

Abstract
Background
Radiotherapy of locally-advanced non-small cell lung cancer is limited by radiation-induced pneumonitis and fibrosis. We have further investigated the role of soy isoflavones to improve the effect of a high intensity radiation and reduce lung damage in a pre-clinical lung tumor model.
Methods
Human A549 NSCLC cells were injected i.v. in nude mice to generate a large tumor burden in the lungs. Mice were treated with lung irradiation at 10 Gy and with oral soy. The therapy effect on the tumor cells and surrounding lung tissue was analyzed on lung sections stained with H&E, Ki-67 and Masson’s Trichrome. Pneumonitis and vascular damage were evaluated by measurements of alveolar septa and immunofluorescent staining of vessel walls.
Results
Combined soy and radiation caused a significantly stronger inhibition of tumor progression compared to each modality alone in contrast to large invasive tumor nodules seen in control mice. At the same time, soy reduced radiation injury in lung tissue by decreasing pneumonitis, fibrosis and protecting alveolar septa, bronchioles and vessels.
Conclusions
These studies demonstrate a differential effect of soy isoflavones on augmenting tumor destruction induced by radiation while radioprotecting normal lung tissue and support using soy to alleviate radiotoxicity in lung cancer.
Keywords: Lung cancer, radiation, soy isoflavones
INTRODUCTION
Lung cancer is the second most common malignancy in both men and women in the USA and the leading cause of death. It is estimated that over 215,000 people per year will be diagnosed with lung cancer (1). Approximately, 85% of lung cancers are classified as non-small cell lung cancer (NSCLC), which includes squamous cell carcinoma, adenocarcinoma and large cell carcinoma. A third of patients with newly diagnosed NSCLC present with unresectable stage III locally advanced disease with an overall 5-year survival rate of 20%, emphasizing the need to improve the therapeutic ratio (2). Locally advanced disease is currently treated by concurrent chemo-radiotherapy (3, 4). High intensity radiotherapy could be more effective but is limited by lung tissue toxicity presenting as radiation pneumonitis, which is an interstitial pulmonary inflammation that develops in up to 30% of patients after thoracic radiation (5–7). Radiation pneumonitis is caused by an early inflammatory process triggered by damage to lung parenchyma, epithelial cells, vascular endothelial cells and stroma that involves induction of pro-inflammatory cytokines and chemokines which recruit inflammatory immune cells in the lung tissue (8–11). It is now believed that this acute early pneumonitis actually progresses to a chronic inflammation mediated by cyclical phases of cytokines, chemokines and growth factors released in the tissue microenvironment (9, 12). These complex events culminate in the later stage of lung fibrosis which is due to excessive accumulation of collagen and other extracellular (ECM) components (9, 12, 13). These adverse events of radiotherapy affect patients’ breathing and their quality of life (5, 6, 12, 14). It is axiomatic that biological-based strategies that enhance damage to malignant cells and reduce damage to normal cells, would be able to increase the volume that could be irradiated with higher doses without increasing toxicity.
Our previous studies indicate that soy isoflavones, which are plant estrogens extracted from soy beans and non-toxic dietary compounds, could be exploited as biological agents to sensitize cancer to radiation while simultaneously protect surrounding normal tissues. These studies demonstrated that soy isoflavones sensitized cancer cells to radiation both in vivo and in vitro in pre-clinical tumor models of lung cancer, prostate cancer and renal cell carcinoma (15–22). Our mechanistic studies showed that soy isoflavones radiosensitized human NSCLC cells by inhibition of critical survival pathways which are constitutively activated in cancer cells and are further upregulated by radiation (20, 22). These include DNA repair processes and key transcription factors such as nuclear factor-kappaB (NF-κB) and hypoxia inducible factor (HIF-1α) that are responsible for transcription of proteins involved in cell-cycle progression, proteolysis, and angiogenesis and are implicated in cancer radioresistance (20–22). In contrast, normal cells do not express such activated malignant survival pathways and thus, are not affected directly by soy isoflavones.
Furthermore, we found that soy isoflavones can have the dual capability of enhancing radiation damage in the malignancy and simultaneously protecting normal lung from radiation injury using a xenograft pre-clinical lung model (15). Soy isoflavones increased radiation-induced destruction of lung tumor nodules, and also mitigated the vascular damage, inflammation and fibrosis, caused by radiation injury to lung tissue (15). Those initial studies were performed with hemithorax irradiation to the left lung to discriminate between radiation and soy effects in the same mouse by analyzing the left and right lungs separately. We have now expanded these observations by performing studies using full lung irradiation to quantitate the tumor response in both lungs and the radioprotective effects of soy on a larger area of lung tissue, as the left lung comprises one lobe and the right lung has four lobes in mice. We also tested the response of a greater tumor burden, which was generated by injecting a double dose of tumor cells to mimic a more advanced model of lung cancer. To further explore the effect of soy isoflavones on irradiated tumor nodules and irradiated lung tissues, new techniques were developed to monitor and quantify soy radioenhancement effect for lung tumors versus soy radioprotection effect for lung tissue. The anti-tumor effect mediated by soy and radiation was assessed by Ki-67 proliferative index of tumor cells and Masson’s Trichrome (MT) staining of tumor nodules to evaluate tumor-associated stroma, which are important issues for translational purposes. New and original methodologies were developed to evaluate and quantitate the radioprotective effects of soy that were previously observed (15). The thickness of alveolar septa was measured quantitatively as a criterion for pneumonitis. Vascular damage was further investigated by fluorescent staining of the basement membrane of vessels using collagen, endothelial and pericyte specific antibodies to detect vessel abnormalities including thickening and projections. These new studies now confirm and establish the differential effect of soy isoflavones on malignant versus normal tissue.
MATERIALS AND METHODS
Establishment of NSCLC advanced lung tumor model
The human non-small cell lung carcinoma (NSCLC) A549 (purchased from ATCC) was cultured in F-12K culture medium containing 7% heat-inactivated fetal bovine serum with supplements. A549 cells, at 4×106 in 200 μl HBSS, were injected i.v. in the tail vein of 5–6 week old female Hsd Athymic Nude-Foxn1nu nu/nu nude mice (Harlan, Indianapolis, IN) (15). Mice were housed and handled under sterile conditions in facilities accredited by the American Association for the Accreditation of Laboratory Animal Care (AAALAC). The animal protocol was approved by Wayne State University Animal Investigation Committee (IACUC). To monitor tumor establishment in the lungs of mice, preliminary kinetics experiments were performed and mice were sacrificed at different time points after i.v. injection of A549 cells. Lungs were resected and processed for histological staining with hematoxylin-eosin (H&E). Established tumor nodules of about 600 μm in diameter were observed by day 16–18 in the midst of the lung tissue, therefore this time point was selected to initiate treatment with soy isoflavones.
