

Abstract
Penile extracorporeal low-intensity shock wave therapy (LIST) to the penis has recently emerged as a novel and promising modality in the treatment of erectile dysfunction (ED). LIST has angiogenic properties and stimulates neovascularization. If applied to the corpora cavernosa, LIST can improve penile blood flow and endothelial function. In a series of clinical trials, including randomized double-blind sham-controlled studies, LIST has been shown to have a substantial effect on penile hemodynamics and erectile function in patients with vasculogenic ED. LIST is effective in patients who are responsive to phosphodiesterase 5 inhibitors (PDE5i) and can also convert PDE5i nonresponders to responders. The response to LIST wanes gradually over time, and after 2 years, about half of the patients maintain their function. Extensive research is needed to understand the effect of LIST on erectile tissue, to modify the treatment protocol to maximize its outcomes, and to identify the patients who will benefit the most from this treatment.
Keywords: Erectile dysfunction, Penile, Shockwave treatment, Therapy
INTRODUCTION
Great advances in the understanding and treatment of erectile dysfunction (ED) have been made in the past two decades. Most patients suffering from ED respond to the available options for treatment, including oral phosphodiesterase type 5 inhibitors (PDE5i) and intracavernosal injections of vasodilating agents. However, these medications are unable to alter the underlying pathophysiology of the erectile mechanism. They are usually taken on demand, prior to the sexual act, and do not improve spontaneous erections [1]. Therefore, a need exists for an effective new treatment concept that would have a durable effect on spontaneous erectile function. Recently, a promising modality was introduced: the application of low-intensity extracorporeal shock wave therapy (LIST) on the penis [2].
Shock waves are acoustic waves that generate a pressure impulse and that carry energy when propagating through a medium. The degree of focus can be modulated noninvasively, resulting in variable concentration of energy at a desired location [3]. When shock waves are applied to an organ, the focused waves interact with the targeted deep tissues and act as transient micromechanical forces that initiate several biological changes [4]. Extracorporeal shock wave therapy has been clinically examined and applied in various medical fields. High-intensity shock wave therapy is used for lithotripsy because of its focused mechanical destructive nature. Medium-intensity shock waves have been shown to have anti-inflammatory properties and are used for treating a wide range of orthopedic conditions, such as nonunion fractures, tendonitis, and bursitis. Low-intensity shock waves probably have angiogenic properties and are used in the management of chronic wounds, peripheral neuropathy, and in cardiac ischemic tissue [1,2,5,6].
When LIST is applied to an organ, the relatively weak yet focused shock waves interact with the targeted deep tissues where they cause mechanical stress and microtrauma, also known as shear stress [3]. This shear force then triggers a chain of events that cause the release of angiogenic factors inducing neovascularization of the affected tissues and enhancing the blood flow. Extrapolation of these findings to ED has led to the assumption that if applied to the corpora cavernosa, LIST could improve penile blood flow and endothelial function by stimulating angiogenesis in the penis [7]. This review summarizes the effect of LIST on erectile tissue as well as the clinical evidence of its effect in patients with vasculogenic ED.
POTENTIAL MECHANISM OF SHOCK WAVE THERAPY
Research on the biological changes that result from LIST has mainly been focused on angiogenesis and local neovascularization. More than a decade ago, Wang et al. [8] revealed that LIST stimulates the expression of angiogenesis-related growth factors, such as endothelial nitric oxide synthase (NOS), vascular endothelial growth factor (VEGF), and endothelial cell proliferation factors, e.g., proliferating cell nuclear antigen (PCNA). This group also reported that LIST induces neovascularization and cell proliferation. This effect is evident 4 weeks after treatment and persists for more than 12 weeks [8]. Moreover, previous studies on transgenic mice revealed an up-regulation of VEGF receptor 2, which is considered a primary mediator of angiogenic signaling. Quantitative immuno-histological studies evaluating ischemic tissue vessel formation showed higher vessel densities in the shock wave-treated groups [6,9,10,11,12].
