

Abstract
Background:
Interprofessional teamwork is considered as the key to improve the quality of patient management in critical settings such as trauma emergency departments, but it is not fully conceptualized in these areas to guide practice. The aim of this article is to explore interprofessional teamwork and its improvement strategies in trauma emergency departments.
Materials and Methods:
Participants of this qualitative study consisted of 11 nurses and 6 supervisors recruited from the emergency departments of a newly established trauma center using purposive sampling. Data were generated using two focus group and six in-depth individual interviews, and analyzed using qualitative content analysis.
Results:
Interprofessional teamwork attributes and improvement strategies were emerged in three main themes related to team, context, and goal. These were categorized as the effective presence of team members, role definition in team framework, managerial and physical context, effective patient management, and overcoming competing goals
Conclusions:
Interprofessional teamwork in trauma emergency departments is explained as interdependence of team, context, and goal; so, it may be improved by strengthening these themes. The findings also provide a basis to evaluate, teach, and do research on teamwork.
Keywords: Emergency hospital services, interprofessional relations, Iran, nurse, patient care team, physician–nurse relations, qualitative research, quality improvement, trauma centers
INTRODUCTION
The emergency care of traumatic patients requires effective participation of different professionals and specialists, so interprofessional teamwork (briefly called teamwork here) is considered crucial in critical settings such as trauma emergency departments (trauma EDs).[1] Improvements in clinical parameters such as time saving after teamwork training in trauma EDs[2,3] and error reduction in emergency settings[4,5] were reported. In addition, teamwork is suggested as the possible solution for dilemmas of service delay in EDs.[6,7]
Few studies have explored interprofessional teamwork in trauma EDs. A team error analysis in trauma resuscitation identified four error types including interpretation, communication, management, and concurrency errors.[8] In a literature review, teamwork behaviors in intensive care units were categorized as team communication, leadership, coordination, and decision making.[9]
Teamwork improvement efforts need an empirical knowledge of teamwork attributes and underpinning features that help or impede its improvement. The current evidence lacks such knowledge, especially in trauma EDs. Teamwork practice may be different in various care settings, so studies in different cultures and settings of healthcare system are important. Considering the importance of teamwork in improving the quality of care, the fact that the lack of teamwork may be attributed to some adverse events,[10] and the personal experience of the authors in EDs, the current study was conducted to explore interprofessional teamwork and its improvement strategies in EDs of a newly established trauma emergency center.
MATERIALS AND METHODS
This qualitative study was conducted in 2011 in the EDs of a level 1 trauma center established from 2008. The EDs in this study consist of three wards including triage area, resuscitation room, and ED 1 that admits patients with non-critical or moderate traumas from the triage area.
The participants were recruited using purposive sampling among nurses and supervisors who had at least 1 year experience in trauma ED. Data were generated from two focus group interviews with 11 nurses and 5 supervisors, separately, and six in-depth individual interviews with 4 nurses and 2 supervisors, two before and four after the focus groups to clarify the previous focus groups’ data. Interviews began with a general question such as “Would you explain a situation in which you experienced teamwork in trauma ED?” and proceeded with probing questions to clarify the information and provide rich data. Each interview lasted about 20-108 min. Data generation continued until data were saturated. The participants also completed a brief demographic profile. Interviews were voice-recorded, transcribed verbatim, carefully read through, and data analysis was carried out using qualitative content analysis. Consequently, the codes, categories, and themes were emerged. Trustworthiness of credibility and dependability was assured by prolonged engagement with participants and data(researchers having experience in trauma emergencies and about 1 year presence in the study setting prior to and during data collection, and data immersion), member checking by five participants, triangulation of focus group and individual interviews, and peer checking by two experienced qualitative researchers.
Ethics committee approval and permission from hospital's director and authorities were obtained. The participants were also given an explanation of the study and were informed that their participation was voluntary and that they could withdraw from the study at any time. Informed consent was obtained from all the participants; confidentiality and data protection were assured.
