

Abstract
Objective:
Plantar fasciitis is a prevalent problem, with limited consensus among clinicians regarding the most effective treatment. The purpose of this literature review is to provide a systematic approach to the treatment of plantar fasciitis based on the windlass mechanism model.
Data Sources:
We searched MEDLINE, SPORT Discus, and CINAHL from 1966 to 2003 using the key words plantar fasciitis, windlass mechanism, pronation, heel pain, and heel spur.
Data Synthesis:
We offer a biomechanical application for the evaluation and treatment of plantar fasciitis based on a review of the literature for the windlass mechanism model. This model provides a means for describing plantar fasciitis conditions such that clinicians can formulate a potential causal relationship between the conditions and their treatments.
Conclusions/Recommendations:
Clinicians' understanding of the biomechanical causes of plantar fasciitis should guide the decision-making process concerning the evaluation and treatment of heel pain. Use of this approach may improve clinical outcomes because intervention does not merely treat physical symptoms but actively addresses the influences that resulted in the condition. Principles from this approach might also provide a basis for future research investigating the efficacy of plantar fascia treatment.
Keywords: heel pain, pronation, rehabilitation
Plantar fasciitis is a commonly encountered orthopaedic problem1,2 affecting a wide range of athletic adults. Chandler and Kibler3 reported a 10% occurrence rate in runners. Plantar fasciitis is an inflammation of the plantar fascia and the perifascial structures.4,5 Kwong et al4 classified it as a syndrome resulting from repeated trauma to the plantar fascia at its origin on the medial tubercle of the calcaneus.
Historically, the literature attributes plantar fasciitis to faulty biomechanics such as excessive pronation.3,4,6,7 Structural deformities such as forefoot varus may result in excessive pronation during gait. Overpronation contributes to excessive foot mobility, which can increase the level of stresses applied to the musculofascial and soft tissue structures through plantar fascial elongation and increased tissue stress.5,8,9
Pronation does not necessarily lead to lower extremity problems. Donatelli et al10 analyzed the static and dynamic foot postures of 74 professional baseball players. Although 43% of subjects demonstrating excessive pronation reported previous lower extremity injuries, the remaining 57% with similar pronatory patterns experienced no difficulties. These researchers concluded that excessive pronators were no more likely to be injured than those without excessive pronation. Other researchers similarly reported that excessive pronation, in and of itself, did not result in lower extremity abnormalities.11,12
Many studies have demonstrated that excessive foot motion is not deterministic of lower extremity problems.13–15 Cornwall16 stated that difficulties result when the joints of the foot are continually functioning beyond a normal end range. This can lead to greater stress along the medial joint capsules and ligamentous structures. Additionally, muscles such as the posterior tibialis can be in a lengthened position and are easily fatigued in an attempt to control excess motion. These stresses lead to pain, discomfort, and further lengthening.3,4 These authors concluded that plantar fasciitis results from the duration of motion and not merely from the motion itself.
Researchers have also reported faulty biomechanics and plantar fasciitis in subjects with a higher-arched foot.16–18 A higher-arched foot lacks the mobility needed to assist in absorbing ground reaction forces. Consequently, its inability to dissipate the forces from heel strike to midstance increases the load applied to the plantar fascia, much like a stretch on a bowstring.4
A review of the literature reveals that a person displaying either a lower- or higher-arched foot can experience plantar fasciitis. Patients with lower arches have conditions resulting from too much motion, whereas patients with higher arches have conditions resulting from too little motion.4,16,19 Therefore, people with different foot types experience plantar fascia pain resulting from different biomechanical stresses.
The “windlass mechanism” is a mechanical model that provides a thorough explanation of these biomechanical factors and stresses. The windlass mechanism describes the manner by which the plantar fascia supports the foot during weight- bearing activities and provides information regarding the biomechanical stresses placed on the plantar fascia. Such information is important clinically because it may provide health care professionals with a clear understanding about the relationship between abnormalities and biomechanical influences.14–16 A clear understanding of these principles will enhance the decision-making process involved in the evaluation and treatment of patients with plantar fasciitis.20
Our purpose is to describe and explain the causes and appropriate treatment of plantar fasciitis from a biomechanical perspective. This article will (1) define the windlass mechanism, (2) relate normal foot biomechanics to the gait cycle, (3) explain changes in arch height during gait, and (4) relate biomechanical dysfunction to plantar fascia abnormalities. We will conclude by applying biomechanical principles to clinical practice. This application will provide the clinician with an evidence-based approach toward the evaluation and treatment of plantar fasciitis.