In recent years, LIST has also been studied in regard to its effect on stem cell recruitment in tissue repair. Stem cells and progenitor cells have the ability to divide and differentiate into specialized cell types. Their key role in the neovascularization of ischemic tissues was widely studied in recent years [13]. One example is the circulating progenitor cells (CPCs). During acute ischemia, the release of chemoattractant factors (i.e., VEGF) acts as a homing factor for CPCs that may contribute to the ongoing endothelial repair [14]. Aicher et al. [5] investigated the effect of LIST on the homing of infused human CPCs in rats with chronic hind limb ischemia. In their study, LIST-treated ischemic muscles attracted significantly more labeled CPCs than did the untreated muscles. The treatment significantly increased the blood flow in the ischemic muscles. Nishida et al. [6] studied LIST in a porcine model of ischemia-induced myocardial dysfunction and found that LIST significantly up-regulated VEGF expression in ischemic myocardium and improved regional myocardial blood flow and left ventricular ejection fraction. Further studies have also demonstrated beneficial effects of LIST on left ventricle remodeling in pigs with experimentally induced myocardial infarction [15] and myocardial ischemia-reperfusion injury [16].
CLINICAL APPLICATIONS OF LIST
Encouraging results in animal model have set the ground for future studies in humans. Several studies have shown positive effects of LIST in human patients with severe ischemic heart disease. Kikuchi et al. [17] reported that LIST improved the ejection fraction and stroke volume and significantly improved chest pain after a 6-minute walk test. Similar results have also been reported by other groups [18,19,20] in patients with severe coronary artery disease and refractory angina to whom LIST was applied. Following the promising results in patients with ischemic heart disease, other reports on the capability of LIST were published with positive results on a wide range of ischemic wounds and ulcers [21,22,23,24].
LIST FOR ED
Because one of the underlying functional causes of ED is poor cavernosal arterial blood flow, it has been suggested that induction of neovascularization by LIST could improve cavernosal arterial flow, which in turn would improve erectile function [13]. The first study of the efficacy of LIST for ED was conducted by Vardi et al. [2] in 2010. In this pilot study, Vardi et al. [2] applied LIST to 20 middle-aged men with mild to moderate vasculogenic ED who responded well to the use of PDE5i. The treatment protocol was based on the described methodology used in patients with cardiovascular disease [17] with modifications according to anatomical differences. The main challenge presented by the authors was to apply shock waves to the whole area of the corpora cavernosa, including the crus. Another challenge was to adapt the shock wave delivery probe to the anatomy of the penis because the corpora cavernosa lies immediately under the penile skin. The protocol consisted of two treatment sessions per week for 3 weeks, a 3-week no-treatment interval, and a second 3-week treatment period of two treatment sessions per week. Each session comprised the application of 300 shock waves (energy intensity of 0.09 mJ/mm2) to each of five different sites: three along the penile shaft and two at the crura (Fig. 1). The results showed that 1 month after treatment, erectile function improved in 15 men (75%). An increase by more than five points in the International Index of Erectile Function Erectile Function (IIEF-EF) domain score was noted in 14 men and an increase of more than 10 points was noted in 7 men. The average increase in the IIEF-EF domain score was 7.4 points. Furthermore, erectile function and penile blood flow were measured by using nocturnal penile tumescence (NPT) and flow-mediated dilation methodology (FMD) of the penis. In the 15 men who responded to LIST, all NPT parameters improved as recorded by significant increases in the duration of the erections and penile rigidity. Penile blood flow also improved significantly at the 1-month follow-up examination. At the 6-month follow-up visit, 10 men reported that they still had spontaneous erections and did not require PDE5i support.
FIG. 1.
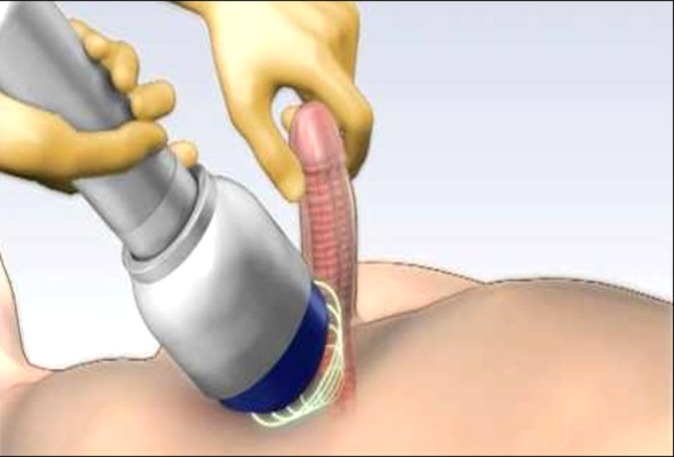
The shock waves are delivered through the applicator covering the corpora cavernosa of the penis along the penile shaft and the crura.
