

Abstract
BACKGROUND:
Anaphylaxis is characterized by acute episodes of potentially life-threatening symptoms that are often treated in the emergency setting. Current guidelines recommend: 1) quick diagnosis using standard criteria; 2) first-line treatment with epinephrine; and 3) discharge with a prescription for an epinephrine auto-injector, written instructions regarding long-term management, and a referral (preferably, allergy) for follow-up. However, studies suggest low concordance with guideline recommendations by emergency medicine (EM) providers. The study aimed to evaluate how emergency departments (EDs) in the United States (US) manage anaphylaxis in relation to guideline recommendations.
METHODS:
This was an online anonymous survey of a random sample of EM health providers in US EDs.
RESULTS:
Data analysis included 207 EM providers. For respondent EDs, approximately 9% reported using agreed-upon clinical criteria to diagnose anaphylaxis; 42% reported administering epinephrine in the ED for most anaphylaxis episodes; and <50% provided patients with a prescription for an epinephrine auto-injector and/or an allergist referral on discharge. Most provided some written materials, and follow-up with a primary care clinician was recommended.
CONCLUSIONS:
This is the first cross-sectional survey to provide “real-world” data showing that practice in US EDs is discordant with current guideline recommendations for the diagnosis, treatment, and follow-up of patients with anaphylaxis. The primary gaps are low (or no) utilization of standard criteria for defining anaphylaxis and inconsistent use of epinephrine. Prospective research is recommended.
KEY WORDS: Anaphylaxis, Guidelines, Epinephrine (adrenaline), Allergic reaction, Life-threatening reaction, Emergency department, Epinephrine autoinjector, Self-injectable epinephrine
INTRODUCTION
Anaphylaxis is a condition that crosses medical boundaries. Though usually allergic in nature, the acute anaphylaxis episode is most frequently treated by an emergency medicine (EM) health professional and not an allergy specialist. For the US, a review of anaphylaxis in children and adolescents over a 6-year period reported that 71% of cases were treated at an emergency department (ED) or urgent care center.[1] The number of annual ED visits for anaphylaxis in the US is estimated to be as high as 500 000.[2]
Despite the primary role of EM in the initial management of anaphylaxis, the majority of reports about anaphylaxis including management guidelines and practice parameters are published in allergy journals.[3–7] In the past decade, these documents have been published by multiple subspecialty groups (e.g., allergy, emergency medicine, pediatrics) in an effort to work together to develop clinical criteria for diagnosing anaphylaxis and specific recommendations for its management. Nonetheless, on a global level, evidence continues to point to both practice and knowledge gaps for emergency health professionals, including low concordance with guideline-recommended treatment, even in patients who were clearly diagnosed with anaphylaxis by medical record or by ICD-9 code.[2,8–17]
To date, only one study has evaluated the implementation of anaphylaxis guideline recommendations.[16] That study, performed using the transnational anaphylaxis registry of Germany, Austria, and Switzerland, confirmed major discrepancies in treatment and follow-up and recommended a revised approach to management, including training and education. No data exist for the US.
In an effort to better understand how US EDs use anaphylaxis guidelines, we conducted an online survey of US ED health professionals focusing on the three components of management common to all guidance documents:
Diagnosis. Are the current clinical criteria for identifying anaphylaxis as published in the National Institutes of Allergy and Infectious Diseases/Food Allergy and Anaphylaxis Network (NIAID/FAAN) 2nd Symposium,[5] the 2010 US Practice Parameters,[4] or the World Allergy Organization (WAO) Guidelines,[3,6] being applied in clinical practice?
Treatment. Is epinephrine being used as the first-line agent for treating all episodes of anaphylaxis-even those with mild or single system symptoms and those in which the diagnosis is only suspected?[3–7,18]
Discharge. Do ED discharge plans meet current guideline recommendations (i.e., a prescription for epinephrine, written instructions for self-management, and a physician-preferably, allergist-referral for follow-up)?[3–7]
METHODS
An on-line survey was conducted between March 19 and April 30, 2012 as a potential pilot project for a more robust evaluation to be developed. The online Survey Monkey tool (SurveyMonkey.com, LLC; Palo Alto, CA) was selected for its simplicity, scalability, and relatively quick data capture and analysis.
The survey included dichotomous and nominal-polytomous closed-ended questions, with additional open-ended responses invited for some queries. The survey questions were developed initially during a discussion at a multidisciplinary roundtable meeting, Anaphylaxis in Emergency Medicine (July 2011; Chicago, IL) that included physicians, nurse practitioners, physician assistants, and pharmacists involved in EM.[17] Following some revision, the questions were approved by the authors, who were among the roundtable attendees.