Soy Isoflavones
The G-4660 soy isoflavone mixture used is a pure extract of 98.16% isoflavones from soybeans consisting of 83.3% genistein, 14.6% daidzein and 0.26% glycitein (manufactured by Organic Technologies and obtained from NIH). The soy isoflavones mixture was dissolved in 0.1 mol/L Na2CO3 and mixed with sesame seed oil at a 2:1 ratio just prior to treatment to facilitate gavage and avoid irritation of the esophagus by Na2CO3 (15). Mice were orally treated with soy isoflavones by gavage. Control mice received the vehicle alone.
Tumor-bearing lung irradiation
Photon irradiation was performed at a dose of 10 Gy with a Siemens Stabilipan X-ray set (Siemens Medical Systems, Inc) operated at 250 kV, 15 mA with 1 mm copper filtration at a distance of 47.5 cm from the target. Three anesthetized mice, in jigs, were positioned under a 6.4 mm lead shield with 3 cut-outs in an aluminum frame mounted on the X-ray machine to permit selective irradiation of tumor-bearing lungs in the thoracic area, as described previously (15). The radiation dose to the lung and the scattered dose to areas of the mouse outside of the radiation field were carefully monitored. To minimize backscattering of radiation, the bottom of the aluminum frame that holds the jigs was hollowed out and the backplate of the jig was thinned to 1.6mm thickness. Under these conditions and with the lead shielding, the X ray dose to the shielded regions was reduced to 1% of the thoracic dose. The dose rate was 101 cGy/min and HVL was 2 mm Cu.
Experimental protocol
Mice bearing established A549 lung tumor nodules were pre-treated with soy isoflavones at a dose of 5mg/day (equivalent to 250mg/kg) for 3 days from day 16–18 after cell injection. On day 19, the full lung was selectively irradiated by delivering 10 Gy to the thorax while shielding the rest of the mouse body with lead. Soy treatment was then continued on a daily basis for 5 more days at 5mg/day. Then mice were treated with a lower dose of 1mg/day (equivalent to 50mg/kg) for an additional four weeks administered five days a week. The rationale for giving a higher dose of soy isoflavones for pre-treatment and just after radiation is to optimize the effect of soy for radiosensitization, based on previous studies (15–19). We found that either dose cause radioenhancement on the tumor. At a dose of 1mg/day of soy the levels of isoflavones measured in the serum of mice treated with soy isoflavones reflected typical in vivo metabolism with significant levels of daidzein (1.6 μM) and genistein (1.7 μM) (18). To assess the therapeutic response of lung tumors to soy and radiation, 9–10 mice per experimental group were treated. By day 50 after cell implant, the tumor nodules in untreated lungs were very large up to 1200 μm in diameter. Therefore this time point was selected for termination of the experiment so that the tumor nodules in treatment groups could be directly compared with those in control group prior to possible mouse death from tumor burden. Mice were killed and lungs were perfused with 10% buffered formalin prior to resection.
Lung tissue preparation for histology
Formalin fixed lungs were embedded in paraffin and cut into 5 μm sections. Sections were stained with hematoxylin-eosin (H&E). Quantitation of histological findings was performed by evaluation of H&E stained lungs using a Nikon E-800 microscope. Morphometric measurements of the surface area of each tumor nodule were performed using Image-ProPlus version 6.2 software (MediaCybernetics). The Image-ProPlus software was also used to make morphometric measurements of the thickness of alveolar septa in order to evaluate the effect of soy isoflavones on radiation-induced lung damage. The ratio of alveolar septa area relative to the total area of a 20X field was quantified while contouring and excluding bronchioles and large vessels (see inset Table 2) and was performed in 20 fields of 20X. Proliferation of tumor cells in lung nodules was assessed by Ki-67 nuclear staining with anti-Ki-67 antibody (Ab) (LifeSpan, Seattle, WA) followed by anti-rabbit biotinylated secondary Ab (Vector Laboratories, Burlingame, CA), using an avidin-biotin immunoperoxidase technique (Vector). The extent of fibrosis was evaluated using Masson’s Trichrome (MT) stain (NovaUltra Kit, IHCWORLD, Woodstock, MD) (15, 23).
Table 2.
Quantitation of alveolar septa thickness in lungs from mice treated with soy and radiation
| Ratio of Alveolar Septa Area/20X Field | |||||
|---|---|---|---|---|---|
| Treatment | Regular Septaa | Thick Septab | Regular Septac | ||
| Area Ratio Range | 0.3 – 0.50 | 0.51 – 0.65 | 0.3–0.50 | ||
| Proportion | Percent | Proportion | Percent |
|
|
| Tumor-Bearing Lungs Control | 13/20 | 65% | 7/20 | 35% | |
| Radiation | 11/20 | 55% | 9/20 | 45% | |
| Soy | 17/20 | 85% | 3/20 | 15% | Thick Septad 0.51–0.65 |
| Radiation + Soy | 14/20 | 70% | 6/20 | 30% |
|
| Normal Lung | 16/20 | 80% | 4/20 | 20% | |
Using software analysis of H&E slides, the ratio of alveolar septa area relative to the total area of 20X field was quantified in 20 fields of 20X while contouring and excluding bronchioles and large vessels (see insetc). Data were stratified by using a ratio of 0.3–0.50 to define regular normal septaa, c and 0.51–0.65 to define thick septab, d which is indicative of pneumonitis (see insetd). Data computed on lungs from 2 representative mice are presented.
