

Abstract
A 4-year-old boy with neurofibromatosis type 1 (NF1), an asymptomatic optic glioma, and a right basal ganglia T2-hyperintense lesion (figure, A and B) developed a left hemiparesis with hyperreflexia over the course of a year. Neuroimaging revealed a cyst-like mass in the region of his previously identified T2 hyperintensity (figure, C and D). While it is often difficult to distinguish T2 hyperintensities from low-grade glioma without tissue diagnosis,1 even with advanced imaging methods,2 T2 hyperintensities typically disappear with age and do not become cystic with associated mass effect. Coupled with the development of new neurologic signs, these MRI features are worrisome for neoplasm in a patient with NF1.
A 4-year-old boy with neurofibromatosis type 1 (NF1), an asymptomatic optic glioma, and a right basal ganglia T2-hyperintense lesion (figure, A and B) developed a left hemiparesis with hyperreflexia over the course of a year. Neuroimaging revealed a cyst-like mass in the region of his previously identified T2 hyperintensity (figure, C and D). While it is often difficult to distinguish T2 hyperintensities from low-grade glioma without tissue diagnosis,1 even with advanced imaging methods,2 T2 hyperintensities typically disappear with age and do not become cystic with associated mass effect. Coupled with the development of new neurologic signs, these MRI features are worrisome for neoplasm in a patient with NF1.
Figure. T2 hyperintensities in a child with neurofibromatosis type 1.
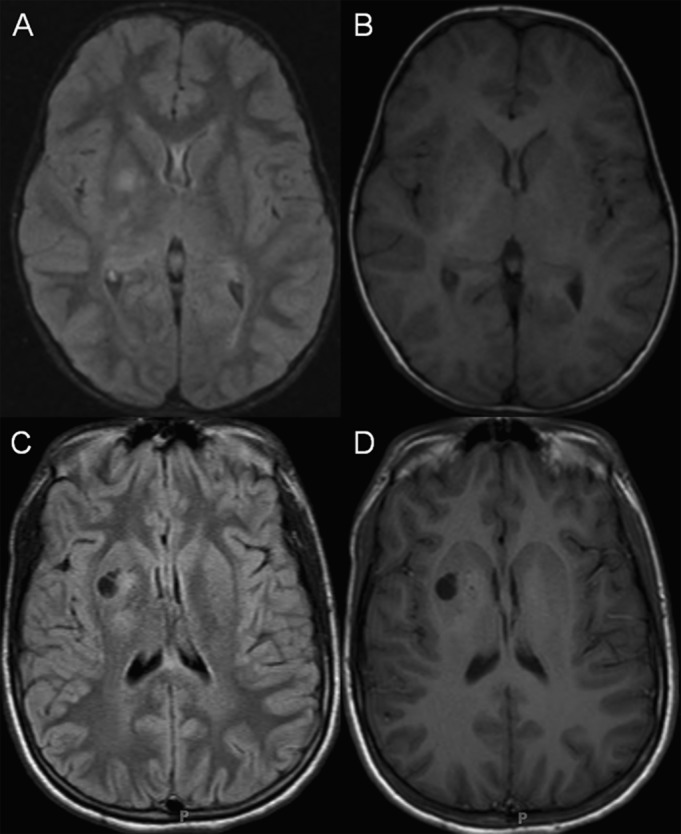
Brain MRI from 2003 revealed a T2 hyperintensity in the right basal ganglia, frequently observed in children with neurofibromatosis type 1. In 2012, a cyst-like mass was found in the identical location associated with a new left hemiparesis and hyperreflexia. (A, C) Fluid-attenuated inversion recovery images; (B, D) T1-weighted images.
Supplementary Material
AUTHOR CONTRIBUTIONS
A.P.O. wrote the initial draft of the manuscript. R.C.M. and J.S.S. reviewed the MRI data. D.H.G. performed the final editing.
STUDY FUNDING
No targeted funding reported.
DISCLOSURE
The authors report no disclosures relevant to the manuscript. Go to Neurology.org for full disclosures.
REFERENCES
- 1.DeBella K, Poskitt K, Szudek J, Friedman JM. Use of “unidentified bright objects” on MRI for diagnosis of neurofibromatosis 1 in children. Neurology 2000;54:1646–1651 [DOI] [PubMed] [Google Scholar]
- 2.Ferraz-Filho JR, da Rocha AJ, Muniz MP, Souza AS, Goloni-Bertollo EM, Pavarino-Bertelli EC. Diffusion tensor MR imaging in neurofibromatosis type 1: expanding the knowledge of microstructural brain abnormalities. Pediatr Radiol 2012;42:449–454 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.