Non-targeted distribution methods were utilized and were conducted independently of the authors and sponsors. EM providers were invited to participate in the survey by notification posted on the website of the Journal of Emergency Medicine (Elsevier, Inc.). Additionally, a randomly sampled national group of 3000 hospital-based EM physicians, nurse practitioners, and physician assistants received an email invitation to participate from a third party provider (List Information Service Technology, Inc., Midland Park, NJ). The first 150 respondents received a stipend of $50. Subsequent respondents were not incentivized or remunerated.
Data analysis
Responses to multiple-choice questions were managed by SurveyMonkey and were directly exported to an Excel spreadsheet (Microsoft Corp., Redmond, WA). The data were deemed evaluable if the respondent was from a US ED and completed at least 80% of the questions.
Data from the multiple-choice questions were evaluated by response count and response percentage. Not all respondents answered all questions; therefore, the results were calculated according to responses to a particular question.
Open-ended responses were reviewed individually by two of the authors. The survey can be accessed at https://www.surveymonkey.com/s/anaphylaxispracticegaps.
RESULTS
A total of 207 EM health professionals responded to the survey, and 166 (80.2%), representing 26 states, completed all questions: 140 physicians, 18 physician assistants, 7 nurses (including five nurse practitioners), and one who did not identify his/her practice.
Diagnosis
Almost 90% of respondents reported that their EDs did not use a written definition of anaphylaxis (Figure 1). Thirty-two of 196 (16.3%) respondents stated that their EDs used a definition based on an established set of criteria (question 2): 17 of these respondents (8.9% of the total) reported using definitions based on consensus criteria recommended by the NIAID/FAAN 2nd Symposium[5] (1.6%), the 2010 US Practice Parameters[4] (4.2%), or the WAO guidelines[3,6] (3.1%) as the source of their definition.
Figure 1.
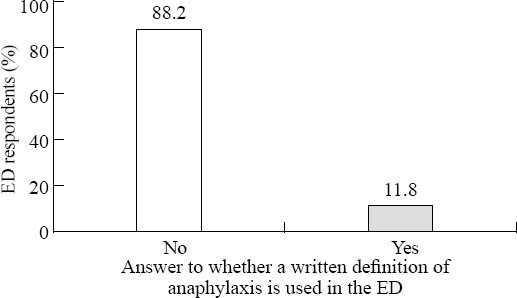
Use of a written definition of anaphylaxis in US EDs. Respondents answered the question: Does your department have a written definition of anaphylaxis? (n=204).
Treatment
When asked whether their ED used a standard protocol for treating patients with anaphylaxis (question 3), 63 of 196 respondents (31.8%) said yes, and 118 (59.6%) said no. The remainder did not know.
Eighty-four of 196 respondents (42.4%) reported that in their EDs the majority of patients (defined as >75%) seen for anaphylaxis received epinephrine as part of their acute care management (Figure 2); 79 (40.3%) reported that ≤50% of patients seen in their EDs received treatment with epinephrine.
Figure 2.
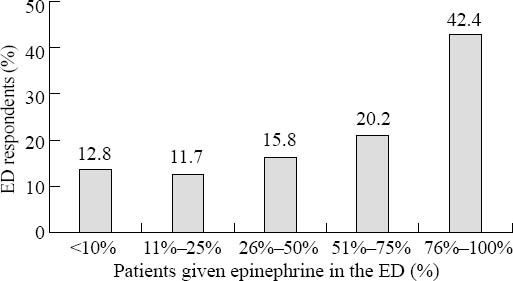
Percentage of patients seen in the ED for anaphylaxis who were treated with epinephrine while in the ED. Respondents answered the question: What percentage of patients treated for anaphylaxis in your ED receive epinephrine as part of their acute care management? (n=196).
Discharge
Ninety-five (48.2%) of the 196 respondents reported that >75% of patients seen for anaphylaxis were discharged with a prescription for an epinephrine auto-injector (Figure 3). However, 61 respondents (31%) reported that in their ED ≤50% of patients received such a prescription.
Figure 3.
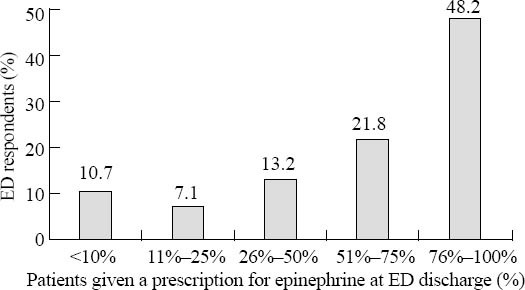
Percentage of patients seen in the ED for anaphylaxis who were discharged with a prescription for self-injectable epinephrine. Respondents answered the question: What percentage of patients treated for anaphylaxis in your ED is discharged with a prescription for self-injectable epinephrine? (n=197).
Two distinct subgroups were identified by the respondents as more likely to receive a prescription for epinephrine at discharge (Figure 4): those with reactions to insect stings or foods (76% and 61% received a prescription, respectively).
Figure 4.
