

Abstract
De Ritis described the ratio between the serum levels of aspartate transaminase (AST) and alanine transaminase (ALT) almost 50 years ago. While initially described as a characteristic of acute viral hepatitis where ALT was usually higher than AST, other authors have subsequently found it useful in alcoholic hepatitis, where AST is usually higher than ALT. These interpretations are far too simplistic however as acute viral hepatitis can have AST greater than ALT, and this can be a sign of fulminant disease, while alcoholic hepatitis can have ALT greater than AST when several days have elapsed since alcohol exposure. The ratio therefore represents the time course and aggressiveness of disease that would be predicted from the relatively short half-life of AST (18 h) compared to ALT (36 h). In chronic viral illnesses such as chronic viral hepatitis and chronic alcoholism as well as non-alcoholic fatty liver disease, an elevated AST/ALT ratio is predictive of long terms complications including fibrosis and cirrhosis. There are methodological issues, particularly whether or not pyridoxal phosphate is used in the transaminase assays, and although this can have specific effects when patient samples are deficient in this vitamin, these method differences generally have mild effects on the usefulness of the assays or the ratio. Ideally laboratories should be using pyridoxal phosphate supplemented assays in alcoholic, elderly and cancer patients who may be pyridoxine deplete. Ideally all laboratories reporting abnormal ALT should also report AST and calculate the De Ritis ratio because it provides useful diagnostic and prognostic information.
Introduction
The ratio of the serum activities of AST and ALT was first described by Fernando De Ritis in 19571 and has been known ever since as the De Ritis ratio. ALT and AST are commonly requested blood tests for liver disease. They are part of the commonly requested ‘Liver Function Test’ (LFT) panel, but rather than assessing functions of the liver, the release of ALT and AST from liver cells to the bloodstream represents hepatocellular damage or death. These enzymes are normally released at a constant rate with their usual levels in health representing the equilibrium between the normal turnover of hepatocytes due to programmed cell death (apoptosis) and the clearance of the enzymes from plasma.
ALT is only present in the hepatocyte cytoplasm whereas AST is present in both the hepatocyte cytoplasm and mitochondria. Cytosolic AST (cAST) and mitochondrial AST (mAST) are true isoenzymes and are immunologically distinct. mAST is the more prevalent isoenzyme with approximately 80% of total AST activity in human liver contributed by mAST.2
The functions of both these transaminases represent important metabolic links between carbohydrate and protein metabolism. ALT is involved in the ‘glucose-alanine cycle’ and interchanges alanine and pyruvate and can regenerate glucose consumed by muscle in the same way that lactate dehydrogenase interchanges lactate and pyruvate in the ‘Cori cycle’ for regeneration of glucose from lactate in anaerobic metabolism (see Figure 1).
Figure 1.
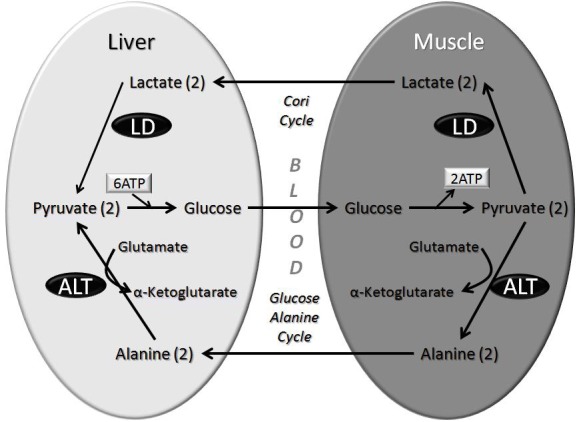
The role of ALT in the glucose-alanine cycle between muscle to liver.
AST is even more vital for aerobic glycolysis by allowing the NADH that has been generated in the cytoplasm to be effectively relocated within the mitochondria through the shuffling of malate (as well as α-ketoglutarate, aspartate and glutamate). While these transaminase reactions are particularly important in the liver and muscle, they are important in all cells with a high metabolc activity and Table 1 lists their relative activities.
Table 1.
Relative activity of transaminases in human tissues.*
| AST Activity | ALT Activity | AST/ALT Ratio | Weight (kg) | AST Total | ALT Total | |
|---|---|---|---|---|---|---|
| Liver | 7,100 | 2,850 | 2.5 | 1.5 | 10,650 | 4,275 |
| Kidney | 4,500 | 1,200 | 3.8 | 0.25 | 1,125 | 300 |
| Heart | 7,800 | 450 | 17 | 0.3 | 2,340 | 135 |
| Muscle | 5,000 | 300 | 17 | 30 | 150,000 | 9,000 |
| Serum | 1 | 1 | 1.0 | 3 | 3 | 3 |
Adapted from King J. Practical Clinical Enzymology, 1965.3
With the hepatic proportion of AST/ALT of 2.5:1, we might expect that hepatocyte turnover should always result in a much higher amount of AST in serum compared to ALT. However, because AST is removed from serum by the liver sinusoids4 twice as quickly (t½=18 h) compared to ALT (t½=36 h), the resulting serum levels of AST and ALT are fairly similar in health where the upper reference limits in apparently healthy reference populations are also similar and approximately 30 IU/L to 40 IU/L for both AST and ALT. Furthermore, in health, circulating AST in blood consists mainly of cAST probably due to the process of cytoplasmic leakage believed to be a process of cytoplasmic budding or blebbing. When hepatocellular death is increased beyond the usual ‘background’ levels, the serum levels of AST compared to ALT will tend to reflect the cellular proportions where AST is over twice as prevalent than ALT.5
The Use of Enzyme Ratios
De Ritis described the AST/ALT ratio as being a useful indicator of the aetiology of hepatitis (e.g. acute viral hepatitis)1 and his work was confirmed and extended by Wroblewski.6 Over the following decades, subsequent studies using improved transaminase methods continued to confirm the original work.7–9
Other enzyme ratios have also been suggested to have similar utility for identification of viral hepatitis such as the ratio of the sum of serum AST+ALT activities divided by the serum glutamate dehydrogenase activity (GDH) as proposed by Schmidt and Schmidt,10,11 and the ratio of GDH to ALT as proposed by Forster et al,12 which is considered to be less reliable.13 Aronsen et al. found that the ratio of ALT to alkaline phosphatase (ALP) activity was better than the individual enzymes but not as good as the ALT to gamma glutamyl transpeptidase (GGT) activity in its ability to differentiate between viral hepatitis and obstructive jaundice.14 The same group also proposed a quotient combining all three enzymes (ALT, GGT and ALP) as a screening test for liver tumours,15 however it is not ALT but GGT that is required to enable liver enzyme ratios to become selective for cholestatic liver disease whereas ALP may be also increased by bone disease.16 Despite all these subsequent proposals, the only enzyme ratio that has stood the test of time and is still widely used is the De Ritis ratio.17
Measurement of Serum Transaminases
The clinical measurement of serum transaminase activity was first described by Karmen et al. in 1954,18 only three years before De Ritis published on the ratio.1 The measurement of serum transaminase activity is relatively new compared to other serum enzymes such as ALP (1930)19 and acid phosphatase (1936).20
Serum contains considerably more immunologically active than catalytically active transaminase enzyme21 and the correlation between the serum concentration of AST protein and AST activity is generally poor.22 One important reason that transaminases may be present but be enzymatically inactive is that both AST and ALT require the cofactor pyridoxal phosphate, or vitamin B6 (B6). The International Federation of Clinical Chemistry (IFCC) recommends that B6 is added to the reagents for both ALT23 and AST24 estimation rather than relying on the concentration of B6 in the patient’s serum. This has been debated however with the Japanese Society of Clinical Chemistry (JSCC) recommending that AST and ALT be measured without addition of B6.25 The omission of B6 from the JSCC method will cause small changes in the AST/ALT ratio.26 Currently, according to participant information from proficiency testing, most laboratories in Australasia are using the ‘modified IFCC method’ which has no B6 added. The most likely reason for laboratories selecting non-B6 supplemented transaminase methods is economical rather than technical or clinical.
The addition of B6 into transaminase reagents generally causes a small increase in the serum AST activity, and to a lesser degree ALT, in healthy persons or patients with liver disease.27 This relative stimulation of AST compared to ALT in chronic liver diseases is typically small resulting in the diagnostic performance of AST, ALT and their ratio not being significantly improved by the addition of B6.28–30 Nevertheless, the effect of B6 addition on AST and ALT activities varies markedly from one patient to another31 and while there may be a small general effect, there may be specific circumstances that argue for the addition of B6.
Alcoholics often have malnutrition, including B6 deficiency, which would translate to decreased transaminase activities.32 The addition of B6 may therefore be of particular importance for patients with alcoholic hepatitis where low serum B6 levels may give falsely low transaminases levels. A higher AST/ALT ratio has been described in alcoholism (qv) which may be influenced by low B6 levels.33,34 However others have shown that correction of B6 deficiency does not significantly alter the high AST/ALT ratio often seen in alcoholic hepatitis.35
Patients being treated for malignancy may also have low B6 levels and underestimated transaminase levels, so using supplemented assays in these patients has been suggested.36 Elderly patients may also be at increased risk of nutritional deficiencies and the addition of B6 generally increases AST and ALT levels in the elderly.37
Isolated Elevation of AST
In liver disease, where AST is markedly elevated but ALT only mildly elevated, B6 deficiency may be sufficient to normalise the mild elevation of ALT, but not enough to normalise the marked elevation of AST. Otherwise an isolated elevation of AST values suggests a non-hepatic source of AST which often occurs artefactually due to release of AST from blood cells such as occurs in sample haemolysis. While isolated elevation of AST could also theoretically be due to a reduction in AST clearance,38 in practice an in vivo isolated elevation of AST is usually due to injury to non-liver cells, particularly cells that contain mitochondria, and therefore is especially indicative of rhabdomyolysis.
