

Abstract
Purpose
To report the clinical presentation, antibiotic sensitivities, treatment strategies, and visual outcomes associated with endophthalmitis caused by Klebsiella species.
Methods
A non-comparative consecutive case series. Microbiology database records were retrospectively reviewed for all patients with endophthalmitis caused by Klebsiella species from 1990 to 2012 at a large university referral center. The corresponding clinical records were then reviewed to evaluate the endophthalmitis clinical features and treatment outcomes.
Results
Seven patients were identified. Clinical settings included endogenous (n=3), post-traumatic (n=2), trabeculectomy bleb-associated (n=1), and post-penetrating keratoplasty (n=1). Five patients presented with hypopyon. Presenting visual acuity ranged from 20/60 to light perception in non-endogenous cases and 1/200 to light perception in endogenous cases. Klebsiella was sensitive to aminoglycosides, 3rd generation cephalosporins, and 2nd and 3rd generation fluoroquinolones in all cases. Initial treatment strategies were vitreous tap and injection (n=4), pars plana vitrectomy with intravitreal antibiotics (n=2), and anterior chamber tap and injection (n=1). All three endogenous cases later underwent enucleation or evisceration. In non-endogenous cases, final visual acuity was 20/70 or better in all four patients.
Conclusions
Endophthalmitis caused by Klebsiella species is associated with poor visual outcomes. Endogenous cases had high rates of enucleation or evisceration.
Keywords: Endophthalmitis, Endogenous, Klebsiella, Bacterial Eye Infections
Introduction
Klebsiella species are gram-negative, encapsulated, anaerobic bacteria that may form part of the normal nasopharyngeal and gastrointestinal flora.1 In recent years Klebsiella species have emerged as a leading cause of pyogenic liver abscesses in Asia.2,3 Klebsiella pneumonaie liver abscesses are associated with a 3 to 11 percent incidence of endogenous endophthalmitis.4,5 This rate of ocular involvement is much higher than ocular involvement with other systemic infections.6 More significantly, endophthalmitis caused by Klebsiella species is associated with increased mortality in patients with liver abscesses.7
Endophthalmitis caused by Klebsiella species has been recognized as an increasingly prevalent cause of endogenous endophthalmitis in Asia, accounting for 54 to 61 percent of cases in selected series.5,8-11 Reported risk factors for endogenous endophthalmitis caused by Klebsiella species include liver abscesses, diabetes mellitus, and systemic immunocompromise.5,8,12,13 In contrast, endophthalmitis caused by Klebsiella, whether endogenous and non-endogenous, is uncommon in the USA, described only in a small number of isolated case reports and series.14-19 Still, it is an emerging entity in the USA associated with poor visual outcomes.12,13,19
Based on a PubMed literature search, the current study is the largest reported series in the USA to date of culture-positive cases of endophthalmitis caused by Klebsiella.
Methods
Institutional review board approval was obtained from the University of Miami Miller School of Medicine Sciences Subcommittee for the Protection of Human Subjects. The ocular microbiology department database was searched to identify all patients with positive intraocular cultures (anterior chamber, vitreous, or both) for Klebsiella species between January 1, 1990, and December 31, 2012. Microbiology department records were reviewed to identify the responsible microbial isolates and antibiotic sensitivities.
Anterior chamber cultures were obtained from an anterior chamber paracentesis. Vitreous cultures were obtained either at the time of vitreous tap and inject or during vitrectomy. Fluids from anterior chamber paracentesis or vitreous tap were plated directly on to culture media including 5% sheep blood and chocolate agars. For vitrectomy specimens, 30–50 cc of vitreous washings were filtered using a 0.45-μm filter. The resultant filter paper was divided into sections and was plated on to different culture media, which typically included chocolate and blood agars. Blood and chocolate agars underwent incubation at 35°C for a period of up to 2 weeks. Additional culture media, including thioglycollate broth, were performed at the discretion of the ophthalmologist performing the culture. All cultures were read and classified by Ocular Microbiology Department staff.
After analyzing microbiology records, the corresponding medical records of these patients were reviewed to ensure clinical course consistent with endophthalmitis. Patient demographics, clinical characteristics, risk factors, treatment strategies, and clinical outcomes were assessed.