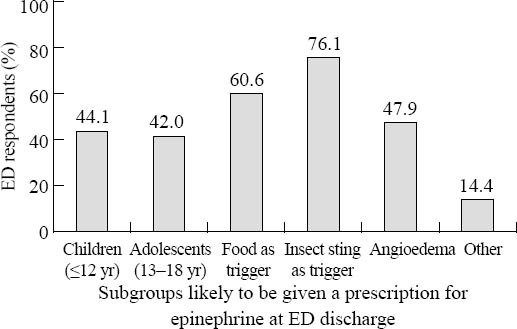
The likelihood of anaphylaxis patient subgroups being discharged with a prescription for self-injectable epinephrine. Respondents answered the question: Are there particular patient populations you are more likely to prescribe self-injectable epinephrine to at discharge? (n=188).
The top three barriers to prescribing epinephrine described by 176 respondents were lack of staff/provider awareness/education (61 respondents, 34.7%); concern about side effects, particularly in older patients (57 respondents, 32.4%); and cost (45 respondents, 25.6%). Other concerns cited included a lack of standard protocols and time. In regards to time, several respondents specifically commented that they did not have the time or, in some cases, the training materials to provide appropriate patient education and follow-up.
At discharge, most patients were advised to follow-up with a physician (Figure 5). Of 198 respondents, 171 (86.4%) recommended that the patient see the primary care physician (PCP). Referrals for follow-up with an allergist, per guideline recommendations, were not as common – 83 respondents (41.9%) reported that their EDs recommended allergist follow-up for >50% of patients seen for an episode of anaphylaxis, but only 34 respondents (17%) recommended follow-up with an allergist for the majority of patients.
Figure 5.
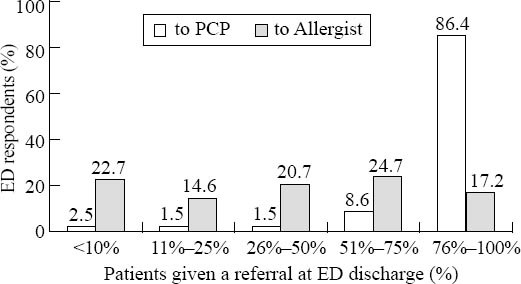
Percentage of patients seen in the ED for anaphylaxis, who were given a referral to see a physician at discharge. Respondents answered the question,What percentage of patients treated for anaphylaxis in your ED are discharged with a referral to a primary care physician (PCP) and/or to an allergist? (n=198 respondents).
Almost all EDs (185 or 94.9% of 195 respondents) provided written information about anaphylaxis to patients at discharge; 134 or 71.3% of 188 respondents reported that patients were given an anaphylaxis action plan.
DISCUSSION
This is the first cross-sectional survey of EM professionals to evaluate management of anaphylaxis in US EDs. The data confirm a wide variability in practice and substantial gaps in the application of guideline-based recommendations for the diagnosis, treatment, and follow-up care of these patients. The survey, while relatively simple in design and limited in scope, captured critical points regarding all three components of management.
The primary gap identified is low utilization of a standard definition of anaphylaxis: 90% of EDs in this survey did not use a formal definition of anaphylaxis despite the agreed-upon criteria in both allergy and EM literature (Table 1).[3–6] Lack of a definition affects all components of care and likely accounts for the substantial diagnostic disparity observed in the “real world.”[13,15–17] It has been estimated that at least 50% of anaphylaxis episodes are misdiagnosed in the ED when the diagnostic criteria of current guidelines are not used.[19,20] More importantly for the patient, low recognition of anaphylaxis in the ED may delay the treatment with epinephrine and result in comorbidity, hospitalization and death.[17,18,21–25]
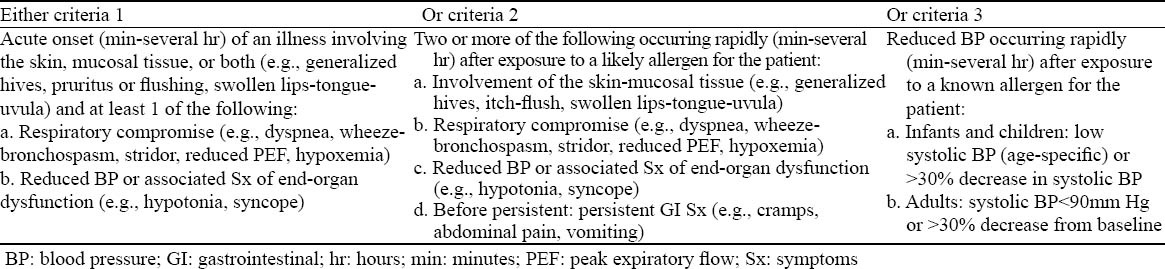
Table 1.