The lung vasculature was visualized by fluorescent immunostaining, as previously shown in other studies (24–26). Endothelial cells were identified with rat anti-mouse CD31 Ab (Thermo Scientific, Fremont, CA) followed by tetramethylrhodamine (TRITC)-labeled secondary goat anti-rat Ab (Molecular Probes, Grand Island, NY). Pericytes were identified with mouse anti-α-SMA (Sigma, St. Louis, MO) followed by Alexa Fluor 350-conjugated secondary goat anti- mouse Ab. The vessel basement membrane was stained with rabbit anti-collagen type IV Ab (Millipore, Billerica, MA) followed by Alexa Fluor 488-conjugated secondary goat anti-rabbit Ab (Molecular Probes). All slides were examined using a Nikon E-800 fluorescent microscope. Digital images were taken separately with each fluorescent dye, including red for endothelial cells, blue for pericytes and green for collagen, and were then processed to create composite images with the three colors using Image-ProPlus version 6.2 software.
Statistical analysis
For histological data analysis, differences in the size of tumor nodules, tumor area and Ki-67 positive tumor nuclei among the various treatments groups were analyzed by two-tailed unpaired Student’s t test.
RESULTS
Enhanced therapeutic response to high dose radiation by soy isoflavones in lung tumor nodules
We have shown previously that soy isoflavones combined with left lung irradiation augments destruction of lung tumor nodules in the A549 orthotopic lung tumor model (15). We have here expanded these studies to investigate the effect of a high thoracic radiation dose of 10 Gy combined with soy isoflavones in lungs bearing a greater tumor burden and analyze further the effect of the therapy on the tumor cells, the surrounding tumor microenvironment and lung tissue structures. Mice bearing established A549 lung tumors were pretreated on day 16 after i.v. cell injection with soy for 3 days, and then received 10 Gy irradiation administered to the whole lung. Soy treatment was continued for 5 days/week for 5 more weeks as detailed in Materials and Methods. In this study, at initiation of treatment, the tumor burden was greater because A549 tumor cells were injected at a double dose of 4 × 106 cells compared to 2 ×106 in the previous study (15). This caused the formation of larger tumor nodules by day 50 after cell injection which invaded most of the lung tissue (Supp Fig 1A). Smaller tumor nodules were observed following soy (Supp Fig 1B) or radiation (Supp Fig 1C) treatments. A few small nodules were detected after treatment of radiation combined with soy resulting in much greater areas of lung parenchyma free of tumors (Supp Fig 1D). In control mice, the tumor nodules were very large with a mean area of about 70 × 104 μm2 and several nodules measured greater than 100 × 104 μm2 (Table 1, Supp Fig 2. A1). These tumor nodules presented with a high Ki-67 proliferation index of a mean of 147 positive nuclei per nodule (Supp Fig 2. A2, Table 1). MT staining revealed blue collagen matrix supporting the tumor cells, and an extensive network of red vessels infiltrating the tumor nodule (Supp Fig 2. A3). Even though the tumor burden was much greater than in our previous studies (15), inhibition of tumor growth by soy or radiation was still evident.
Table 1.
Morphometric measurements of A549 lung tumor nodules from mice treated with soy and radiation
| Nodule Areaa mean±SE×104 μm2 | Rangeb (×104 μm2) | Tumor Areac (%) | Ki-67+ Nucleid mean±SE | |
|---|---|---|---|---|
| Control | 70 ± 8 | 31–180 | 62 ± 4 | 147 ± 17 |
| Soy | 18 ± 3 | 4–52 | 32 ± 7 | 50 ± 8 |
| Radiation | 10 ± 4 | 1–35 | 17 ± 5 | 38 ± 6 |
| Rad + Soy | 3 ± 1 | 1–8 | 8 ± 2 | 16 ± 3 |
The surface areas of lung tumor nodules were estimated by morphometric measurements of each nodule in an average of 20 fields, using H&E stained lung tissue sections obtained from 3 mice per treatment group. In control and soy-treated groups, we are reporting the mean of 100 representative measurable tumor nodules and the mean of 24 tumor nodules in radiation-treated group. In radiation + soy -treated groups (Rad + Soy), 19 fields were analyzed showing 0–2 tumors per field. The mean tumor nodule area ± SE is reported for each treatment group.
The ranges of tumor nodule areas are presented.
The percent tumor area was calculated by dividing the area covered with tumor nodules by the total area of the field comprising tumor nodules and lung tissue. The area covered with tumor nodules was obtained by the sum of all nodules measured in each field. The area of lung tissue surrounding the tumor nodules was morphometrically measured in all analyzed fields. The mean percent tumor area ± SE is reported.
The number of Ki-67 positive nuclei in tumor cells was enumerated in representative tumor nodules. The mean positive nuclei per tumor nodule ± SE is reported.
Soy caused a marked decrease in tumor nodule size with a mean area of 18 × 104 μm2 compared to control tumors (Table 1, p<0.001). In addition, tumor nodules showed degenerative changes, including stromal edema, cell vacuolization and overall a marked decrease in cellularity (Supp Fig 2. B1–2) reflected by a lower number of Ki-67 positive nuclei per nodule compared to control (Table 1, p<0.001). MT staining of tumor nodules revealed changes in tumor associated stroma seen as disruption of collagen matrix and tumor vessels (Supp Fig 2. B3). The effect of radiation was more pronounced resulting in smaller tumor nodules relative to control with a mean area of 10 × 104 μm2 (Table 1, p<0.001). As seen with soy, radiation caused a decrease in cellularity and in the number of Ki-67 positive nuclei per nodule (Table 1, p<0.001), as well as the formation of vacuolated and multinucleated cells (Supp Fig 2. C1–3). Treatment with soy and radiation inhibited tumor growth, and only a few remaining small nodules were found, with a mean area of 3 × 104 μm2 and a much narrower range of 1–8 × 104 μm2 (Table 1, p<0.001 relative to control). Marked cellular aberrations in tumor cell morphology and a heavy infiltration of inflammatory cells were observed (Supp Fig 2. D1–3) while there were only 16 Ki-67 positive nuclei per nodule (Table 1, p<0.001 relative to control). Tumor cells were separated by prominent collagen, probably representing tissue repair after radiation damage (Supp Fig 2. C3, D3). Compared to control mice showing an average of 62% of the total lung area covered by tumor nodules, a significant decrease was observed in soy or radiation treated lungs in which the relative tumor area shrank respectively to 32% and 17% (Table 1, p<0.001). This process was further reduced to 8% of lung tissue after combined treatment (Table 1, p< 0.001). These data demonstrate a marked effect of soy and radiation in tumor-bearing lungs with a large tumor burden and expand on alterations in the tumor cells and tumor microenvironment.