Results
Over the 22-year study period, 10 eyes from 10 patients were identified to have positive intraocular cultures for Klebsiella species and clinical course consistent with endophthalmitis. three eyes had been reported previously from the same institution by Scott et al15 and were excluded. In the remaining 7 eyes, cultures were positive for Klebsiella pneumoniae (n=5) or Klebsiella oxytoca (n=2, Table 1). Cultures were obtained from vitreous tap (n=4), vitrectomy specimen (n=2), or anterior chamber tap (n=1).
Table 1. Endophthalmitis caused by Klebsiella species: Clinical Characteristics, Initial Treatment Strategies, and Outcomes.
| Patient | Demographics | Etiology | Organism (source) | Presenting VA | Initial Treatment | Clinical Improvement | Follow-up (months) | Last VA |
|---|---|---|---|---|---|---|---|---|
| 1 | 43 year-old man diagnosed with liver abscess after ocular presentation | Endogenous | K. pneumonaie (vitreous tap) | 2/200 | Vitreous tap/injection | No | 1 | enucleated |
| 2 | 58 year-old woman with history of DM and recent spider bite and cellulitis on arm | Endogenous | K. pneumonaie (PPV specimen) | 1/200 | PPV with intravitreal injection | No | 4 | enucleated |
| 3 | 60 year-old woman with history of multiple myeloma on chemotherapy and DM | Endogenous | K. pneumonaie (vitreous tap) | Light perception | Vitreous tap/injection | No | 20 | eviscerated |
| 4 | 60 year-old man status post penetrating trauma with retained IOFB (glass) | Penetrating Trauma | K. pneumonaie (PPV specimen) | Light perception | PPV with intravitreal injection | Yes | 2 | 20/60 |
| 5 | 31 year-old woman status post penetrating trauma | Penetrating Trauma | K. oxytoca (anterior chamber tap) | 20/60 | Anterior chamber tap/injection* | Yes | 4 | 20/25 |
| 6 | 78 year-old man status post PK/IOL exchange | Post-operative | K. oxytoca (vitreous tap) | Hand movements | Vitreous tap/injection | Yes | 83 | 20/70 |
| 7 | 67 year-old woman with history of trabeculectomy 7 months prior | Bleb-related | K. pneumonaie (vitreous tap) | Hand movements | Vitreous tap/injection | No+ | 76 | 20/70 |
DM: diabetes mellitus; IOFB: intraocular foreign body; PPV: pars plana vitrectomy; PK: penetrating keratoplasty; IOL: intraocular lens; VA: Snellen visual acuity; Last VA: visual acuity at last follow-up examination
Patient 5 underwent repair of corneal laceration simultaneously
Patient 7 subsequently underwent pars plana vitrectomy
The median patient age was 60 years (range, 31 to 78 years). Median follow-up was 4 months (range, 1 month to 6 years). Endophthalmitis occurred in the clinical setting of penetrating trauma (n=2), post-trabeculectomy (n=1), post-penetrating keratoplasty (n=1), and endogenous (n=3). Two of the three patients with endogenous endophthalmitis were diabetic and had negative systemic workup including blood cultures. The third patient was found to have a liver abscess with positive blood cultures.
Five patients presented with pain. Visual acuity on presentation ranged from 20/60 to light perception (Table 2). Hypopyon was noted in five patients on presentation. Two patients had diffuse vitritis with no view of the posterior segment. One patient was noted to develop a subretinal abscess (Figure 1). One patient presented with orbital cellulitis in addition to endophthalmitis (Figure 2).
Table 2. Initial Treatment Strategies and Outcomes of Patients with Endophthalmitis caused by Klebsiella species.
| Patient | Presenting VA | Initial Treatment | Clinical Improvement | Follow-up (months) | Last VA |
|---|---|---|---|---|---|
| 1 | 2/200 | Vitreous tap/injection | No | 1 | enucleated |
| 2 | 1/200 | PPV with intravitreal injection | No | 4 | enucleated |
| 3 | Light perception | Vitreous tap/injection | No | 20 | eviscerated |
| 4 | Light perception | PPV with intravitreal injection | Yes | 2 | 20/60 |
| 5 | 20/60 | Anterior chamber tap/injection* | Yes | 4 | 20/25 |
| 6 | Hand movements | Vitreous tap/injection | Yes | 83 | 20/70 |
| 7 | Hand movements | Vitreous tap/injection | No+ | 76 | 20/70 |
VA: Snellen visual acuity; Last VA: visual acuity at last follow-up examination; PPV: pars plana vitrectomy
Patient 5 underwent repair of corneal laceration simultaneously
Patient 7 subsequently underwent pars plana vitrectomy
Figure 1.