Clinical criteria for the diagnosis of acute anaphylactic episode:[3–7] Anaphylaxis is highly likely when any one of the following 3 criteria is fulfilled
However, even when the patient has been appropriately diagnosed with anaphylaxis, epinephrine may not be given as the first-line treatment. This is in direct contrast to the recommendations of all current practice guidelines for anaphylaxis.[3–7] It may reflect the lack of standard protocols for anaphylaxis treatment as reported by approximately two-thirds of the EM providers who participated in this survey. Alternatively, it may represent a low awareness of guideline recommendations and mistaken concerns about the safety of IM epinephrine for anaphylaxis (i.e., confusion about adverse physiological effects associated with epinephrine administered at the intravenous doses used for cardiopulmonary resuscitation).[15,17]
With regard to discharge recommendations for patients seen in the ED for an episode of anaphylaxis or serious allergic reaction, only one (provision of written information) was regularly followed. The others (prescription of an epinephrine auto-injector and referral to an allergist) occurred less consistently. Nevertheless, almost all responding EDs recommended that patients follow up with their PCP. It is unclear whether this recommendation was specific to anaphylaxis management or whether it reflected a general discharge requirement that all patients be told to contact their PCP after an ED visit, independent of specific diagnosis. Furthermore, the critical information would be the percentage of patients who follow-through on the referral, and we did not collect these data. However, using a similar model in which follow-up outpatient appointments are strongly recommended (children seen for a severe asthma exacerbation in a pediatric ED) a retrospective cohort study reported that only 12% of patients followed up with their PCP.[26] This could be an area of further study.
Our data are similar to practice gaps identified in the study assessing implementation of anaphylaxis guidelines in Germany, Austria, and Switzerland[16] as well as in an earlier global review of anaphylaxis emergency care.[14]
To date, there is no systematic review focusing on anaphylaxis management in US EDs, nor are there any studies specifically evaluating gaps in practice in relation to guideline-based recommendations for managing anaphylaxis. However, we were able to find 13 US studies (8 in adults, 5 in adolescents and children) in which individual gaps in diagnosis, treatment, and follow-up could be inferred.[1,8–10,19,20,27–34] The applicable data are summarized in Table 2.
Table 2.
Gaps where clinical practice differs from guideline recommendations for managing the anaphylaxis in the ED, indirectly suggested by studies of the incidence or management of anaphylaxis at US EDs. All studies evaluated US data only and used a definition of anaphylaxis based on current guideline criteria. Gaps in diagnosis, ED treatment, and discharge are noted.
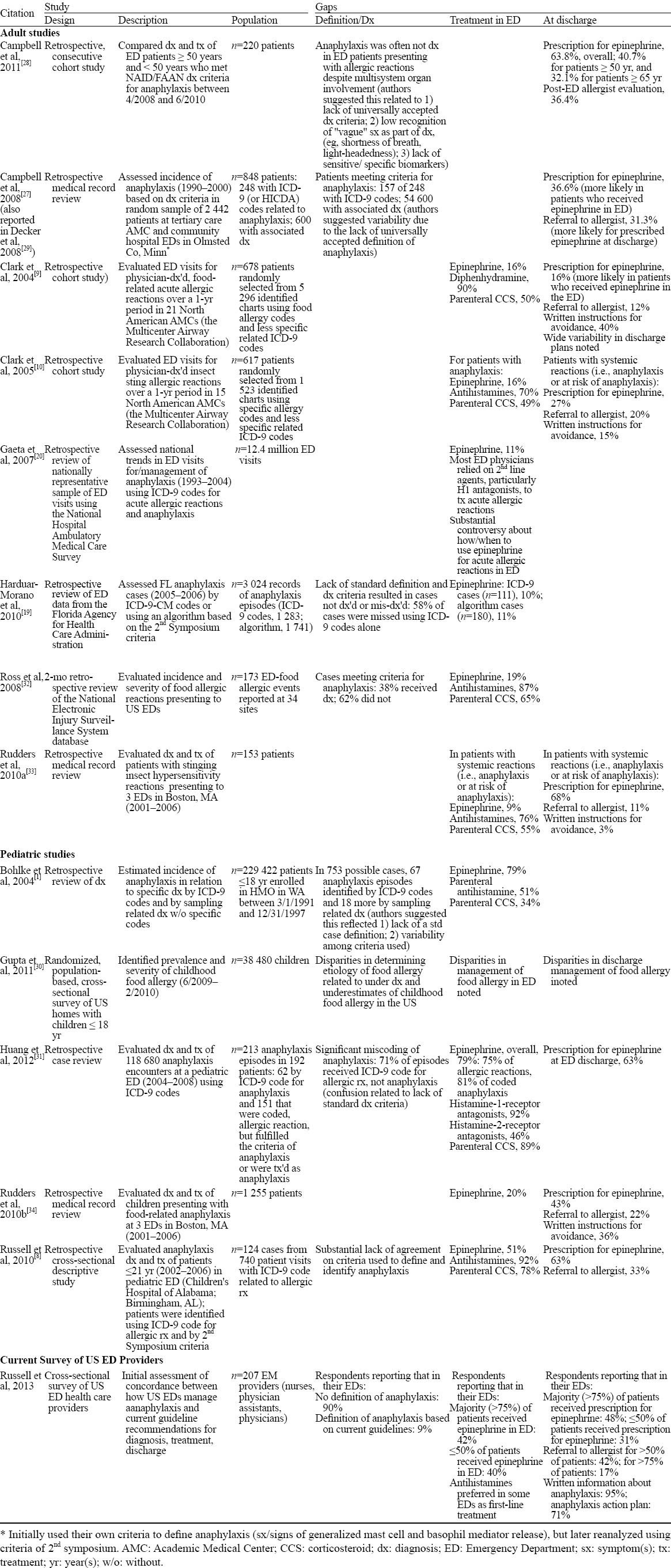
Eight studies (4 adults, 4 children) evaluated the diagnosis by ICD-9 coding with or without application of the clinical criteria recommended by anaphylaxis guidelines.[1,8,19,27–32] Regardless of the age of the patients or the causative trigger of the acute allergic reaction, the number of episodes receiving a diagnosis of anaphylaxis increased with application of the additional criteria, sometimes, dramatically. For example, a 2-month retrospective review of ED-food allergic events reported at 34 sites within the database of the US National Electronic Injury Surveillance System found that 62% of anaphylaxis cases did not receive the correct diagnosis. [32] Our data would suggest that some of these EDs probably did not use a formal definition of anaphylaxis. Would this help providers be more compliant with published guidelines? Probably. A study validating a diagnostic algorithm based on guideline recommended criteria (Table 1) to help capture previously unidentified anaphylaxis cases in the ED estimated that without the algorithm as many as 58% of anaphylaxis cases reported to the Florida Agency for Health Care Administration were missed, including 88% of the insect sting/venom-related cases.[19] We believe that an accurate definition is the starting point for better care.