Rhabdomyolysis
Release of muscular AST (and to a much lesser extent muscular ALT) can occur with exercise leading to increased serum transaminases.39,40 More severe muscle damage or rhabdomyolysis will cause larger elevations of serum AST (and to a lesser extent ALT), however creatine kinase (CK) is the serum enzyme of choice in estimating the degree of rhabdomyolysis, because the levels of CK in muscle are an order of magnitude higher than the transaminases.41
Because both CK (t½=12 h) and AST (t½=18 h) decline rapidly, and ALT (t½=36 h) declines relatively slowly,42 studies have shown that the AST/ALT ratio, which is high in acute skeletal muscle injury, can fall towards 1:1 after a few days due to the faster decline in AST.43,44 In chronic muscle injury such as polymyositis, the ALT is much the same as the AST45 and this is consistent with the expected faster clearance of AST compared to ALT.46
The persistence of elevated ALT following rhabdomyloysis may also result in the misdiagnosis of hepatitis, such as when hepatitis is attributed to the hepatic effects of anabolic steroids47 rather than the more obvious association of these substances with skeletal muscle dysfunction. Elevated serum ALT levels in the absence of other evidence of liver disease should lead to consideration of chronic or resolving muscle injury.48
Acute Viral Hepatitis
While it is clearly recognised that serum levels of both serum ALT and AST are elevated several fold in ‘acute’ viral hepatitis (e.g. hepatitis A and E), De Ritis was the first to describe that the ALT is usually higher than the AST with the AST/ALT ratio usually well below 1.0, and typically in the range 0.5 to 0.7.49–54 It is important to note that the diagnosis of acute viral hepatitis today (when serology and PCR can clearly diagnose a viral cause) is very different to that question 60 years ago. Nevertheless, even today, when transaminases are elevated several fold, a low De Ritis ratio still provides an important clue to aetiology of acute hepatitis.
Investigators have however noted that acute viral hepatitis can occasionally cause a high AST/ALT ratio of up to 2.0, however these are atypical cases representing fulminant hepatitis where there is often a very poor prognosis. This supports the explanation that the reason that AST/ALT ratio in ‘acute’ viral hepatitis is <1.0 is because the condition is usually resolving when testing occurs. If acute viral hepatitis was not resolving, the AST/ALT ratio will not fall and AST/ALT ratios of 2.0 or greater reflect immediate release of the typical cellular proportions and a potentially fulminant course of acute viral hepatitis. We have recently shown that when ALT is between 200 and 500 U/L and the De Ritis ratio is over 1.5, there is a forty-fold likelihood that the transaminase levels will be over 1000 U/L in a day or two.55 The 95% confidence limits for the AST/ALT ratio in acute viral hepatitis survivors was 0.3–0.6, while in non survivors the AST/ALT ratio was 1.2–2.356. The De Ritis ratio therefore reflects the time course of acute viral hepatitis and is generally a vital clue to the patient’s prognosis.57
Chronic Viral Hepatitis
AST/ALT ratios below 1.0 are also typical of chronic viral hepatitis (e.g. hepatitis B and C), however ratios slightly above 1.0 may be found in chronic viral hepatitis but this is particularly when progression to fibrosis and cirrhosis is present.58–66 In chronic hepatitis B patients without clinical evidence of cirrhosis, the presence of progressive fibrosis might be predicted using an AST/ALT ratio over 1.0 however the ratio does not go above 2.0 in any patient.67 In chronic hepatitis C the raised AST/ALT ratio similarly correlates with fibrosis rather than necroinflammatory activity (e.g. Knodel score).68 The best routine marker of hepatic fibrosis is the De Ritis ratio69 and although a plethora of better markers have been developed, their use is not routine, other than in specialist settings, and as they are beyond the topic of this review, readers are referred to other recent reviews.70–73 In patients with hepatitis C, confirmed fibrosis correlates more closely to AST serum activity (p <0.002) than ALT activity (p <0.03)74 and an increased AST/ALT ratio of over 1.16 is predictive of poor survival as well as correlating with other accepted prognostic scores for liver disease such as the Child-Pugh Test and Model for End Stage Liver Disease (MELD) scores.75,76 A raised AST/ALT ratio of only slightly above 1 (1.09) is predictive of the progression of chronic viral hepatitis C to cirrhosis.77
It is therefore the elevation of AST, rather than ALT, which is predictive of fibrosis and other ratios involving AST, such as the AST to Platelet Ratio Index (APRI)78 and FIB4 index (which involves the four parameters: AST, ALT, platelets and age) are also more predictive.79,80 The reason why the AST is more elevated than ALT with progression of fibrosis is uncertain but may be either because of increased production, such as mitochondrial release,81,82 or a relatively reduced clearance.83
Chronic viral hepatitis may also progress to hepatocellular carcinoma, however GGT is the best predictor of this complication, while AST is not predictive in multivariate analysis and ALT is not predictive at all.84
Alcoholic Hepatitis
The predominance of AST over ALT in alcohol-related liver disease was first reported by Harinasuta et al. in 1967.85 Many authors have since described AST/ALT ratios greater than 1.5 or greater than 2.0 as being highly suggestive of alcoholic hepatitis.86–89 Takahashi et al. described the ratio in alcoholic liver disease as being as high as 5.090, which is not possible given the cellular proportions of AST and ALT and could be explained by concurrent muscle injury (not unusual in alcoholism) or methodological underestimation of ALT activity.
While many of the studies of the De Ritis ratio in alcoholism are over 25 years old and used outdated formulations of the transaminase assays, more recent papers also quote these ratios of over 1.5 or 2.0 as being strongly suggestive or indicative of alcohol abuse.91,92 Most patients with alcoholic liver disease will have AST/ALT ratios below 2.0 and many below 1.0, which could conceivably be because some patients could have coexisting alcoholic as well as viral liver disease.93
The reasons for a classical 2:1 excess of serum AST activity compared to serum ALT activity in alcoholic hepatitis have been attributed to (i) decreased ALT activity94 most likely due to B6 depletion in the livers of alcoholics95 and/or (ii) mitochondrial damage leading to increased release of mAST in serum.96 This is supported by the finding that normally most of the AST activity in serum is the cytosolic isoenzyme,97 however in alcoholism mAST is preferentially released.98 Specificity can be improved using the mAST/AST ratio99 although sensitivity is decreased.100,101
AST/ALT ratios below 1.0 are not uncommon in alcoholic liver disease and in an Australian clinical series of 190 patients with biopsy proven alcoholic cirrhosis one third of patients with cirrhosis exhibited an AST/ALT ratio below 1.0.102 This may be due to a selection bias in this series which exclude patients with clinical evidence of cirrhosis (e.g. portal hypertension or ascites) but could also be due to the AST/ALT data being recorded in connection with liver biopsies which would generally not be performed during an alcoholic binge and when performed in the following period of days the AST/ALT ratio might have declined because of the relatively shorter half-life of AST (18 h) compared to ALT (36 h). This evidence provides a rationale behind why so many patients who consume high amounts of alcohol display elevated serum aminotransferase levels but do not show a high AST/ALT ratio.103 One of the main reasons why acute alcoholic hepatitis has a relatively high AST/ALT ratio is because patients are often tested within 24 h of alcohol exposure so the faster clearance of AST (t½ =18 h) hasn’t had time to take effect. The difference in AST/ALT ratios in viral vs alcoholic liver disease could be partly attributable to disease duration.104 Therefore a likely explanation of 2:1 AST/ALT ratios in alcoholic hepatitis is the dynamics of serum transaminase release and removal. Many patients with chronic alcohol consumption do not have an AST/ALT ratio above 1 but a high AST/ALT ratio is suggestive of either recent exposure or advanced alcoholic liver disease.105 The transaminases alone, or in combination, were not helpful in identifying heavy drinking in the NHANES study106 and others have found that the AST/ALT ratio may fall with increasing consumption.107
Another argument that the association of an AST/ALT ratio of over 2.0 with alcoholic cirrhosis is more to do with recent alcohol exposure rather than cirrhosis per se is the fact that other causes of liver related death such as primary biliary cirrhosis108 and primary sclerosing cholangitis109 are associated with AST/ALT ratios of above 1.0 but not 2.0. Other non-hepatic alcohol related diseases such as oesophageal cancer also have AST/ALT ratios >2.0 as a risk factor.110 Furthermore other acute hepatic toxicities, e.g. paracetamol, can have AST/ALT ratios over 2.0.111 Drug induced hepatitis is typically associated with higher serum AST compared to ALT112 particularly when the drug is known to damage mitochondria.113 Some drugs (e.g. cyproterone) have been described as causing a hepatitis with ALT far greater than AST, suggesting that some drugs may effect the release of cytoplasmic enzymes rather than the more prevalent mitochondrial AST enzyme.114
Fatty Liver
Almost 10% of Americans in the NHANES survey have elevations of ALT and AST115 with fatty liver being one of the most common causes.116,117 Excess alcohol consumption is associated with fatty liver118,119 with more than three drinks per day causing an elevated ALT and AST in both men and women.120 Obesity has a greater impact than moderate or heavy alcohol use121 however when obesity and alcohol are both present they have a multiplicative rather than additive interaction.122 Paradoxically, obesity is the most likely cause of a raised ALT in men123 while alcohol was the more likely cause of an elevated ALT in women.
