

Abstract
Background
Dicer, an RNase III-type endonuclease, is the key enzyme involved in RNA interference and microRNA pathways. Aberrant expression of Dicer is reported in several human cancers. Our aim was to assess the prognostic role of Dicer in breast cancer.
Methods
The entire series comprised 666 invasive breast cancers (IBCs), 480 DCIS cases (397 associated with IBC and 83 pure DCIS) and 305 lymph node metastases. Cytoplasmic Dicer expression by immunohistochemistry was scored as negative (no staining) and positive (weak, moderate or strong staining).
Results
Dicer staining was assessable in 446 IBC, 128 DCIS and 101 lymph node metastases. Expression of Dicer was observed in 33% (145/446) of IBCs, 34% (44/128) of DCIS and 57% (58/101) of lymph node metastases. Dicer expression was increased in nodal metastases compared to primary tumours (p<0.001); and was associated with ER negativity (p<0.001), HER2 positivity (p<0.001), high Ki67 labeling index (p<0.001) and expression of basal-like biomarkers (p = 0.002). Dicer positivity was more frequent in the HER2 overexpressing (p<0.001) and basal-like (p = 0.002) subtypes compared to luminal A subtype. Dicer expression was associated with reduced overall survival (OS) on univariate analysis (p = 0.058) and remained an independent predictor of OS on multivariate analysis (HR 2.84, 95% CI 1.43–5.62, p = 0.003), with nodal status (HR 2.61, 95% CI 1.18–5.80, p = 0.018) and PR (HR 0.28, 95% CI 0.13–0.59, p = 0.001). Further, moderate or strong expression of Dicer was associated with improved disease-free survival in the HER2-overexpressing subtype compared to negative or weak expression (p = 0.038).
Conclusion
Deregulated Dicer expression is associated with aggressive tumour characteristics and is an independent prognostic factor for OS. Our findings suggest that Dicer is an important prognostic marker in breast cancer and that its prognostic role may be subtype specific.
Introduction
MicroRNAs (miRNAs) are a family of short (∼20–23 nucleotide), endogenous, single-stranded RNA molecules that regulate gene expression in a sequence-specific manner [1]. Drosha and Dicer are two key enzymes involved in biogenesis of miRNAs. Following transcription, the primary miRNA transcript (pri-miRNA) undergoes endonucleocytic cleavage by the Drosha into a ∼60–100 nt hairpin precursor-miRNA (pre-miRNA) [2]. Following cleavage by Drosha, the pre-miRNA is transported out of the nucleus through interaction with exportin-5 (XPO5) and Ran-GTP [3] via recognition of the ∼2 nt 3′ overhangs of pre-miRNA hairpins [3]. In the cytoplasm, pre-miRNA is cleaved by RNase III enzyme Dicer, into a ∼22 nt double-stranded RNA product containing the mature miRNA guide strand and the passenger (miRNA*) strand. Mature miRNAs and Argonaute (Ago) proteins constitute the RNA-induced silencing complex (RISC), a ribonucleo-protein complex mediating post-transcriptional gene silencing [4]. Deregulation of miRNAs is associated with a broad range of human diseases including cancers [5] and miRNAs have been shown to be critically involved in control of cell survival and cell death decisions [6]. Global down-regulation of microRNAs (miRNAs) is a common feature of human tumours and impairment of miRNA biogenesis has been shown to enhance cancer progression [7].
The several components of miRNA biogenesis machinery have been shown to act as haploinsufficient tumour suppressors. For example, inactivating mutations have been reported in exportin-5 (XPO5) and TAR RNA-binding protein (TRBP2) in sporadic and hereditary colon carcinomas with microsatellite instability [8], [9]. Germline-inactivating mutations in Dicer have been shown to contribute significantly to familial pleuropulmonaryblastoma, cystic nephroma, ovarian Sertoli-Leydig tumour and intraocular medulloepithelioma [10], [11]. Analysis of eight tumours from Dicer mutation-positive patients showed there was no loss of the wild-type allele in any tumour [10]. These data suggest that Dicer down-regulation rather than its complete loss-of-function is selected for during tumourigenesis. Indeed, Dicer has been shown to act as a haploinsufficient tumour suppressor in K-Ras-induced mouse model of lung cancer and pre-clinical mouse model of retinoblastoma [12], [13]. Furthermore, analysis of Dicer copy number using data from Cancer Genome Project at the Sanger Institute revealed hemizygous deletions of DICER1 in 27% (207/761) of tumours derived from tissues of diverse origins such as central nervous system, lung, pancreas, soft tissues, breast and bone [12] and hemizygous deletion of Dicer was also observed in approximately 37% of breast cancers [12]. Consistent with Dicer being a haploinsufficient tumour suppressor, homozygous deletions have not been observed in any of these 761 tumours [10].
Several studies have investigated the role Dicer in cancer tissues from different sites and aberrant expression is commonly reported. However in breast cancer, the role of Dicer in progression and behaviour is unclear. Dicer mRNA has been more extensively studied than protein in invasive breast cancer (IBC) [14]–[20] and some report an association between reduced mRNA levels and poor outcome [15] whereas others do not [16], [18]. Reports of the prognostic role of Dicer protein are similarly contradictory with some demonstrating an association between reduced expression and outcome [17] and others failing to show an association [15]. The aim of this study is to investigate Dicer protein expression in breast cancer and to explore its association with progression of disease, clinico-pathological features and outcome in a large series of IBC. We demonstrate herein that deregulated Dicer expression is significantly associated with several adverse clinical features such as ER negativity, Ki67 labelling index and expression of basal markers. We report that deregulated Dicer expression is associated with poor overall survival in IBC and is associated with a reduced disease free survival in the HER2 overexpressing subtype of breast cancer.
Materials and Methods
Ethics Statement
Use of patient material in this study was approved by the Clinical Research Ethics Committee, Merlin Park Hospital, Galway at the meeting of 18th January 2006 (reference CA 41). The ethics committee waived the need for consent.
Patients and Tumour Material
Tumour material from 749 consecutive breast cancer cases managed at Galway University Hospital from 1999 to 2005 wasused for this study. Tissue microarrays (TMAs) were constructed from a single core (0.6 mm diameter) of formalin-fixed paraffin-embedded tissue as described previously [21]. The series comprised 666 invasive breast cancers, 480 DCIS cases (397 associated with IBC and 83 pure DCIS) and 305 lymph node metastases. The presence of tumour was confirmed by haematoxylin and eosin staining of TMA sections. The clinico-pathological characteristics of the series are shown in Table 1. Pathological data was taken from the original pathology report and all cases were reported by specialist breast pathologists. Grading of IBC was performed according to Elston and Ellis’ modified Bloom Richardson system [22] and DCIS was graded based on nuclear pleomorphism [23]. One hundred and thirteen patients diagnosed with IBC died during follow-up. Of the surviving patients, 301 had no evidence of disease progression. The median follow-up time was 48 months (range 1 to 177 months).
