

Abstract
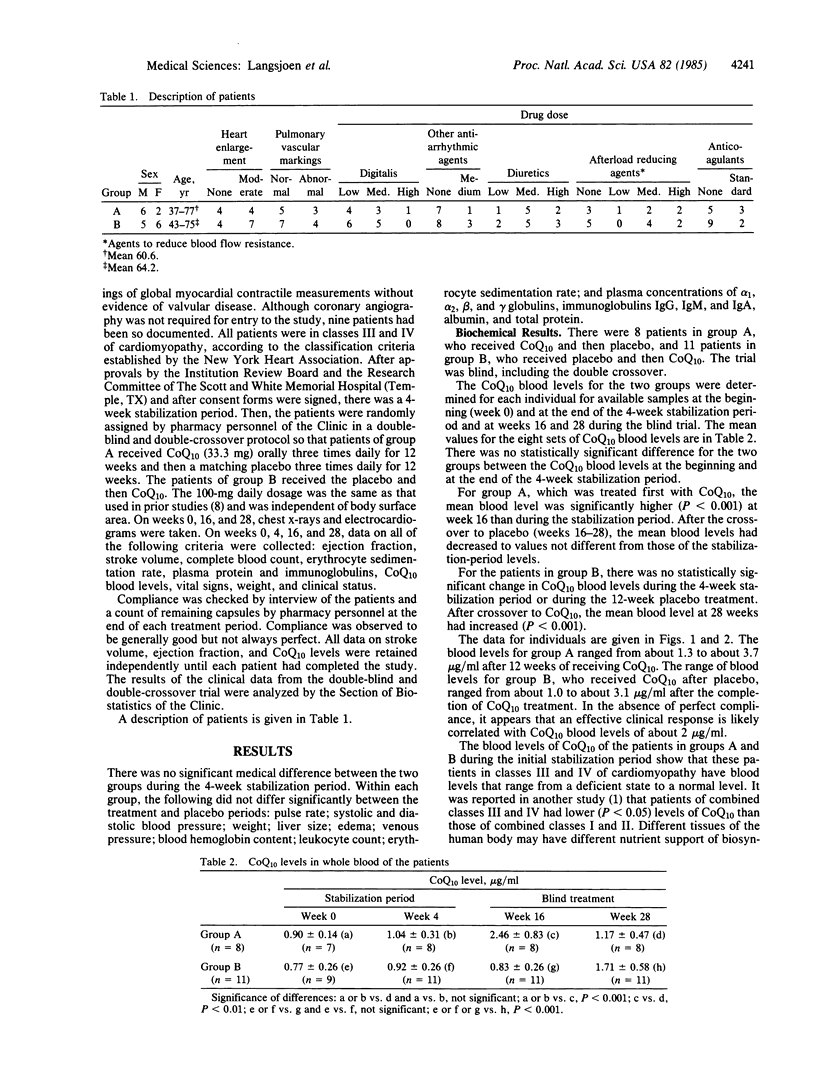
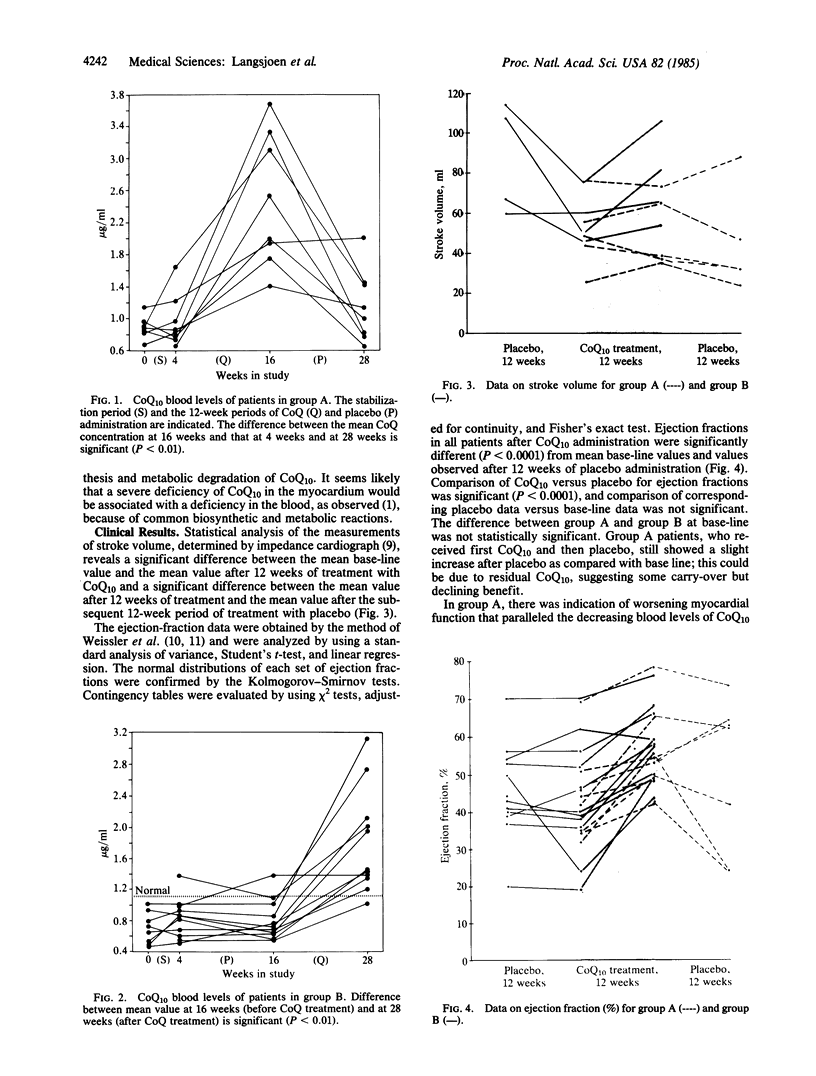
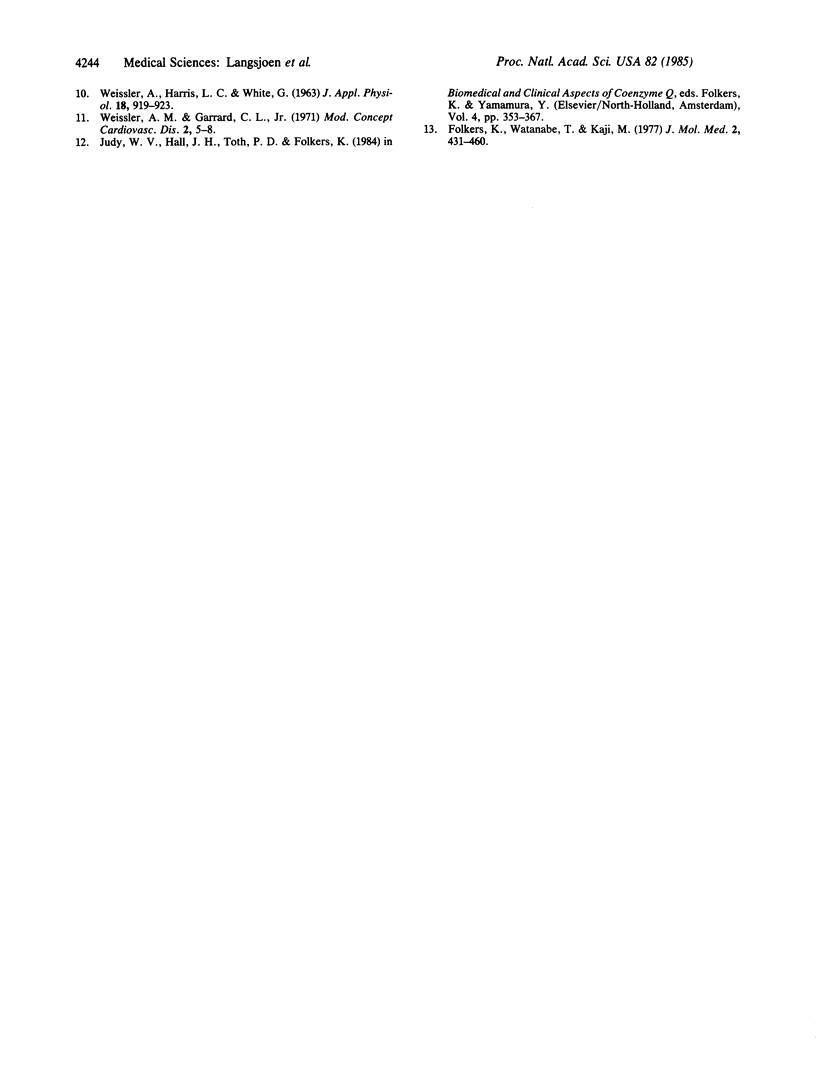
Coenzyme Q10 (CoQ10), a biochemically established redox component of respiration including the coupled mechanisms of electron transfer and oxidative phosphorylation, is naturally present in the human myocardium. A double-blind and double-crossover trial has been conducted by administering CoQ10 and a matching placebo orally to two groups of patients having class III or IV cardiomyopathy (classification according to criteria of the New York Heart Association). Group A received CoQ10 and then placebo; group B received placebo and then CoQ10. Blood levels of CoQ10 and cardiac function were determined at 0 and 4 weeks (control stabilization period) and at 16 and 28 weeks (after the 12-week CoQ/placebo-treatment periods). For group A, significant increases in CoQ10 blood levels and cardiac function occurred during CoQ10 treatment and then decreased during crossover to placebo. For group B, there was no change in CoQ10 blood levels and cardiac function during placebo treatment, but increases in both parameters occurred in crossover to CoQ10. These patients, steadily worsening and expected to die within 2 years under conventional therapy, generally showed an extraordinary clinical improvement, indicating that CoQ10 therapy might extend the lives of such patients. This improvement could be due to correction of a myocardial deficiency of CoQ10 and to enhanced synthesis of CoQ10-requiring enzymes.