Studies have suggested an integral role of the cytochrome P450 enzyme ‘CYP2E1’ in the pathogenesis of fatty liver disease due to alcohol and obesity.124 It is well accepted that both diet-induced obesity and increased alcohol consumption lead to induction of CYP2E1 in the liver, which may explain the synergistic effect of these two factors in causing liver injury or elevated serum ALT and AST.125
Non Alcoholic Fatty Liver Diseases (NAFLD)
The prevalence of NAFLD is over 20% in developed countries and nearly 10% in developing nations, making NAFLD the most common liver condition in the world. The pathogenesis of obesity related NAFLD is known to be due to increased de novo hepatic lipogenesis, and the hepatic triglyceride production is increasingly thought to be a consequence of increasing sugar intake.126–131 Dietary ‘sugar’ is invariably composed of both glucose and fructose regardless of whether the source is cane sugar (sucrose) or high fructose corn syrup (HFCS). Dietary glucose can be stored as muscle and liver glycogen under the control of glucose stimulated insulin secretion. The other ‘half’ of common sugar (sucrose or HFCS) is fructose which is solely absorbed by the liver. While the liver could convert fructose to glucose, this is not likely to occur when fructose is virtually always ingested with glucose,132 and obligatory insulin secretion will ensure that hepatic metabolism is directed to convert fructose to triglycerides.133 There are other causes of NAFLD including viral infection, medications, toxins, surgical procedures, total parenteral nutrition and inborn errors of metabolism.
NAFLD refers to the accumulation of fat in the liver beginning as nonalcoholic fatty liver (NAFL) or simple steatosis, progressing to non-alcoholic steatohepatitis (NASH) and then hepatic fibrosis then cirrhosis.134 Although the first stage (NAFL) is typically benign, NASH is a potentially serious condition, since as many as 25% of patients with NASH may progress to cirrhosis and experience complications of portal hypertension, liver failure and hepatocellular carcinoma.135–137
Fatigue, malaise, and vague right upper quadrant abdominal discomfort can antedate the diagnosis of NASH to medical attention in one third of cases however it is generally asymptomatic and frequently identified incidentally by blood liver function tests or abdominal imaging. Sonographic definitions of NAFLD are required because liver biopsy would rarely be considered. Fatty liver defined by presence of at least two of three findings on abdominal ultrasound including (i) diffusely increased echogenicity (a “bright liver” with greater echogenicity than the kidney), (ii) blurring of hepatic vessels and/or (iii) deep attenuation of ultrasound signal.138 Clinically evident hepatomegaly occurs in up to 75% of patients with NAFLD and is even greater (85%) when assessed by ultrasound.
Both serum AST and ALT increase with body weight but this is more prominent for ALT rather than AST.139 Most cases of elevated ALT can be attributed to being overweight (body mass index [BMI] ≥ 25 kg/m2) and obesity (BMI ≥ 30 kg/m2). The five components that compose the metabolic syndrome are central (truncal) obesity, hyperglycaemia, low levels of high-density lipoprotein cholesterol, hypertriglyceridemia, and hypertension. Subjects with specified values for at least three of these components are considered to have metabolic syndrome. All the components of metabolic syndrome are univariate factors associated with elevated ALT. Fasting serum insulin levels and other markers of insulin resistance were associated with elevated ALT independent of BMI and waist circumference. At least 40% of patients with NAFLD fulfil the criteria for metabolic syndrome and subjects with metabolic syndrome are more likely to have elevated ALT.140,141 Whereas in alcoholic steatohepatitis the De Ritis ratio is always over 1.0,142 in patients with NASH the AST/ALT ratio is <1 particularly in morbidly obese patients.143 Not surprisingly, patients with NAFLD have a higher mortality rate than the general population and are at increased risk of developing cardiovascular disease and diabetes in the future.
Increased aminotransferase activities are the most common abnormality reported in patients with NASH, however the true sensitivity and specificity of liver enzyme elevations for detection of NAFLD is unknown because of the interaction between the relatively small increases in ALT (and AST) but the relatively large differences in laboratory reference limits for these serum enzymes. Reference limits have often been derived using reference populations that include high prevalence of obesity in the mistaken reassurance that excluding alcoholism or known chronic liver disease is a sufficient precaution to ensure the reference population does not have liver dysfunction.
While the elevation in ALT in fatty liver may be assumed to be due to liver damage, evidence of liver damage is not always evident.144 There is evidence of increased apoptosis, including caspase activation and cytokeratin 18 breakdown. Cytokeratin-18 fragment levels predict NASH and correlate with severity and both AST and ALT correlate with cytokeratin levels with some investigators also suggesting that transaminase transcription may be increased in fatty liver.145 The AST/ALT ratio however does not correlate with cytokeratin 18.146
When ALT is elevated, the AST/ALT ratio has been described as the best routine marker of insulin resistance, in obese and non-obese adults147 with some authors suggesting that the changes in transaminase levels may precede fatty liver and be caused by increased hepatic transamination of amino acids in the liver especially glutamate.148 Only ALT levels predict the progression to metabolic syndrome149,150 while both ALT and AST predict the progression to diabetes.151
In NASH, fibrosis may be present with normal transaminase levels152 particularly if high transaminase reference limits (>>40 IU/L) are used. It is therefore recommended that patients monitored for progressive liver disease should have their AST and ALT compared to appropriate reference limits as well as having the AST/ALT ratio estimated and reported.153,154 While the AST/ALT ratio is not significantly different across the stages of fibrosis, the ratio may also need to be adjusted for gender.155 An increased AST to ALT ratio in NASH is associated with the development of cirrhosis.156,157
Physiological Determinants of the AST/ALT Ratio
The AST/ALT ratio is typically over 3.0 in a new born infant but should fall by day 5 to below 2.0 and persistent elevation may be due to neonatal asphyxia.158 The AST/ALT ratio often did not fall below 1.5 in children in the poor-outcome group while it usually decreased below 1.5 in children in the good-outcome group. Calculating the AST/ALT ratio appears to be an easy, early, and reliable prognostic indicator for infants with hepatic disease.159
Reference interval studies for AST and ALT have shown that men have higher levels of both of these enzymes. Reference intervals for ALT have been proposed as <30 IU/L for men and <20 IU/L for women.160 While both AST and ALT are higher in men than women, the AST/ALT ratio is higher in women.161 In order to accurately use AST/ALT ratios in the assessment of the aetiology or chronicity of liver disease, the patient’s gender also should be taken into consideration.162 The intra-individual variations of both AST (CVi=13.9%) and ALT (CVi=20.4%) are relatively large and 30% of patients with a mild increase in transaminase level(s) can be reclassified as ‘normal’ on repeat testing,163 however the intraindividual variability of the De Ritis ratio may not necessarily be as large as predicted by the product of the individual variances and further studies are needed in this area.
Conclusion
When medical students are first taught about the clinical value in serum transaminase estimation the name ‘De Ritis’ is usually mentioned but subsequently enzyme ratios are frequently neglected and possibly despised.164 Very few laboratory reports include the De Ritis ratio and there are several reasons that could be proposed for its absence. While simple clinical decision limits have been established for the De Ritis ratio (e.g. >2.0 for alcoholic hepatitis or >1.0 for fibrosis/cirrhosis), there aren’t any generally accepted reference intervals for the ratio and indeed it is difficult to define ‘healthy’ limits for the ratio if its main application is when transaminases are abnormal. We have listed the various limits that have been discussed in this review in Table 2.
Table 2.
Clinical decision limits that can be applied to the De Ritis ratio. Healthy limits are derived from reference 162.
| De Ritis Ratio Decision Limit | ||||
|---|---|---|---|---|
| Condition | <1.0 | 1.0 to <1.5 | 1.5 to <2.0 | ≥ 2.0 |
|
| ||||
| Healthy | Women (up to 1.7) | Children | Neonate | |
| Men (up to 1.3) | ||||
|
| ||||
| Acute Viral Hepatitis | Resolving | Worsening | Fulminant | |
|
| ||||
| Alcoholic Hepatitis | Resolving | Alcohol Abuse | Acute Hepatitis | |
|
| ||||
| Chronic Liver Disease | Stable | Fibrosis risk | Other Causes | |
|
| ||||
| Muscle Disease | Chronic | Resolving | Acute | |
Many laboratories do not include AST as part of the LFT because it is not a liver specific test. For example, it can also be affected by in vitro haemolysis. However in our experience the reason why most laboratories omit AST is economical, which may also be the main reason why laboratories choose non-B6 supplemented transaminase reagents.
We hope that this review provides the evidence that the De Ritis ratio has continued to stand the test of time and remains a useful indicator of liver disease. Its relevance today may be strengthened because of the importance of hepatic diseases such as chronic viral disease and NAFLD. Furthermore serum transaminase estimations are now one of the cheapest laboratory tests available and all laboratory information systems are capable of calculating and comparing simple ratios. Today, patient safety is paramount and practising medicine has also become increasingly litigious, we believe that use of both transaminases and the ratio between them, which has continued to be useful for almost half a century, provides important clinical information which is worth the small additional cost.165
Figure 2.
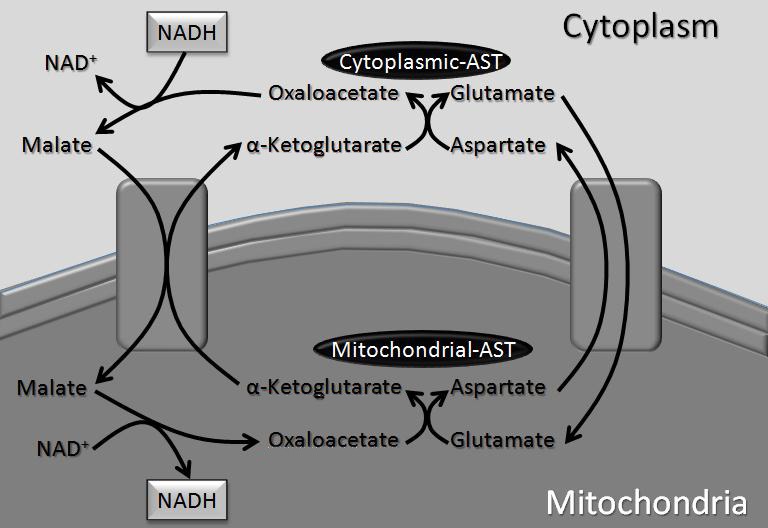
The role of AST in the cytoplasmic-mitochondrial ‘malate shuttle’.