Table 1. Clinico-pathological features and biomarker profile of the series.
| Parameter | na | na (%) | |
| IBC | |||
| Tumour grade | 601 | ||
| 1 | 82 (14) | ||
| 2 | 307 (51) | ||
| 3 | 212 (35) | ||
| Tubule formation score | 583 | ||
| 1 | 31 (5) | ||
| 2 | 74 (13) | ||
| 3 | 478 (82) | ||
| Nuclear pleomorphism score | 583 | ||
| 1 | 7 (1) | ||
| 2 | 287 (49) | ||
| 3 | 289 (50) | ||
| Mitotic count score | 583 | ||
| 1 | 367 (3) | ||
| 2 | 103 (18) | ||
| 3 | 113 (19) | ||
| Histological type | 661 | ||
| Ductal | 509 (77) | ||
| Lobular | 102 (15) | ||
| Mucinous | 14 (2) | ||
| Mixed ductal and lobular | 10 (2) | ||
| Tubular | 5 (1) | ||
| Medullary | 5 (1) | ||
| Microinvasive ductal | 5 (1) | ||
| Apocrine | 3 (0.5) | ||
| Ductal and papillary or cribriform | 3(0.5) | ||
| Invasive papillary | 2 (0.3) | ||
| Other | 3 (0.5) | ||
| Tumour size (mm) | 625 | ||
| ≤20 | 239 (38) | ||
| 21–50 | 314 (50) | ||
| >50 | 72 (12) | ||
| Nodal status | 596 | ||
| Positive | 302 (51) | ||
| Negative | 294 (49) | ||
| Number of positive lymph nodes | 596 | ||
| 0 | 294 (49) | ||
| 1–3 | 165 (28) | ||
| 4–9 | 88 (15) | ||
| ≥10 | 49 (8) | ||
| Lymphovascular invasion | 386 | ||
| Present | 203 (53) | ||
| Absent | 174 (45) | ||
| Probable | 9 (2) | ||
| Number of events | 663 | ||
| Alive, no disease | 301 (45) | ||
| Alive, LR disease | 191 (29) | ||
| Alive, distant metastases | 58 (9) | ||
| Dead with disease progression | 87 (13) | ||
| Dead with no disease progression | 26 (4) | ||
| ER | 522 | ||
| Positive | 344 (66) | ||
| Negative | 178 (34) | ||
| PR | 534 | ||
| Positive | 297 (56) | ||
| Negative | 237 (44) | ||
| HER2 | 602 | ||
| Positive | 85 (14) | ||
| Negative | 517 (86) | ||
| BCL2 | 534 | ||
| Positive | 290 (54) | ||
| Negative | 244 (46) | ||
| Ki67 | 540 | ||
| Positive | 163 (30) | ||
| Negative | 377 (70) | ||
| EGFR | 527 | ||
| Positive | 77 (14) | ||
| Negative | 450 (85) | ||
| CK5/6 | 463 | ||
| Positive | 42 (9) | ||
| Negative | 421 (91) | ||
| CK14 | 444 | ||
| Positive | 94 (21) | ||
| Negative | 350 (79) | ||
| p53 | 523 | ||
| Positive | 105 (20) | ||
| Negative | 418 (80) | ||
| DCIS associated with IBC | 397 | ||
| Grade | 339 | ||
| Low | 13 (4) | ||
| Intermediate | 137 (40) | ||
| High | 189 (56) | ||
| Size b (mm) | 59 | ||
| Median | 38 | ||
| Range | 2–236 | ||
| Pure DCIS | 83 | ||
| Grade | 54 | ||
| Low | 7 (13) | ||
| Intermediate | 21 (39) | ||
| High | 26 (48) | ||
| Size (mm) | 41 | ||
| Median | 15 | ||
| Range | 0.8–83 | ||
| Number of events | 81 | ||
| Alive, no disease | 63 (78) | ||
| Alive, LR disease | 4 (5) | ||
| Alive, distant metastases | 1 (1) | ||
| Dead with disease progression | 9 (11) | ||
| Dead with no disease progression | 4 (5) |
a no. of cases for which data is available.
b whole tumour measurement is given in cases if it differs from the size of the IBC.
LR: locoregional.
Immunohistochemistry
TMA sections of IBC were stained with oestrogen receptor (ER) (Neomarker, clone SP, 1∶100), progesterone receptor (PR) (Leica, clone 16, 1∶200), HER2 (Dako), Ki67 (Dako, MIB-1, 1∶200), BCL2 (Novocastra, bcl-2/100/D5, 1∶200), cytokeratin (CK) 14 (Novocastra, LL002, 1∶20), CK5/6 (Dako, D5/16, 1∶100), EGFR (Dako, pharmDx kit) and p53 (Dako, DO-7, 1∶100) using standard indirect immunoperoxidase procedures. Nuclear staining for ER, PR [24]–[27], p53 [28]–[30] and Ki67 was scored as positive with a cut-off of 10% [31]–[36]. Membranous staining with HER2 was recorded as negative, weakly positive and positive (Dako Herceptest method) [37] with confirmation of 2+ cases by fluorescent in situ hybridisation (FISH). Cytoplasmic expression of BCL2 with a 10% cut-off was used [38]–[40] and any observed cytoplasmic staining with CK14, CK5/6 and EGFR was considered positive. Molecular subtypes were defined based on these markers as luminal A (ER and/or PR positive, HER2 negative); luminal B (ER and/or PR positive, HER2 positive); HER2-overexpressing (ER and PR negative, HER2 positive); triple negative (ER, PR and HER2 negative); and basal-like (ER, PR, HER2 negative and positive for at least one basal marker (CK5/6, CK14 or EGFR)). IHC was scored by two pathologists independently each blinded to the clinico-pathological data and outcome (Table 1).
We tested two commercially available anti-Dicer antibodies [Clonegene rabbit polyclonal antibody, (CG031, clone 13D6R) and Abcam mouse monoclonal antibody, (ab14601, clone 13D6)]. We observed specific myoepithelial staining with the Clonegene antibody (Figure 1a) as reported previously [19]. We confirmed the specificity of the Clonegene antibody by pre-incubation with an excess of its competing peptide (CG302, Clonegene) and staining of breast whole tissue sections (WTS) (Figure 1b). A blocking peptide against the Abcam anti-Dicer antibody was not available. The anti-Dicer antibody from Clonegene (CG301) was used for subsequent analysis. TMA sections were cut at 4 µm thickness and mounted onto glass slides, deparaffinised in xylene, followed by hydration in graded ethanol solutions. Antigen retrieval involved microwaving of sections in citrate buffer (pH 6) at 98°C for 20 mins. Sections were blocked for 10 mins in 2% horse serum in 0.1 M phosphate buffered saline. Slides were then incubated with anti-Dicer antibody at a dilution of 1∶2500 at room temperature overnight. After washing, ImmPRESS universal reagent (Vector) was applied for 40 minutes. The chromogen was then developed with ImmPACT DAB (Vector). A haematoxylin counterstain was used.
Figure 1. Dicer expression by IHC in normal breast tissue.
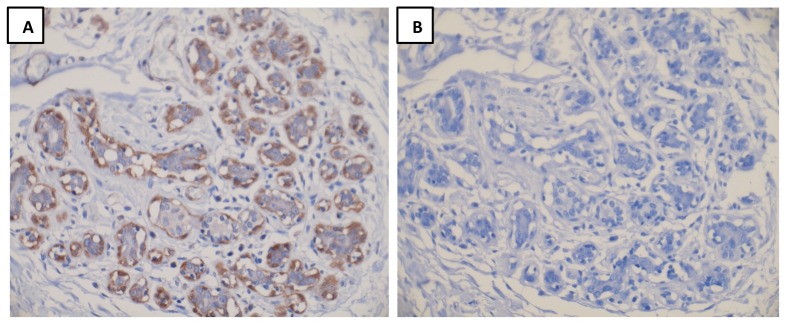
Representative images of Dicer staining (A) without blocking peptide and (B) with blocking peptide are shown. Panel A is representative of Dicer staining in normal breast tissue.