In eight studies reporting data on epinephrine use for acute anaphylaxis in the ED, the variability is striking, with the proportion of treated patients ranging from 9% to 79%.[8–10,27–13;29,31,33,34] Our data show a similar range. An overall rate of 11% has been reported using data from the US National Hospital Ambulatory Medical Care Survey (1993–2004)[20] and, separately, by the Florida Agency for Health Care Administration (2005–2006).[19] The published data confirm the greater use of second-line agents than epinephrine in the treatment of anaphylaxis in the ED with approximately 80% of patients receiving antihistamines (range 51%–92%)[1,8–10,20,31–34] and 60%, corticosteroids (range 34%–89%).[1,8–10,31,33] While we did not specifically ask about these second-line agents, several respondents commented that antihistamines were a preferred first treatment for anaphylaxis in their ED.
Studies also indicate discordance with guideline recommendations for discharge in the US: approximately 45% of patients treated for anaphylaxis in the ED received a discharge prescription for epinephrine (range 16%–63%);[8–10,27,29,31,33,34] and even fewer were given a referral to an allergist (21.6%, range 11%–33%)[8–10,27,29,33,34] and/or information about avoiding causative agents (23.5%, range 3%–40%).[9,10,33,34] Treatment with epinephrine in the ED may predict the likelihood of a prescription for epinephrine at discharge and referral to an allergist.[9,27,29] Anecdotally, our data agree. In written comments, respondents who themselves were likely to treat with epinephrine in the ED (regardless of protocol or lack thereof) were also more likely to prescribe epinephrine at discharge and to recommend allergist follow-up. Similar outcomes were reported for physicians who used an anaphylaxis protocol in pediatric EDs in Spain as epinephrine use in the ED increased, so did prescription of self-injectable epinephrine on discharge.[15] The survey data also suggest that patients treated for (suspected) anaphylaxis to insect stings/venom or foods may be more likely to receive a prescription for an epinephrine auto-injector. Differences between this survey and published studies probably reflect specific wording of the questions and differences in data collection.
LIMITATIONS
The primary limitations of this survey are its reliance on participant self-reporting and the seemingly low response rate (7%, based on the email notification to 3000 ED health care professionals). As a pilot study assessing how guideline recommendations are incorporated in current ED practice, we sought a tool that would provide a relatively rapid response. The survey was not validated, and the data (based on response counts and percentages) represent a baseline. We sought 200 to 300 responses within a 6-week period, or a response rate of 7% to 10%, which was achieved, but was not sufficient for statistical analysis.
There also is the possibility that individual responses were inaccurate or biased according to the respondent's role in the ED and interest in anaphylaxis. In this regard, we noted that some respondents reported personal variation from the general practice of their ED, e.g., 76% of respondents reported always prescribing an epinephrine auto-injector for their patients on ED discharge, but only 48% reported this to be true for their ED overall.