Footnotes
Competing Interests: None declared.
References
- 1.De Ritis F, Coltorti M, Giusti G. An enzymic test for the diagnosis of viral hepatitis; the transaminase serum activities. Clin Chim Acta. 1957;2:70–4. doi: 10.1016/0009-8981(57)90027-x. [DOI] [PubMed] [Google Scholar]
- 2.Rej R. Aspartate aminotransferase activity and isoenzyme proportions in human liver tissues. Clin Chem. 1978;24:1971–9. [PubMed] [Google Scholar]
- 3.King J. Practical Clinical Enzymology. London: D Van Nostrand Company Limited; 1965. [Google Scholar]
- 4.Kamimoto Y, Horiuchi S, Tanase S, Morino Y. Plasma clearance of intravenously injected aspartate aminotransferase isozymes: evidence for preferential uptake by sinusoidal liver cells. Hepatology. 1985;5:367–75. doi: 10.1002/hep.1840050305. [DOI] [PubMed] [Google Scholar]
- 5.Feldstein AE, Canbay A, Angulo P, Taniai M, Burgart LJ, Lindor KD, et al. Hepatocyte apoptosis and fas expression are prominent features of human nonalcoholic steatohepatitis. Gastroenterology. 2003;125:437–43. doi: 10.1016/s0016-5085(03)00907-7. [DOI] [PubMed] [Google Scholar]
- 6.Wroblewski F. The significance of alterations in transaminase activities of serum and other body fluids. Adv Clin Chem. 1958;1:313–51. [PubMed] [Google Scholar]
- 7.Goldberg DM. Enzymes in the diagnosis of myocardial infarction and liver disease. Ann Clin Biochem. 1971;8:195–200. [Google Scholar]
- 8.Goldberg DM. Clinical Enzymology. In: Ellis GP, West GB, editors. Progress in Medicinal Chemistry. Vol. 13. Amsterdam: North Holland; 1976. pp. 1–158. [DOI] [PubMed] [Google Scholar]
- 9.Goldberg DM, Fletcher MJ, Watts C. Serum adenosine deaminase activity in hepatic disease: a comparative enzymological evaluation. Clin Chim Acta. 1966;14:720–8. [Google Scholar]
- 10.Schmidt E, Schmidt FW. [Methods and value of determination of glutamic acid dehydrogenase activity in the serum. A contribution to the importance of examination of enzyme relations in the serum] Klin Wochenschr. 1962;40:962–9. doi: 10.1007/BF01481421. [DOI] [PubMed] [Google Scholar]
- 11.Schmidt E, Schmidt FW. [Enzyme determinations in the serum in liver diseases. Function patterns as a means of diagnosis] Enzymol Biol Clin (Basel) 1963;79:1–52. [PubMed] [Google Scholar]
- 12.Forster G, Filippa G, Landolt M. [The significance of glutamate dehydrogenase for the differential diagnosis of jaundices] Helv Med Acta. 1963;30:672–84. [PubMed] [Google Scholar]
- 13.Konttinen A, Härtel G, Louhija A. Multiple serum enzyme analyses in chronic alcoholics. Acta Med Scand. 1970;188:257–64. doi: 10.1111/j.0954-6820.1970.tb08034.x. [DOI] [PubMed] [Google Scholar]
- 14.Aronsen KF, Hanson A, Nosslin B. The value of gamma glutamyl transpeptidase in differentiating viral hepatitis from obstructive jaundice. A statistical comparison with alkaline phosphatase. Acta Chir Scand. 1965;130:92–9. [PubMed] [Google Scholar]
- 15.Aronsen KF, Nosslin B, Pihl B. The value of gamma-glutamyl transpeptidase as a screen test for liver tumour. Acta Chir Scand. 1970;136:17–22. [PubMed] [Google Scholar]
- 16.Betro MG, Oon RC, Edwards JB. Gamma-glutamyl transpeptidase in diseases of the liver and bone. Am J Clin Pathol. 1973;60:672–8. doi: 10.1093/ajcp/60.5.672. [DOI] [PubMed] [Google Scholar]
- 17.Goldberg DM, Ellis G. Mathematical and computer-assisted procedures in the diagnosis of liver and biliary tract disorders. Adv Clin Chem. 1978;20:49–128. doi: 10.1016/s0065-2423(08)60020-7. [DOI] [PubMed] [Google Scholar]
- 18.Karmen A, Wroblewski F, Ladue JS. Transaminase activity in human blood. J Clin Invest. 1955;34:126–31. doi: 10.1172/JCI103055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kay HD. Plasma phosphatase: method of determination, some properties of the enzyme. J Biol Chem. 1930;89:235–47. [Google Scholar]
- 20.Gutman EB, Sproul EE, Gutman AB. Significance of increased phosphatase activity of bone at the site of osteoplastic metastases secondary to carcinoma of the prostate gland. Am J Cancer. 1936;28:485–95. [Google Scholar]
- 21.Rej R. Immunochemical quantitation of isoenzymes of aspartate aminotransferase and lactate dehydrogenase. Clin Biochem. 1983;16:17–9. doi: 10.1016/s0009-9120(83)94262-5. [DOI] [PubMed] [Google Scholar]
- 22.Hirano K, Matsuda K, Adachi T, Ito Y, Hayashi K, Okuno F, et al. Determination of mitochondrial aspartate aminotransferase in serum. Clin Chim Acta. 1986;155:251–62. doi: 10.1016/0009-8981(86)90245-7. [DOI] [PubMed] [Google Scholar]
- 23.Schumann G, Bonora R, Ceriotti F, Férard G, Ferrero CA, Franck PF, et al. IFCC primary reference procedures for the measurement of catalytic activity concentrations of enzymes at 37 degrees C. International Federation of Clinical Chemistry and Laboratory Medicine. Part 4. Reference procedure for the measurement of catalytic concentration of alanine aminotransferase. Clin Chem Lab Med. 2002;40:718–24. doi: 10.1515/CCLM.2002.124. [DOI] [PubMed] [Google Scholar]
- 24.Schumann G, Bonora R, Ceriotti F, Férard G, Ferrero CA, Franck PF, et al. IFCC primary reference procedures for the measurement of catalytic activity concentrations of enzymes at 37 degrees C. International Federation of Clinical Chemistry and Laboratory Medicine. Part 5. Reference procedure for the measurement of catalytic concentration of aspartate aminotransferase. Clin Chem Lab Med. 2002;40:725–33. doi: 10.1515/CCLM.2002.125. [DOI] [PubMed] [Google Scholar]
- 25.Yoneda K. [Aspartate aminotransferase (glutamic oxalacetic transaminase) and alanine aminotransferase (glutamic pyruvic transaminase)] Rinsho Byori. 2001;(Suppl 116):72–80. [PubMed] [Google Scholar]
- 26.Kotani K, Maekawa M, Kanno T. [Reestimation of aspartate aminotransferase (AST)/alanine aminotransferase (ALT) ratio based on JSCC consensus method—changes of criteria for a differential diagnosis of hepatic disorders following the alteration from Karmen method to JSCC method] Nihon Shokakibyo Gakkai Zasshi. 1994;91:154–61. [PubMed] [Google Scholar]
- 27.Hafkenscheid JC, Dijt CC. Determination of serum aminotransferases: activation by pyridoxal-5′-phosphate in relation to substrate concentration. Clin Chem. 1979;25:55–9. [PubMed] [Google Scholar]
- 28.Jung K, Ohlrich B, Mildner D, Zubek A, Schimmelpfennig W, Egger E. The apoenzyme of aspartate aminotransferase and alanine aminotransferase in the serum of healthy persons and patients suffering from liver diseases. Clin Chim Acta. 1978;90:143–9. doi: 10.1016/0009-8981(78)90515-6. [DOI] [PubMed] [Google Scholar]
- 29.Dols JL, van Zanten AP. Clinical implications of differences between two recommended procedures for determination of aspartate aminotransferase. Clin Chem. 1983;29:523–6. [PubMed] [Google Scholar]
- 30.Vanderlinde RE. Review of pyridoxal phosphate and the transaminases in liver disease. Ann Clin Lab Sci. 1986;16:79–93. [PubMed] [Google Scholar]
- 31.Férard G, Imbert-Bismut F, Messous D, Piton A, Abella A, Burnat P, et al. [Influence of pyridoxal phosphate in measuring aminotransferases activities in patients with viral hepatitis] Ann Biol Clin (Paris) 2004;62:717–20. [PubMed] [Google Scholar]
- 32.Ning M, Baker H, Leevy CM. Reduction of glutamic pyruvic transaminase in pyridoxine deficiency in liver disease. Proc Soc Exp Biol Med. 1966;121:27–30. doi: 10.3181/00379727-121-30687. [DOI] [PubMed] [Google Scholar]
- 33.Matloff DS, Selinger MJ, Kaplan MM. Hepatic transaminase activity in alcoholic liver disease. Gastroenterology. 1980;78:1389–92. [PubMed] [Google Scholar]
- 34.Diehl AM, Potter J, Boitnott J, Van Duyn MA, Herlong HF, Mezey E. Relationship between pyridoxal 5′-phosphate deficiency and aminotransferase levels in alcoholic hepatitis. Gastroenterology. 1984;86:632–6. [PubMed] [Google Scholar]
- 35.McIntyre N, Heathcote J. The laboratory in the diagnosis and management of viral hepatitis. Gastroenterology. 1974;3:317–36. [PubMed] [Google Scholar]