The Windlass Mechanism
Hicks21 originally described the foot and its ligaments as an arch-like triangular structure or truss. The calcaneus, midtarsal joint, and metatarsals (the medial longitudinal arch) formed the truss's arch. The plantar fascia formed the tie-rod that ran from the calcaneus to the phalanges. Vertical forces from body weight travel downward via the tibia and tend to flatten the medial longitudinal arch. Furthermore, ground reaction forces travel upward on the calcaneus and the metatarsal heads, which can further attenuate the flattening effect because these forces fall both posterior and anterior to the tibia (Figure 1).22
Figure 1.

The triangle shows the truss formed by the calcaneus, midtarsal joint, and metatarsals. The hypotenuse (horizontal line) represents the plantar fascia. The upward arrows depict ground reaction forces. The downward arrow depicts the body's vertical force. The orientation of the vertical and ground reaction forces would cause a collapse of the truss; however, increased plantar- fascia tension in response to these forces maintains the truss's integrity.
The plantar fascia prevents foot collapse by virtue of its anatomical orientation and tensile strength. The plantar aponeurosis originates from the base of the calcaneus and extends distally to the phalanges (Figure 2). Stretch tension from the plantar fascia prevents the spreading of the calcaneus and the metatarsals and maintains the medial longitudinal arch.14,20,23
Figure 2.

The plantar aponeurosis originates from the base of the calcaneus and extends distally to the phalanges.
A “windlass” is the tightening of a rope or cable.14 The plantar fascia simulates a cable attached to the calcaneus and the metatarsophalangeal joints. Dorsiflexion during the propulsive phase of gait winds the plantar fascia around the head of the metatarsal. This winding of the plantar fascia shortens the distance between the calcaneus and metatarsals to elevate the medial longitudinal arch. The plantar fascia shortening that results from hallux dorsiflexion is the essence of the windlass mechanism principle.4,5,20,22–25
Biomechanical Considerations of the Foot During Gait
The foot serves several important functions.26 It enables propulsion through space, adaptation to uneven terrain, absorption of shock, and support of body weight. The foot forms a rigid lever arm that gives us the ability to push off, primarily from the hallux, during the terminal-stance phase of gait. Terrain adaptability is necessary to walk or run on uneven surfaces.19 Shock absorption refers to dissipation of ground reaction forces. Ground reaction force represents the force generated when the foot contacts the ground; this force is equal but opposite to the force the foot applies to the ground.27 Finally, the foot supports the body's weight in both static and dynamic weight-bearing positions.19
Donatelli6 described the following phases of gait during stance: heel contact, weight acceptance, midstance, push-off and propulsion, and toe-off. The gait cycle begins with the foot in a supinated position at heel strike. The subtalar joint then immediately pronates when going from heel strike to weight acceptance. This period of pronation results in the increased foot mobility needed to absorb ground reaction forces and adapt to uneven terrain.18 The foot reaches maximum pronation at the end of the weight-acceptance phase, and the subtalar joint supinates the foot from midstance through toe-off.26 This supination movement transforms the foot into the rigid lever arm needed for propulsion.
During gait, many forces stress the foot and could disrupt the medial longitudinal arch. Without a mechanism to maintain this arch, we could not walk in a systematic and efficient manner. The orientation of the plantar fascia helps maintain the arch throughout gait and contributes significantly to the appropriate amount and timing of pronation and supination during the gait cycle.
Variations During Gait
Radiographic examination of the foot can describe the changes in the medial longitudinal arch height. The articular facets of the talonavicular and calcaneocuboid joints form a continuous S-shaped curve on lateral radiograph named the Cyma line.28 During pronation, the talus slides anteriorly, forms an anterior break in the Cyma line, and places the talonavicular joint distal to the calcaneocuboid joint. During supination, the talus moves posteriorly into the ankle mortise. This translation forms a posterior break in the Cyma line because the talonavicular joint is now proximal to the calcaneocuboid joint. These radiographic data depict the normal stresses placed on the plantar fascia in the pronated and supinated positions.