Twenty-nine respondents did not identify their practice. A sub-analysis of the data with and without these respondents showed no difference in the trends observed. We included the data from these respondents in the survey analysis.
All regions of the US are represented in the responses to our survey, but we did not separate community hospitals from academic medical centers, nor did we evaluate the data for multiple respondents from any single health care system. Both could affect the generalizability of the results. However, while the data cannot be directly compared, the trends from our “real world” survey are reassuringly similar to trends reported for retrospective case studies that looked individually at the diagnosis, treatment, or discharge of patients with anaphylaxis in US EDs.[9,10,19,27,32] We believe that the limitations of our survey are not likely to be clinically significant and that the reported findings can be generalized to most American EDs.
IMPLICATIONS
This is the first survey to specifically evaluate the concordance between how US EDs manage anaphylaxis and guideline recommendations. The outcomes confirm deficits in all three components of care-application of diagnostic criteria, use of epinephrine in the ED, and discharge plans. Our survey suggests that despite a preponderance of documents providing specific criteria for managing anaphylaxis and studies supporting those management recommendations, current practice in US EDs has not changed and does not reflect the recommended standard for patient care. Specifically, despite repeated attempts to ensure that epinephrine is the first-line therapy for anaphylaxis, “real world” practice does not reflect this paradigm. Many articles have commented on the likely link between lack of a standard definition for anaphylaxis and diagnostic confusion resulting in low or delayed use of epinephrine in the ED, but this is the first study to provide data for that association. Most EDs (90%) used no standard definition of anaphylaxis; and for the few that did, there was a wide variability in source.
RECOMMENDATIONS
This survey provides a baseline for how to improve the management of anaphylaxis in the emergency setting. We believe that the first and most critical recommendation would be adoption of a standard definition of anaphylaxis that is appropriate for EM health professionals.[17] Furthermore, the definition needs to include the two components of anaphylaxis: the acute and potentially life-threatening episode that is seen in the ED and the chronic risk for such episodes requiring follow-up and long-term management. The second recommendation is to develop programming again specific to EM that addresses the first-line role of epinephrine in the treatment of anaphylaxis. This is a two-fold recommendation: first encompassing the importance of quickly administering epinephrine in the ED even when anaphylaxis is only suspected, and second, a reminder that all patients seen in the ED for anaphylaxis are at risk for future episodes and should be discharged with a prescription for an epinephrine auto-injector. As EM professionals we are the first line of defense for many of these patients. Their ED visit provides the chance to show them, by treating them, how to administer epinephrine, what it feels like, and how quickly it works and then to inform them of the likelihood of future episodes and the actions they can take to minimize that risk.
Finally, further study is needed to determine how to bridge the specific gaps identified in this survey. We know now that in the “real EM world” adherence to the recommendations of anaphylaxis guidelines is not good,[15–17] but we do not really understand the impact on patient outcomes as the data predominantly reflect inferences made from retrospective reviews or case series. The low concordance in clinical application itself may provide feedback on the practicality of the criteria, their acceptance, and potential barriers to implementation-independent of the patient's condition. More discussion will be needed on this point.
While clinical trials of recommended strategies cannot be conducted for ethical reasons, prospective data are needed to better evaluate the short- and long-term outcomes of implementing different management recommendations for patients with anaphylaxis seen in the ED, and perhaps could be obtained through national or international registries.
Footnotes
Funding: This manuscript was supported in part by an unrestricted educational grant from Mylan Specialty Pharmaceuticals (Basking Ridge, NJ).
Ethical approval: Not needed.
Conflicts of interest: The authors have no competing interests relevant to the present study.
Contributors: All authors participated in creating the online survey as well as reviewing the responses, evaluating the other studies for comparative review as described in the discussion section, and developing and editing multiple drafts of the manuscript. All authors met the ICMJE definition of authorship.