Scoring of Dicer was optimised on 26 WTSs of IBC. Dicer was expressed consistently in the cytoplasm of myoepithelial cells (Figure 1b). Luminal epithelium was negative. Cases of IBC, pure DCIS and DCIS associated with IBC and lymph node metastases were stained with Dicer. Tumour cells showed cytoplasmic expression with nuclear staining rarely observed in cases with moderate or strong cytoplasmic expression. Cores of normal breast parenchyma and normal tissue within tumour cores served as positive controls. Intensity of cytoplasmic staining was scored as 0, absent; 1, weak; 2, moderate; or 3, strong staining (Figures 2 and 3), where score 0 and score 3 showed expression equal to that seen in benign luminal cells and in normal myoepithelial cells respectively. The percentage of positive tumour cells was recorded and was homogeneous throughout each tumour.
Figure 2. Dicer expression in DCIS.
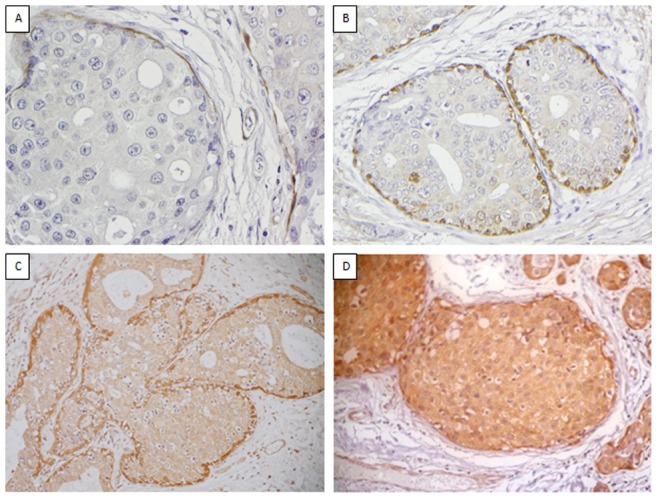
Representative images of the spectrum of the staining intensity observed for Dicer in DCIS where 0 = negative (A), 1 = weak (B), 2 = moderate (C) and 3 = strong (D).
Figure 3. Dicer expression in IBC.
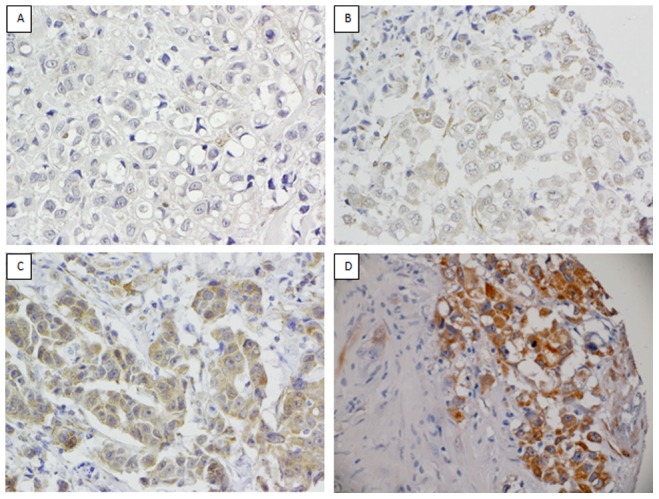
Representative images of the spectrum of staining observed for Dicer in IBC where 0 = negative (A), 1 = weak (B), 2 = moderate (C) and 3 = strong (D).
Statistical Analysis
Since the staining for Dicer was homogeneous, only intensity of Dicer staining was used for analysis as reported by others [41]–[45]. Cases with no staining (score 0) were considered negative and cases with any staining intensity (scores 1 to 3) were considered positive. This cut off was used because the number of cases with an intensity score of 2 and 3 were quite small and it also demonstrated the strongest association with outcome. Cases without a representative stained core were excluded from the analysis. Summary statistics included proportions for categorical variables. Comparisons between Dicer expression and clinico-pathological features were initially analysed using Chi-square tests. p values <0.0025 were considered significant when the Bonferroni correction for multiple tests was applied. Two proportion tests were then used to estimate the effect (difference in proportions) of significant variables. Kaplan-Meier estimates were plotted for overall survival (OS) and disease-free survival (DFS). The log-rank test was used to examine the statistical significance of the differences observed between the groups. A multivariate Cox regression model was also used to compute hazard ratios (HR) and 95% confidence intervals (95% CI), adjusting for known prognostic variables (including grade, tumour size, nodal status). Stepwise variable selection was used to identify the most parsimonious model with Dicer expression which best predicted DFS and OS. p values reported were two tailed and p<0.05 was considered statistically significant. Statistical analysis was performed using R statistical software (v2.12.0) and SPSS (v20).
Results
Dicer Expression in Breast Cancer Progression
Data on Dicer expression by immunohistochemistry was available in 446 IBCs, the associated DCIS in 108 cases, 20 cases of pure DCIS and 101 lymph node metastases. The number of pure DCIS cases was small, therefore for analysis these cases were combined with data on DCIS with associated IBC (total = 128). Expression of Dicer (scores 1, 2 or 3) was observed less frequently in DCIS (44/128, 34%), and IBC (145/446, 33%) compared with lymph node metastasis (58/101, 57%) (χ2 = 22.37, p<0.001) (Table 2). There was no association between Dicer staining and grade of DCIS and there was no difference in Dicer expression comparing pure DCIS to DCIS with associated IBC. Dicer was expressed in 36% (n = 24) of high grade, 23% (n = 11) of intermediate grade and 50% (n = 1) of low grade DCIS (p = 0.23, Fisher’s exact test). Dicer expression was examined in paired samples. There was no difference between expression of Dicer in DCIS and IBC in 42 of 65 (14 positive and 28 negative) of paired cases. However, up-regulation of expression between DCIS (score 0) and invasive tumour (score 1, 2 or 3) was seen in 20% (n = 13) while 15% (n = 10) showed the converse. Next we analysed 76 paired IBCs and lymph node metastases. Dicer expression was unchanged in 42 (55%) paired cases (15 positive and 27 negative), and was negative in IBC and positive in lymph node metastasis in 26 (34%) cases while 8 (11%) showed the converse.
Table 2. Dicer expression scores in invasive carcinoma, DCIS and lymph node metastasis.
| Dicer Score (intensity) | DCIS | Invasive Carcinoma | Lymph Node Metastasis |
| na(%) | na(%) | na(%) | |
| Negative (0) | 84 (66) | 301 (67) | 43 (43) |
| Positive (1,2,3) | 44 (34) | 145 (33) | 58 (57) |
| Intensity | |||
| 1 | 28 (22) | 76 (17) | 42 (42) |
| 2 | 15 (12) | 40 (9) | 12 (12) |
| 3 | 1 (1) | 29 (7) | 4 (4) |
| Total | 128b | 446 | 101 |
a number of cases for which Dicer expression data was available.
b includes 108 DCIS cases associated with DCIS and 20 pure DCIS cases.
Dicer Expression in IBC and its Associations with Clinico-pathological Features
Associations between Dicer expression and clinico-pathological variables are shown in Table 3. Dicer positivity (score 1, 2 or 3) was seen in a significantly higher proportion of ER negative as compared to ER positive cases (estimate of difference in proportions of 27.4%). There was a significant association between Dicer positivity and HER2 overexpression (estimate of difference in proportions of 20.3%) and Ki67 labelling index. Dicer positivity was also associated with expression of basal-like biomarker EGFR and, in the analysis of breast cancer subtypes, luminal A subtype showed a significantly lower proportion of Dicer positive patients than basal-like and HER2 overexpressing subtypes.