These radiographic data also depict the stresses placed on the plantar fascia during gait. From heel strike to weight acceptance, pronation increases the relative distance between the calcaneus and metatarsals and applies a tension stress to the plantar fascia (Figure 3). From midstance through the propulsive phase, supination occurs so that the foot can become a rigid lever arm, using the windlass mechanism, to propel the body forward. Forces generated during supination also apply tension to the plantar fascia, just as in pronation.14,20
Figure 3.

The figure compares the length of the plantar fascia in different foot positions. A, The foot in a supinated (higher-arch) position. B, The foot is in a pronated (lower-arch) position. The ratio of the supination length to the pronation length is 1:1.09.
Forces generated during pronation and supination increase plantar fascia tension. Inefficient foot function can lead to increased tissue stress.4,16 The foot must have a balance between pronation and supination. Too much or too little of either motion at the wrong time of the gait cycle leads to inefficient foot function and potential dysfunction.
Biomechanical Influences on Plantar Fascia Abnormalities
The previous discussion illustrates how the vertical and ground reaction forces stress the plantar fascia tissues. Integral to this discussion is the fact that plantar fascia pain results from excessive traction forces (increased tension) applied to the calcaneus. Fuller20 stated that fascial stretching caused pain either to the plantar fascia itself or at the attachment to the bone. High tension in the fascia could also cause a periosteal lifting at its insertion on the calcaneus, and bone healing could cause growth of a spur that might be seen at the calcaneus. An understanding of this traction stress explains why the bone spur grows in a direction horizontal to the ground. The Wolff law states that mechanical stresses influence and modulate bone growth.29,30 The direction and amount of pull from the fascia on the calcaneus form the bone spur.
Onwuanyi31 noted that plantar heel pain in combination with heel-spur formation occurs in about 50% of patients; however, other researchers doubt the contribution of the heel spur to the condition.13,18 Tountas and Fornasier13 retrospectively reviewed the charts of 20 patients who had undergone resection of the proximal plantar fascia and heel spur. They took radiographic images an average of 40 months after surgery and found that subjects with a re-emergence of the bone spur still reported high functional outcomes. The authors concluded that the intrinsic changes within the plantar fascia rather than the heel spur itself resulted in the condition.
These results support the belief that pain occurs not from the bone spur but from the excessive tension applied to the plantar fascia.4,8 Excessive tension causes tissue irritation to the plantar fascia as well as to its origin at the medial calcaneal tubercle. Clinicians can reproduce this symptom using the windlass test, as described by Brown32 in a weight-bearing position. This test employs forceful great-toe extension with the person standing; a positive test reproduces pain at the medial calcaneal tubercle. Even though researchers33 have reported 100% specificity but only 31.8% sensitivity with this test, clinicians may find it useful in determining plantar-fascial tissue irritation. In summary, the review of the literature provides evidence that plantar fasciitis results from increased plantar fascia tension; therefore, successful management depends on reversing the factors leading to excessive strain.
Bridging Science to Clinical Practice
Abnormalities Resulting From Overpronation
One cause of plantar fasciitis is prolonged foot pronation.3,8,16,17 Patients with pronation problems have a more flexible, lower- arched foot; thus, effective treatment depends on controlling pronation. Factors that contribute to excessive pronation include muscle weakness, heel-cord tightness, and structural foot deformities.4,16
Thordarson et al34 found that the posterior tibialis muscle provided the most significant dynamic arch support during the stance phase of gait. The posterior tibialis eccentrically lengthens to control pronation and reduce the tension applied to the plantar fascia during weight acceptance. Excessive pronation can cause posterior tibialis weakness and plantar fascia elongation. The elongation minimizes efficient use of the foot's windlass mechanism because of instability during the propulsive phase of gait.17,18,35 Alternately, controlled pronation provides for the appropriate timing of supination during gait.
