

Hepcidin, the key hormone in iron homeostasis,1 is regulated by erythropoietic activity and hypoxia (negative feedback),2 as well as iron stores (hepcidin induction by iron) and inflammation (upregulation).1,3 Only a few publications have focused on hepcidin in the context of hematopoietic cell transplantation (HCT).4–7 We hypothesized that changes in erythropoietic activity (myelosuppression followed by engraftment) and iron parameters (raised ferritin and transferrin saturation (TSAT)) following conditioning and transplantation had an impact on hepcidin levels.
One hundred and twenty-seven patients were included in our randomized trial comparing no erythropoietic therapy, darbepoetin alpha (DA) therapy (300 μg QOW from Day 28 to Day 112 posttransplant) in the DA group and DA (same DA schedule) + intravenous (iv) iron sucrose (200 mg on Days 28, 42 and 56) in the DA + iron group, following autologous HCT.8 From among these, we randomly selected 15 patients in each group. Patients’ characteristics are summarized in Table 1. Details about transfusion thresholds, blood analyses and patient eligibility are reported elsewhere.8 Erythropoietic activity was evaluated by soluble transferrin receptor (sTfR). Serum hepcidin-25 was quantified on serum samples stored before conditioning and on Days 7, 14, 28, 60, 100 and 180 post transplant, by weak cation exchange time-of-flight mass spectrometry.9
Table 1.
Patients’ characteristics.
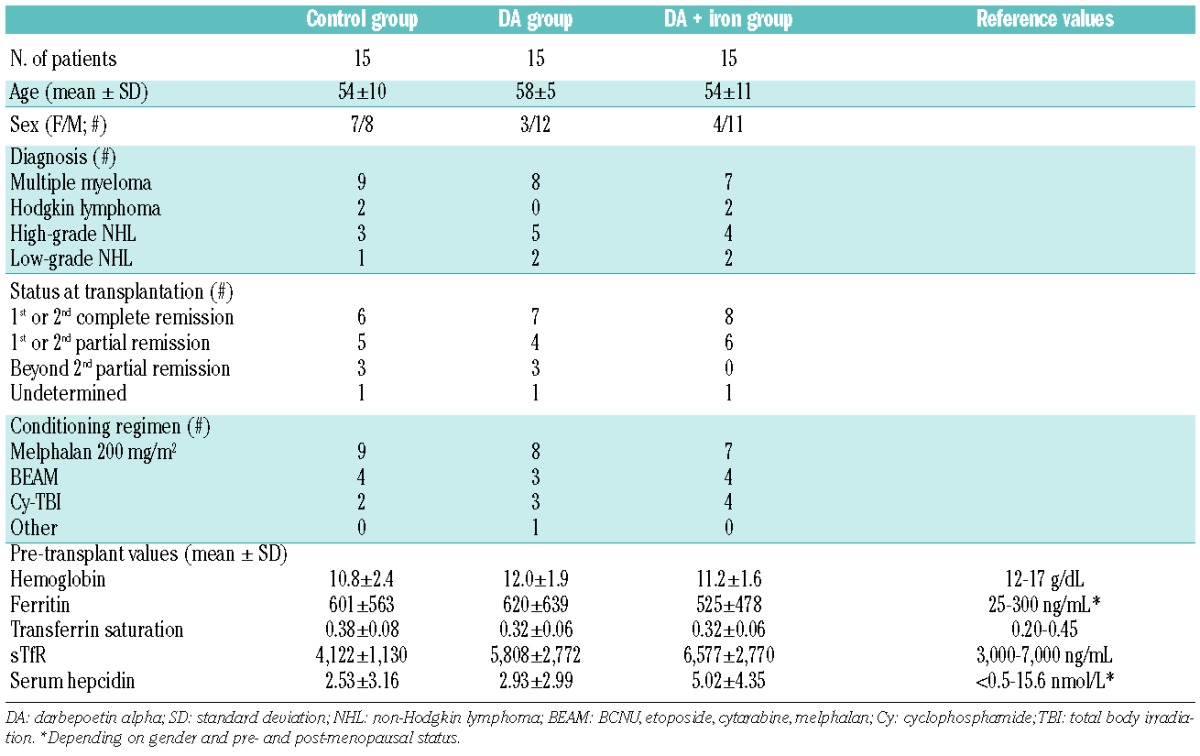
Figure 1A shows serum hepcidin over time in the 3 groups. Before HCT, hepcidin values were 2.53±3.16 (mean ± standard deviation), 3.93±2.99 and 5.02±4.35 nmol/L in the control, DA and DA + iron groups, respectively (NS). Hepcidin peaked seven days after HCT, followed by a rapid decrease until Day 28. Thereafter, hepcidin levels in the control group remained stable, whereas those in DA groups decreased rapidly until Day 60. This decrease was better illustrated with hepcidin expressed as a percentage of Day 28 value (before DA treatment) (Figure 1B). From Day 60, hepcidin levels in the DA + iron group increased again and surpassed those in the control and DA groups on Day 100. Two-way analyses of variance (ANOVA) confirmed the effect of treatment group (control vs. DA vs. DA + iron groups) and posttransplant time on hepcidin levels (P<0.001). Hepcidin levels prior to transplantation and on Days 14 and 28 correlated with nearly all subsequent ones except with Day-7 values (P<0.01).