Table 3. Associations between Dicer expression and clinico-pathological variables in IBC.
| Variable | Total | Dicer positive (Intensity 1,2,3) | Dicer negative (Intensity 0) | ?2 | p valueb |
| na (%) | na (%) | na (%) | |||
| Patient age (years) | |||||
| <50 | 131 (29) | 44 (34) | 87 (66) | 0.10 | 0.754 |
| ≥50 | 315 (71) | 101 (32) | 214 (68) | ||
| Histological tumour type | |||||
| Ductal | 345 (78) | 119 (34) | 226 (66) | 2.58 | 0.275 |
| Lobular | 72 (16) | 18 (25) | 54 (75) | ||
| Other | 24 (6) | 7 (29) | 17 (71) | ||
| Tumour grade | |||||
| 1/2 | 305 (69) | 88 (29) | 217 (71) | 9.07 | 0.024 |
| 3 | 134 (31) | 56 (42) | 78 (58) | ||
| Tubule formation score | |||||
| 1 | 25 (6) | 6 (24) | 19 (76) | 1.75 | 0.417 |
| 2 | 52 (13) | 20 (38) | 32 (62) | ||
| 3 | 335 (81) | 106 (32) | 229 (68) | ||
| Nuclear pleomorphism score | |||||
| 1 | 5 (1) | 1 (20) | 4 (33) | 2.52 | 0.284 |
| 2 | 208 (51) | 60 (29) | 148 (56) | ||
| 3 | 199 (48) | 71 (36) | 128 (64) | ||
| Mitotic count score | |||||
| 1 | 265 (64) | 74 (28) | 191 (72) | 8.66 | 0.007 |
| 2/3 | 147 (36) | 58 (39) | 89 (61) | ||
| UICC c T stage | |||||
| pT1 | 121 (28) | 30 (25) | 91 (75) | 4.52 | 0.104 |
| pT2 | 249 (58) | 89 (36) | 160 (64) | ||
| pT3 | 62 (14) | 21 (34) | 41 (66) | ||
| UICC c N stage | |||||
| pN0 | 210 (49) | 71 (34) | 139 (66) | 1.47 | 0.681 |
| pN1 | 119 (28) | 36 (30) | 83 (70) | ||
| pN2 | 65 (15) | 23 (35) | 42 (65) | ||
| pN3 | 32 (8) | 8 (25) | 24 (75) | ||
| Lymphovascular invasion | |||||
| Present | 144 (54) | 46 (32) | 98 (68) | 0.59 | 0.444 |
| Absent | 123 (46) | 34 (28) | 89 (72) | ||
| ER status | |||||
| Positive | 274 (67) | 66 (24) | 208 (76) | 30.31 | <0.001 |
| Negative | 132 (33) | 68 (52) | 64 (48) | ||
| PR status | |||||
| Positive | 236 (57) | 69 (29) | 167 (71) | 3.37 | 0.066 |
| Negative | 180 (43) | 68 (38) | 112 (62) | ||
| HER2 | |||||
| Positive | 64 (14) | 32 (50) | 32 (50) | 10.23 | 0.001 |
| Negative | 380 (86) | 113 (30) | 267 (70) | ||
| Triple negative | |||||
| Yes | 57 (14) | 28 (49) | 29 (51) | 8.47 | 0.004 |
| No | 355 (86) | 106 (30) | 249 (70) | ||
| Molecular subtype | |||||
| Luminal A | 277 (76) | 71 (26) | 206 (74) | ||
| Luminal B | 27 (7) | 10 (37) | 17 (63) | 1.11 | 0.293d |
| HER2 overexpressing | 34 (9) | 21 (62) | 13 (38) | 17.29 | <0.001d |
| Basal-like | 27 (7) | 15 (56) | 12 (44) | 9.43 | 0.002d |
| Ki67 labelling index | |||||
| <10% | 294 (71) | 79 (27) | 215 (73) | 12.16 | <0.001 |
| ≥10% | 119 (29) | 53 (45) | 66 (55) | ||
| BCL2 | |||||
| Positive | 226 (55) | 64 (28) | 162 (72) | 3.18 | 0.074 |
| Negative | 186 (45) | 68 (37) | 118 (63) | ||
| CK14 | |||||
| Positive | 80 (21) | 34 (43) | 46 (57) | 5.04 | 0.025 |
| Negative | 297(79) | 87 (29) | 210 (71) | ||
| CK5/6 | |||||
| Positive | 52 (14) | 21 (40) | 31 (60) | 1.15 | 0.285 |
| Negative | 326 (86) | 107 (33) | 219 (67) | ||
| EGFR | |||||
| Positive | 54 (13) | 31 (57) | 23 (43) | 17.69 | <0.001 |
| Negative | 356 (87) | 102 (29) | 254 (71) | ||
| p53 | |||||
| Positive | 83 (21) | 37 (45) | 46 (55) | 6.75 | 0.009 |
| Negative | 318 (79) | 94 (30) | 224 (70) |
a number of cases for which Dicer expression and data for the relevant parameter was available.
b p values <0.0025 were considered significant when the Bonferroni correction for multiple tests was applied.
c UICC TNM Classification of Malignant Tumours 7th Edition [70].
d compared to luminal A subtype.
Dicer Expression and Patient Outcome
In the whole series, Dicer expression (score 1, 2 or 3) was associated with reduced overall survival (OS) compared with Dicer negativity by Kaplan Meier estimates (p = 0.058, log-rank test) (Figure 4a) but there was no significant difference in disease free survival (DFS) between those who were Dicer positive or negative (Figure 4b). Cox regression revealed that Dicer positivity was associated with an increased likelihood of death of 1.55 (CI: 0.98–2.45) compared with Dicer negativity (p = 0.061). Multivariate Cox proportional hazard regression analysis, adjusting for lymph node status, pathological T stage, tumour grade, lymphovascular invasion, ER, PR and HER2 status, revealed that Dicer expression was a strong (significant) predictor for OS (p = 0.003). In the final model, selected using variable selection, Dicer expression was associated with an increased likelihood of death from breast cancer by a factor of 2.84 (HR, 2.84; 95% CI, 1.43–5.62; p = 0.003) adjusting for lymph node status and PR status (Table 4). Dicer expression in IBC was not a significant predictor of DFS in the multivariate analysis, neither was Dicer expression in the lymph node metastases associated with OS or DFS (p = 0.57 and p = 0.15 respectively, log-rank test).
Figure 4. Kaplan-Meier curves for OS (A) and DFS (B) in IBC categorised according to Dicer expression in the entire series.
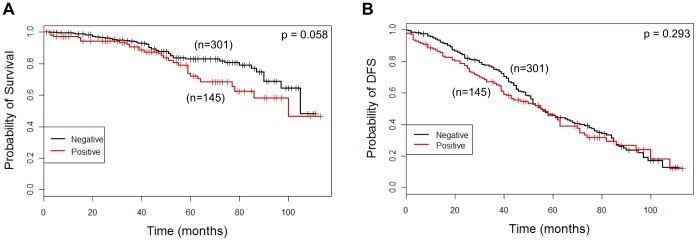
Dicer expression is categorised as negative (intensity score 0) and positive (intensity score 1, 2 or 3).
Table 4. Multivariate analysis of Dicer expression for OS.
| Variable | Coefficient | HRa | 95% CI | p value |
| Dicer expression | 1.04 | 2.84 | 1.43–5.62 | 0.003 |
| Lymph node status | 0.96 | 2.61 | 1.18–5.80 | 0.018 |
| PR status | −1.28 | 0.28 | 0.13–0.59 | 0.001 |
a HR: Hazard ratio.