Full text
PDF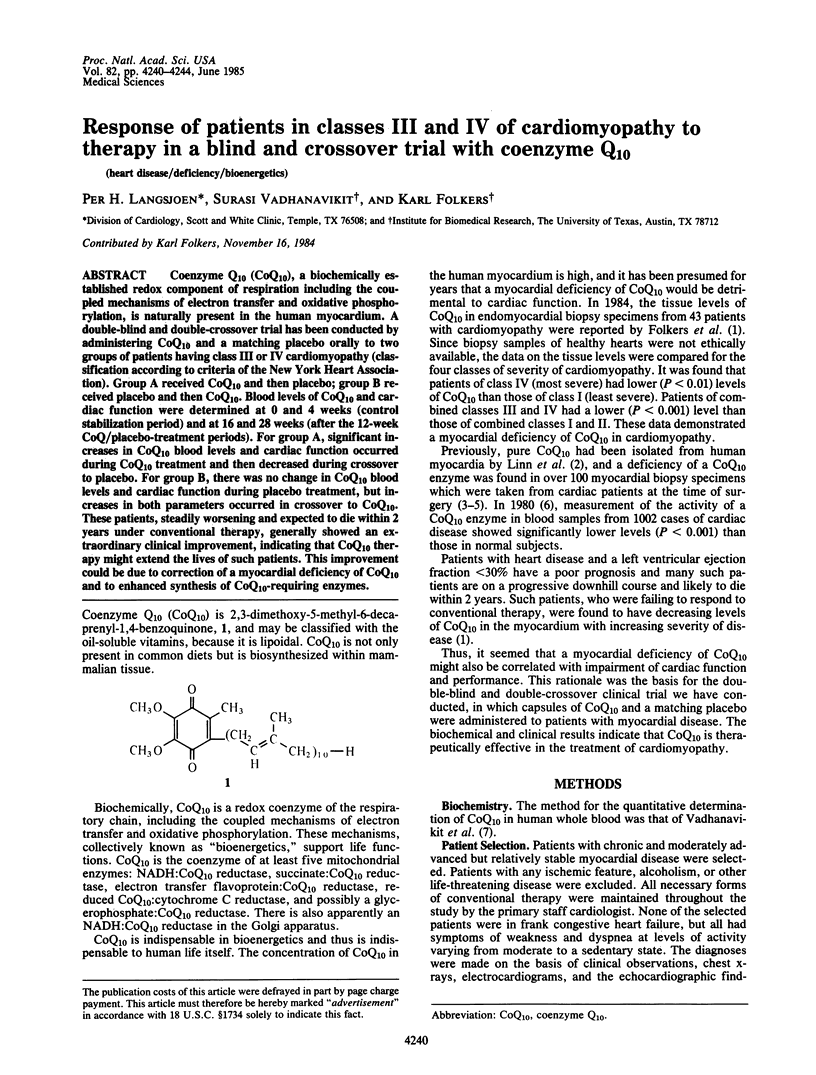

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Folkers K., Littarru G. P., Ho L., Runge T. M., Havanonda S., Cooley D. Evidence for a deficiency of coenzyme Q10 in human heart disease. Int Z Vitaminforsch. 1970;40(3):380–390. [PubMed] [Google Scholar]
- Folkers K., Vadhanavikit S., Mortensen S. A. Biochemical rationale and myocardial tissue data on the effective therapy of cardiomyopathy with coenzyme Q10. Proc Natl Acad Sci U S A. 1985 Feb;82(3):901–904. doi: 10.1073/pnas.82.3.901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kubicek W. G., From A. H., Patterson R. P., Witsoe D. A., Castaneda A., Lillehei R. C., Ersek R. Impedance cardiography as a noninvasive means to monitor cardiac function. J Assoc Adv Med Instrum. 1970 Mar-Apr;4(2):79–84. [PubMed] [Google Scholar]
- Littarru G. P., Ho L., Folkers K. Deficiency of coenzyme Q 10 in human heart disease. II. Int J Vitam Nutr Res. 1972;42(3):413–434. [PubMed] [Google Scholar]
- Littaru G. P., Ho L., Folkers K. Deficiency of coenzyme Q 10 in human heart disease. I. Int J Vitam Nutr Res. 1972;42(2):291–305. [PubMed] [Google Scholar]
- WEISSLER A. M., HARRIS L. C., WHITE G. D. LEFT VENTRICULAR EJECTION TIME INDEX IN MAN. J Appl Physiol. 1963 Sep;18:919–923. doi: 10.1152/jappl.1963.18.5.919. [DOI] [PubMed] [Google Scholar]
- Weissler A. M., Garrard C. L., Jr Systolic time intervals in cardiac disease (II). Mod Concepts Cardiovasc Dis. 1971 Feb;40(2):5–8. [PubMed] [Google Scholar]