Figure 1.
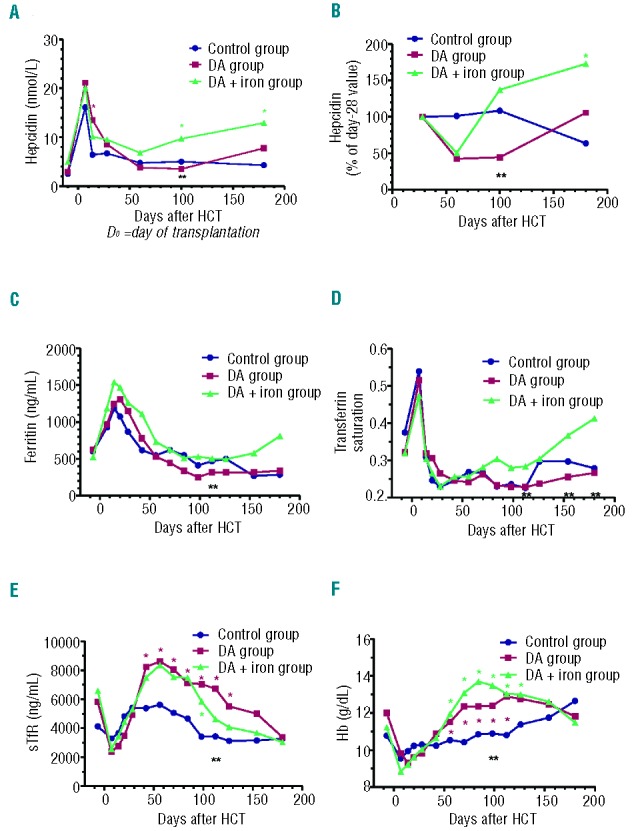
Temporal evolution of mean hepcidin (absolute values (A) and percentage of Day-28 values (B)), ferritin (C), transferrin saturation (D), sTfR (E) and hemoglobin (F) following transplantation in the 3 groups. *Comparisons between either the DA group (*in red) or the DA + iron group (*in green) and the control group, P<0.05. **Comparisons between the DA group and the DA + iron group, P<0.05.
Figures 1C, 1D, 1E and 1F show the evolution over time of ferritin, TSAT, sTfR and Hb, respectively. Two weeks after HCT, ferritin peaked in the 3 groups, then decreased. TSAT was highest on Day 7, then decreased until Day 28. After DA initiation on Day 28, TSAT tended to increase in the DA + iron group. STfR levels dropped on Day 7 due to conditioning, followed by a sharp increase with engraftment. After DA initiation, sTfR increased in both DA groups, but levelled off in the control group.