Recently, we tested the role of soy pre-treatment prior to radiation as a radiosensitizer in vivo, by giving soy on the same day than radiation delivery without pre-treatment. We found that soy was more effective for increasing tumor response if it was given three days prior to radiation. The mean size of the tumors was 2.5 fold smaller in treatment groups receiving 3 days of soy prior to radiation than in treatment groups receiving soy on the day of radiation, without prior treatment. These data support a radiosensitization effect of soy for lung tumors.
Effect of soy and/or radiation on lung alveolar septa and evaluation of pneumonitis
Lung tissue injury induced by radiotherapy leads to an inflammatory process caused by radiation damage to capillary endothelial cells and epithelial lung cells which results in pneumonitis and fibrosis. To evaluate the extent of lung tissue injury induced by radiation and the effect of soy, we developed a novel method to measure the thickness of alveolar septa, which may be considered as one indicator of radiation-induced pneumonitis (27, 28). Morphometric measurements of the thickness of alveolar septa were conducted on H&E stained lung tissue sections. The ratio of alveolar septa area relative to the total area of 20X field was quantified while contouring and excluding bronchioles and large vessels (see inset Table 2). Data were stratified by using an arbitrary cut-off ratio of 0.3–0.5 for normal septa and 0.51–0.65 to define thick septa regarded as reflective of pneumonitis (see insets Table 2). Interestingly, untreated control mice bearing lung tumors had 35% thickened septa, compared to 20% in lungs of naïve mice (not bearing tumor), probably due to an inflammatory response induced by the tumor. Lungs treated with soy showed 15% thickened septa, which could be due to either lower tumor burden or to modulation of the inflammatory response by soy. Radiation increased thickened septa to 45% which suggests an increase in pneumonitis. However, reduction of thickened septa to 30% was observed with radiation and soy (Table 2).
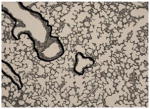
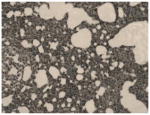
Quantitation of the thickness of alveolar septa demonstrated pneumonitis induced by radiation which was reduced by addition of soy treatment. Because fibrosis in lung tissue is associated with pneumonitis, we evaluated the extent of fibrosis in lung tissue sections obtained on Day 50 by staining with Masson’s Trichrome (Fig. 1). Thin interstitial collagen staining surrounding the vessels and bronchioles was observed in lungs of control tumor-bearing mice (Fig. 1A) and of mice treated with soy (Fig. 1B). In contrast, radiation caused a striking increase in collagen fibers supporting the large vessel walls and bronchial walls, visualized as intense blue staining in the matrix enveloping bronchovascular bundles (Fig. 1C). However, the addition of soy to radiation treatment annulled this effect and the bronchovascular bundles showed only light stain by MT (Fig. 1D), indistinguishable from that found in control, soy-treated lungs or naïve mice not bearing tumors (Fig. 1E). These data suggest that soy inhibits the formation of fibrosis induced by radiation, which can be observed in large vessels and bronchi at a relatively early time point of 4 weeks after radiation.
Fig 1. Soy inhibition of radiation-induced fibrosis in bronchovascular bundles.

Lung tissue sections were stained with Masson’s Trichrome for detection of fibrosis. (A) Control lungs from tumor-bearing mice showing regular pattern of thin collagen fibers (stained in blue) around vessels (V) and bronchioles (B) in lung tissue. (B) Lungs from soy-treated mice showing regular pattern of collagen staining like in control mice. (C) Radiation (Rad) caused a marked increase in density of collagen fibers around vessels and bronchioles in lung tissue. (D) Lung tissues treated with radiation and soy showed normal bronchovascular collagen fibers similar in density to that observed in untreated tumor-bearing lungs (A) or in lung tissue from naïve mice not bearing tumors (E). All magnifications 20X.
Soy isoflavones protect against vessel damage induced by radiation in lung tissue
In the current study and in previous studies, we observed extensive hemorrhages induced by radiation which appeared to be mitigated by soy isoflavones complementary treatment (15, 16, 19). To evaluate further the effect of soy isoflavones on radiation-induced damage to the lung vasculature, lung sections were processed for triple fluorescent staining using anti-CD31 antibody, anti-collagen and anti-SMA to stain endothelial cells, pericytes and the basement membrane of the vessels respectively (24–26). Representative images of large and small vessels of the lung are presented in Figure 2. Lungs from untreated control mice bearing lung-tumors (Fig. 2, A2) or soy-treated mice (Fig. 2B1, B2) showed normal contours of vessels delineated by integral basement membrane, as well as thin normal alveolar septa surrounding bronchioles and vessels. Lungs treated with radiation showed disruption and distortion of the basement membrane of vessels (Fig. 2C1, C2) and thickened, inflamed and hemorrhagic septa (Fig. 2C2). Interestingly, lungs treated with soy and radiation showed less abnormalities in the vascular walls and less septal thickening (Fig. 2D1, D2). These fluorescent stained lung sections were also used to quantitate the total number of vessels and the number of damaged vessels per 40x field in 20 fields. Vessels were considered damaged if the basement membrane was distorted and had abnormal projections (Fig. 2C1, C2). The percentage of disrupted vessels was greater in lungs treated with radiation (42%, Fig. 2C1, C2 ) compared to 29% in control (Fig. 2A1, A2) or soy-treated lungs (Fig. 2B1, B2) which showed mostly vessels with integral basement membrane. In lungs treated with soy combined with radiation, a lower percentage of 25% vessels looked damaged while the other vessels looked healthy (Fig. 2D1, D2).
Fig 2. Fluorescent staining of vasculature in lung tissue sections.

Lung tissue sections were immunostained with fluorescent dyes, including red for endothelial cells (anti-CD31), blue for pericytes (anti-SMA) and green for collagen (anti-collagen IV) as detailed in Materials & Methods. Representative images of large and small vessels (white arrows) of the lung tissues are presented. (A1–2) Vessels with integral basement membranes from control mice. (B 1–2) Vessels from soy-treated mice showing regular green collagen staining of vessel basement membranes. (C1–2) Vessels from radiation-treated mice (Rad) showing disruption or distortion in the continuity of the collagen staining of basement membranes as well as thickening of alveolar septa surrounding the vessels (C2). (D1–2) Vessels from radiation and soy treated mice (Rad + Soy) showing integrity and continuity of vessel walls. The percentage of damaged vessels estimated in 20 fields of 40X, obtained from two mice per group, is reported in the third column. All magnifications 40X.