RESULTS
A total of 18 participants (12 nurses and 6 supervisors) with a mean age of 29.714 (25-40) years, nursing experience of 6.72 (1-19) years, and trauma ED experience of 3.5 (1-12) years were interviewed
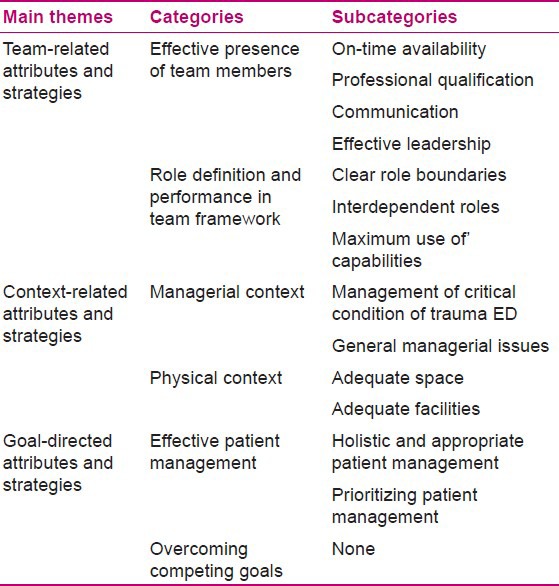
Teamwork attributes and improvement strategies were emerged in three main themes including: team-related, context–related, and goal-directed attributes and strategies [Table 1]
Table 1.
Themes, categories, and subcategories
Team-related attributes and strategies
This theme includes attributes and strategies related to team members’ and leader's traits, functions, competencies, etc. [Table 1].
Effective presence of team members
An important aspect of teamwork was prompt and effective presence of team members and auxiliary personnel (e.g. messenger). The following statements by a participant reflect the effective presence of a physician:
“One night a patient was transferred from the county to resuscitation room with neurosurgery admission. The patient had respiratory problem and needed chest tube insertion. The neurosurgery resident suspected the need for operation, so he didn’t leave the scene and waited until completion of the procedure. He came with the patient to CT scan department, and then to OR and operated the patient. Consequently, the patient didn’t encounter any delay and there was no need for us to find someone to visit the patient.” (Nurse 6)
An important obstacle to teamwork in trauma ED was inappropriate ratio of workforce to workload and some team members’ absence occasionally due to multiplicity of tasks. Examples are physicians busy in the operating room, or nurses involved in the care of other critically patients or accompanying other patients to radiology.
“… For example, if we have two nurses in a ward and 40 patients come in, the only thing you don’t think is teamwork; In my opinion, the only thing you think is to manage the situation … In our hospital, the number of nurses is low and the number of work shifts is high; they are tired and sometimes don’t find a time to have their dinner….” (Supervisor 1)
The two recommended solutions were using the services of nurses working in other wards with lower workload or on-call nurses from the same ward who were ready to cooperate with trauma ED if the ward was busy. But previous experiences of the participants indicated the problems with nurses of the other wards:
“… When we send nurses from other wards to resuscitation or screening room, they are not effective even if they are good nurses because they are not oriented to the ward environment, patients, the work to be done.” (Supervisor 5)
Dissatisfaction of both nurses in the original ward and nurses from other wards was also reported. Preparing specific nurses to help ED nurses in crowded times, increasing the number of nurses, anticipating occasions of absence of team members and taking action accordingly, and defining feasible tasks and workload were the other suggested solutions.
Other attributes and strategies that improve the effectiveness of the team are related to team members’ qualification (including competency, accountability, commitment, and conscience), effective leadership, feeling of autonomy, and communication style. Competency implies that team members possess the necessary knowledge, skills, innovation, ability to cope with the situation, and experience in trauma ED:
“A disoriented nurse couldn’t do any work because even if his/her job description is defined, he/she doesn’t know what to do. In EDs, those nurses should be recruited who are completely oriented. Disoriented nurses haven’t any efficiency in EDs; they are obstacles to others and cause interruption.” (Supervisor 3)
Effective leadership is related to leader's attributes, role performance, and presence. Leader's attributes were described as power, technical and managerial skills, and being influential. The main identified leader roles were to make decisions, prioritize, coordinate, supervise, and follow the patient management. For instance:
“In fact, general surgery residents are the leaders, but some have the potential to fallow up and some don’t. Some don’t consider that the neurosurgeon has visited the patient or not … even if the patient is stable from general surgery, they must consider that the CT scan is seen, laboratory tests are done or not, etc.” (Nurse 6)
Occasions when the team leader was absent were reported leading to difficulties such as ambiguity in decisions, disorganization, and interpersonal conflict.