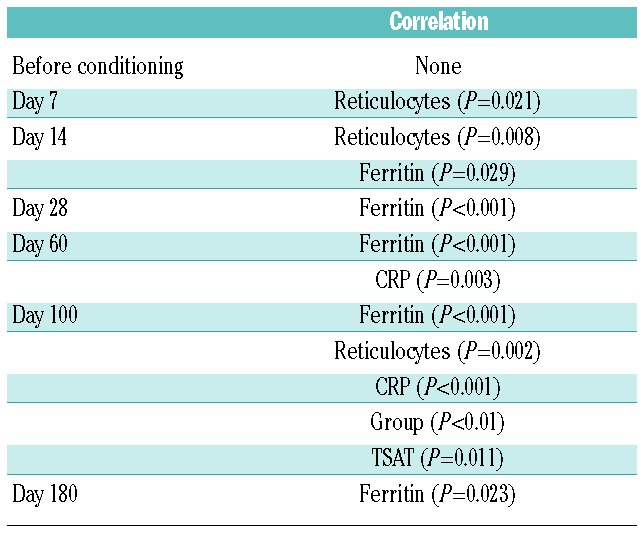
All hepcidin values except those on Day 7 correlated with preceding, same day or subsequent ferritin levels; correlations were strongest when examined in same day samples, as well as on Days 60 and 100 (r approx. 0.75, P<0.0001). Otherwise, hepcidin weakly correlated with TSAT (r between 0.32 and 0.65, P values ranging from 0.05 to <0.0001) and negatively with sTfR (on Days 60 and 100: r between −0.41 and −0.58, P<0.02) and reticulocytes (only on Day 100, r=−0.42, P=0.004). Finally, no significant correlations were observed between hepcidin and C-reactive protein (CRP), Hb, Hct, percentages of hypochromic red cells and erythropoietin. In multiple linear regression, we found that ferritin was the independent variable most commonly associated with hepcidin from Day 14 to 180 (Table 2). Erythropoiesis (reticulocytes) was also an important determinant of hepcidin on Days 7 and 100. Interestingly, CRP had also an impact on hepcidin on Days 60 and 100.
Table 2.
Multiple linear regression of various parameters with hepcidin as the dependent variable at each time point after HCT (group, Hb, sTfR, reticulocytes, ferritin, transferrin saturation (TSAT) and CRP were included into the model).
Hepcidin is the key regulator of iron metabolism but has been little investigated in the context of HCT.4–7 Hepcidin peaked at Day 7 post transplant and then gradually decreased in the following three weeks without returning to pre-transplant levels.5 In another study,6 hepcidin levels at 3–5 months post transplant remained unchanged compared to (high) pre-transplant values. On the other hand, hepcidin response to erythropoietin therapy has been examined in healthy volunteers10 or chronic kidney disease10,11 in whom erythropoietin (EPO) elicited a rapid and persistent drop in serum hepcidin levels. Therefore, we decided to investigate the long-term kinetics of hepcidin after HCT in a group of patients participating in a clinical trial of post-transplant DA with and without intravenous iron therapy.8 In our study, hepcidin levels prior to HCT were not increased compared to healthy controls.9 This is in agreement with a previous study7 and is explained by the low transfusion rates in our lymphoma and myeloma patients before transplantation, contrarily to other studies investigating mostly polytransfused patients with acute leukemia or myelodysplastic syndromes.4–6 We also identified a hepcidin peak one week after transplantation. Whereas Kanda attributed this peak to inflammation because of a concomitant elevation of serum IL-6 levels (not measured in our study),5 and although CRP in our study also peaked at Day 7 (data not shown), we did not observe any correlation between hepcidin and CRP values.
Among factors associated with hepcidin regulation, erythropoietic activity and iron status are essential.1,3,12 We also identified erythropoiesis and iron as major determinants of serum hepcidin levels. The Day-7 peak (Figure 1A) could result from concomitant suppression of erythropoietic activity and elevated serum ferritin levels (due mainly to the drop in iron utilization from the bone marrow and inflammatory complications) (Figure 1C). However, we cannot exclude the possibility that ferritin increased because of iron retention in hepatocytes and macrophages following the hepcidin peak. The ensuing rapid hepcidin drop appears to correspond to fast recovery of erythropoiesis, as illustrated by the quick TSAT normalization (Figure 1D) and sTfR surge (Figure 1E), whereas serum ferritin decreased much slower. This rapid hepcidin decline is coherent with the week-long hepcidin suppression following a single EPO injection observed by Ashby10 in healthy volunteers. In addition, analyzing hepcidin relatively to its Day-28 (pre-DA) value (Figure 1B) clearly showed that patients receiving no DA had stable values while patients receiving DA experienced a marked drop corresponding to further stimulation of erythropoiesis, whereas TSAT and ferritin evolution remained superimposable in the 3 groups. Obviously, our observations also support the experimental evidence that suppression of hepcidin during anemia requires erythropoietic activity.13
Hepcidin values showed significant correlations with all preceding or subsequent values, suggesting that whatever the changes in erythropoietic activity, hepcidin remained under the influence of a less variable parameter, i.e. iron stores. The most robust associations were found between serum hepcidin and ferritin, whereas those with sTfR were less consistent, but the correlations were stronger prior to and away from the day of transplantation, when inflammatory complications had resolved and erythropoiesis recovered. Moreover, in the DA + iron group, hepcidin increased from Day 60 onwards (Figure 1B), in parallel to the evolution of ferritin and TSAT.