The combined effects of the flexor digitorum longus, flexor hallucis longus, peroneus longus, and Achilles tendons permit the supination needed to enhance the windlass mechanism.34 The peroneus longus courses under the cuboid and attaches to the base of the first ray. Supination from midstance to the propulsive phase transforms the cuboid into a rigid structure that enhances the peroneus longus pulley system.6 This pulley system assists the peroneus longus with first metatarsal plantar flexion.6 Therefore, the plantar flexors enhance supination so that the cuboid pulley system can plantar flex the first ray and promote efficient use of the windlass mechanism.
Proximal muscle weakness from the gluteus medius, gluteus minimus, tensor fascia latae, or quadriceps muscles can contribute to plantar fascia abnormalities. Weakness in these muscles inhibits their ability to assist with the lower extremity load response, which results in greater transmission of shock to the supporting foot structures.8 Furthermore, gluteus medius, gluteus minimus, and tensor fascia latae weakness can accelerate lower extremity pronation.36 In summary, proximal muscle weaknesses can lead to poor shock absorption and decreased pronation control.
The literature reports heel-cord tightness in patients with plantar fasciitis.15 Ankle dorsiflexion is necessary during the gait cycle to allow the body to pass over the foot26; a tight Achilles tendon limits the amount of dorsiflexion available during gait. A person with a flexible foot type can compensate for this lack of ankle dorsiflexion by unlocking the midtarsal joint because dorsiflexion and abduction are movements allowed at the midtarsal joint's oblique axis. This increased motion results in excessive pronation that can stress the plantar fascia.6,8,15
Structural deformities such as an excessive subtalar or forefoot varus can contribute to plantar fascia problems. An excessive forefoot varus is a frontal-plane deformity in which the forefoot is in an inverted position of more than 8° relative to the rearfoot.6,8,37 Johanson et al37 defined a compensated forefoot varus as compensatory subtalar pronation that allows the medial metatarsal heads to contact the weight-bearing surface. In other words, when the heel initially hits the ground, the foot must pronate excessively to allow the forefoot to contact the ground. This excessive pronation stresses the plantar fascia and inhibits efficient use of the windlass mechanism. A subtalar varus deformity of more than 10° can similarly contribute to excessive pronation.38
Treatment Principles Related to Abnormalities Resulting From Overpronation
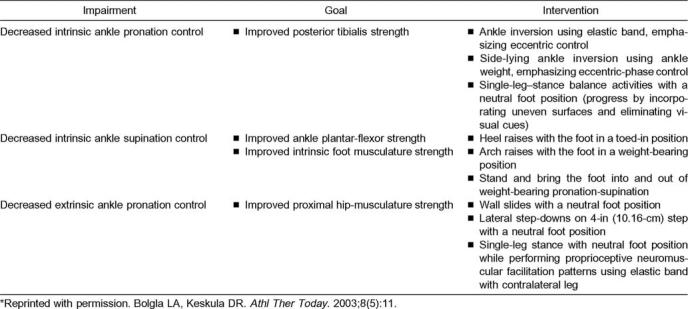
When the cause is mechanical, the rehabilitation plan should use interventions designed to relieve plantar fascia inflammation while correcting mechanical factors.4,9,19 Rehabilitation interventions should focus on restoring normal muscle strength, improving muscle flexibility, and normalizing biomechanical influences. First, strengthening should incorporate all muscles involved with controlling pronation and facilitating the windlass mechanism. The program should strengthen the posterior tibialis, ankle plantar flexors, and peroneus longus muscles as well as the proximal hip and knee musculature. The Table summarizes exercises that effectively strengthen these muscle groups.
Exercises to Control Excessive Pronation*
The rehabilitation program should also include pain-free calf stretching. Worrell et al39 reported increased ankle dorsiflexion after calf stretching regardless of foot position. Patients may perform stretches in a non–weight-bearing position and progress to a more aggressive weight-bearing position. Backstrom and Moore8 also suggested stretching using a contract- relax-contract proprioceptive neuromuscular facilitation method.
Finally, the clinician should consider biomechanical control if the patient has a foot deformity that contributes to excessive pronation. Orthoses are commonly prescribed, and the literature supports the use of medial wedging in controlling pronation.4,37,40 Alternatively, Kogler et al41 measured plantar aponeurosis strain in cadaveric lower limbs using different wedging combinations under the forefoot and hindfoot. They reported that a 6° wedge placed under the lateral aspect of the forefoot demonstrated the greatest reduction in plantar aponeurosis strain. Although these researchers suggested a lateral wedging approach, we believe that further studies should be conducted to determine the effectiveness of lateral wedging in people with plantar fasciitis.