Autonomy means each party has boundaries of authorization. Examples of intrusion of autonomy are given below:
“The physician says do venous access in this way, do it faster, do this procedure yourself (not others)….” (Nurse 1)
Communication style is related to collaboration, coordination, empathy, rapport, respect, and calming the climate. The participants described collaboration as an essential concept of teamwork or even defined teamwork as collaboration:
«Teamwork means a general collaboration between physician, nurse, messenger, and other systems such as radiology and laboratory to promote patient care.” (Nurse 2)
Also, coordination was considered an important component of teamwork. However, instances of inconsistency in prioritization of actions and writing orders among specialties were reported.
Calming the climate was considered important in critical condition of trauma EDs. Nurses complained that some physicians force them to hurry, which provokes stress, enhances the rate of their injury (needle sticks, etc.), and eventually disturbs teamwork.
Lack of respect, empathy, and rapport was also interpreted as hindrance to teamwork. Some nurses complained about the physicians’ and supervisors’ lack of understanding their workload. One complaint was that some physicians expect them to do multiple actions simultaneously without apprehending the fact that doing is more difficult and time consuming than ordering. They believed that some physicians underestimate their paper work and some think a nurse who is sitting in the nursing station is inactive, etc.
Measures such as recruitment of competent team members, continual training, encouraging negotiation and consensus on the plan of care, interaction and counseling, continuity in the leader's presence, and preparing leaders for their roles were recommended.
Team members’ roles
Role definition and performance in team framework was the second category of the measures to improve team-related attributes [Table 1]. It means that team roles should be defined so that role boundaries are clear, roles are interdependent and complementary to each other, and maximum use of team capabilities is possible. Some instances are:
“… Doing arterial blood gas is the physicians’ duty, but it is done by nurses. Writing radiology request is also the physicians’ duty, but in our EDs nurses do all of these….” (Supervisor 4)
“If nurses only do their own work, we don’t see them in the nursing station so much.” (Supervisor 5)
“Since the scribe nurse was employed in resuscitation room, work condition is much better because other nurses don’t work with patients’ chart; they feel tranquil because they only do patient care.” (Nurse 1)
Context-related attributes and strategies
This theme is related to managerial and physical context [Table 1]
Managerial context
Some measures are directed to manage critical conditions of trauma EDs, including plans to deal with critical condition of trauma EDs and workplace security. Some conditions had been experienced frequently in trauma EDs. These include stressful climate, fluctuation in workload according to daytime or season, high turnover, high number of patients in EDs and post-ED wards, simultaneous arrival of multiple patients that may prevent comprehensive care, etc. Preparation for these conditions through planning to manage trauma EDs in crowded times and otherwise, defining standard timing of actions especially in resuscitation room (such as visit by neurosurgeon, etc.), and development of challenge resolution and alternative plans were extracted from the participants’ statements.
“It is not defined that how many nurses and physicians are needed for an intubated patient or a patient in critical condition. It is expected that two nurses cover the resuscitation room, no difference if the number of patients is one or ten….” (Nurse 6)
Lack of workplace security was a concern that distracts the team from patient care:
“Nurses are worried about insecurity. Few nights ago, two patients in ED were fighting; one of them threw a chair, removed his venous line and blood spread in the ward floor…. I think when there is no security, the efficiency of our work could be affected.” (Supervisor1)
They recommended ensuring security by strengthening hospital security services and development of employees’ bill of rights.
Other solutions in this category are about general managerial actions such as appropriate supervision and evaluation systems, providing motivation and support, and ensuring system integrity. Improving motivation through internal motivators (recognition, psychological support, fair accountability, power, professional status, and responsibility) and external motivators (financial support, welfare facilities, and fair payments) was addressed. An example of fair accountability and power is:
“… The physician says: I will visit the patient 20 minutes later. Now if the patient encounters a problem, the administrators will tell me, ‘you should follow!’” (Nurse 6)
The participants argued that an integral system should be more influential than individuals, so that an individual, whether a nurse or a physician, could not violate the systems’ laws. Other threats to the system's integrity, especially in newly established systems, were frequent changes in protocols (some called it trial and error) and inadequate notifications that may also affect teamwork.