Soy isoflavones inhibit radiation-induced cytokine release in lungs
Inflammatory cytokines are implicated in radiation-induced pulmonary injury (9, 29). The effect of soy supplementary treatment on the release of inflammatory cytokines in irradiated lungs was tested. In preliminary studies, at 30 and 60 days after irradiation, cytokines were measured by ELISA in lung homogenates obtained from mice receiving whole thorax 10 Gy irradiation alone or combined with soy treatment given prior and after radiation, as detailed in Materials and Methods. An increase in IL-6 was observed after radiation on day 30 but was significantly decreased by addition of soy (p<0.05; Supp Fig. 3). Radiation also induced increases in TNF-α, IL-1β and IFN-γ inflammatory cytokines measured at 1–2 months post-radiation and these cytokine levels were significantly reduced by addition of soy (p<0.05; Supp Fig. 3).
DISCUSSION
The success of radiotherapy for NSCLC patients, presenting with inoperable locally-advanced disease, has been severely restricted by poor local tumor control and by post-therapy toxicity which presents as pneumonitis and later fibrosis (30, 31). The greater the radiation dose that can be delivered to a lung malignancy defined as the gross tumor volume (GTV), the better is the chance of achieving local tumor control and cure. However, this is countered by increased dose to surrounding normal tissue within the radiotherapy planning treatment volume (PTV) which increases the probability of radiation toxicity (4–6). Therefore, there is considerable interest in developing non-toxic biological interventions that can enhance the radiation effect in the GTV and/or reduce unwanted radiation injury in the normal lung tissue within the PTV. Based on our previous studies, we hypothesize that soy isoflavones could be an ideal complementary strategy that simultaneously increases radiation effectiveness on the malignancy while reducing pneumonitis and fibrosis in the normal lung tissue. In this study, we have further explored the differential effect of soy isoflavones on enhancing radiation response of lung tumors and decreasing radiation injury to lung tissue in an orthotopic pre-clinical model of NSCLC.
We selected a high dose of radiation of 10 Gy administered to the whole thorax containing the tumor-bearing lungs to inflict greater damage to normal tissue and evaluate the alleviation of radiation injury by soy. In addition, there is a trend to explore hypofractionation using higher doses per fraction with the total treatment given in a reduced number of fractions and less overall time, which is potentially more effective and more convenient to patients (32, 33). At the same time, this approach could lead to a substantial risk of severe complications driven by radiation-induced pneumonitis and fibrosis (34), which makes the use of soy an attractive strategy to attenuate lung injury. In an advanced model of A549 lung tumors, we demonstrated a considerable effect of lung irradiation combined with systemic soy given before and after radiation, which was much greater than with each modality alone. In contrast to multiple large tumors invading the lung tissues in control mice, soy combined with radiation significantly inhibited the growth of the tumor nodules with only few remaining tumor nodules showing a 95% reduction in size and up to 92% of lung tissue free of tumor. In detectable tumor nodules, marked aberrations included the formation of large vacuoles in tumor cells and inflammatory infiltrates indicative of degenerative changes, as previously described (15). In the current study, we now demonstrate that these nodules had a much lower Ki-67 index of proliferation associated with decreased cellularity and increase in collagen matrix probably as a result of tissue repair after tumor cell destruction. These findings were also observed with radiation alone but were more pronounced with radiation combined with soy. Although soy treatment alone partially inhibited the tumor growth, its effects were not as strong as the combined radiation and soy therapy. These data confirm our previous findings of potentiation of radiation tumor destruction by soy isoflavones (15) and now demonstrate a marked effect of soy and radiation in tumor-bearing lungs with a large tumor burden as well as expand on alterations in the tumor cells and tumor microenvironment.
In NSCLC patients treated with radiotherapy, lung pneumonitis is induced early on following radiation and is associated with the later onset of fibrosis apparently resulting from inflammatory processes (5, 6, 12, 14). Radiation-induced pneumonitis was also documented following single dose or fractionated radiation by 2–4 months after radiation in naïve mice and rats not-bearing lung tumors (8, 23, 35). End-points to assess pneumonitis included measurement of DNA damage in lung cells by micronucleus assay, macrophage activation, cytokine expression and lung function by measuring breathing rate (10, 23, 35, 36). These studies in naïve rodents have also documented a decrease in radiation-induced pneumonitis using the genistein isoflavone or EUK-207 superoxide dismutase (S0D) catalase mimetic confirming a radioprotective effect of genistein, the most active component of soy. Our previous studies showed that the natural extract of soy isoflavones, consisting of the mixture of genistein, daidzein and glycetein isoflavones, is more potent and safer than purified genistein (18, 19). To evaluate further the effect of soy isoflavones on radiation-injury to lungs bearing tumors, we quantitated the extent of pneumonitis by measuring the thickness of alveolar septa, which is thickened by the inflammatory process caused by damage to alveolar structures. A reproducible and consistent increase in pneumonitis was seen in tumor-bearing lungs from control mice, compared to lungs from naïve nude mice, probably as a result of alterations induced by the presence of tumor nodules. Interestingly, lungs treated with soy alone showed mostly normal septa thickness, which could reflect modulation of the inflammatory response by soy. Pneumonitis was increased by radiation as early as 4 weeks after radiation in the lung tissue surrounding tumor nodules, but was decreased when soy was combined with radiation. This new quantitative analysis further confirms the process of attenuation of radiation-induced pneumonitis by soy treatment on a larger irradiated lung parenchyma in support of our previous findings in the left lung (15).
The decreased pneumonitis noted in lungs treated with radiation and soy was also associated with a striking decrease in fibrosis in lung tissue. Extensive studies on MT stained lung tissue sections showed that radiation caused a prominent increase in collagen fibers supporting the vessel walls and bronchiole walls. However, bronchovascular bundles of lungs treated with combined soy and radiation treatment stained lightly with MT, akin to those found in control and in soy-treated lungs. These data suggest that soy inhibits the formation of fibrosis induced by radiation, which can be observed in the periphery of vessels and bronchi at a relatively early time point of 4 weeks after radiation. A decrease in fibrosis caused by genistein or EUK-207 was also observed in irradiated lungs of naïve rodents that could be associated with anti-oxidant and anti-inflammatory mechanisms involving inhibition of TGF-β1 expression which is a major fibrogenic cytokine (13, 36).