Proper shoe wear is another very important component because a shoe's design can enhance stability.42 Today's market offers motion-control and stability shoes. Features of these shoes include a semicurved outer sole shape with either a slip or combination last (construction of the insole). The shoes should have sufficient toe-box width and forefoot flexibility to enable the midfoot and rearfoot to easily roll over the forefoot.
Motion-control and stability shoes also have a firm heel counter and a firm midsole to control the amount of pronation.4 Polyurethane or a combination of polyurethane and ethylene vinyl acetate is commonly used in midsole construction. Polyurethane is a synthetic rubber material that can enhance shoe support and durability. Ethylene vinyl acetate is a lightweight material that provides cushioning and resiliency against compressive forces. The clinician's choice between either a motion-control or stability shoe generally depends on the degree of pronation control required in relation to the person's size.
Abnormalities Resulting From Underpronation
Plantar fasciitis in the rigid, higher-arched foot (pes cavus) results from the foot's inability to dissipate force.16,19 Effective treatment depends on improving flexibility. Factors that contribute to underpronation include limited joint mobility, decreased plantar fascia extensibility, and increased muscle tightness.
A cavus foot lacks normal joint mobility; it also has limited pronation to dissipate forces.43 Decreased shock absorption results in increased tension forces being applied to the insertion of the plantar fascia at the medial calcaneal tubercle. Kwong et al4 described this increased load to the plantar fascia as a stretch on a bowstring.
Patients with a cavus foot have a decreased distance between the calcaneus and metatarsal heads (Figure 3). People with a cavus foot also have a rigid, plantar-flexed first ray that can further shorten this distance. A plantar-flexed first ray occurs when the first ray has dropped to a relatively plantar- flexed position in comparison with the other rays.8 This position effectively increases the “winding” under the first metatarsal head as described by the windlass model. Therefore, the combination of a high arch and plantar-flexed first ray places a continuous tension on the plantar fascia that can lead to adaptive tissue shortening.
People with a cavus foot also have decreased gastrocnemius, soleus, and Achilles tendon flexibility. Collagen fibers from the Achilles tendon surround the posterior aspect of the calcaneus to blend into the superficial layers of the plantar fascia.14 By virtue of this orientation, ankle dorsiflexion during the gait cycle applies more tension to the plantar fascia. This increased tension leads to inflammation either at the medial calcaneal tubercle or within the plantar fascia itself.
Treatment Principles Related to Abnormalities Resulting From Underpronation
Rehabilitation interventions should focus on improving plantar fascia extensibility, normalizing joint mobility, improving muscle flexibility, and supporting the longitudinal arch. Ultrasound and soft tissue techniques can improve plantar fascia extensibility; joint mobilization techniques can improve first ray and subtalar joint mobility. Together, soft tissue extensibility and improved joint mobility will enhance normal pronation to assist with shock absorption.
Gastrocnemius and soleus muscle stretching is most frequently recommended in the literature.9 Pfeffer et al44 reported a 72% improvement in subjects participating in an 8-week stretching program. This study demonstrates the efficacy of stretching because improved Achilles tendon flexibility decreases the tension applied directly to the plantar fascia.14 Clinicians can also use proprioceptive neuromuscular facilitation techniques to improve flexibility.8
The literature also supports using a night splint to improve flexibility.1,45 Plantar fascia pain is the most severe in the morning.3,9,45 Overnight, the foot is in a prolonged plantar- flexed position. Consequently, the first steps taken in the morning result in pain because of the stretch to the inflamed tissues. The premise of night splints is to keep the foot in a slightly dorsiflexed position to minimize plantar-fascial shortening during sleeping hours.