Finally, we examined the association between Dicer expression and outcome in the different molecular subtypes as Dicer expression was significantly associated with HER2 overexpressing and basal-like subtypes on univariate analysis (Table 3). Dicer expression was associated with a poorer OS compared with Dicer negativity in the luminal B subtype (p = 0.057, log-rank test) but was not significant for the other subtypes (Figure A in file Figure S1). Neither was there a significant association between Dicer expression and DFS in the different subtypes (Figure A in file Figure S1). Because Dicer expression appeared to be paradoxically associated with improved DFS in the HER2 overexpressing subtype (shown in Figure 5a), we examined this association further. For this purpose the Dicer-positive group was divided into Dicer low (score 1) and Dicer high (score 2 or 3) categories. Although the number of cases and events at extended follow up are small, we observed a better prognosis for DFS with high Dicer expression compared to low or negative Dicer expression in the HER2 overexpressing subgroup (p = 0.0376) (Figure 5b).
Figure 5. Kaplan-Meier curves for DFS (A, B) and OS (C) in the HER2 overexpressing subtype of IBC categorized according to Dicer expression.

(A, C) Dicer expression is categorised as negative (intensity score 0) and positive (intensity scores 1, 2 and 3). (B) Dicer expression is categorised as negative (intensity score 0), low (intensity score 1) and high (intensity score 2 and 3).
Association between High Dicer Expression and Clinico-pathological Variables and Outcome
Associations between high Dicer expression and clinico-pathological variables, biomarker expression and outcome were also examined by dichotomising Dicer expression as low (intensity scores 0 and 1) and high (intensity scores 2 and 3). Again, there was a significant association between high Dicer expression and the HER2 overexpressing compared to the luminal A subtype (χ2 = 8.31, p = 0.004); and high Dicer expression was more common in HER2 positive (χ2 = 4.29, p = 0.04) and EGFR positive (χ2 = 4.73, p = 0.03) compared to HER2 and EGFR negative cases respectively. No other statistically significant associations between high Dicer expression and clinico-pathological variables, biomarker expression, or outcome were found, perhaps due to the lower numbers of cases in the score 2/3 group (n = 69) (Supplementary Table S1).
Discussion
We examined expression of the Dicer protein, a critical enzyme involved in miRNA biogenesis, in breast cancer with the aim of exploring its role in disease progression and its impact on outcome. We found that Dicer expression was similar in the majority of in situ and invasive tumours and was increased in nodal metastases suggesting a role for in Dicer in progression to metastatic disease. Dicer expression was associated with features of aggressive disease and was a predictor of reduced OS that was independent of clinico-pathological variables, steroid hormone and HER2 receptor status in the entire series. Paradoxically, low Dicer expression was significantly associated with reduced DFS in HER2 expressing subtype of disease.
Deregulation of Dicer is commonly observed in several tumour types however there are conflicting results regarding its prognostic role. Increased Dicer protein expression was associated with adverse prognostic features in cancers of the prostate [41], ovary [42], colon [44], in malignant melanomas [45], soft tissue sarcomas [46] and nasopharyngeal carcinomas [47], whereas low protein expression was associated with tumour invasiveness, metastasis and poor survival in carcinomas of the gallbladder [48], colon [49], ovary [50], and breast [17]. Results from studies of Dicer mRNA across tumour types are also contradictory. Reduced Dicer mRNA in cancers of the breast [14]–[16], [51]–[53], lung [54], [55] and ovary [56] was associated with aggressive phenotypic features, whereas the converse is described in prostatic [41], ovarian [42], [57], oesophageal [58] and colorectal [44] cancers by others. The data for Dicer is also conflicting within tumours of the same type. We show a paradoxical association for Dicer protein and outcome in the HER2 overexpressing subtype of breast cancer compared to the whole series. In ovarian cancer, Flavin et al. found an association between increased Dicer protein expression and both nodal metastasis and high Ki67 proliferation index [42], while Faggad et al. observed low levels of Dicer in tumours with lymph node metastasis, high grade and poor survival [50]. Similarly, both low [49] and high [44] Dicer protein expression were associated with and adverse features and/or outcome in colorectal cancer.
In IBC, Dicer mRNA has been evaluated more commonly than protein and an association between low mRNA levels and adverse clinico-pathological features and/or adverse outcome is reported by most [14]–[16], [51], [52], [59] but not all [20]. Only two other reports have evaluated the prognostic role of Dicer protein in breast cancer tissue samples [15], [17]. Grelier et al. found that low mRNA levels were associated with non-luminal subtype and reduced metastases free survival whereas low protein expression was significantly associated with luminal A subtype and not with outcome in 86 cases [15], [17]. The present study is one of only two reports that examined Dicer protein in a large patient series and both show that Dicer is an independent predictor of outcome. In a series of over 1000 IBCs, Khoshnaw et al. showed that reduced protein expression was an independent predictor of improved DFS and was significantly associated with high tumour grade, hormone receptor negativity and absence of luminal keratins [17]. The pattern of Dicer expression in that study however conflicts both with data from our study, where Dicer positivity was associated with aggressive phenotypic features (high Ki67, ER negativity, basal phenotype and with reduced OS) and also with the data from Grelier et al. where Dicer protein was associated with ER positivity and the luminal A subtype [15], [17].
Several reasons have been proposed for these discrepancies. miRNA expression patterns are highly specific for cell type and cellular differentiation status. Thus, depending on whether the net effect of the majority of miRNAs in a given cell is oncogenic or tumour suppressive, the loss of Dicer expression can have opposite consequences on cell survival and proliferation. Thus, Dicer deregulation may be site specific and its role may differ in different tumours and in different subtypes. This is supported by functional studies where knockdown of Dicer expression rendered MDAMB-231 and MDA-MB-436 cells significantly more invasive, while knockdown of Dicer in MCF-7 cells led to G1 arrest and increase sensitivity to cisplatin [60], [61] suggesting that the effects of Dicer on development and progression of cancer are context-dependent. Secondly, Dicer mRNA levels are not well correlated with protein levels with a 72% concordance reported in cell lines using microarray hybridisation and real-time reverse transcription-PCR (qPCR) [15]. Furthermore, the regulation of Dicer expression is largely post-transcriptional and complex. A regulatory feedback loop exists through which Dicer expression is regulated by mature miRNAs such as miR-103/107 and let-7 family members [18], [62].
Technical issues are also likely to be important. Unresolved issues about the specificity and sensitivity of commercially available anti-Dicer antibodies are a major limiting factor in the interpretation of protein expression by IHC. Different antibodies have been used by investigators and all describe cytoplasmic expression of Dicer. Notably, nuclear staining was seen in triple negative breast cancer in one report [19], and we also observed nuclear staining in a minority of samples where there was strong cytoplasmic staining. Nuclear expression would be consistent with a function of Dicer in the nucleus and, indeed, Dicer has been shown to shuttle between the cytoplasm and the nucleus in the fission yeast Schizosaccharomyces pombe and mammalian cells [63], [64]. In IBC both strong and weak staining was observed in normal luminal epithelial cells in two reports [15], [17] whereas our study and that of Passon et al. [19] observed strong staining in normal myoepithelial cells. Notably, the specificity of the antibody used by us was confirmed by pre-incubation with an excess of its competing peptide. Finally, the small size of series and different scoring systems employed by investigators compound the issue. Only six reports, including the present report, included more than 200 cases from cancers of the breast [17], stomach [43], colon [49], malignant melanomas [45] and nasopharyngeal carcinoma [47], and scoring systems based on the intensity of staining [15], [41]–[46], [54], [65]–[67] or the percentage of positive cells with [17], [47], [49], [50] or without [48] intensity have been employed. The extent to which these technical variations influence the interpretation of the clinical role of Dicer protein expression remains unclear.