REFERENCES
- 1.Bohlke K, Davis RI, DeStefano F, Marcy SM, Braun MM, Thompson RS, et al. Epidemiology of anaphylaxis among children and adolescents enrolled in a health maintenance organization. J Allergy Clin Immunol. 2004;113:536–542. doi: 10.1016/j.jaci.2003.11.033. [DOI] [PubMed] [Google Scholar]
- 2.Clark S, Camargo CA., Jr Epidemiology of anaphylaxis. Immunol Allergy Clin N Am. 2007;27:145–163. doi: 10.1016/j.iac.2007.03.002. [DOI] [PubMed] [Google Scholar]
- 3.Simons FE, Ardusso LR, Bilo MB, El-Gamal YM, Ledford DK, Ring J, et al. World Allergy Organization guidelines for the assessment and management of anaphylaxis. J Allergy Clin Immunol. 2011;127:593.e1–e22. doi: 10.1097/WOX.0b013e318211496c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lieberman P, Nicklas RA, Oppenheimer J, Kemp SF, Lang DM, Bernstein DI, et al. The diagnosis and management of anaphylaxis practice parameter: 2010 update. J Allergy Clin Immunol. 2010;126:477–480. doi: 10.1016/j.jaci.2010.06.022. [DOI] [PubMed] [Google Scholar]
- 5.Sampson HA, Munoz-Furlong A, Campbell R, Adkinson NF, Jr, Bock SA, Branum A, et al. Second symposium on the definition and management of anaphylaxis: summary report. Ann Emerg Med. 2006;47:373–380. doi: 10.1016/j.annemergmed.2006.01.018. Also published in J Allergy Clin Immunol 2006; 117: 391-397. [DOI] [PubMed] [Google Scholar]
- 6.Simons FE, Ardusso LRF, Bilo MB, Dimov V, Ebisawa M, El-Gamal YM, et al. 2012 update: World Allergy Organization Guidelines for the assessment and management of anaphylaxis. Curr Opin Allergy Clin Immunol. 2012;12:389–399. doi: 10.1097/ACI.0b013e328355b7e4. [DOI] [PubMed] [Google Scholar]
- 7.Boyce JA, Assa’ad A, Burks AW, Jones SM, Sampson HA, Wood RA, et al. Guidelines for the diagnosis and management of food allergy in the United States: Report of the NIAID-sponsored expert panel. J Allergy Clin Immunol. 2010;126(suppl 1):S1–58. doi: 10.1016/j.jaci.2010.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Russell S, Lozano D, Monroe K, Losek JD. Anaphylaxis management in the pediatric emergency department Opportunities for improvement. Pediatr Emerg Care. 2010;26:71–76. doi: 10.1097/PEC.0b013e3181ce2e1c. [DOI] [PubMed] [Google Scholar]
- 9.Clark S, Bock SA, Gaeta TJ, Brenner BE, Cydulka RK, Camargo CA., Jr Muticenter study of emergency department visits for food allergies. J Allergy Clin Immunol. 2004;113:347–352. doi: 10.1016/j.jaci.2003.10.053. [DOI] [PubMed] [Google Scholar]
- 10.Clark S, Long AA, Gaeta TJ, Kamarthi GS, Camargo CA., Jr Multicenter study of emergency department visits for insect sting allergy. J Allergy Clin Immunol. 2005;116:643–649. doi: 10.1016/j.jaci.2005.06.026. [DOI] [PubMed] [Google Scholar]
- 11.Beno SM, Nadel FM, Alessandri EA. A survey of emergency department management of acute urticaria in children. Pediatr Emerg Care. 2007;23:862–868. doi: 10.1097/pec.0b013e31815c9dac. [DOI] [PubMed] [Google Scholar]
- 12.Klein JS, Yocum MW. Underreporting of anaphylaxis in a community emergency room. J Allergy Clin Immunol. 1995;95:637–638. doi: 10.1016/s0091-6749(95)70329-2. [DOI] [PubMed] [Google Scholar]
- 13.Camargo CA., Jr Potter Stewart and the definition of anaphylaxis. J Allergy Clin Immunol. 2012;129:753–754. doi: 10.1016/j.jaci.2012.01.030. [DOI] [PubMed] [Google Scholar]
- 14.Kastner M, Harada L, Waserman S. Gaps in anaphylaxis management at the level of physicians, patients, and the community: a systematic review of the literature. Allergy. 2010;65:435–444. doi: 10.1111/j.1398-9995.2009.02294.x. [DOI] [PubMed] [Google Scholar]
- 15.Arroabarren E, Lasa EM, Olaciregui I, Sarasqueta C, Munoz JA, Perez-Yarza EG. Improving anaphylaxis management in a pediatric emergency department. Ped Allergy Immunol. 2010;22:708–714. doi: 10.1111/j.1399-3038.2011.01181.x. [DOI] [PubMed] [Google Scholar]
- 16.Grabenhenrich L, Hompes S, Gough H, Rueff F, Scherer K, Pfohler C, et al. Implementation of anaphylaxis management guidelines: A register-based study. PLOS one. 2012;7:e35778. doi: 10.1371/journal.pone.0035778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nowak R, Farrar JR, Brenner BE, Lewis L, Silverman RA, Emerman C, et al. Customizing anaphylaxis guidelines for emergency medicine. J Emerg Med. 2013. Available at http://dx.doi.org/10.1016/j.jemermed.2013.01.018 . [DOI] [PubMed]