Following these impressive preliminary clinical results, the effect of LIST on erectile function was examined in an animal model. Several groups investigated the effects of LIST on erectile function in diabetes mellitus rats, using the changes in the intracavernosal pressure following electrostimulation of the cavernous nerve to assess erectile function. Qiu et al. [25] found that erectile function was significantly decreased in all diabetic rats, but this effect was less evident in the LIST group. Additionally, histological analysis revealed an abundant amount of nNOS-containing nerves, endothelial and smooth muscle cells, and mesenchymal stem cells (MSCs) in the LIST group compared with untreated diabetic rats. Such findings support the idea that the underlying mechanism of the therapeutic action of LIST is the recruitment of MSCs, which was first postulated by Chen et al. [26] almost a decade before. Two more groups have recently examined the effect of extracorporeal shock waves on nerve stimulation-induced erection in rats. Chen and Chang [23] and Liu et al. [24] demonstrated that shock wave energy improved erectile function as well as pathological changes in the erectile tissue of diabetic rats.
Vardi and colleagues [13] further extended their clinical study in vasculogenic ED patients and examined LIST as a possible treatment for patients with severe ED who responded poorly to PDE5i therapy. The aim of this second study was to investigate the ability of LIST to convert nonresponders to PDE5i therapy to PDE5i responders so that they were able to achieve satisfactory erections for vaginal penetration. This study included 29 men who had multiple cardiovascular disease risk factors, cardiovascular disease, and diabetes mellitus and who did not respond to oral PDE5i therapy. The study results showed that 3 months after the completion of the LIST protocol, the IIEF-EF domain scores improved by at least five points in 76% of men, and the mean IIEF-EF domain score increased by 10 points. Overall, 72% were converted to PDE5i responders. This increase in the IIEF-EF domain scores was also accompanied by improvements in cavernosal blood flow and penile endothelial function as measured by FMD. One of the key issues addressed in these studies was the participants' subjective opinions regarding their sexual function. At screening, all patients were thoroughly interviewed about their medical and sexual history. The total IIEF questionnaire, the Erection Hardness Scale (EHS), the Quality of Erection, the Self-Esteem and Relationship questionnaires, and the Clinical Global Impression of Change rating scale were used to subjectively determine the sexual function of each patient. In these studies, a significant correlation between the subjective assessment of sexual function by use of validated sexual function questionnaires and the objective results of penile blood flow and endothelial function was found. Most importantly, none of the men in either study reported treatment-associated pain or any adverse events during or after the treatment.
A prospective, randomized, double-blind, sham-controlled study was designed to confirm these positive outcomes. Sixty ED patients were treated in a similar fashion [27]. The probe used for the sham treatment looked identical to the active probe and made the same noise yet did not produce any shock wave energy. The patients in the active treatment group had significantly higher IIEF-EF domain scores as well as improved penile endothelial function compared with the sham-treated men. The overall success rate of LIST was later analyzed by Gruenwald et al. [28]. In this cohort of 184 patients from various studies, the mean IIEF-EF domain scores increased after LIST by 7 points with the greatest improvement occurring in men with severe ED. Moreover, further analysis revealed that the increases in the IIEF-EF domain scores in the men who were PDE5i nonresponders were higher than in the men who were PDE5i responders (7.52 points vs. 5.7 points).
FURTHER CLINICAL STUDIES
Another study recently introduced by Vardi et al. [29] evaluated the effect of LIST after 2 years of follow-up and reported that the beneficial response that was achieved immediately after therapy had not faded in about 50% of the patients. The success rate after 2 years was lower mainly in patients with severe ED and diabetes. The same group also reported their preliminary results regarding a second round of penile LIST. They aimed to discover whether an additional LIST protocol would be therapeutically beneficial in patients whose first round of treatment was unsuccessful. Thirty patients were included in this study, 22 of whom (73.3%) had severe ED. Their median baseline IIEF-EF score before treatment was 8 and improved to a median of 10 points after the first treatment protocol. In the "second round" protocol, LIST was effective in approximately half the patients, and the median IIEF-EF score increased from 8 to 13.5 points, demonstrating that there are patients who probably need additional exposure to shock wave energy in order to respond [30].
Several other groups have recently studied penile LIST with different shock wave machines. Preliminary results with a machine that produced linear shock waves at 4 anatomical areas were presented by Reisman et al. [31]. In this study, 82% out of 57 patients had a successful treatment, with the average IIEF-EF domain score increase of 8 points. Similar results were presented by Lacono [32]. The preliminary results of a third shock wave machine were presented by Lund [33]. In a prospective, randomized, blinded, placebo-controlled study, they demonstrated that LIST significantly improved the EHS in more than 50% of patients, allowing full sexual intercourse without medication.