Pneumonitis has also been associated with vascular damage induced by radiation. In the current and previous studies, we observed extensive hemorrhages induced by radiation which appeared to be mitigated by soy isoflavones complementary treatment (15, 19). Vascular damage plays an important role in the development of radiation-induced pulmonary toxicity and pulmonary hypertension (37). In the current study, we have evaluated and quantified the effect of soy isoflavones on radiation-induced damage to the lung vasculature by fluorescent staining of the basement membrane of vessels using collagen, endothelial and pericyte specific antibodies which allowed for visualization of vessel abnormalities including thickening and projections, as previously described (24, 25). Radiation caused alterations, interruptions and abnormal projections in the basement membrane of 42% of lung vessels whereas only 25% of vessels were altered in lungs treated with soy combined with radiation. These data suggest a protective role of soy in vascular damage caused by radiation in the lung tissue.
These data confirm that soy mitigated the vascular damage, pneumonitis and fibrosis caused by high dose radiation injury to lung tissue in a pre-clinical lung cancer model, suggesting that soy can alter the radiation-induced inflammatory response. The release of inflammatory cytokines induced by radiation has been implicated in the development of pneumonitis and fibrosis (9, 29). In this study, recent preliminary mechanistic studies on the radioprotective effect of soy on lung tissue demonstrate that soy mediates inhibition of inflammatory cytokine release in irradiated lung tissue. Further studies are currently ongoing to determine the mechanisms of modulation of inflammatory response by soy isoflavones in irradiated lungs. We recently reported further evidence for the radioprotective effect of soy showing that soy inhibited the radiation-increased breathing rate, inflammation and fibrosis in normal lung tissue from immunocompetent BALB/c mice which were not bearing tumors (Hillman et al., In Press, Journal of Thoracic Oncology, 2013). These studies, in normal mice with an intact immune system, confirm our findings on radioprotection of normal lung tissue by soy in tumor-bearing nude mice suggesting that these radioprotective events are mediated by immune inflammatory cells present in nude mice and are independent of T and B cells. Further studies are ongoing to identify the nature of these inflammatory cells. Our findings on soy radioprotective effects are in agreement with previous studies documenting that soy isoflavones act as anti-oxidants in normal tissues as well as chemopreventive agents (22). Soy isoflavones were found to protect normal tissues from treatment-induced toxicity, as clinically observed in prostate cancer patients treated with soy isoflavone tablets during and after radiotherapy showing reduced radiation toxicity to urinary and gastrointestinal functions (38).
Several studies on radioprotectors and mitigators to minimize radiation toxicity are ongoing and include radical scavengers and anti-oxidants, some of which such as amifostine, tempol and melatonin have been clinically tested (14, 39). However, limitations include their safety and tumor protection from radiation effect. The use of soy isoflavones as radioprotectors is attractive because they were proven to be safe in controlled human clinical trials (40). Furthermore, the differential effect of soy isoflavones acting as radioprotectants for normal lung tissue and radiosensitizers for lung tumors suggest that the addition of soy would improve the effectiveness of radiation on the tumor target and reduce the dose-limiting radiotoxicity to the normal lung in advanced stage NSCLC.
Supplementary Material
Lung tissue sections were processed for H& E staining. (A) Control lung from untreated mice showing numerous large tumor nodules (T) and thickened alveolar septa at the vicinity of tumor nodules. (B) Soy-treated lungs with fewer and smaller nodules. (C) Radiation-treated lungs with small tumor nodules and focal areas of hemorrhages. (D) Radiation + Soy treated lungs showing a very small tumor nodule and larger area of lung tissue without tumors. All magnifications 4X.
Lung sections were stained with H&E, anti-Ki-67, and Masson’s Trichrome (MT). (A1–3) Tumor nodules from untreated tumor-bearing mice (Control) showing large tumor nodules with morphological features of adenocarcinoma consisting of large pleomorphic tumor cells, cytoplasmic vacuoles and large nuclei (A1). Numerous nuclei were stained for Ki-67 (A2) and MT revealed blue collagen matrix supporting the tumor cells, and vessels infiltrating the tumor nodule (stained in red) (A3). (B1–3) Tumor nodules from soy-treated mice (Soy) showing degenerative changes, vacuolization and a marked decrease in cellularity and in Ki-67 nuclei staining (B1–2). Disruption of collagen matrix and tumor vessels was seen by MT staining of tumor nodules (B3). (C1–3) Tumor nodules from radiation-treated mice (Rad) were smaller consisting mostly of cells with degenerative changes in the nuclei and cytoplasm with multiple large vacuoles (C1–3), with a decrease in proliferation index (C2, Ki-67) and increase in matrix collagen staining (C3, MT). (D1–3) Tumor nodules from mice treated with soy and radiation (Rad + Soy) showing very small residual tumor nodules (arrowheads) consisting of degenerating giant tumor cells with large vacuoles and inflammatory infiltrates, low Ki-67 staining and strong matrix collagen staining in areas of the nodules devoid of tumor cells. All magnifications 40X.
Cytokine levels were measured in lung homogenates obtained from naïve mice on day 30 (D30) and day 60 (D60) following radiation (RT) or radiation combined with soy (RT+Soy) by ELISA. The results represent the mean ± SE of 3–4 mice per treatment group and of 9 mice in control untreated group; *p < 0.05 in RT+Soy compared to RT only on D30 and D60.
Acknowledgments
These studies were supported by Grant Number 1R21CA155518-01A1 from the National Cancer Institute and American Institute for Cancer Research #10A108. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or National Institutes of Health. We thank Mohit Agarwal for excellent technical assistance.
