

Abstract
A 32-year-old woman presented with a 5-year history of left shoulder pain, medial hand and forearm numbness, and progressive hand weakness and atrophy. Electrodiagnostic studies were characteristic of true neurogenic thoracic outlet syndrome,1 and a chest X-ray showed bilateral elongated C7 transverse processes. High-resolution ultrasound studies revealed compression of the left lower trunk (LT) between a fibrous band and artery (figure, A). Magnetic resonance neurography (figure, B) and operative exploration (figure, C) confirmed the ultrasound findings. Clinical improvement was noted following surgical neurolysis of the LT. High-resolution ultrasound may be a useful and quick bedside tool to identify causative structural pathology in this classic neuromuscular disorder.
A 32-year-old woman presented with a 5-year history of left shoulder pain, medial hand and forearm numbness, and progressive hand weakness and atrophy. Electrodiagnostic studies were characteristic of true neurogenic thoracic outlet syndrome,1 and a chest x-ray showed bilateral elongated C7 transverse processes. High-resolution ultrasound studies revealed compression of the left lower trunk (LT) between a fibrous band and artery (figure, A). Magnetic resonance neurography (figure, B) and operative exploration (figure, C) confirmed the ultrasound findings. Clinical improvement was noted following surgical neurolysis of the LT. High-resolution ultrasound may be a useful and quick bedside tool to identify causative structural pathology in this classic neuromuscular disorder.
Figure. Imaging findings in true neurogenic thoracic outlet syndrome.
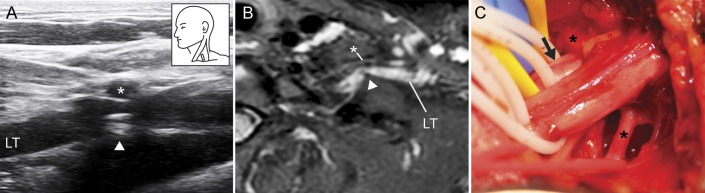
Correlation between ultrasound (A) and MRI (B) demonstrates compression of the lower trunk (LT) between an artery (*) and fibrous band (arrowhead) arising from an elongated C7 transverse process. At operation (C), the artery (*) passed between the middle and lower trunks. Fibrous bands were resected to release the LT (arrow).
Footnotes
Author contributions: Dr. Simon: study design, data acquisition and analysis, drafting and critical revision of the manuscript. Dr. Ralph: data acquisition and analysis, critical revision of the manuscript for important intellectual content. Dr. Chin: data acquisition and analysis, critical revision of the manuscript for important intellectual content. Dr. Kliot: study design, data acquisition and analysis, critical revision of the manuscript for important intellectual content.
Study funding: Dr. Simon acknowledges funding from the National Health and Medical Research Council and the Motor Neurone Disease Research Institute of Australia (grant 1039520).
Disclosure: The authors report no disclosures relevant to the manuscript. Go to Neurology.org for full disclosures.
References
- 1.Wilbourn AJ. The thoracic outlet syndrome is overdiagnosed. Arch Neurol 1990;47:328–330 [DOI] [PubMed] [Google Scholar]