DISCUSSION
During the past 2 decades, the treatment options for ED have greatly expanded and include PDE5i, intracavernosal injections, and penile prostheses. Despite the efficacy and safety profiles of the current treatments, most of them are "on-demand" therapies, and their effect is essentially time limited. The search for a better treatment that enables men to regain spontaneous sexual activity is the next step in ED management. Although investigations in this direction, such as stem cell therapy or gene therapy, are ongoing, no significant progress has yet been made, and the quest for a cure of ED is still premature.
The data presented here demonstrate that LIST of the corpora cavernosa is a novel therapeutic concept. LIST may have a fundamental effect on penile endothelial function, increasing penile blood flow, and improving erectile function and consequently sexual satisfaction. Up to 60% to 70% of ED patients who used to rely on PDE5i can achieve adequate erection without medications after LIST, and a similar rate of patients who have ceased to respond to PDE5i can again benefit from the PDE5i effect after treatment.
Although the efficacy and safety of LIST have been established, evidence is still limited.
To date, most clinical studies originate from one center and the total number of treated patients is relatively low. The current protocol, shared by most studies, is empirical and preliminary: 12 twice-weekly sessions of shock waves, a 3-week break in the middle of the protocol, 1,500 shock waves in every session, and five target foci on the penis. Extensive research is needed to discover the optimal treatment protocol and the modifications needed to improve efficacy and durability. Additionally, the target population, that is, the patients who will benefit most from LIST, has not yet been adequately defined. Finally, there are insufficient data on the mechanism of action of LIST at the cellular and histological level. Basic research is urgently required to explore and understand the mechanism of action of LIST on erectile tissue.
CONCLUSIONS
LIST is a promising novel therapeutic modality for restoring erectile function in men with vasculogenic ED. It is a safe and nonpainful treatment with a long-lasting effect on erectile function. Additional well-designed, randomized, large-scale studies are necessary to confirm these findings and to outline the optimal treatment protocol and the suitable candidates.
Footnotes
Yoram Vardi is a consultant of Medispec Ltd.
References
- 1.Gruenwald I, Appel B, Kitrey ND, Vardi Y. Shockwave treatment of erectile dysfunction. Ther Adv Urol. 2013;5:95–99. doi: 10.1177/1756287212470696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vardi Y, Appel B, Jacob G, Massarwi O, Gruenwald I. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction. Eur Urol. 2010;58:243–248. doi: 10.1016/j.eururo.2010.04.004. [DOI] [PubMed] [Google Scholar]
- 3.Seidl M, Steinbach P, Worle K, Hofstadter F. Induction of stress fibres and intercellular gaps in human vascular endothelium by shock-waves. Ultrasonics. 1994;32:397–400. doi: 10.1016/0041-624x(94)90111-2. [DOI] [PubMed] [Google Scholar]
- 4.Qureshi AA, Ross KM, Ogawa R, Orgill DP. Shock wave therapy in wound healing. Plast Reconstr Surg. 2011;128:721e–727e. doi: 10.1097/PRS.0b013e318230c7d1. [DOI] [PubMed] [Google Scholar]
- 5.Aicher A, Heeschen C, Sasaki K, Urbich C, Zeiher AM, Dimmeler S. Low-energy shock wave for enhancing recruitment of endothelial progenitor cells: a new modality to increase efficacy of cell therapy in chronic hind limb ischemia. Circulation. 2006;114:2823–2830. doi: 10.1161/CIRCULATIONAHA.106.628623. [DOI] [PubMed] [Google Scholar]
- 6.Nishida T, Shimokawa H, Oi K, Tatewaki H, Uwatoku T, Abe K, et al. Extracorporeal cardiac shock wave therapy markedly ameliorates ischemia-induced myocardial dysfunction in pigs in vivo. Circulation. 2004;110:3055–3061. doi: 10.1161/01.CIR.0000148849.51177.97. [DOI] [PubMed] [Google Scholar]