Footnotes
Conflict of Interest: No financial disclosures.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. doi: 10.3322/caac.20138. [DOI] [PubMed] [Google Scholar]
- 2.van Meerbeeck JP, Meersschout S, De Pauw R, et al. Modern radiotherapy as part of combined modality treatment in locally advanced non–small cell lung cancer: present status and future prospects. Oncologist. 2008;13:700–708. doi: 10.1634/theoncologist.2007-0196. [DOI] [PubMed] [Google Scholar]
- 3.Blackstock AW, Govindan R. Definitive chemoradiation for the treatment of locally advanced non small-cell lung cancer. J Clin Oncol. 2007;25:4146–4152. doi: 10.1200/JCO.2007.12.6581. [DOI] [PubMed] [Google Scholar]
- 4.Bradley JD, Bae K, Graham MV, et al. Primary analysis of the phase II component of a phase I/II dose intensification study using three-dimensional conformal radiation therapy and concurrent chemotherapy for patients with inoperable non-small-cell lung cancer: RTOG 0117. J Clin Oncol. 2010;28:2475–2480. doi: 10.1200/JCO.2009.27.1205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kong FM, Hayman JA, Griffith KA, et al. Final toxicity results of a radiation-dose escalation study in patients with non-small-cell lung cancer (NSCLC): predictors for radiation pneumonitis and fibrosis. Int J Radiat Oncol Biol Phys. 2006;65:1075–1086. doi: 10.1016/j.ijrobp.2006.01.051. [DOI] [PubMed] [Google Scholar]
- 6.Schallenkamp JM, Miller RC, Brinkmann DH, et al. Incidence of radiation pneumonitis after thoracic irradiation: Dose-volume correlates. Int J Radiat Oncol Biol Phys. 2007;67:410–416. doi: 10.1016/j.ijrobp.2006.09.030. [DOI] [PubMed] [Google Scholar]
- 7.Jin H, Tucker SL, Liu HH, et al. Dose-volume thresholds and smoking status for the risk of treatment-related pneumonitis in inoperable non-small cell lung cancer treated with definitive radiotherapy. Radiother Oncol. 2009;91:427–432. doi: 10.1016/j.radonc.2008.09.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hill RP. Radiation effects on the respiratory system. BJR Suppl. 2005;27:75–81. [Google Scholar]
- 9.Bentzen SM. Preventing or reducing late side effects of radiation therapy: radiobiology meets molecular pathology. Nat Rev Cancer. 2006;6:702–713. doi: 10.1038/nrc1950. [DOI] [PubMed] [Google Scholar]
- 10.Hill RP, Zaidi A, Mahmood J, et al. Investigations into the role of inflammation in normal tissue response to irradiation. Radiother Oncol. 2011;101:73–79. doi: 10.1016/j.radonc.2011.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tsoutsou PG, Koukourakis MI. Radiation pneumonitis and fibrosis: mechanisms underlying its pathogenesis and implications for future research. Int J Radiat Oncol Biol Phys. 2006;66:1281–1293. doi: 10.1016/j.ijrobp.2006.08.058. [DOI] [PubMed] [Google Scholar]
- 12.Williams JP, Jackson IL, Shah JR, et al. Animal models and medical countermeasures development for radiation-induced lung damage: report from an NIAID Workshop. Radiat Res. 2012;177:e0025–0039. doi: 10.1667/rrol04.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Yarnold J, Brotons MC. Pathogenetic mechanisms in radiation fibrosis. Radiother Oncol. 2010;97:149–161. doi: 10.1016/j.radonc.2010.09.002. [DOI] [PubMed] [Google Scholar]
- 14.Williams JP, Johnston CJ, Finkelstein JN. Treatment for radiation-induced pulmonary late effects: spoiled for choice or looking in the wrong direction? Curr Drug Targets. 2010;11:1386–1394. doi: 10.2174/1389450111009011386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hillman GG, Singh-Gupta V, Runyan L, et al. Soy isoflavones radiosensitize lung cancer while mitigating normal tissue injury. Radiother Oncol. 2011;101:329–336. doi: 10.1016/j.radonc.2011.10.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hillman GG, Wang Y, Kucuk O, et al. Genistein potentiates inhibition of tumor growth by radiation in a prostate cancer orthotopic model. Mol Cancer Ther. 2004;3:1271–1279. [PubMed] [Google Scholar]
- 17.Hillman GG, Wang Y, Che M, et al. Progression of renal cell carcinoma is inhibited by genistein and radiation in an orthotopic model. BMC Cancer. 2007;7:4. doi: 10.1186/1471-2407-7-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Raffoul JJ, Banerjee S, Che M, et al. Soy isoflavones enhance radiotherapy in a metastatic prostate cancer model. Int J Cancer. 2007;120:2491–2498. doi: 10.1002/ijc.22548. [DOI] [PubMed] [Google Scholar]
- 19.Raffoul JJ, Banerjee S, Singh-Gupta V, et al. Down-regulation of apurinic/apyrimidinic endonuclease 1/redox factor-1 expression by soy isoflavones enhances prostate cancer radiotherapy in vitro and in vivo. Cancer Res. 2007;67:2141–2149. doi: 10.1158/0008-5472.CAN-06-2147. [DOI] [PubMed] [Google Scholar]
- 20.Singh-Gupta V, Joiner MC, Runyan L, et al. Soy isoflavones augment radiation effect by inhibiting APE1/Ref-1 DNA repair activity in non-small cell lung cancer. J Thorac Oncol. 2011;6:688–698. doi: 10.1097/JTO.0b013e31821034ae. [DOI] [PubMed] [Google Scholar]
- 21.Singh-Gupta V, Zhang H, Banerjee S, et al. Radiation-induced HIF-1alpha cell survival pathway is inhibited by soy isoflavones in prostate cancer cells. Int J Cancer. 2009;124:1675–1684. doi: 10.1002/ijc.24015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hillman GG, Singh-Gupta V. Soy isoflavones sensitize cancer cells to radiotherapy. Free Radic Biol Med. 2011;51:289–298. doi: 10.1016/j.freeradbiomed.2011.04.039. [DOI] [PubMed] [Google Scholar]
- 23.Para AE, Bezjak A, Yeung IW, et al. Effects of genistein following fractionated lung irradiation in mice. Radiother Oncol. 2009;92:500–510. doi: 10.1016/j.radonc.2009.04.005. [DOI] [PubMed] [Google Scholar]