We found that Dicer expression differed significantly between the primary tumour (either in situ or invasive) and the metastasis. A putative role for Dicer in neoplastic progression from normal to malignant to metastatic disease has been demonstrated in clinical studies at other sites including the prostate [41], ovary [57], lung [54] and colon [68] as well as breast [15], [17]. Khoshnaw et al. observed a gradual change in Dicer expression with progression from normal tissue, to either in situ or invasive disease to nodal metastasis [17] and Dicer mRNA levels differed between breast cancers with nodal metastases and those without [15]. While the precise level of Dicer expression differs between these studies, nonetheless they support a role for its deregulation in breast cancer progression. A putative mechanism through induction of a mesenchymal phenotype in breast cancer has been proposed. Dicer mRNA was lower in cell lines that underwent epithelial to mesenchymal transition (EMT) [15], [69] and down-regulation of Dicer protein by miR-103/107 was shown to be associated with EMT and metastasis [18].
In summary, we report the second largest study of Dicer protein expression in clinical breast cancer samples. We show that expression of Dicer protein is deregulated and stepwise alterations occur between in situ or invasive disease and nodal metastases. Deregulated, namely increased, expression was significantly associated with features of aggressive disease and was an predictor of reduced OS in independent of clinico-pathological variables, steroid hormone and HER2 receptor status the whole series whereas high Dicer expression was associated with an improved DFS in the HER2 overexpressing subgroup. There are clear discrepancies between reports about the precise expression level of Dicer mRNA and protein in clinical samples from tumours at the same and different sites and their correlation with clinico-pathological features and outcome. However, not withstanding the inconsistencies it is encouraging that Dicer was an independent predictor of outcome in the two largest series studied. These support a role for Dicer in progression of disease and in prognostication. Studies to further elucidate the complex mechanisms regulating expression of Dicer and to investigate its relationship with other factors and pathways in human cancer types are warranted. Furthermore, issues about the specificity and sensitivity of commercially available anti-Dicer antibodies need to be investigated further.
Supporting Information
Figure A. Kaplan-Meier curves for OS in the different subtypes of IBC categorised according to Dicer expression. (A) Luminal A, (B) luminal B, (C) HER2 overexpressing, (D) triple negative and (E) basal-like. In each subtype, Dicer expression is categorised as negative (intensity score 0) and positive (intensity score 1, 2 and 3). Figure B. Kaplan-Meier curves for DFS in the different subtypes of IBC categorised according to Dicer expression. (A) Luminal A, (B) luminal B, (C) HER2 overexpressing, (D) triple negative and (E) basal-like subtype. In each subtype, Dicer expression is categorised as negative (intensity score 0) and positive (intensity score 1, 2 and 3).
(PPTX)
Associations between Dicer expression dichotomised as positive (intensity score 2 and 3) and negative (intensity score 0, 1) and clinico-pathological variables in IBC.
(DOC)
Funding Statement
This publication has emanated from research conducted with the financial support of the Health Research Board [grant number HRA_HSR/2010/24], Millennium Fund from National University of Ireland, Galway to S.G. and Breast Cancer Campaign [grant number 2011PR26 (to G.C.)]. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Bartel DP (2004) MicroRNAs: Genomics, Biogenesis, Mechanism, and Function. Cell 116: 281–297. [DOI] [PubMed] [Google Scholar]
- 2. Beezhold KJ, Castranova V, Chen F (2010) Microprocessor of microRNAs: regulation and potential for therapeutic intervention. Mol Cancer 9: 134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Yi R, Qin Y, Macara IG, Cullen BR (2003) Exportin-5 mediates the nuclear export of pre-microRNAs and short hairpin RNAs. Genes Dev 17: 3011–3016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Gregory RI, Chendrimada TP, Cooch N, Shiekhattar R (2005) Human RISC couples microRNA biogenesis and posttranscriptional gene silencing. Cell 123: 631–640. [DOI] [PubMed] [Google Scholar]
- 5. Farazi TA, Horlings HM, Ten Hoeve JJ, Mihailovic A, Halfwerk H, et al. (2011) MicroRNA sequence and expression analysis in breast tumours by deep sequencing. Cancer Res 71: 4443–4453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bushati N, Cohen SM (2007) microRNA functions. Annu Rev Cell Dev Biol 23: 175–205. [DOI] [PubMed] [Google Scholar]
- 7. Kumar MS, Lu J, Mercer KL, Golub TR, Jacks T (2007) Impaired microRNA processing enhances cellular transformation and tumourigenesis. Nat Genet 39: 673–677. [DOI] [PubMed] [Google Scholar]
- 8. Melo SA, Moutinho C, Ropero S, Calin GA, Rossi S, et al. (2010) A Genetic Defect in Exportin-5 Traps Precursor MicroRNAs in the Nucleus of Cancer Cells. Cancer Cell 18: 303–315. [DOI] [PubMed] [Google Scholar]
- 9. Melo SA, Ropero S, Moutinho C, Aaltonen LA, Yamamoto H, et al. (2009) A TARBP2 mutation in human cancer impairs microRNA processing and DICER1 function. Nat Genet 41: 365–370. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 10. Slade I, Bacchelli C, Davies H, Murray A, Abbaszadeh F, et al. (2011) DICER1 syndrome: clarifying the diagnosis, clinical features and management implications of a pleiotropic tumour predisposition syndrome. J Med Genet 48: 273–278. [DOI] [PubMed] [Google Scholar]
- 11. Hill DA, Ivanovich J, Priest JR, Gurnett CA, Dehner LP, et al. (2009) DICER1 mutations in familial pleuropulmonary blastoma. Science 325: 965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Kumar MS, Pester RE, Chen CY, Lane K, Chin C, et al. (2009) Dicer1 functions as a haploinsufficient tumour suppressor. Genes Dev 23: 2700–2704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Lambertz I, Nittner D, Mestdagh P, Denecker G, Vandesompele J, et al. (2010) Monoallelic but not biallelic loss of Dicer1 promotes tumourigenesis in vivo. Cell Death Differ 17: 633–641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Blenkiron C, Goldstein LD, Thorne NP, Spiteri I, Chin SF, et al. (2007) MicroRNA expression profiling of human breast cancer identifies new markers of tumour subtype. Genome Biol 8: R214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Grelier G, Voirin N, Ay AS, Cox DG, Chabaud S, et al. (2009) Prognostic value of Dicer expression in human breast cancers and association with the mesenchymal phenotype. Br J Cancer 101: 673–683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Dedes KJ, Natrajan R, Lambros MB, Geyer FC, Lopez-Garcia MA, et al. (2011) Down-regulation of the miRNA master regulators Drosha and Dicer is associated with specific subgroups of breast cancer. Eur J Cancer 47: 138–150. [DOI] [PubMed] [Google Scholar]
- 17. Khoshnaw SM, Rakha EA, Abdel-Fatah TM, Nolan CC, Hodi Z, et al. (2012) Loss of Dicer expression is associated with breast cancer progression and recurrence. Breast Cancer Res Treat 135: 403–413. [DOI] [PubMed] [Google Scholar]
- 18. Martello G, Rosato A, Ferrari F, Manfrin A, Cordenonsi M, et al. (2010) A MicroRNA Targeting Dicer for Metastasis Control. Cell 141: 1195–1207. [DOI] [PubMed] [Google Scholar]
- 19. Passon N, Gerometta A, Puppin C, Lavarone E, Puglisi F, et al. (2012) Expression of Dicer and Drosha in triple-negative breast cancer. J Clin Pathol 65: 320–326. [DOI] [PubMed] [Google Scholar]
- 20. Yan M, Huang H-Y, Wang T, Wan Y, Cui S-D, et al. (2012) Dysregulated Expression of Dicer and Drosha in Breast Cancer. Pathology & Oncology Research 18: 343–348. [DOI] [PubMed] [Google Scholar]
- 21. Kononen J, Bubendorf L, Kallioniemi A, Barlund M, Schraml P, et al. (1998) Tissue microarrays for high-throughput molecular profiling of tumour specimens. Nat Med 4: 844–847. [DOI] [PubMed] [Google Scholar]
- 22. Elston CW, Ellis IO (1991) Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: experience from a large study with long-term follow-up. Histopathology 19: 403–410. [DOI] [PubMed] [Google Scholar]
- 23.(January 2005) NHSBSP Publication No. 58 Pathology Reporting of Breast Disease. NHS Cancer Screening Programmes and The Royal College of Pathologists.