- 7.Lei H, Liu J, Li H, Wang L, Xu Y, Tian W, et al. Low-intensity shock wave therapy and its application to erectile dysfunction. World J Mens Health. 2013;31:208–214. doi: 10.5534/wjmh.2013.31.3.208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wang CJ, Wang FS, Yang KD, Weng LH, Hsu CC, Huang CS, et al. Shock wave therapy induces neovascularization at the tendon-bone junction: a study in rabbits. J Orthop Res. 2003;21:984–989. doi: 10.1016/S0736-0266(03)00104-9. [DOI] [PubMed] [Google Scholar]
- 9.Stojadinovic A, Elster EA, Anam K, Tadaki D, Amare M, Zins S, et al. Angiogenic response to extracorporeal shock wave treatment in murine skin isografts. Angiogenesis. 2008;11:369–380. doi: 10.1007/s10456-008-9120-6. [DOI] [PubMed] [Google Scholar]
- 10.Yan X, Zeng B, Chai Y, Luo C, Li X. Improvement of blood flow, expression of nitric oxide, and vascular endothelial growth factor by low-energy shockwave therapy in random-pattern skin flap model. Ann Plast Surg. 2008;61:646–653. doi: 10.1097/SAP.0b013e318172ba1f. [DOI] [PubMed] [Google Scholar]
- 11.Oi K, Fukumoto Y, Ito K, Uwatoku T, Abe K, Hizume T, et al. Extracorporeal shock wave therapy ameliorates hindlimb ischemia in rabbits. Tohoku J Exp Med. 2008;214:151–158. doi: 10.1620/tjem.214.151. [DOI] [PubMed] [Google Scholar]
- 12.Mittermayr R, Antonic V, Hartinger J, Kaufmann H, Redl H, Teot L, et al. Extracorporeal shock wave therapy (ESWT) for wound healing: technology, mechanisms, and clinical efficacy. Wound Repair Regen. 2012;20:456–465. doi: 10.1111/j.1524-475X.2012.00796.x. [DOI] [PubMed] [Google Scholar]
- 13.Gruenwald I, Appel B, Vardi Y. Low-intensity extracorporeal shock wave therapy: a novel effective treatment for erectile dysfunction in severe ED patients who respond poorly to PDE5 inhibitor therapy. J Sex Med. 2012;9:259–264. doi: 10.1111/j.1743-6109.2011.02498.x. [DOI] [PubMed] [Google Scholar]
- 14.Hill JM, Zalos G, Halcox JP, Schenke WH, Waclawiw MA, Quyyumi AA, et al. Circulating endothelial progenitor cells, vascular function, and cardiovascular risk. N Engl J Med. 2003;348:593–600. doi: 10.1056/NEJMoa022287. [DOI] [PubMed] [Google Scholar]
- 15.Uwatoku T, Ito K, Abe K, Oi K, Hizume T, Sunagawa K, et al. Extracorporeal cardiac shock wave therapy improves left ventricular remodeling after acute myocardial infarction in pigs. Coron Artery Dis. 2007;18:397–404. doi: 10.1097/MCA.0b013e328089f19b. [DOI] [PubMed] [Google Scholar]
- 16.Ito Y, Ito K, Shiroto T, Tsuburaya R, Yi GJ, Takeda M, et al. Cardiac shock wave therapy ameliorates left ventricular remodeling after myocardial ischemia-reperfusion injury in pigs in vivo. Coron Artery Dis. 2010;21:304–311. doi: 10.1097/mca.0b013e32833aec62. [DOI] [PubMed] [Google Scholar]
- 17.Kikuchi Y, Ito K, Ito Y, Shiroto T, Tsuburaya R, Aizawa K, et al. Double-blind and placebo-controlled study of the effectiveness and safety of extracorporeal cardiac shock wave therapy for severe angina pectoris. Circ J. 2010;74:589–591. doi: 10.1253/circj.cj-09-1028. [DOI] [PubMed] [Google Scholar]
- 18.Yang P, Guo T, Wang W, Peng YZ, Wang Y, Zhou P, et al. Randomized and double-blind controlled clinical trial of extracorporeal cardiac shock wave therapy for coronary heart disease. Heart Vessels. 2013;28:284–291. doi: 10.1007/s00380-012-0244-7. [DOI] [PubMed] [Google Scholar]
- 19.Vasyuk YA, Hadzegova AB, Shkolnik EL, Kopeleva MV, Krikunova OV, Iouchtchouk EN, et al. Initial clinical experience with extracorporeal shock wave therapy in treatment of ischemic heart failure. Congest Heart Fail. 2010;16:226–230. doi: 10.1111/j.1751-7133.2010.00182.x. [DOI] [PubMed] [Google Scholar]