- 18.Kemp SF, Lockey RF, Simons FER on behalf of the World Allergy Oraganization ad hoc Committee on Epinephrine in Anaphylaxis. Epinephrine: the drug of choice for anaphylaxis. A statement of the World Allergy Organization. Allergy. 2008;63:1061–1070. doi: 10.1111/j.1398-9995.2008.01733.x. [DOI] [PubMed] [Google Scholar]
- 19.Harduar-Morano L, Simon MR, Watkins S, Blackmore C. Algorithm for the diagnosis of anaphylaxis and its validation using population-based data on emergency department visits for anaphylaxis in Florida. J Allergy Clin Immunol. 2010;126:98–104. doi: 10.1016/j.jaci.2010.04.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gaeta TJ, Clark S, Pelletier AJ, Camargo CA., Jr National study of US emergency department visits for acute allergic reactions 1993-2004. Ann Allergy Asthma Immunol. 2007;98:360–365. doi: 10.1016/S1081-1206(10)60883-6. [DOI] [PubMed] [Google Scholar]
- 21.Davis JE, Norris RL., Jr Allergic emergencies in children: the pivotal role of epinephrine. Ped Emerg Med Pract. 2007;4:1–28. [Google Scholar]
- 22.Simons FER. Anaphylaxis. J Allergy Clin Immunol. 2010;125:S161–181. doi: 10.1016/j.jaci.2009.12.981. [DOI] [PubMed] [Google Scholar]
- 23.Pumphrey RSH. Lessons for management of anaphylaxis from a study of fatal reactions. Clin Exp Allergy. 2000;30:1144–1150. doi: 10.1046/j.1365-2222.2000.00864.x. [DOI] [PubMed] [Google Scholar]
- 24.Sicherer SH, Simons ER. and the Section on Allergy and Immunology. Self-injectable epinephrine for first-aid management of anaphylaxis. Pediatrics. 2007;119:638–646. doi: 10.1542/peds.2006-3689. [DOI] [PubMed] [Google Scholar]
- 25.Bock SA, Munoz-Furlong A, Sampson HA. Fatalaties due to anaphylactic reactions to food. J Allergy Clin Immunol. 2001;107:191–193. doi: 10.1067/mai.2001.112031. [DOI] [PubMed] [Google Scholar]
- 26.Andrews Al, Teufel RJ, II, Basco WT., Jr Low rates of controller medication initiation and outpatient follow-up after emergency department visits for asthma. J Pediatr. 2012;160:325–330. doi: 10.1016/j.jpeds.2011.07.037. [DOI] [PubMed] [Google Scholar]
- 27.Campbell RL, Luke A, Weaver Al, Decker WW, Kanthala AR, Bellolio MF, et al. Prescriptions for self-injectable epinephrine and follow-up referral in emergency department patients presenting with anaphylaxis. Ann Allergy Asthma Immunol. 2008;101:631–636. doi: 10.1016/S1081-1206(10)60227-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Campbell RL, Hagan JB, Li JT, Vukov SC, Kanthala AR, Smith VD, et al. Anaphylaxis in emergency department patients 50 or 65 years or older. Ann Allergy Asthma Immunol. 2011;106:401–406. doi: 10.1016/j.anai.2011.01.011. [DOI] [PubMed] [Google Scholar]
- 29.Decker WW, Campbell RL, Manivannan V, Luke A, St Sauver JL, Weaver A, et al. The etiology and incidence of anaphylaxis in Rochester Minnesota: A report from the Rochester Epidemiology Project. J Allergy Clin Immunol. 2008;122:1161–1165. doi: 10.1016/j.jaci.2008.09.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gupta RS, Springston EE, Warrier MR, Smith B, Kumar R, Pongracic J, et al. The prevalence, severity, and distribution of childhood food allergy in the United States. Pediatrics. 2011;128:e9–e17. doi: 10.1542/peds.2011-0204. [DOI] [PubMed] [Google Scholar]
- 31.Huang F, Chawla K, Jarvinen KM, Nowak-Wegzyn Anaphylaxis in a New York City pediatric emergency department: Triggers, treatments, and outcomes. J Allergy Clin Immunol. 2012;129:162–168. doi: 10.1016/j.jaci.2011.09.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ross MP, Ferguson M, Street D, Klontz K, Schroeder T, Luccioli S. Analysis of food-allergic and anaphylactic events in the National Electronic Injury Surveillance System. J Allergy Clin Immunol. 2008;121:166–171. doi: 10.1016/j.jaci.2007.10.012. [DOI] [PubMed] [Google Scholar]
- 33.Rudders SA, Banerji A, Katzman DP, Clark S, Camargo CA., Jr Multiple epinephrine doses for stinging insect hypersensitivity reactions treated in the emergency department. Ann Allergy Asthma Immunol. 2010;105:85–93. doi: 10.1016/j.anai.2010.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rudders SA, Banerji A, Corel B, Clark S, Camargo CA., Jr Multicenter study of repeat epinephrine treatments for food-related anaphylaxis. Pediatrics. 2010;125:e711–718. doi: 10.1542/peds.2009-2832. [DOI] [PMC free article] [PubMed] [Google Scholar]