In summary, the evolution of serum hepcidin prior to and following autologous HCT in our study was determined by the levels of both erythropoietic activity and iron stores, while the effect of inflammation was less apparent.
Acknowledgments
FB is senior research associate of the National Fund for Scientific Research (FNRS) and AJ is (FNRS)-Televie PhD student. We are grateful to Yvette Fairon and Olivier Dengis for their excellent technical assistance.
Footnotes
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Ganz T. Hepcidin and iron regulation, 10 years later. Blood. 2011;117(17):4425–33 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nicolas G, Chauvet C, Viatte L, Danan JL, Bigard X, Devaux I, et al. The gene encoding the iron regulatory peptide hepcidin is regulated by anemia, hypoxia, and inflammation. J Clin Invest. 2002; 110(7):1037–44 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kroot JJ, Tjalsma H, Fleming RE, Swinkels DW. Hepcidin in human iron disorders: diagnostic implications. Clin Chem. 2011; 57(12):1650–69 [DOI] [PubMed] [Google Scholar]
- 4.Armand P, Kim HT, Rhodes J, Sainvil MM, Cutler C, Ho VT, et al. Iron overload in patients with acute leukemia or MDS undergoing myeloablative stem cell transplantation. Biol Blood Marrow Transplant. 2011;17(6):852–60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kanda J, Mizumoto C, Kawabata H, Tsuchida H, Tomosugi N, Matsuo K, et al. Serum hepcidin level and erythropoietic activity after hematopoietic stem cell transplantation. Haematologica. 2008; 93(10):1550–4 [DOI] [PubMed] [Google Scholar]
- 6.Eisfeld AK, Westerman M, Krahl R, Leiblein S, Liebert UG, Hehme M, et al. Highly Elevated Serum Hepcidin in Patients with Acute Myeloid Leukemia prior to and after Allogeneic Hematopoietic Cell Transplantation: Does This Protect from Excessive Parenchymal Iron Loading? Adv Hematol. 2011:491058 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kanda J, Mizumoto C, Kawabata H, Ichinohe T, Tsuchida H, Tomosugi N, et al. Clinical significance of serum hepcidin levels on early infectious complications in allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2009;15(8):956–62 [DOI] [PubMed] [Google Scholar]
- 8.Beguin Y, Maertens J, De Prijck B, Schots R, Seidel L, Bonnet C, et al. Darbepoetin-alfa and I.V. iron administration after autologous hematopoietic stem cell transplantation: A prospective multicenter randomized trial. Am J Hematol. 2013;88(12):990–6 [DOI] [PubMed] [Google Scholar]
- 9.Kroot JJ, Laarakkers CM, Geurts-Moespot AJ, Grebenchtchikov N, Pickkers P, van Ede AE, et al. Immunochemical and mass-spectrometry-based serum hepcidin assays for iron metabolism disorders. Clin Chem. 2010;56(10):1570–9 [DOI] [PubMed] [Google Scholar]
- 10.Ashby DR, Gale DP, Busbridge M, Murphy KG, Duncan ND, Cairns TD, et al. Erythropoietin administration in humans causes a marked and prolonged reduction in circulating hepcidin. Haematologica. 2010;95(3):505–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.van der Putten K, Jie KE, van den Broek D, Kraaijenhagen RJ, Laarakkers C, Swinkels DW, et al. Hepcidin-25 is a marker of the response rather than resistance to exogenous erythropoietin in chronic kidney disease/chronic heart failure patients. Eur J Heart Fail. 2010;12(9):943–50 [DOI] [PubMed] [Google Scholar]
- 12.Tanno T, Bhanu NV, Oneal PA, Goh SH, Staker P, Lee YT, et al. High levels of GDF15 in thalassemia suppress expression of the iron regulatory protein hepcidin. Nat Med. 2007;13(9):1096–101 [DOI] [PubMed] [Google Scholar]
- 13.Pak M, Lopez MA, Gabayan V, Ganz T, Rivera S. Suppression of hepcidin during anemia requires erythropoietic activity. Blood. 2006;108(12):3730–5 [DOI] [PMC free article] [PubMed] [Google Scholar]