- 36.Mastroianni A, Longoni PD, Franzini C, Facchetti G. Importance of pyridoxal-5′-phosphate addition to the assay medium for the measurement of catalytic concentrations of plasma aspartate and alanine aminotransferases in patients undergoing antineoplastic chemotherapy. Eur J Clin Chem Clin Biochem. 1996;34:507–10. [PubMed] [Google Scholar]
- 37.Succari M, Ponteziere C, Meneguzzer E, Desmoulins D, Amoros-Le Fay A, Miocque M, et al. Aminotransferases in elderly people: influence of pyridoxal 5′-phosphate addition on the determination of serum aminotransferases in healthy elderly subjects. Age Ageing. 1987;16:94–100. doi: 10.1093/ageing/16.1.94. [DOI] [PubMed] [Google Scholar]
- 38.Prati D, Taioli E, Zanella A, Della Torre E, Butelli S, Del Vecchio E, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med. 2002;137:1–10. doi: 10.7326/0003-4819-137-1-200207020-00006. [DOI] [PubMed] [Google Scholar]
- 39.Häkkinen K, Alén M. Training volume, androgen use and serum creatine kinase activity. Br J Sports Med. 1989;23:188–9. doi: 10.1136/bjsm.23.3.188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Koutedakis Y, Raafat A, Sharp NC, Rosmarin MN, Beard MJ, Robbins SW. Serum enzyme activities in individuals with different levels of physical fitness. J Sports Med Phys Fitness. 1993;33:252–7. [PubMed] [Google Scholar]
- 41.Garcin-Webb P, Bhagat CS, Beilby JP. Plasma creatine kinase/aspartate aminotransferase ratio in the diagnosis of acute myocardial infarction. Clin Chem. 1985;31:498–9. [PubMed] [Google Scholar]
- 42.Weibrecht K, Dayno M, Darling C, Bird SB. Liver aminotransferases are elevated with rhabdomyolysis in the absence of significant liver injury. J Med Toxicol. 2010;6:294–300. doi: 10.1007/s13181-010-0075-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Nathwani RA, Pais S, Reynolds TB, Kaplowitz N. Serum alanine aminotransferase in skeletal muscle diseases. Hepatology. 2005;41:380–2. doi: 10.1002/hep.20548. [DOI] [PubMed] [Google Scholar]
- 44.Pettersson J, Hindorf U, Persson P, Bengtsson T, Malmqvist U, Werkström V, et al. Muscular exercise can cause highly pathological liver function tests in healthy men. Br J Clin Pharmacol. 2008;65:253–9. doi: 10.1111/j.1365-2125.2007.03001.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Helfgott SM, Karlson E, Beckman E. Misinterpretation of serum transaminase elevation in “occult” myositis. Am J Med. 1993;95:447–9. doi: 10.1016/0002-9343(93)90319-k. [DOI] [PubMed] [Google Scholar]
- 46.Price CP, Alberti KG. Biochemical assessment of liver function. In: Wright R, Alberti KGMM, Karran S, Millward-Sadler GH, editors. Liver and Biliary Disease-Pathophysiology, Diagnosis and Management. London: W.B. Saunders; 1979. pp. 381–416. [Google Scholar]
- 47.Pertusi R, Dickerman RD, McConathy WJ. Evaluation of aminotransferase elevations in a bodybuilder using anabolic steroids: hepatitis or rhabdomyolysis? J Am Osteopath Assoc. 2001;101:391–4. [PubMed] [Google Scholar]
- 48.Veropalumbo C, Del Giudice E, Esposito G, Maddaluno S, Ruggiero L, Vajro P. Aminotransferases and muscular diseases: a disregarded lesson. Case reports and review of the literature. J Paediatr Child Health. 2012;48:886–90. doi: 10.1111/j.1440-1754.2010.01730.x. [DOI] [PubMed] [Google Scholar]
- 49.De Ritis F, Coltorti M, Giusti G. [Transaminase activity of human serum in viral hepatitis; preventive note] Minerva Med. 1955;46:1207–9. [PubMed] [Google Scholar]
- 50.De Ritis F, Coltorti M, Giusti G. [Transaminase activity of the blood in viral hepatitis] Boll Soc Ital Biol Sper. 1955;31:394–6. [PubMed] [Google Scholar]
- 51.De Ritis F, Coltorti M, Giusti G. [Diagnostic value and pathogenetic significance of transaminase activity changes in viral hepatitis] Minerva Med. 1956;47:167–71. [PubMed] [Google Scholar]
- 52.De Ritis F, Coltorti M, Giusti G. Serum and liver transaminase activities in experimental virus hepatitis in mice. Science. 1956;124:32. doi: 10.1126/science.124.3210.32. [DOI] [PubMed] [Google Scholar]
- 53.De Ritis F, Mallucci L, Coltorti M, Giusti G, Caldera M. Anicteric virus hepatitis in a closed environment as shown by serum transaminase activity. Bull World Health Organ. 1959;20:589–602. [PMC free article] [PubMed] [Google Scholar]
- 54.De Ritis F, Giusti G, Piccinino F, Cacciatore L. Biochemical laboratory tests in viral hepatitis and other hepatic diseases. Bull World Health Organ. 1965;32:59–72. [PMC free article] [PubMed] [Google Scholar]
- 55.Botros M, Sikaris KA, Lu ZX, McNeil A. The short term prognostic usefulness of the De Ritis ratio. Clin Biochem Rev. 2013;34:S18. [PMC free article] [PubMed] [Google Scholar]
- 56.Gitlin N. The serum glutamic oxaloacetic transaminase/serum glutamic pyruvic transaminase ratio as a prognostic index in severe acute viral hepatitis. Am J Gastroenterol. 1982;77:2–4. [PubMed] [Google Scholar]
- 57.Sunheimer R, Capaldo G, Kashanian F, Finck C, Woo J, Korins M, et al. Serum analyte pattern characteristic of fulminant hepatic failure. Ann Clin Lab Sci. 1994;24:101–9. [PubMed] [Google Scholar]
- 58.Williams AL, Hoofnagle JH. Ratio of serum aspartate to alanine aminotransferase in chronic hepatitis; relationship to cirrhosis. Gastroenterology. 1988;95:734–9. doi: 10.1016/s0016-5085(88)80022-2. [DOI] [PubMed] [Google Scholar]
- 59.Cadiot G, Ink O, Boutron A, Hanny P, Laurent-Puig P, Buffet C. Mitochondrial aspartate aminotransferase in nonalcoholic cirrhosis. Gastroenterology. 1989;97:240–1. doi: 10.1016/0016-5085(89)91462-5. [DOI] [PubMed] [Google Scholar]
- 60.Reedy DW, Loo AT, Levine RA. AST/ALT ratio > or = 1 is not diagnostic of cirrhosis in patients with chronic hepatitis C. Dig Dis Sci. 1998;43:2156–9. doi: 10.1023/a:1018888021118. [DOI] [PubMed] [Google Scholar]
- 61.Sheth SG, Flamm SL, Gordon FD, Chopra S. AST/ALT ratio predicts cirrhosis in patients with chronic hepatitis C virus infection. Am J Gastroenterol. 1998;93:44–8. doi: 10.1111/j.1572-0241.1998.044_c.x. [DOI] [PubMed] [Google Scholar]
- 62.Anderson FH, Zeng L, Rock NR, Yoshida EM. An assessment of the clinical utility of serum ALT and AST in chronic hepatitis C. Hepatol Res. 2000;18:63–71. doi: 10.1016/s1386-6346(99)00085-6. [DOI] [PubMed] [Google Scholar]
- 63.Assy N, Minuk GY. Serum aspartate but not alanine aminotransferase levels help to predict the histological features of chronic hepatitis C viral infections in adults. Am J Gastroenterol. 2000;95:1545–50. doi: 10.1111/j.1572-0241.2000.02027.x. [DOI] [PubMed] [Google Scholar]
- 64.Park GJ, Lin BP, Ngu MC, Jones DB, Katelaris PH. Aspartate aminotransferase: alanine aminotransferase ratio in chronic hepatitis C infection: is it a useful predictor of cirrhosis? J Gastroenterol Hepatol. 2000;15:386–90. doi: 10.1046/j.1440-1746.2000.02172.x. [DOI] [PubMed] [Google Scholar]
- 65.Giannini E, Risso D, Testa R. Transportability and reproducibility of the AST/ALT ratio in chronic hepatitis C patients. Am J Gastroenterol. 2001;96:918–9. doi: 10.1111/j.1572-0241.2001.03646.x. [DOI] [PubMed] [Google Scholar]
- 66.Pohl A, Behling C, Oliver D, Kilani M, Monson P, Hassanein T. Serum aminotransferase levels and platelet counts as predictors of degree of fibrosis in chronic hepatitis C virus infection. Am J Gastroenterol. 2001;96:3142–6. doi: 10.1111/j.1572-0241.2001.05268.x. [DOI] [PubMed] [Google Scholar]
- 67.Park SY, Kang KH, Park JH, Lee JH, Cho CM, Tak WY, et al. [Clinical efficacy of AST/ALT ratio and platelet counts as predictors of degree of fibrosis in HBV infected patients without clinically evident liver cirrhosis] Korean J Gastroenterol. 2004;43:246–51. [PubMed] [Google Scholar]
- 68.Ustündag Y, Bilezikçi B, Boyacioğlu S, Kayataş M, Odemir N. The utility of AST/ALT ratio as a non-invasive demonstration of the degree of liver fibrosis in chronic HCV patients on long-term haemodialysis. Nephrol Dial Transplant. 2000;15:1716–7. doi: 10.1093/ndt/15.10.1716. [DOI] [PubMed] [Google Scholar]
- 69.Mardini H, Record C. Detection assessment and monitoring of hepatic fibrosis: biochemistry or biopsy? Ann Clin Biochem. 2005;42:441–7. doi: 10.1258/000456305774538210. [DOI] [PubMed] [Google Scholar]