- 24. Regan MM, Viale G, Mastropasqua MG, Maiorano E, Golouh R, et al. (2006) Re-evaluating adjuvant breast cancer trials: assessing hormone receptor status by immunohistochemical versus extraction assays. J Natl Cancer Inst 98: 1571–1581. [DOI] [PubMed] [Google Scholar]
- 25. Viale G, Regan MM, Maiorano E, Mastropasqua MG, Dell’Orto P, et al. (2007) Prognostic and predictive value of centrally reviewed expression of estrogen and progesterone receptors in a randomized trial comparing letrozole and tamoxifen adjuvant therapy for postmenopausal early breast cancer: BIG 1–98. J Clin Oncol 25: 3846–3852. [DOI] [PubMed] [Google Scholar]
- 26. Dowsett M, Allred C, Knox J, Quinn E, Salter J, et al. (2008) Relationship between quantitative estrogen and progesterone receptor expression and human epidermal growth factor receptor 2 (HER-2) status with recurrence in the Arimidex, Tamoxifen, Alone or in Combination trial. J Clin Oncol 26: 1059–1065. [DOI] [PubMed] [Google Scholar]
- 27. Viale G, Regan MM, Maiorano E, Mastropasqua MG, Golouh R, et al. (2008) Chemoendocrine compared with endocrine adjuvant therapies for node-negative breast cancer: predictive value of centrally reviewed expression of estrogen and progesterone receptors–International Breast Cancer Study Group. J Clin Oncol 26: 1404–1410. [DOI] [PubMed] [Google Scholar]
- 28. Le MG, Mathieu MC, Douc-Rasy S, Le Bihan ML, Adb El All H, et al. (1999) c-myc, p53 and bcl-2, apoptosis-related genes in infiltrating breast carcinomas: evidence of a link between bcl-2 protein over-expression and a lower risk of metastasis and death in operable patients. Int J Cancer 84: 562–567. [DOI] [PubMed] [Google Scholar]
- 29. Osanai T, Takagi Y, Toriya Y, Nakagawa T, Aruga T, et al. (2005) Inverse correlation between the expression of O6-methylguanine-DNA methyl transferase (MGMT) and p53 in breast cancer. Jpn J Clin Oncol 35: 121–125. [DOI] [PubMed] [Google Scholar]
- 30. Moran MS, Yang Q, Haffty BG (2009) The Yale University Experience of Early-Stage Invasive Lobular Carcinoma (ILC) and Invasive Ductal Carcinoma (IDC) Treated with Breast Conservation Treatment (BCT): Analysis of Clinical-Pathologic Features, Long-Term Outcomes, and Molecular Expression of COX-2, Bcl-2, and p53 as a Function of Histology. The Breast Journal 15: 571–578. [DOI] [PubMed] [Google Scholar]
- 31. Veronese SM, Gambacorta M, Gottardi O, Scanzi F, Ferrari M, et al. (1993) Proliferation index as a prognostic marker in breast cancer. Cancer 71: 3926–3931. [DOI] [PubMed] [Google Scholar]
- 32. Brown RW, Allred CD, Clark GM, Osborne CK, Hilsenbeck SG (1996) Prognostic value of Ki-67 compared to S-phase fraction in axillary node-negative breast cancer. Clin Cancer Res 2: 585–592. [PubMed] [Google Scholar]
- 33. Tan P, Cady B, Wanner M, Worland P, Cukor B, et al. (1997) The cell cycle inhibitor p27 is an independent prognostic marker in small (T1a,b) invasive breast carcinomas. Cancer Res 57: 1259–1263. [PubMed] [Google Scholar]
- 34. Harbeck N, Dettmar P, Thomssen C, Berger U, Ulm K, et al. (1999) Risk-group discrimination in node-negative breast cancer using invasion and proliferation markers: 6-year median follow-up. Br J Cancer 80: 419–426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Spyratos F, Ferrero-Pous M, Trassard M, Hacene K, Phillips E, et al. (2002) Correlation between MIB-1 and other proliferation markers: clinical implications of the MIB-1 cutoff value. Cancer 94: 2151–2159. [DOI] [PubMed] [Google Scholar]
- 36. Jansen RL, Hupperets PS, Arends JW, Joosten-Achjanie SR, Volovics A, et al. (1998) MIB-1 labelling index is an independent prognostic marker in primary breast cancer. Br J Cancer 78: 460–465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Wolff AC, Hammond ME, Schwartz JN, Hagerty KL, Allred DC, et al. (2007) American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch Pathol Lab Med 131: 18–43. [DOI] [PubMed] [Google Scholar]
- 38. Silvestrini R, Veneroni S, Daidone MG, Benini E, Boracchi P, et al. (1994) The Bcl-2 Protein: a Prognostic Indicator Strongly Related to p53 Protein in Lymph Node-Negative Breast Cancer Patients. Journal of the National Cancer Institute 86: 499–504. [DOI] [PubMed] [Google Scholar]
- 39. Elledge RM, Green S, Howes L, Clark GM, Berardo M, et al. (1997) bcl-2, p53, and response to tamoxifen in estrogen receptor-positive metastatic breast cancer: a Southwest Oncology Group study. Journal of Clinical Oncology 15: 1916–1922. [DOI] [PubMed] [Google Scholar]
- 40. Ménard S, Casalini P, Tomasic G, Pilotti S, Cascinelli N, et al. (1999) Pathobiologic identification of two distinct breast carcinoma subsets with diverging clinical behaviors. Breast Cancer Research and Treatment 55: 167–175. [DOI] [PubMed] [Google Scholar]
- 41. Chiosea S, Jelezcova E, Chandran U, Acquafondata M, McHale T, et al. (2006) Up-regulation of dicer, a component of the MicroRNA machinery, in prostate adenocarcinoma. Am J Pathol 169: 1812–1820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Flavin RJ, Smyth PC, Finn SP, Laios A, O’Toole SA, et al. (2008) Altered eIF6 and Dicer expression is associated with clinicopathological features in ovarian serous carcinoma patients. Mod Pathol 21: 676–684. [DOI] [PubMed] [Google Scholar]
- 43. Tchernitsa O, Kasajima A, Schafer R, Kuban RJ, Ungethum U, et al. (2010) Systematic evaluation of the miRNA-ome and its downstream effects on mRNA expression identifies gastric cancer progression. J Pathol 222: 310–319. [DOI] [PubMed] [Google Scholar]
- 44. Faber C, Horst D, Hlubek F, Kirchner T (2011) Overexpression of Dicer predicts poor survival in colorectal cancer. Eur J Cancer 47: 1414–1419. [DOI] [PubMed] [Google Scholar]
- 45. Ma Z, Swede H, Cassarino D, Fleming E, Fire A, et al. (2011) Up-Regulated Dicer Expression in Patients with Cutaneous Melanoma. PLoS ONE 6: e20494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Papachristou DJ, Rao UN, Korpetinou A, Giannopoulou E, Sklirou E, et al. (2012) Prognostic significance of Dicer cellular levels in soft tissue sarcomas. Cancer Invest 30: 172–179. [DOI] [PubMed] [Google Scholar]