- 20.Wang Y, Guo T, Ma TK, Cai HY, Tao SM, Peng YZ, et al. A modified regimen of extracorporeal cardiac shock wave therapy for treatment of coronary artery disease. Cardiovasc Ultrasound. 2012;10:35. doi: 10.1186/1476-7120-10-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Saggini R, Figus A, Troccola A, Cocco V, Saggini A, Scuderi N. Extracorporeal shock wave therapy for management of chronic ulcers in the lower extremities. Ultrasound Med Biol. 2008;34:1261–1271. doi: 10.1016/j.ultrasmedbio.2008.01.010. [DOI] [PubMed] [Google Scholar]
- 22.Larking AM, Duport S, Clinton M, Hardy M, Andrews K. Randomized control of extracorporeal shock wave therapy versus placebo for chronic decubitus ulceration. Clin Rehabil. 2010;24:222–229. doi: 10.1177/0269215509346083. [DOI] [PubMed] [Google Scholar]
- 23.Chen KK, Chang LS. The effect of extracorporeal shock wave on cavernous nerve stimulation-induced intracavernous pressure increase in the rat [abstract 816] J Urol. 2013;189:e335. [Google Scholar]
- 24.Liu J, Li GY, Zhou F, Wang L, Li HX, Xin ZC. Efficacy and possible mechanism of extracorporeal shock wave therapy on streptozotocin induced diabetic erectile dysfunction rats model [abstract 1028] J Urol. 2013;189:e421. [Google Scholar]
- 25.Qiu X, Lin G, Xin Z, Ferretti L, Zhang H, Lue TF, et al. Effects of low-energy shockwave therapy on the erectile function and tissue of a diabetic rat model. J Sex Med. 2013;10:738–746. doi: 10.1111/jsm.12024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chen YJ, Wurtz T, Wang CJ, Kuo YR, Yang KD, Huang HC, et al. Recruitment of mesenchymal stem cells and expression of TGF-beta 1 and VEGF in the early stage of shock wave-promoted bone regeneration of segmental defect in rats. J Orthop Res. 2004;22:526–534. doi: 10.1016/j.orthres.2003.10.005. [DOI] [PubMed] [Google Scholar]
- 27.Vardi Y, Appel B, Kilchevsky A, Gruenwald I. Does low intensity extracorporeal shock wave therapy have a physiological effect on erectile function? Short-term results of a randomized, double-blind, sham controlled study. J Urol. 2012;187:1769–1775. doi: 10.1016/j.juro.2011.12.117. [DOI] [PubMed] [Google Scholar]
- 28.Gruenwald I, Kitrey ND, Appel B, Vardi Y. Low-intensity extracorporeal shock wave therapy in vascular disease and erectile dysfunction: theory and outcomes. Sex Med Rev. 2013;1:83–90. doi: 10.1002/smrj.9. [DOI] [PubMed] [Google Scholar]
- 29.Vardi Y, Appel B, Kitrey ND, Massarwa O, Gruenwald I. Low-intensity shockwave treatment for ED - long term follow up of 2 years [abstract]; The 29th European Association of Urology Annual Congress; 2014 Apr 11-14; Stockholm, Sweden. Arnhem: European Association of Urology; 2014. [Google Scholar]
- 30.Vardi Y, Appel B, Kitrey ND, Massarwa O, Gruenwald I. Additional shockwave treatment improves erectile function in patients with poor response to the standard shockwave protocol [abstract]; The 29th European Association of Urology Annual Congress; 2014 Apr 11-14; Stockholm, Sweden. Arnhem: European Association of Urology; 2014. [Google Scholar]
- 31.Reisman Y, Hind A, Varaneckas A, Motil I. Efficacy and Safety of Linear Focused Shockwaves for Erectile Dysfunction (RENOVA) - A Second Generation Technolog [abstract]; The 12th congress of the Latin American Society for Sexual Medicine; 2013 Aug 28-31; Cancun, Mexico. Latin American Society for Sexual Medicine; 2013. [Google Scholar]
- 32.Lacono F. Low intensity shock wave (LISW) treatment (Renova) in order to improve male sexual function: a preliminary data on 42 patients [abstract]; The 16th Congress of the European Society for Sexual Medicine; 2014 Jan 29-Feb. 1; Istanbul, Turkey. European Society for Sexual Medicine; 2014. [Google Scholar]
- 33.Lund L. Treatment of erectile dysfunction with extracorporeal shockwave therapy (ESWT). A prospective, randomised, double-blind, placebo-controlled study [abstract]; The 16th Congress of the European Society for Sexual Medicine; 2014 Jan 29-Feb. 1; Istanbul, Turkey. European Society for Sexual Medicine; 2014. [Google Scholar]