- 70.Zarski JP, Sturm N, Guechot J, Paris A, Zafrani ES, Asselah T, et al. ANRS HCEP 23 Fibrostar Group Comparison of nine blood tests and transient elastography for liver fibrosis in chronic hepatitis C: the ANRS HCEP-23 study. J Hepatol. 2012;56:55–62. doi: 10.1016/j.jhep.2011.05.024. [DOI] [PubMed] [Google Scholar]
- 71.Crisan D, Radu C, Lupsor M, Sparchez Z, Grigorescu MD, Grigorescu M. Two or more synchronous combination of noninvasive tests to increase accuracy of liver fibrosis assessement in chronic hepatitis C; results from a cohort of 446 patients. Hepat Mon. 2012;12:177–84. doi: 10.5812/hepatmon.853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Stevenson M, Lloyd-Jones M, Morgan MY, Wong R. Non-invasive diagnostic assessment tools for the detection of liver fibrosis in patients with suspected alcohol-related liver disease: a systematic review and economic evaluation. Health Technol Assess. 2012;16:1–174. doi: 10.3310/hta16040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Chou R, Wasson N. Blood tests to diagnose fibrosis or cirrhosis in patients with chronic hepatitis C virus infection: a systematic review. Ann Intern Med. 2013;158:807–20. doi: 10.7326/0003-4819-158-11-201306040-00005. [DOI] [PubMed] [Google Scholar]
- 74.Stránský J, Ryzlová M, Striteský J, Horák J. [Aspartate aminotransferase (AST) more than alanine aminotransferase (ALT) levels predict the progression of liver fibrosis in chronic HCV infection] Vnitr Lek. 2002;48:924–8. [PubMed] [Google Scholar]
- 75.Giannini E, Botta F, Testa E, Romagnoli P, Polegato S, Malfatti F, et al. The 1-year and 3-month prognostic utility of the AST/ALT ratio and model for end-stage liver disease score in patients with viral liver cirrhosis. Am J Gastroenterol. 2002;97:2855–60. doi: 10.1111/j.1572-0241.2002.07053.x. [DOI] [PubMed] [Google Scholar]
- 76.Giannini E, Risso D, Botta F, Chiarbonello B, Fasoli A, Malfatti F, et al. Validity and clinical utility of the aspartate aminotransferase-alanine aminotransferase ratio in assessing disease severity and prognosis in patients with hepatitis C virus-related chronic liver disease. Arch Intern Med. 2003;163:218–24. doi: 10.1001/archinte.163.2.218. [DOI] [PubMed] [Google Scholar]
- 77.Fortunato G, Castaldo G, Oriani G, Cerini R, Intrieri M, Molinaro E, et al. Multivariate discriminant function based on six biochemical markers in blood can predict the cirrhotic evolution of chronic hepatitis. Clin Chem. 2001;47:1696–700. [PubMed] [Google Scholar]
- 78.Wai CT, Greenson JK, Fontana RJ, Kalbfleisch JD, Marrero JA, Conjeevaram HS, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38:518–26. doi: 10.1053/jhep.2003.50346. [DOI] [PubMed] [Google Scholar]
- 79.Mummadi RR, Petersen JR, Xiao SY, Snyder N. Role of simple biomarkers in predicting fibrosis progression in HCV infection. World J Gastroenterol. 2010;16:5710–5. doi: 10.3748/wjg.v16.i45.5710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Poynard T, Ngo Y, Perazzo H, Munteanu M, Lebray P, Moussalli J, et al. Prognostic value of liver fibrosis biomarkers: a meta-analysis. Gastroenterol Hepatol (NY) 2011;7:445–54. [PMC free article] [PubMed] [Google Scholar]
- 81.Okuda M, Li K, Beard MR, Showalter LA, Scholle F, Lemon SM, et al. Mitochondrial injury, oxidative stress, and antioxidant gene expression are induced by hepatitis C virus core protein. Gastroenterology. 2002;122:366–75. doi: 10.1053/gast.2002.30983. [DOI] [PubMed] [Google Scholar]
- 82.Nalpas B, Vassault A, Le Guillou A, Lesgourgues B, Ferry N, Lacour B, et al. Serum activity of mitochondrial aspartate aminotransferase: a sensitive marker of alcoholism with or without alcoholic hepatitis. Hepatology. 1984;4:893–6. doi: 10.1002/hep.1840040517. [DOI] [PubMed] [Google Scholar]
- 83.Kamimoto Y, Horiuchi S, Tanase S, Morino Y. Plasma clearance of intravenously injected aspartate aminotransferase isozymes: evidence for preferential uptake by sinusoidal liver cells. Hepatology. 1985;5:367–75. doi: 10.1002/hep.1840050305. [DOI] [PubMed] [Google Scholar]
- 84.Hann HW, Wan S, Myers RE, Hann RS, Xing J, Chen B, et al. Comprehensive analysis of common serum liver enzymes as prospective predictors of hepatocellular carcinoma in HBV patients. PLoS One. 2012;7:e47687. doi: 10.1371/journal.pone.0047687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Harinasuta U, Chomet B, Ishak K, Zimmerman HJ. Steatonecrosis—Mallory body type. Medicine (Baltimore) 1967;46:141–62. doi: 10.1097/00005792-196703000-00008. [DOI] [PubMed] [Google Scholar]
- 86.Cohen JA, Kaplan MM. The SGOT/SGPT ratio—an indicator of alcoholic liver disease. Dig Dis Sci. 1979;24:835–8. doi: 10.1007/BF01324898. [DOI] [PubMed] [Google Scholar]
- 87.Correia JP, Alves PS, Camilo EA. SGOT-SGPT ratios. Dig Dis Sci. 1981;26:284. doi: 10.1007/BF01391646. [DOI] [PubMed] [Google Scholar]
- 88.Alves PS, Camilo EA, Correia JP. The SGOT/SGPT ratio in alcoholic liver disease. Acta Med Port. 1981;3:255–60. [PubMed] [Google Scholar]
- 89.Salaspuro M. Use of enzymes for the diagnosis of alcohol-related organ damage. Enzyme. 1987;37:87–107. doi: 10.1159/000469243. [DOI] [PubMed] [Google Scholar]
- 90.Takahashi A, Sekiya C, Yazaki Y, Ono M, Sato H, Hasebe C, et al. [Hepatic GOT and GPT activities in patients with various liver diseases—especially alcoholic liver disease] Hokkaido Igaku Zasshi. 1986;61:431–6. [PubMed] [Google Scholar]
- 91.Sharpe PC. Biochemical detection and monitoring of alcohol abuse and abstinence. Ann Clin Biochem. 2001;38:652–64. doi: 10.1258/0004563011901064. [DOI] [PubMed] [Google Scholar]
- 92.Hietala J, Puukka K, Koivisto H, Anttila P, Niemelä O. Serum gamma-glutamyl transferase in alcoholics, moderate drinkers and abstainers: effect on gt reference intervals at population level. Alcohol Alcohol. 2005;40:511–4. doi: 10.1093/alcalc/agh201. [DOI] [PubMed] [Google Scholar]
- 93.Rosman AS, Lieber CS. Diagnostic utility of laboratory tests in alcoholic liver disease. Clin Chem. 1994;40:1641–51. [PubMed] [Google Scholar]
- 94.Matloff DS, Selinger MJ, Kaplan MM. Hepatic transaminase activity in alocholic liver disease. Gastroenterology. 1980;78:1389–92. [PubMed] [Google Scholar]
- 95.Diehl AM, Potter J, Boitnott J, Van Duyn MA, Herlong HF, Mezey E. Relationship between pyridoxal 5′-phosphate deficiency and aminotransferase levels in alcoholic hepatitis. Gastroenterology. 1984;86:632–6. [PubMed] [Google Scholar]
- 96.Nalpas B, Vassault A, Le Guillou A, Lesgourgues B, Ferry N, Lacour B, et al. Serum activity of mitochondrial aspartate aminotransferase: a sensitive marker of alcoholism with or without alcoholic hepatitis. Hepatology. 1984;4:893–6. doi: 10.1002/hep.1840040517. [DOI] [PubMed] [Google Scholar]
- 97.Rej R. Aspartate aminotransferase activity and isoenzyme proportions in human liver tissues. Clin Chem. 1978;24:1971–9. [PubMed] [Google Scholar]
- 98.Ishii H, Okuno F, Shigeta Y, Tsuchiya M. Enhanced serum glutamic oxaloacetic transaminase activity of mitochondrial origin in chronic alcoholics. Curr Alcohol. 1979;5:101–8. [PubMed] [Google Scholar]
- 99.Nalpas B, Vassault A, Charpin S, Lacour B, Berthelot P. Serum mitochondrial aspartate aminotransferase as a marker of chronic alcoholism: diagnostic value and interpretation in a liver unit. Hepatology. 1986;6:608–14. doi: 10.1002/hep.1840060410. [DOI] [PubMed] [Google Scholar]
- 100.Nalpas B, Vassault A, Le Guillou A, Lesgourgues B, Ferry N, Lacour B, et al. Serum activity of mitochondrial aspartate aminotransferase: a sensitive marker of alcoholism with or without alcoholic hepatitis. Hepatology. 1984;4:893–6. doi: 10.1002/hep.1840040517. [DOI] [PubMed] [Google Scholar]
- 101.Okuno F, Ishii H, Kashiwazaki K, Takagi S, Shigeta Y, Arai M, et al. Increase in mitochondrial GOT (m-GOT) activity after chronic alcohol consumption: clinical and experimental observations. Alcohol. 1988;5:49–53. doi: 10.1016/0741-8329(88)90043-2. [DOI] [PubMed] [Google Scholar]