- 47. Guo X, Liao Q, Chen P, Li X, Xiong W, et al. (2012) The microRNA-processing enzymes: Drosha and Dicer can predict prognosis of nasopharyngeal carcinoma. J Cancer Res Clin Oncol 138: 49–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Shu GS, Yang ZL, Liu DC (2012) Immunohistochemical study of Dicer and Drosha expression in the benign and malignant lesions of gallbladder and their clinicopathological significances. Pathol Res Pract 208: 392–397. [DOI] [PubMed] [Google Scholar]
- 49.Faggad A, Kasajima A, Weichert W, Stenzinger A, Elwali NE, et al.. (2012) Down-regulation of the microRNA processing enzyme Dicer is a prognostic factor in human colorectal cancer. Histopathology. [DOI] [PubMed]
- 50. Faggad A, Budczies J, Tchernitsa O, Darb-Esfahani S, Sehouli J, et al. (2010) Prognostic significance of Dicer expression in ovarian cancer-link to global microRNA changes and oestrogen receptor expression. J Pathol 220: 382–391. [DOI] [PubMed] [Google Scholar]
- 51. Ivshina AV, George J, Senko O, Mow B, Putti TC, et al. (2006) Genetic reclassification of histologic grade delineates new clinical subtypes of breast cancer. Cancer Res 66: 10292–10301. [DOI] [PubMed] [Google Scholar]
- 52. Pawitan Y, Bjohle J, Amler L, Borg AL, Egyhazi S, et al. (2005) Gene expression profiling spares early breast cancer patients from adjuvant therapy: derived and validated in two population-based cohorts. Breast Cancer Res 7: R953–964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Cheng C, Fu X, Alves P, Gerstein M (2009) mRNA expression profiles show differential regulatory effects of microRNAs between estrogen receptor-positive and estrogen receptor-negative breast cancer. Genome Biol 10: R90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Chiosea S, Jelezcova E, Chandran U, Luo J, Mantha G, et al. (2007) Overexpression of Dicer in precursor lesions of lung adenocarcinoma. Cancer Res 67: 2345–2350. [DOI] [PubMed] [Google Scholar]
- 55. Karube Y, Tanaka H, Osada H, Tomida S, Tatematsu Y, et al. (2005) Reduced expression of Dicer associated with poor prognosis in lung cancer patients. Cancer Sci 96: 111–115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Merritt WM, Lin YG, Han LY, Kamat AA, Spannuth WA, et al. (2008) Dicer, Drosha, and outcomes in patients with ovarian cancer. N Engl J Med 359: 2641–2650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Vaksman O, Hetland TE, Trope CG, Reich R, Davidson B (2012) Argonaute, Dicer, and Drosha are up-regulated along tumour progression in serous ovarian carcinoma. Human pathology. [DOI] [PubMed]
- 58. Sugito N, Ishiguro H, Kuwabara Y, Kimura M, Mitsui A, et al. (2006) RNASEN Regulates Cell Proliferation and Affects Survival in Esophageal Cancer Patients. Clinical Cancer Research 12: 7322–7328. [DOI] [PubMed] [Google Scholar]
- 59. Chin K, DeVries S, Fridlyand J, Spellman PT, Roydasgupta R, et al. (2006) Genomic and transcriptional aberrations linked to breast cancer pathophysiologies. Cancer Cell 10: 529–541. [DOI] [PubMed] [Google Scholar]
- 60. Noh H, Hong S, Dong Z, Pan ZK, Jing Q, et al. (2011) Impaired MicroRNA Processing Facilitates Breast Cancer Cell Invasion by Upregulating Urokinase-Type Plasminogen Activator Expression. Genes Cancer 2: 140–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Bu Y, Lu C, Bian C, Wang J, Li J, et al. (2009) Knockdown of Dicer in MCF-7 human breast carcinoma cells results in G1 arrest and increased sensitivity to cisplatin. Oncol Rep 21: 13–17. [PubMed] [Google Scholar]
- 62. Hinkal GW, Grelier G, Puisieux A, Moyret-Lalle C (2011) Complexity in the regulation of Dicer expression: Dicer variant proteins are differentially expressed in epithelial and mesenchymal breast cancer cells and decreased during EMT. Br J Cancer 104: 387–388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Emmerth S, Schober H, Gaidatzis D, Roloff T, Jacobeit K, et al. (2010) Nuclear retention of fission yeast dicer is a prerequisite for RNAi-mediated heterochromatin assembly. Dev Cell 18: 102–113. [DOI] [PubMed] [Google Scholar]
- 64. Sinkkonen L, Hugenschmidt T, Filipowicz W, Svoboda P (2010) Dicer is associated with ribosomal DNA chromatin in mammalian cells. PLoS ONE 5: e12175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Chiosea SI, Barnes EL, Lai SY, Egloff AM, Sargent RL, et al. (2008) Mucoepidermoid carcinoma of upper aerodigestive tract: clinicopathologic study of 78 cases with immunohistochemical analysis of Dicer expression. Virchows Arch 452: 629–635. [DOI] [PubMed] [Google Scholar]
- 66. Papachristou DJ, Sklirou E, Corradi D, Grassani C, Kontogeorgakos V, et al. (2012) Immunohistochemical analysis of the endoribonucleases Drosha, Dicer and Ago2 in smooth muscle tumours of soft tissues. Histopathology 60: E28–36. [DOI] [PubMed] [Google Scholar]
- 67. Zheng ZH, Sun XJ, Fu WN, Guan Y, Gao F, et al. (2007) Decreased expression of DICER1 in gastric cancer. Chin Med J (Engl) 120: 2099–2104. [PubMed] [Google Scholar]
- 68. Stratmann J, Wang CJ, Gnosa S, Wallin A, Hinselwood D, et al. (2011) Dicer and miRNA in relation to clinicopathological variables in colorectal cancer patients. BMC Cancer 11: 345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Cochrane D, Cittelly D, Howe E, Spoelstra N, McKinsey E, et al. (2010) MicroRNAs Link Estrogen Receptor Alpha Status and Dicer Levels in Breast Cancer. Hormones and Cancer 1: 306–319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Cancer IUA (2009) TNM Classification of Malignant Tumours, 7th ed. In: Sobin LH GM, Wittekind C editor. Oxford: Wiley-Blackwell.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure A. Kaplan-Meier curves for OS in the different subtypes of IBC categorised according to Dicer expression. (A) Luminal A, (B) luminal B, (C) HER2 overexpressing, (D) triple negative and (E) basal-like. In each subtype, Dicer expression is categorised as negative (intensity score 0) and positive (intensity score 1, 2 and 3). Figure B. Kaplan-Meier curves for DFS in the different subtypes of IBC categorised according to Dicer expression. (A) Luminal A, (B) luminal B, (C) HER2 overexpressing, (D) triple negative and (E) basal-like subtype. In each subtype, Dicer expression is categorised as negative (intensity score 0) and positive (intensity score 1, 2 and 3).
(PPTX)
Associations between Dicer expression dichotomised as positive (intensity score 2 and 3) and negative (intensity score 0, 1) and clinico-pathological variables in IBC.
(DOC)