Assertive feedback and other measures to guarantee implementation of the rules and regulations, establishment of an effective notification system to inform all the team members and auxiliary personnel, and rational stability and flexibility of the protocols were suggested to ensure the system's integrity.
Physical context
Preparing sufficient physical space and equipment such as adequate monitoring devices was identified to facilitate teamwork in a trauma ED.
Goal-directed attributes and strategies
This theme comprises team goals and efforts promoting team activities toward them [Table 1].
Effective patient management
Patient management which is holistic, prompt, and appropriate, and prioritizes the patients was considered an important team goal. Considering the patient as a whole and preventing the ignorance of some parts was reflected in the participants’ experiences. They expressed some cases of inattention to holistic care, such as disregarding problems related to other specialties or the importance of comprehensive patient assessment resulting in undetected patients’ problems, etc.
Overcoming competing goals
Some competing goals such as task orientation, preferring routine work, indolence, and competition for position were found to impede moving toward the main goals. Task orientation means focusing on tasks more than patients. It was reflected in instances of nurses’ more attention to paperwork than direct patient care, or physicians’ intention to visit patients not attentively, etc. For instance, one participant in arguing about the statement, “the works are done routinely,” that was stated in focus group, said:
“The reason is that workload is high and everyone wants to do his/her work faster and faster, because nurses in the next shift do not pay attention whether you had 2 or 10 patients. You must do everything completely and sound.” (Nurse 4)
Finally, the participants recommended directing all team activities toward the main goals while being aware of competing goals.
DISCUSSION
The findings suggest that in a trauma ED, a set of defined attributes related to team, context, and goal are interdependent to form interprofessional teamwork; so, all efforts to improve it should be directed toward these attributes. Strategies to strengthen the team through training, ensuring appropriate number and qualification of team members, role description in team framework, fortifying context through enriching physical environment and facilities, improving managerial climate, and reinforcing goals by directing team activities toward comprehensive, prompt, and appropriate patient management by prioritizing the patients and overcoming competing goals were recommended accordingly. Plans to deal with critical conditions of trauma EDs may also be introduced in the EDs’ practice guideline. The main identified teamwork obstacles were workforce shortage, frequent changes, fatigue, and lack of competency, motivation, assertiveness, and information sharing system.
Previous studies reported findings somehow similar to the current study. For instance, nurses in a trauma ED complained stress and frustration due to request for equipment and procedures by senior physicians without considering its feasibility. They described other concerns about teamwork as confusion about leadership and lack of consistency in managerial styles of different physicians. Nurses with little trauma experience also reported feelings of lack of support and clarity about their roles in the trauma team.[11] These are parallel with rapport, support, role clarity, and coordination of this study. Similarly, effectiveness of clinical expertise and coordination,[12] positive and negative effects of the practitioners’ role, education and training, and cultural perspectives on collaborative practices of emergency care practitioners[13] were also reported.
In a qualitative study, team members considered authority, professional competence, decision-making skill, and the ability to communicate clearly and convey confidence and calmness as the important qualities of a successful team leader.[14] In addition, positive association is reported between trauma team's perception of leadership and the leaders’ clinical efficiency.[15]
In another study, the nurses described working together as personal and professional attributes such as shared goal, mutual respect, working together for the patient›s sake, assisting each other during crises, heavy workload, developing and maintaining relationships, and concurrence which meant shared understanding of roles, abilities, and responsibilities, and feeling of frustration and uncertainty due to unclear leadership.[16] Nurses in acute London hospitals in a survey reported overwork, lack of staff, space, equipment, and high levels of aggressive behavior as the barriers to delivering high-quality care.[17] The failure of interdisciplinary team to acknowledge the importance of the nursing's core caring values was considered as the important factor underpinning the nurses’ interprofessional disengagement.[18] Team context, structure, process, and perfor-mance, and their subsequent effects on cancer treatment care processes and patient outcomes had been presented as a conceptual model based on a targeted review of the literature.[19] Iranian nurses considered administrators’ supervision, co-workers’ communication and support, and skilfulness as the most important organizational climate, and lack of rewards and encouragement, inappropriate workload, and lack of participation in important decisions as the most negatively influential factors affecting their opinion about the organizational climate.[20]
Considering fatigue and stress as hindrance to teamwork is similar to the findings of a previous study about nurses and pilots, but different with the findings about the medical staff who denied these factors’ impact on their performance. The authors emphasized the importance of awareness of these factors to reduce the likelihood of error.[21]
Our findings highlight the active and dynamic nature of teamwork that fights with inactivity inherent in indolence, routinizing, and task orientation. A definition of interprofessional teamwork in trauma EDs may be suggested as:
“The active and prompt participation of an effective team under the command of an effective leader in activities toward prompt, holistic, and appropriate patient management while prioritising the patients, according to clear, complement, and interdependent role definition which is facilitated with appropriate physical and managerial context.”