- 24.Morikawa S, Baluk P, Kaidoh T, et al. Abnormalities in pericytes on blood vessels and endothelial sprouts in tumors. Am J Pathol. 2002;160:985–1000. doi: 10.1016/S0002-9440(10)64920-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Baluk P, Morikawa S, Haskell A, et al. Abnormalities of basement membrane on blood vessels and endothelial sprouts in tumors. Am J Pathol. 2003;163:1801–1815. doi: 10.1016/S0002-9440(10)63540-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bergers G, Song S. The role of pericytes in blood-vessel formation and maintenance. Neuro Oncol. 2005;7:452–464. doi: 10.1215/S1152851705000232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ashcroft T, Simpson JM, Timbrell V. Simple method of estimating severity of pulmonary fibrosis on a numerical scale. J Clin Pathol. 1988;41:467–470. doi: 10.1136/jcp.41.4.467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hubner RH, Gitter W, El Mokhtari NE, et al. Standardized quantification of pulmonary fibrosis in histological samples. Biotechniques. 2008;44:507–511. 514–507. doi: 10.2144/000112729. [DOI] [PubMed] [Google Scholar]
- 29.Ao X, Zhao L, Davis MA, et al. Radiation produces differential changes in cytokine profiles in radiation lung fibrosis sensitive and resistant mice. J Hematol Oncol. 2009;2:6. doi: 10.1186/1756-8722-2-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Baumann M, Herrmann T, Koch R, et al. Final results of the randomized phase III CHARTWEL-trial (ARO 97-1) comparing hyperfractionated-accelerated versus conventionally fractionated radiotherapy in non-small cell lung cancer (NSCLC) Radiother Oncol. 2011;100:76–85. doi: 10.1016/j.radonc.2011.06.031. [DOI] [PubMed] [Google Scholar]
- 31.Farr KP, Khalil AA, Knap MM, et al. Development of radiation pneumopathy and generalised radiological changes after radiotherapy are independent negative prognostic factors for survival in non-small cell lung cancer patients. Radiother Oncol. 2013 doi: 10.1016/j.radonc.2013.04.024. [DOI] [PubMed] [Google Scholar]
- 32.Timmerman R, Paulus R, Galvin J, et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA. 2010;303:1070–1076. doi: 10.1001/jama.2010.261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Senan S, Palma DA, Lagerwaard FJ. Stereotactic ablative radiotherapy for stage I NSCLC: Recent advances and controversies. J Thorac Dis. 2011;3:189–196. doi: 10.3978/j.issn.2072-1439.2011.05.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lo SS, Sahgal A, Chang EL, et al. Serious complications associated with stereotactic ablative radiotherapy and strategies to mitigate the risk. Clin Oncol (R Coll Radiol) 2013;25:378–387. doi: 10.1016/j.clon.2013.01.003. [DOI] [PubMed] [Google Scholar]
- 35.Calveley VL, Jelveh S, Langan A, et al. Genistein can mitigate the effect of radiation on rat lung tissue. Radiat Res. 2010;173:602–611. doi: 10.1667/RR1896.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Mahmood J, Jelveh S, Zaidi A, et al. Mitigation of Radiation-Induced Lung Injury with EUK-207 and Genistein: Effects in Adolescent Rats. Radiat Res. 2013;179:125–134. doi: 10.1667/RR2954.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ghobadi G, Bartelds B, van der Veen SJ, et al. Lung irradiation induces pulmonary vascular remodelling resembling pulmonary arterial hypertension. Thorax. 2012;67:334–341. doi: 10.1136/thoraxjnl-2011-200346. [DOI] [PubMed] [Google Scholar]
- 38.Ahmad IU, Forman JD, Sarkar FH, et al. Soy isoflavones in conjunction with radiation therapy in patients with prostate cancer. Nutr Cancer. 2010;62:996–1000. doi: 10.1080/01635581.2010.509839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Citrin D, Cotrim AP, Hyodo F, et al. Radioprotectors and mitigators of radiation-induced normal tissue injury. Oncologist. 2010;15:360–371. doi: 10.1634/theoncologist.2009-S104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Messina M, Kucuk O, Lampe JW. An overview of the health effects of isoflavones with an emphasis on prostate cancer risk and prostate-specific antigen levels. J AOAC Int. 2006;89:1121–1134. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Lung tissue sections were processed for H& E staining. (A) Control lung from untreated mice showing numerous large tumor nodules (T) and thickened alveolar septa at the vicinity of tumor nodules. (B) Soy-treated lungs with fewer and smaller nodules. (C) Radiation-treated lungs with small tumor nodules and focal areas of hemorrhages. (D) Radiation + Soy treated lungs showing a very small tumor nodule and larger area of lung tissue without tumors. All magnifications 4X.
Lung sections were stained with H&E, anti-Ki-67, and Masson’s Trichrome (MT). (A1–3) Tumor nodules from untreated tumor-bearing mice (Control) showing large tumor nodules with morphological features of adenocarcinoma consisting of large pleomorphic tumor cells, cytoplasmic vacuoles and large nuclei (A1). Numerous nuclei were stained for Ki-67 (A2) and MT revealed blue collagen matrix supporting the tumor cells, and vessels infiltrating the tumor nodule (stained in red) (A3). (B1–3) Tumor nodules from soy-treated mice (Soy) showing degenerative changes, vacuolization and a marked decrease in cellularity and in Ki-67 nuclei staining (B1–2). Disruption of collagen matrix and tumor vessels was seen by MT staining of tumor nodules (B3). (C1–3) Tumor nodules from radiation-treated mice (Rad) were smaller consisting mostly of cells with degenerative changes in the nuclei and cytoplasm with multiple large vacuoles (C1–3), with a decrease in proliferation index (C2, Ki-67) and increase in matrix collagen staining (C3, MT). (D1–3) Tumor nodules from mice treated with soy and radiation (Rad + Soy) showing very small residual tumor nodules (arrowheads) consisting of degenerating giant tumor cells with large vacuoles and inflammatory infiltrates, low Ki-67 staining and strong matrix collagen staining in areas of the nodules devoid of tumor cells. All magnifications 40X.
Cytokine levels were measured in lung homogenates obtained from naïve mice on day 30 (D30) and day 60 (D60) following radiation (RT) or radiation combined with soy (RT+Soy) by ELISA. The results represent the mean ± SE of 3–4 mice per treatment group and of 9 mice in control untreated group; *p < 0.05 in RT+Soy compared to RT only on D30 and D60.