- 102.Hourigan KJ, Bowling FG. Alcoholic liver disease: a clinical series in an Australian private practice. J Gastroenterol Hepatol. 2001;16:1138–43. doi: 10.1046/j.1440-1746.2001.02603.x. [DOI] [PubMed] [Google Scholar]
- 103.Nyblom H, Berggren U, Balldin J, Olsson R. High AST/ALT ratio may indicate advanced alcoholic liver disease rather than heavy drinking. Alcohol Alcohol. 2004;39:336–9. doi: 10.1093/alcalc/agh074. [DOI] [PubMed] [Google Scholar]
- 104.Larsson A, Tryding N. Is it necessary to order aspartate aminotransferase with alanine aminotransferase in clinical practice? Clin Chem. 2001;47:1133–5. [PubMed] [Google Scholar]
- 105.Nyblom H, Berggren U, Balldin J, Olsson R. High AST/ALT ratio may indicate advanced alcoholic liver disease rather than heavy drinking. Alcohol Alcohol. 2004;39:336–9. doi: 10.1093/alcalc/agh074. [DOI] [PubMed] [Google Scholar]
- 106.Liangpunsakul S, Qi R, Crabb DW, Witzmann F. Relationship between alcohol drinking and aspartate aminotransferase:alanine aminotransferase (AST:ALT) ratio, mean corpuscular volume (MCV), gamma-glutamyl transpeptidase (GGT), and apolipoprotein A1 and B in the U.S. population. J Stud Alcohol Drugs. 2010;71:249–52. doi: 10.15288/jsad.2010.71.249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Yue M, Ni Q, Yu CH, Ren KM, Chen WX, Li YM. Transient elevation of hepatic enzymes in volunteers after intake of alcohol. Hepatobiliary Pancreat Dis Int. 2006;5:52–5. [PubMed] [Google Scholar]
- 108.Eriksson LS, Olsson R, Glauman H, Prytz H, Befrits R, Rydén BO, et al. Ursodeoxycholic acid treatment in patients with primary biliary cirrhosis. A Swedish multicentre, double-blind, randomized controlled study. Scand J Gastroenterol. 1997;32:179–86. doi: 10.3109/00365529709000190. [DOI] [PubMed] [Google Scholar]
- 109.Nyblom H, Nordlinder H, Olsson R. High aspartate to alanine aminotransferase ratio is an indicator of cirrhosis and poor outcome in patients with primary sclerosing cholangitis. Liver Int. 2007;27:694–9. doi: 10.1111/j.1478-3231.2007.01471.x. [DOI] [PubMed] [Google Scholar]
- 110.Kimm H, Kim S, Jee SH. The independent effects of cigarette smoking, alcohol consumption, and serum aspartate aminotransferase on the alanine aminotransferase ratio in korean men for the risk for esophageal cancer. Yonsei Med J. 2010;51:310–7. doi: 10.3349/ymj.2010.51.3.310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Himmelstein DU, Woolhandler SJ, Adler RD. Elevated SGOT/SGPT ratio in alcoholic patients with acetaminophen hepatotoxicity. Am J Gastroenterol. 1984;79:718–20. [PubMed] [Google Scholar]
- 112.Miquel M, Soler A, Vaqué A, Ojanguren I, Costa J, Planas R. Suspected cross-hepatotoxicity of flutamide and cyproterone acetate. Liver Int. 2007;27:1144–7. doi: 10.1111/j.1478-3231.2007.01549.x. [DOI] [PubMed] [Google Scholar]
- 113.Kashimshetty R, Desai VG, Kale VM, Lee T, Moland CL, Branham WS, et al. Underlying mitochondrial dysfunction triggers flutamide-induced oxidative liver injury in a mouse model of idiosyncratic drug toxicity. Toxicol Appl Pharmacol. 2009;238:150–9. doi: 10.1016/j.taap.2009.05.007. [DOI] [PubMed] [Google Scholar]
- 114.Hsu YC, Tai DI. Unusually high alanine aminotransferase to aspartate aminotransferase ratio in a patient with cyproterone-induced icteric hepatitis. Chang Gung Med J. 2011;34:34–8. [PubMed] [Google Scholar]
- 115.Clark JM, Brancati FL, Diehl AM. The prevalence and etiology of elevated aminotransferase levels in the United States. Am J Gastroenterol. 2003;98:960–7. doi: 10.1111/j.1572-0241.2003.07486.x. [DOI] [PubMed] [Google Scholar]
- 116.Angulo P. GI epidemiology: nonalcoholic fatty liver disease. Aliment Pharmacol Ther. 2007;25:883–9. doi: 10.1111/j.1365-2036.2007.03246.x. [DOI] [PubMed] [Google Scholar]
- 117.Ioannou GN, Boyko EJ, Lee SP. The prevalence and predictors of elevated serum aminotransferase activity in the United States in 1999–2002. Am J Gastroenterol. 2006;101:76–82. doi: 10.1111/j.1572-0241.2005.00341.x. [DOI] [PubMed] [Google Scholar]
- 118.Fuchs CS, Stampfer MJ, Colditz GA, Giovannucci EL, Manson JE, Kawachi I, et al. Alcohol consumption and mortality among women. N Engl J Med. 1995;332:1245–50. doi: 10.1056/NEJM199505113321901. [DOI] [PubMed] [Google Scholar]
- 119.Jackson R, Beaglehole R. Alcohol consumption guidelines: relative safety vs absolute risks and benefits. Lancet. 1995;346:716. doi: 10.1016/s0140-6736(95)91496-x. [DOI] [PubMed] [Google Scholar]
- 120.Loomba R, Bettencourt R, Barrett-Connor E. Synergistic association between alcohol intake and body mass index with serum alanine and aspartate aminotransferase levels in older adults: the Rancho Bernardo Study. Aliment Pharmacol Ther. 2009;30:1137–49. doi: 10.1111/j.1365-2036.2009.04141.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Adams LA, Knuiman MW, Divitini ML, Olynyk JK. Body mass index is a stronger predictor of alanine aminotransaminase levels than alcohol consumption. J Gastroenterol Hepatol. 2008;23:1089–93. doi: 10.1111/j.1440-1746.2008.05451.x. [DOI] [PubMed] [Google Scholar]
- 122.Park EY, Lim MK, Oh JK, Cho H, Bae MJ, Yun EH, et al. Independent and supra-additive effects of alcohol consumption, cigarette smoking, and metabolic syndrome on the elevation of serum liver enzyme levels. PLoS One. 2013;8:e63439. doi: 10.1371/journal.pone.0063439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Lee DH, Ha MH, Christiani DC. Body weight, alcohol consumption and liver enzyme activity—a 4-year follow-up study. Int J Epidemiol. 2001;30:766–70. doi: 10.1093/ije/30.4.766. [DOI] [PubMed] [Google Scholar]
- 124.Nagata K, Suzuki H, Sakaguchi S. Common pathogenic mechanism in development progression of liver injury caused by non-alcoholic or alcoholic steatohepatitis. J Toxicol Sci. 2007;32:453–68. doi: 10.2131/jts.32.453. [DOI] [PubMed] [Google Scholar]
- 125.Lieber CS. Alcoholic fatty liver: its pathogenesis and mechanism of progression to inflammation and fibrosis. Alcohol. 2004;34:9–19. doi: 10.1016/j.alcohol.2004.07.008. [DOI] [PubMed] [Google Scholar]
- 126.Tappy L, Lê KA. Does fructose consumption contribute to non-alcoholic fatty liver disease? Clin Res Hepatol Gastroenterol. 2012;36:554–60. doi: 10.1016/j.clinre.2012.06.005. [DOI] [PubMed] [Google Scholar]
- 127.Lustig RH, Schmidt LA, Brindis CD. Public health: The toxic truth about sugar. Nature. 2012;482:27–9. doi: 10.1038/482027a. [DOI] [PubMed] [Google Scholar]
- 128.Nomura K, Yamanouchi T. The role of fructose-enriched diets in mechanisms of nonalcoholic fatty liver disease. J Nutr Biochem. 2012;23:203–8. doi: 10.1016/j.jnutbio.2011.09.006. [DOI] [PubMed] [Google Scholar]
- 129.Vos MB, Lavine JE. Dietary fructose in nonalcoholic fatty liver disease. Hepatology. 2013;57:2525–31. doi: 10.1002/hep.26299. [DOI] [PubMed] [Google Scholar]
- 130.Basaranoglu M, Basaranoglu G, Sabuncu T, Sentürk H. Fructose as a key player in the development of fatty liver disease. World J Gastroenterol. 2013;19:1166–72. doi: 10.3748/wjg.v19.i8.1166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Neuschwander-Tetri BA. Carbohydrate intake and nonalcoholic fatty liver disease. Curr Opin Clin Nutr Metab Care. 2013;16:446–52. doi: 10.1097/MCO.0b013e328361c4d1. [DOI] [PubMed] [Google Scholar]
- 132.Coss-Bu JA, Sunehag AL, Haymond MW. Contribution of galactose and fructose to glucose homeostasis. Metabolism. 2009;58:1050–8. doi: 10.1016/j.metabol.2009.02.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Stanhope KL, Schwarz JM, Havel PJ. Adverse metabolic effects of dietary fructose: results from the recent epidemiological, clinical, and mechanistic studies. Curr Opin Lipidol. 2013;24:198–206. doi: 10.1097/MOL.0b013e3283613bca. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Brunt EM, Janney CG, Di Bisceglie AM, Neuschwander-Tetri BA, Bacon BR. Nonalcoholic steatohepatitis: a proposal for grading and staging the histological lesions. Am J Gastroenterol. 1999;94:2467–74. doi: 10.1111/j.1572-0241.1999.01377.x. [DOI] [PubMed] [Google Scholar]