“An effective team is composed of different specialists and nurses equipped with professional qualifications and communication skills who actively participate in activities toward goal.”
Limitations of the study are the young age and low experience of the participants in nursing and trauma EDs, the newness of the hospital, and confining participants to nurses and supervisors and data generation method to individual and focus group interviews. So, studies exploring teamwork from other team members’ and leaders’ perspectives, using observational methods and in various work settings are recommended
CONCLUSION
The findings explain how attributes related to team, context, and goal interrelate to produce teamwork in a trauma ED, and the potential of strategies related to these themes in improving it. The concepts related to teamwork were identified, and the participants’ quotations adds the applicability of the findings, by making them understandable by nurses, physicians, managers, educators, etc., who wish to implement, improve, teach, learn, or do research on teamwork in trauma EDs. The results also provide a significant guide for authorities in newly established EDs or those who are going to establish new trauma EDs. The findings may have broader applicability to other collaborative and dynamic work settings, especially health care related ones.
ACKNOWLEDGMENTS
This article is an extract from the dissertation of Zahra Khademian, and the work was financially supported by Shiraz University of Medical Sciences Grant No. 89-5338. The authors would like to thank Dr. Nasrin Shokrpour at Center for Development of Clinical Research of Nemazee Hospital for editorial assistance, Miss Leila Shayan at Center for Trauma Research of Shahid Rajaee Hospital, and physicians, nurses, supervisors, and authorities of Shahid Rajaee Trauma Center for their kind cooperation.
Footnotes
Source of Support: This article is an extract from the dissertation of Zahra Khademian, and the work was financially supported by Shiraz University of Medical Sciences Grant No. 89-5338
Conflict of Interest: None declared.
REFERENCES
- 1.Reeves S, Lewin S, Espin Sh, Zwarenstein M. 1st ed. New Delhi: Wiley-Blackwell; 2010. Interprofessional Teamwork for Health and Social Care; p. 68. [Google Scholar]
- 2.Steinemann S, Berg B, Skinner A, Ditulio A, Anzelon K, Teráda K, et al. In situ, multidisciplinary, simulation-based teamwork training improves early trauma care. J Surg Educ. 2011;68:472–7. doi: 10.1016/j.jsurg.2011.05.009. [DOI] [PubMed] [Google Scholar]
- 3.Capella J, Smith S, Philp A, Putnam T, Gilbert C, Fry W, et al. Teamwork training improves the clinical care of trauma patients. J Surg Educ. 2010;67:439–43. doi: 10.1016/j.jsurg.2010.06.006. [DOI] [PubMed] [Google Scholar]
- 4.Morey JC, Simon R, Jay GD, Wears RL, Salisbury M, Dukes KA, et al. Error reduction and performance improvement in the emergency department through formal teamwork training: Evaluation results of the MedTeams project. Health Serv Res. 2002;37:1553–81. doi: 10.1111/1475-6773.01104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Patel PB, Vinson DR. Team Assignment System: Expediting Emergency Department Care. Ann Emerg Med. 2005;46:499–506. doi: 10.1016/j.annemergmed.2005.06.012. [DOI] [PubMed] [Google Scholar]
- 6.Tabibi SJ, Najafi B, Shoaie SH. Waiting time in the emergency department in selected hospitals of Iran University of Medical Sciences in 2007. Pejouhesh. 2009;33:117–22. [Google Scholar]
- 7.Zohoor AR, Pilevar Zadeh M. Study of speed of offering services in emergency department at Kerman Bahonar Hospital in 2000. J Iran Univ Med Sci. 2003;10:413–20. [Google Scholar]
- 8.Sarcevic A. Understanding teamwork in trauma resuscitation through analysis of team errors, Dissertation; Rutgers University. [Last accessed on 2011 Aug 18]. Available from: http://www.mss3.libraries.rutgers.edu/dlr/outputds.php?pid=rutgers-lib:26395 .