During waking hours, arch taping is a viable treatment choice. Low-dye taping helps support the foot to optimize ligament and muscle function that can help decrease the tensile forces placed on the plantar fascia.46 Taping is a cost-efficient treatment choice, especially for people having acute symptoms of plantar fascia problems.46,47
Shoe wear is an important treatment consideration. A cushion-type running shoe can provide shock absorption. Features of a cushion shoe include a curved outer sole shape with a slip last. This shoe should allow for mobility in both the rearfoot and forefoot and should not contain features such as a heel counter. Unlike the motion-control or stability shoe, the cushion shoe midsole is commonly made with ethylene vinyl acetate. As mentioned previously, ethylene vinyl acetate is a lightweight material that is resilient against compressive forces and offers much shock absorption. Finally, an accommodative orthosis or silicone heel pad can further enhance shock absorption.8,44
CONCLUSIONS
Plantar fasciitis is a commonly treated foot problem and affects a variety of people with different foot types. Although plantar fasciitis is a prevalent problem, little scientific evidence exists concerning the most appropriate intervention.1 We provide a biomechanical application for the evaluation and treatment of plantar fasciitis based on the windlass mechanism model. This model can describe plantar fascia abnormalities in terms of overpronation and underpronation to help formulate possible relationships between conditions and treatments. Such relationships should guide the decision-making process concerning the evaluation and treatment of heel pain. Use of this approach may improve clinical outcomes because rehabilitation intervention does not merely treat physical symptoms but actively addresses the influences that resulted in the condition. Finally, principles from this approach might provide a basis for future research investigating the efficacy of plantar fascia interventions.
ACKNOWLEDGMENTS
We thank Ruth A. Heubner, PhD, OTR/L, FAOTA, for her assistance in the preparation of this manuscript and editorial input. We also thank Monte Hunter, MD, for his assistance with the radiographs.
REFERENCES
- 1.Crawford F, Atkins D, Edwards J. Interventions for treating plantar heel pain. Foot. 2002;11:228–250. doi: 10.1002/14651858.CD000416. [DOI] [PubMed] [Google Scholar]
- 2.Gudeman SD, Eisele SA, Heidt Jr RS, Colosimo AJ, Stroupe AL. Treatment of plantar fasciitis by iontophoresis of 0.4% dexamethasone: a randomized, double-blind, placebo-controlled study. Am J Sports Med. 1997;25:312–316. doi: 10.1177/036354659702500307. [DOI] [PubMed] [Google Scholar]
- 3.Chandler TJ, Kibler WB. A biomechanical approach to the prevention, treatment and rehabilitation of plantar fasciitis. Sports Med. 1993;15:344–352. doi: 10.2165/00007256-199315050-00006. [DOI] [PubMed] [Google Scholar]
- 4.Kwong PK, Kay D, Voner PT, White MW. Plantar fasciitis: mechanics and pathomechanics of treatment. Clin Sports Med. 1988;7:119–126. [PubMed] [Google Scholar]
- 5.Whiting WC, Zernicke RF. Biomechanics of Musculoskeletal Injury. Champaign, IL: Human Kinetics; 1998. Lower-extremity injuries; pp. 172–173. [Google Scholar]
- 6.Donatelli RA. Abnormal biomechanics. In: Donatelli RA, editor. Biomechanics of the Foot and Ankle. 2nd ed. Philadelphia, PA: FA Davis; 1996. pp. 34–72. [Google Scholar]
- 7.Shama SS, Kominsky SJ, Lemont H. Prevalence of non-painful heel spur and its relation to postural foot position. J Am Podiatry Assoc. 1983;73:122–123. doi: 10.7547/87507315-73-3-122. [DOI] [PubMed] [Google Scholar]
