

Dear Editor:
Retinopathy of prematurity (ROP) is a vasoproliferative retinal disease that is a major cause of blindness in children.1 According to a national survey, approximately 37% of ophthalmologists who screen for ROP are general ophthalmologists without fellowship training.2 This raises the question of whether residency training is adequate to produce ophthalmologists competent in ROP care, especially in light of studies demonstrating variable diagnostic competency for ROP by less experienced board-eligible ophthalmologists.3,4 Because ROP is a rapidly progressive disease that can result in blindness, basic competency in ROP should be expected of all ophthalmologists-in-training. Through a web-based survey of ophthalmology residency program directors and third-year residents across the United States, we sought to characterize the quality and extent of ROP training during ophthalmology residency.
All ophthalmology residency programs listed in the San Francisco Match database were invited to participate in the spring of 2010. Out of 117 program directors, 42 (36%) indicated willingness to participate, allowing us to contact 139 of 446 (31%) third-year residents. These individuals were sent an anonymous survey approved by the institutional review board.
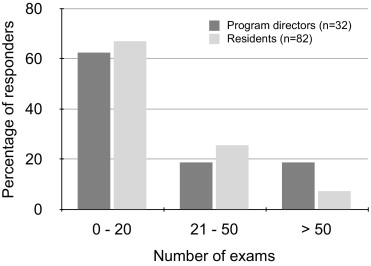
Thirty three of 42 (79%) program directors and 82 of 139 (59%) third-year residents completed the survey. This yielded a total of 114 responders representing 42 of 117 (36%) ophthalmology residency programs from throughout the United States. Supplementary Figure 1 (available at http://aaojournal.org) displays the estimated number of exams performed by residents. The estimates made by program directors and by residents were similar (Fisher exact test of independence, P = 0.2). Seventy five of 114 (66%) responders—program directors and residents—estimated that residents perform ≤20 ROP exams during residency. In particular, 22 of 114 (19%) responders reported zero exams, and only 12 of 114 (11%) estimated that residents perform >50 exams. The number of exams directly supervised by an attending ophthalmologist is depicted in Supplementary Figure 2 (available at http://aaojournal.org.); 55 of 94 (59%) responders estimated that an attending directly supervises all bedside ROP examinations performed by residents, whereas 28 of 94 (30%) estimated that attending supervision occurred during less than one-third of exams. The estimates by program directors and residents were again highly concordant (P = 0.96).
Fourteen of 82 (17%) residents felt confident with their ROP examination skills at the end of residency. Supplementary Figure 3 (available at http://aaojournal.org) demonstrates that residents who felt confident versus not confident had performed a greater number of exams (P = 0.0002). Only 5 of 114 (4%) survey participants reported a formal assessment of competency in ROP at their institution.
Anecdotally, it has been our observation that some residents believe the presence of fellows may interfere with their clinical experience. Twenty nine of 42 (69%) programs were associated with either a pediatric, medical retina, or surgical retina fellowship, or a combination thereof. Supplementary Figure 4 (available at http://aaojournal.org) illustrates the estimated number of ROP exams performed by residents at programs with versus without fellowship programs. Residents at programs with associated fellowships performed significantly fewer examinations (P = 0.039). Notably, the percentage of responders who estimated doing ≤20 exams during residency was 43% (9 of 21) in programs lacking fellows, compared with 71% (66 of 93) in programs with fellows.
Because the standard of care for treatment-requiring ROP involves laser photocoagulation of the peripheral retina, we asked residents and program directors to estimate the number of laser procedures performed by a resident. Seventy three of 94 (78%) responders estimated that residents perform zero laser procedures, and 19/94 (20%) estimated that residents perform 1-5 laser procedures.