- 9.Reader TW, Flin R, Mearns K, Cuthbertson BH. Developing a team performance framework for the intensive care unit. Crit Care Med. 2009;37:1787–93. doi: 10.1097/CCM.0b013e31819f0451. [DOI] [PubMed] [Google Scholar]
- 10.Manser T. Teamwork and patient safety in dynamic domains of healthcare: A review of the literature. Acta Anaesthesiol Scand. 2009;53:143–51. doi: 10.1111/j.1399-6576.2008.01717.x. [DOI] [PubMed] [Google Scholar]
- 11.Frakes P, Neely I, Tudoe R. Effective teamwork in trauma management. Emerg Nurse. 2009;17:12–7. doi: 10.7748/en2009.12.17.8.12.c7428. [DOI] [PubMed] [Google Scholar]
- 12.Bosch M, Faber MJ, Cruijsberg J, Voerman GE, Leatherman S, Grol RP, et al. Review article: Effectiveness of patient care teams and the role of clinical expertise and coordination: A literature review. Med Care Res Rev. 2009;66:5–35S. doi: 10.1177/1077558709343295. [DOI] [PubMed] [Google Scholar]
- 13.Cooper S, O’Carroll J, Jenkin A, Badger B. Collaborative practices in unscheduled emergency care: Role and impact of the emergency care practitioner--qualitative and summative findings. Emerg Med J. 2007;24:625–9. doi: 10.1136/emj.2006.043943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hjortdahl M, Ringen AH, Naess AC, Wisborg T. Leadership is the essential non-technical skill in the trauma team--results of a qualitative study. Scand J Trauma Resusc Emerg Med. 2009;17:48. doi: 10.1186/1757-7241-17-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sakran JV, Finneman B, Maxwell C, Sonnad SS, Sarani B, Pascual J, et al. Trauma leadership: Does perception drive reality? J Surg Educ. 2012;69:236–40. doi: 10.1016/j.jsurg.2011.09.004. [DOI] [PubMed] [Google Scholar]
- 16.Simmons D, Sherwood G. Neonatal intensive care unit and emergency department nurses’ descriptions of working together: Building team relationships to improve safety. Crit Care Nurs Clin North Am. 2010;22:253–60. doi: 10.1016/j.ccell.2010.03.007. [DOI] [PubMed] [Google Scholar]
- 17.West E, Barron DN, Reeves R. Overcoming the barriers to patient-centered care: Time, tools and training. J Clin Nurs. 2005;14:435–43. doi: 10.1111/j.1365-2702.2004.01091.x. [DOI] [PubMed] [Google Scholar]
- 18.Miller KL, Reeves S, Zwarenstein M, Beales JD, Kenaszchuk C, Conn LG. Nursing emotion work and interprofessional collaboration in general internal medicine wards: A qualitative study. J Adv Nurs. 2008;64:332–43. doi: 10.1111/j.1365-2648.2008.04768.x. [DOI] [PubMed] [Google Scholar]
- 19.Fennell ML, Das IP, Clauser S, Petrelli N, Salner A. The organization of multidisciplinary care teams: Modeling internal and external influences on cancer care quality. J Natl Cancer Inst Monogr. 2010;40:72–80. doi: 10.1093/jncimonographs/lgq010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nicpeyma N, Gholamnejad H. Influencing factors on hospital nurses’ perspectives about different Dimensions of Organizational Climate. Hayat. 2010;16:72–8. [Google Scholar]
- 21.Sexton JB, Thomas EJ, Helmreich RL. Error, stress, and teamwork in medicine and aviation: Cross sectional surveys. BMJ. 2000;320:745–9. doi: 10.1136/bmj.320.7237.745. [DOI] [PMC free article] [PubMed] [Google Scholar]