- 8.Backstrom KM, Moore A. Plantar fasciitis. Phys Ther Case Rep. 2000;3:154–162. [Google Scholar]
- 9.Cornwall MW, McPoil TG. Plantar fasciitis: etiology and treatment. J Orthop Sports Phys Ther. 1999;29:756–760. doi: 10.2519/jospt.1999.29.12.756. [DOI] [PubMed] [Google Scholar]
- 10.Donatelli RA, Wooden M, Ekedahl SR, Wilkes JS, Cooper J, Bush AJ. Relationship between static and dynamic foot postures in professional baseball players. J Orthop Sports Phys Ther. 1999;29:316–330. doi: 10.2519/jospt.1999.29.6.316. [DOI] [PubMed] [Google Scholar]
- 11.Reischl SF, Powers CM, Rao S, Perry J. Relationship between foot pronation and rotation of the tibia and femur during walking. Foot Ankle Int. 1999;20:513–520. doi: 10.1177/107110079902000809. [DOI] [PubMed] [Google Scholar]
- 12.Powers CM, Chen PY, Reischl SF, Perry J. Comparison of foot pronation and lower extremity rotation in persons with and without patellofemoral pain. Foot Ankle Int. 2002;23:634–640. doi: 10.1177/107110070202300709. [DOI] [PubMed] [Google Scholar]
- 13.Tountas AA, Fornasier VL. Operative treatment of subcalcaneal pain. Clin Orthop. 1996;332:170–178. doi: 10.1097/00003086-199611000-00023. [DOI] [PubMed] [Google Scholar]
- 14.Viel E, Esnault M. The effect of increased tension in the plantar fascia: a biomechanical analysis. Physiother Pract. 1989;5:69–73. [Google Scholar]
- 15.Rome K, Howe T, Haslock I. Risk factors associated with the development of plantar heel pain in athletes. Foot. 2001;11:119–125. [Google Scholar]
- 16.Cornwall MW. Common pathomechanics of the foot. Athl Ther Today. 2000;5(1):10–16. [Google Scholar]
- 17.Aquino A, Payne C. Function of the plantar fascia. Foot. 1999;9:73–78. [Google Scholar]
- 18.Karr SD. Subcalcaneal heel pain. Orthop Clin North Am. 1994;25:161–175. [PubMed] [Google Scholar]
- 19.Hunter LJ, Fortune J. Foot and ankle biomechanics. S Afr J Physiother. 2000;56:17–20. [Google Scholar]
- 20.Fuller EA. The windlass mechanism of the foot: a mechanical model to explain pathology. J Am Podiatr Med Assoc. 2000;90:35–46. doi: 10.7547/87507315-90-1-35. [DOI] [PubMed] [Google Scholar]
- 21.Hicks JH. The mechanics of the foot, II: the plantar aponeurosis and the arch. J Anat. 1954;88:25–30. [PMC free article] [PubMed] [Google Scholar]
- 22.Kim W, Voloshin AS. Role of plantar fascia in the load bearing capacity of the human foot. J Biomech. 1995;28:1025–1033. doi: 10.1016/0021-9290(94)00163-x. [DOI] [PubMed] [Google Scholar]
- 23.Sarrafian SK. Functional characteristics of the foot and plantar aponeurosis under tibiotalar loading. Foot Ankle. 1987;8:4–18. doi: 10.1177/107110078700800103. [DOI] [PubMed] [Google Scholar]
- 24.Sammarco GJ, Hockenbury RT. Biomechanics of the foot and ankle. In: Nordin M, Frankel VH, editors. Basic Biomechanics of the Musculoskeletal System. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001. pp. 223–255. [Google Scholar]
- 25.Lombardi CM, Silhanek AD, Connolly FG, Dennis LN. The effect of first metatarsophalangeal joint arthrodesis on the first ray and the medial longitudinal arch: a radiographic study. J Foot Ankle Surg. 2002;41:96–103. doi: 10.1016/s1067-2516(02)80032-1. [DOI] [PubMed] [Google Scholar]
- 26.Norkin CC, Levangie PK. Joint Structure and Function. A Comprehensive Analysis. 4th ed. Philadelphia, PA: FA Davis; 2001. [Google Scholar]
- 27.Soutas-Little RW. Motion analysis and biomechanics. In: DeLisa JA, editor. Gait Analysis in the Science of Rehabilitation. Baltimore, MD: Department of Veterans Affairs; 1998. pp. 49–68. [Google Scholar]
- 28.Vito G, Kalish S. Biomechanical radiographic evaluation. In: Donatelli RA, editor. The Biomechanics of the Foot and Ankle. 2nd ed. Philadelphia, PA: FA Davis; 1996. pp. 137–167. [Google Scholar]