The key findings of this study are as follows: (1) most residents receive limited or no exposure to ROP examination and treatment during residency; (2) ROP exams are sometimes performed by residents without direct attending supervision; and (3) residents at programs with pediatric ophthalmology or retina fellows perform fewer exams than those without fellows. Although this survey study is limited by the low overall response rate, these findings raise concerns about the adequacy of ROP training during residency. Interestingly, a recent study on ROP training during fellowship also demonstrated similar deficiencies, including limited supervision of exams by attending.5 We therefore encourage residency program directors to scrutinize the ROP training paradigm at their institutions and establish formal training expectations with attending physicians. We hope these survey results will provide the basis for improvements in ROP care and limit or even reverse the decline in ophthalmologists who care for infants with ROP.
Supplementary Material
Figure 1. Estimated number of retinopathy of prematurity (ROP) examinations performed by a resident during residency. The dark gray bars represent estimates by program directors (n=32), whereas the light gray bars represent estimates by residents (n=82).
{kind=link}
Figure 2. Estimated percentage of retinopathy of prematurity (ROP) examinations performed by residents that were directly supervised by an attending physician. The dark gray bars represent estimates made by program directors (n=28), and the light gray bars represent estimates by residents (n=64).
{kind=link}
Figure 3. Proportion of residents who felt confident with retinopathy of prematurity (ROP) screening versus not confident as a function of the number of examinations performed. The dark gray bars represent the proportion of residents who felt confident (n=14), and the light gray bars represent the proportion of residents who did not feel confident (n=68).
{kind=link}
Figure 4. Estimated number of exams performed by residents at programs with and without pediatric or retina fellows. There were 13 programs lacking fellowships represented by 21 responders (dark gray bars), and 29 programs with associated fellowships represented by 93 responders in this survey (light gray bars).
{kind=link}
Acknowledgments
Financial Disclosure(s): Supported by the St. Giles Foundation (R.V.P.C.), grant EY19474 from the National Institutes of Health (M.F.C.), and by Research to Prevent Blindness (R.V.P.C., M.F.C., A.K.L.). The sponsors of funding organizations had no role in the design or conduct of this research.
References
- 1.National Eye Institute. Retinopathy of Prematurity. [Accessed April 14, 2012]; Available at: http://www.nei.nih.gov/health/rop.
- 2.Kemper AR, Freedman SF, Wallace DK. Retinopathy of prematurity care: patterns of care and workforce analysis. J AAPOS. 2008;12:344–8. doi: 10.1016/j.jaapos.2008.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Myung JS, Paul Chan RV, Espiritu MJ, et al. Accuracy of retinopathy of prematurity image-based diagnosis by pediatric ophthalmology fellows: implications for training. J AAPOS. 2011;15:573–8. doi: 10.1016/j.jaapos.2011.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Paul Chan RV, Williams SL, Yonekawa Y, et al. Accuracy of retinopathy of prematurity diagnosis by retinal fellows. Retina. 2010;30:958–65. doi: 10.1097/IAE.0b013e3181c9696a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wong RK, Ventura CV, Espiritu MJ, et al. Training fellows for retinopathy of prematurity care: a Web-based survey. J AAPOS. 16:177–81. doi: 10.1016/j.jaapos.2011.12.154. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure 1. Estimated number of retinopathy of prematurity (ROP) examinations performed by a resident during residency. The dark gray bars represent estimates by program directors (n=32), whereas the light gray bars represent estimates by residents (n=82).
Figure 2. Estimated percentage of retinopathy of prematurity (ROP) examinations performed by residents that were directly supervised by an attending physician. The dark gray bars represent estimates made by program directors (n=28), and the light gray bars represent estimates by residents (n=64).
Figure 3. Proportion of residents who felt confident with retinopathy of prematurity (ROP) screening versus not confident as a function of the number of examinations performed. The dark gray bars represent the proportion of residents who felt confident (n=14), and the light gray bars represent the proportion of residents who did not feel confident (n=68).
Figure 4. Estimated number of exams performed by residents at programs with and without pediatric or retina fellows. There were 13 programs lacking fellowships represented by 21 responders (dark gray bars), and 29 programs with associated fellowships represented by 93 responders in this survey (light gray bars).