- 24.Kilpatrick E, Bloomgarden Z, Zimmet P. Is haemoglobin A1c a step forward for diagnosing diabetes? BMJ 2009;339:b4432. [DOI] [PubMed] [Google Scholar]
- 25.Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405–412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Selvin E, Marinopoulos S, Berkenblit G, et al. Meta-analysis: glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann Intern Med 2004;141:421–431 [DOI] [PubMed] [Google Scholar]
- 27.Currie CJ, Peters JR, Tynan A, et al. Survival as a function of HbA(1c) in people with type 2 diabetes: a retrospective cohort study. Lancet 2010;375:481–489 [DOI] [PubMed] [Google Scholar]
- 28.Zoungas S, Chalmers J, Ninomiya T, et al. ADVANCE Collaborative Group Association of HbA1c levels with vascular complications and death in patients with type 2 diabetes: evidence of glycaemic thresholds. Diabetologia 2012;55:636–643 [DOI] [PubMed] [Google Scholar]
- 29.Pradhan AD, Rifai N, Buring JE, Ridker PM. Hemoglobin A1c predicts diabetes but not cardiovascular disease in nondiabetic women. Am J Med 2007;120:720–727 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Woerle HJ, Pimenta WP, Meyer C, et al. Diagnostic and therapeutic implications of relationships between fasting, 2-hour postchallenge plasma glucose and hemoglobin a1c values. Arch Intern Med 2004;164:1627–1632 [DOI] [PubMed] [Google Scholar]
- 31.DECODE Study Group, the European Diabetes Epidemiology Group. Glucose tolerance and cardiovascular mortality: comparison of fasting and 2-hour diagnostic criteria. Arch Intern Med 2001;161:397–405 [DOI] [PubMed] [Google Scholar]
- 32.Zia E, Pessah-Rasmussen H, Khan FA, et al. Risk factors for primary intracerebral hemorrhage: a population-based nested case-control study. Cerebrovasc Dis 2006;21:18–25 [DOI] [PubMed] [Google Scholar]
- 33.Megherbi S-E, Milan C, Minier D, et al. European BIOMED Study of Stroke Care Group Association between diabetes and stroke subtype on survival and functional outcome 3 months after stroke: data from the European BIOMED Stroke Project. Stroke 2003;34:688–694 [DOI] [PubMed] [Google Scholar]
- 34.Inagawa T. Risk factors for primary intracerebral hemorrhage in patients in Izumo City, Japan. Neurosurg Rev 2007;30:225–234 [DOI] [PubMed] [Google Scholar]
- 35.Hyvärinen M, Tuomilehto J, Mähönen M, et al. DECODE Study Group Hyperglycemia and incidence of ischemic and hemorrhagic stroke-comparison between fasting and 2-hour glucose criteria. Stroke 2009;40:1633–1637 [DOI] [PubMed] [Google Scholar]
- 36.Burchfiel CM, Curb JD, Rodriguez BL, Abbott RD, Chiu D, Yano K. Glucose intolerance and 22-year stroke incidence. The Honolulu Heart Program. Stroke 1994;25:951–957 [DOI] [PubMed] [Google Scholar]
- 37.Collins C. Pathophysiology and classification of stroke. Nurs Stand 2007;21:35–39 [DOI] [PubMed] [Google Scholar]
- 38.MacMahon S, Peto R, Cutler J, et al. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 1990;335:765–774 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.