- 29.Wolff J. Das Gesetz der Transformation der Knochen. Berlin, Germany: Hirschwald; 1892. [Google Scholar]
- 30.Frankel VH, Nordin M. Biomechanics of bone. In: Nordin M, Frankel VH, editors. Basic Biomechanics of the Musculoskeletal System. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001. p. 51. [Google Scholar]
- 31.Onwuanyi ON. Calcaneal spurs and plantar heel pad pain. Foot. 2000;10:182–185. [Google Scholar]
- 32.Brown C. A review of subcalcaneal heel pain and plantar fasciitis. Aust Fam Physician. 1996;25:875–885. [PubMed] [Google Scholar]
- 33.De Garceau D, Dean D, Requejo SM, Thordarson DB. The association between diagnosis of plantar fasciitis and Windlass test results. Foot Ankle Int. 2003;24:251–255. doi: 10.1177/107110070302400309. [DOI] [PubMed] [Google Scholar]
- 34.Thordarson DB, Schmotzer H, Chon J, Peters J. Dynamic support of the human longitudinal arch: a biomechanical evaluation. Clin Orthop. 1995;316:165–172. [PubMed] [Google Scholar]
- 35.Kappel-Bargas A, Woolf RD, Cornwall MW, McPoil TG. The windlass mechanism during normal walking and passive first metatarsalphalangeal joint extension. Clin Biomech (Bristol, Avon) 1998;13:190–194. doi: 10.1016/s0268-0033(97)00038-7. [DOI] [PubMed] [Google Scholar]
- 36.Sahrmann SA. Diagnosis and Treatment of Movement Impairment Syndromes. St Louis, MO: Mosby; 2002. Movement impairment syndromes at the hip; pp. 121–193. [Google Scholar]
- 37.Johanson MA, Donatelli RA, Wooden MJ, Andrew PD, Cummings GS. Effects of three different posting methods on controlling abnormal subtalar pronation. Phys Ther. 1994;74:149–161. doi: 10.1093/ptj/74.2.149. [DOI] [PubMed] [Google Scholar]
- 38.Hoke BR. Biomechanics of the Foot, Ankle and Lower Extremity. Aiken, SC: Motivations, Inc; 2002. [Google Scholar]
- 39.Worrell TW, McCullough M, Pfeiffer A. Effect of foot position on gastrocnemius/soleus stretching in subjects with normal flexibility. J Orthop Sports Phys Ther. 1994;19:352–356. doi: 10.2519/jospt.1994.19.6.352. [DOI] [PubMed] [Google Scholar]
- 40.Turlik MA, Donatelli TJ, Veremis MG. A comparison of shoe inserts in relieving mechanical heel pain. Foot. 1999;9:84–87. [Google Scholar]
- 41.Kogler GF, Veer FB, Solomonidis SE, Paul JP. The influence of medial and lateral placement of orthotic wedges on loading of the plantar aponeurosis. J Bone Joint Surg Am. 1999;81:1403–1413. doi: 10.2106/00004623-199910000-00005. [DOI] [PubMed] [Google Scholar]
- 42.Wilk BR, Fisher KL, Gutierrez W. Defective running shoes as a contributing factor in plantar fasciitis in a triathlete. J Orthop Sports Phys Ther. 2000;30:21–28. doi: 10.2519/jospt.2000.30.1.21. [DOI] [PubMed] [Google Scholar]
- 43.Nawoczenski DA, Saltzman CL, Cook TM. The effect of foot structure on the three-dimensional kinematic coupling behavior of the leg and rear foot. Phys Ther. 1998;78:404–417. doi: 10.1093/ptj/78.4.404. [DOI] [PubMed] [Google Scholar]
- 44.Pfeffer G, Becchetti P, Deland J, et al. Comparison of custom and prefabricated orthoses in the initial treatment of proximal plantar fasciitis. Foot Ankle Int. 1999;20:214–221. doi: 10.1177/107110079902000402. [DOI] [PubMed] [Google Scholar]
- 45.Rodstein B, Oh-Park M. Hindfoot pain and plantar fasciitis. Phys Med Rehabil. 2001;15:477–487. [Google Scholar]
- 46.Ross A. Foot taping: why, how and when. Available at: www.klm-lab.com/klm_article04.htm. Accessed November 18, 2003. [Google Scholar]
- 47.Lynch DM, Goforth WP, Martin JE, Odom RD, Preece CK, Kotter MW. Conservative treatment of plantar fasciitis. J Am Podiatr Med Assoc. 1998;88:375–380. doi: 10.7547/87507315-88-8-375. [DOI] [PubMed] [Google Scholar]