- 135.Adams LA, Lymp JF, St Sauver J, Sanderson SO, Lindor KD, Feldstein A, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology. 2005;129:113–21. doi: 10.1053/j.gastro.2005.04.014. [DOI] [PubMed] [Google Scholar]
- 136.Ekstedt M, Franzén LE, Mathiesen UL, Thorelius L, Holmqvist M, Bodemar G, et al. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology. 2006;44:865–73. doi: 10.1002/hep.21327. [DOI] [PubMed] [Google Scholar]
- 137.Matteoni CA, Younossi ZM, Gramlich T, Boparai N, Liu YC, McCullough AJ. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology. 1999;116:1413–9. doi: 10.1016/s0016-5085(99)70506-8. [DOI] [PubMed] [Google Scholar]
- 138.Yajima Y, Ohta K, Narui T, Abe R, Suzuki H, Ohtsuki M. Ultrasonographical diagnosis of fatty liver: significance of the liver-kidney contrast. Tohoku J Exp Med. 1983;139:43–50. doi: 10.1620/tjem.139.43. [DOI] [PubMed] [Google Scholar]
- 139.Siest G, Schiele F, Galteau MM, Panek E, Steinmetz J, Fagnani F, et al. Aspartate aminotransferase and alanine aminotransferase activities in plasma: statistical distributions, individual variations, and reference values. Clin Chem. 1975;21:1077–87. [PubMed] [Google Scholar]
- 140.Ruhl CE, Everhart JE. Determinants of the association of overweight with elevated serum alanine aminotransferase activity in the United States. Gastroenterology. 2003;124:71–9. doi: 10.1053/gast.2003.50004. [DOI] [PubMed] [Google Scholar]
- 141.Ioannou GN, Boyko EJ, Lee SP. The prevalence and predictors of elevated serum aminotransferase activity in the United States in 1999–2002. Am J Gastroenterol. 2006;101:76–82. doi: 10.1111/j.1572-0241.2005.00341.x. [DOI] [PubMed] [Google Scholar]
- 142.Zamin JI, de Mattos AA, Perin C, Ramos GZ. [The importance of AST / ALT rate in nonalcoholic steatohepatitis diagnosis] Arq Gastroenterol. 2002;39:22–6. doi: 10.1590/s0004-28032002000100005. [DOI] [PubMed] [Google Scholar]
- 143.Nanji AA, French SW, Freeman JB. Serum alanine aminotransferase to aspartate aminotransferase ratio and degree of fatty liver in morbidly obese patients. Enzyme. 1986;36:266–9. doi: 10.1159/000469304. [DOI] [PubMed] [Google Scholar]
- 144.Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N Engl J Med. 2000;342:1266–71. doi: 10.1056/NEJM200004273421707. [DOI] [PubMed] [Google Scholar]
- 145.Josekutty J, Iqbal J, Iwawaki T, Kohno K, Hussain MM. Microsomal triglyceride transfer protein inhibition induces endoplasmic reticulum stress and increases gene transcription via Ire1α/cJun to enhance plasma ALT/AST. J Biol Chem. 2013;288:14372–83. doi: 10.1074/jbc.M113.459602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Feldstein AE, Wieckowska A, Lopez AR, Liu YC, Zein NN, McCullough AJ. Cytokeratin-18 fragment levels as noninvasive biomarkers for nonalcoholic steatohepatitis: a multicenter validation study. Hepatology. 2009;50:1072–8. doi: 10.1002/hep.23050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Kawamoto R, Kohara K, Kusunoki T, Tabara Y, Abe M, Miki T. Alanine aminotransferase/aspartate aminotransferase ratio is the best surrogate marker for insulin resistance in non-obese Japanese adults. Cardiovasc Diabetol. 2012;11:117. doi: 10.1186/1475-2840-11-117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Sookoian S, Pirola CJ. Alanine and aspartate aminotransferase and glutamine-cycling pathway: their roles in pathogenesis of metabolic syndrome. World J Gastroenterol. 2012;18:3775–81. doi: 10.3748/wjg.v18.i29.3775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Khedmat H, Fallahian F, Abolghasemi H, Hajibeigi B, Attarchi Z, Alaeddini F, et al. Serum γ-glutamyltransferase, alanine aminotransferase, and aspartate aminotransferase activity in Iranian healthy blood donor men. World J Gastroenterol. 2007;13:889–94. doi: 10.3748/wjg.v13.i6.889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Hsu CH, Wang JY, Chen YL, Liu CC, Chang YL, Chen HS, et al. Relationships between alanine aminotransferase levels, abnormal liver echogenicity, and metabolic syndrome. J Am Board Fam Med. 2011;24:407–14. doi: 10.3122/jabfm.2011.04.100267. [DOI] [PubMed] [Google Scholar]
- 151.Goessling W, Massaro JM, Vasan RS, D’Agostino RB, Sr, Ellison RC, Fox CS. Aminotransferase levels and 20-year risk of metabolic syndrome, diabetes, and cardiovascular disease. Gastroenterology. 2008;135:1935–44. doi: 10.1053/j.gastro.2008.09.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Uslusoy HS, Nak SG, Gülten M, Bıyıklı Z. Non-alcoholic steatohepatitis with normal aminotransferase values. World J Gastroenterol. 2009;15:1863–8. doi: 10.3748/wjg.15.1863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Mardini H, Record C. Detection assessment and monitoring of hepatic fibrosis: biochemistry or biopsy? Ann Clin Biochem. 2005;42:441–7. doi: 10.1258/000456305774538210. [DOI] [PubMed] [Google Scholar]
- 154.Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB. Diagnosis and monitoring of hepatic injury. II. Recommendations for use of laboratory tests in screening, diagnosis, and monitoring. Clin Chem. 2000;46:2050–68. doi: 10.1093/clinchem/46.12.2050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Lin CS, Chang CS, Yang SS, Yeh HZ, Lin CW. Retrospective evaluation of serum markers APRI and AST/ALT for assessing liver fibrosis and cirrhosis in chronic hepatitis B and C patients with hepatocellular carcinoma. Intern Med. 2008;47:569–75. doi: 10.2169/internalmedicine.47.0595. [DOI] [PubMed] [Google Scholar]
- 156.Sorbi D, Boynton J, Lindor KD. The ratio of aspartate aminotransferase to alanine aminotransferase: potential value in differentiating nonalcoholic steatohepatitis from alcoholic liver disease. Am J Gastroenterol. 1999;94:1018–22. doi: 10.1111/j.1572-0241.1999.01006.x. [DOI] [PubMed] [Google Scholar]
- 157.Neuschwander-Tetri BA, Clark JM, Bass NM, Van Natta ML, Unalp-Arida A, Tonascia J, et al. NASH Clinical Research Network Clinical, laboratory and histological associations in adults with nonalcoholic fatty liver disease. Hepatology. 2010;52:913–24. doi: 10.1002/hep.23784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158.Brucknerová I, Benedeková M, Holomán K, Bieliková E, Kostrová A, Ujházy E, et al. Delivery as “physiological stress” and its influence on liver enzymatic systems in asphyxial newborns. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2005;149:409–11. [PubMed] [Google Scholar]
- 159.Rosenthal P, Haight M. Aminotransferase as a prognostic index in infants with liver disease. Clin Chem. 1990;36:346–8. [PubMed] [Google Scholar]
- 160.Prati D, Taioli E, Zanella A, Della Torre E, Butelli S, Del Vecchio E, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med. 2002;137:1–10. doi: 10.7326/0003-4819-137-1-200207020-00006. [DOI] [PubMed] [Google Scholar]
- 161.Parise ER, Oliveira AC, Figueiredo-Mendes C, Lanzoni V, Martins J, Nader H, et al. Noninvasive serum markers in the diagnosis of structural liver damage in chronic hepatitis C virus infection. Liver Int. 2006;26:1095–9. doi: 10.1111/j.1478-3231.2006.01356.x. [DOI] [PubMed] [Google Scholar]
- 162.Mera JR, Dickson B, Feldman M. Influence of gender on the ratio of serum aspartate aminotransferase (AST) to alanine aminotransferase (ALT) in patients with and without hyperbilirubinemia. Dig Dis Sci. 2008;53:799–802. doi: 10.1007/s10620-007-9924-z. [DOI] [PubMed] [Google Scholar]
- 163.Lazo M, Selvin E, Clark JM. Brief communication: clinical implications of short-term variability in liver function test results. Ann Intern Med. 2008;148:348–52. doi: 10.7326/0003-4819-148-5-200803040-00005. [DOI] [PubMed] [Google Scholar]
- 164.Schmidt E, Schmidt FW, Chemnitz G, Kubale R, Lobers J. The Szasz-ratio (CK/GOT) as example for the diagnostic significance of enzyme ratios in serum. Klin Wochenschr. 1980;58:709–18. doi: 10.1007/BF01478458. [DOI] [PubMed] [Google Scholar]
- 165.Dufour DR. Is it necessary to order aspartate aminotransferase with alanine aminotransferase in clinical practice? Author’s Reply. Clin Chem. 2001;47:1134–5. [PubMed] [Google Scholar]