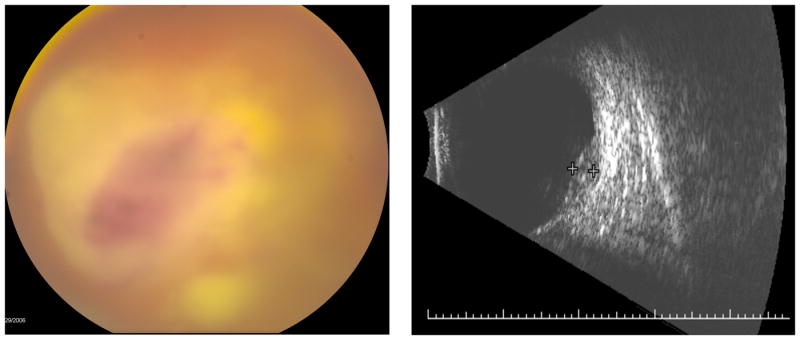
Patient 2 was a 58 year-old woman with history of diabetes mellitus and recent localized cellulitis on the arm who presented with pain and 1/200 visual acuity in the right eye. Posterior segment examination revealed a hazy view with moderately dense vitritis obscuring a subretinal abscess (left). B-Scan ultrasonography confirmed the subretinal abscess adjacent to the optic nerve (right). The patient underwent pars plana vitrectomy with intravitreal injection of antibiotics. Vitreous specimen culture grew Klebsiella pneumonaie. One month after presentation the patient was enucleated for blind, painful eye.
Figure 2.
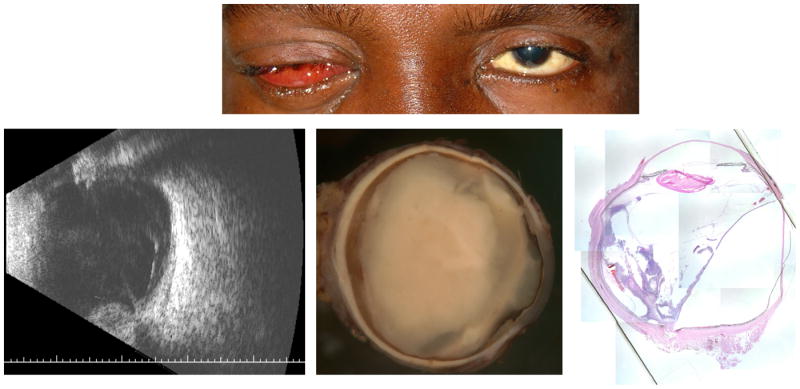
Patient 1 was a 43-year-old man with no past medical history who presented with pain, chemosis, and finger count vision in the right eye (top). Posterior segment examination revealed dense vitritis with no view in the right eye. Initial B-scan ultrasonography confirmed no evidence of retinal detachment. The patient underwent vitreous tap and injection of intravitreal antibiotics. Vitreous culture grew Klebsiella pneumonaie. Systemic workup revealed positive blood cultures for Klebsiella pneumonaie and large liver abscess. The patient clinically worsened and repeat B-scan ultrasonography revealed a bullous retinal detachment and evidence of panophthalmitis (bottom left). The patient underwent enucleation one week after presentation (bottom center). Histopathlogic examination with hematoxylin and eosin at 1.25x magnification revealed a subretinal inflammatory collection underlying the detachment (bottom right).
Four patients underwent diagnostic vitreous tap with injection of intravitreal antibiotics the same day as presentation. Two patients, with visual acuity of 1/200 and light perception respectively, were evaluated in the evening the day of presentation, received topical fortified antibiotics overnight, and the following morning underwent pars plana vitrectomy with injection of intravitreal antibiotics. One patient status post penetrating trauma underwent anterior chamber tap with injection of intracameral antibiotics during repair of a corneal laceration the same day as presentation. Intraocular antibiotics consisted of vancomycin and ceftazidime for all patients except the one patient post-penetrating keratoplasty who received intravitreal vancomycin and gentamicin. Only the patient with endogenous endophthalmitis with liver abscess received intravitreal corticosteroids.
Initial intraocular cultures were positive for Klebsiella species in all patients. All isolates were sensitive to one of the initially administered intraocular antibiotics. The two Klebsiella oxytoca isolates were resistant to penicillin but sensitive to gentamicin, ceftazidime, ciprofloxacin, sulfa-trimethoprim, and levofloxacin. All five Klebsiella pneumonaie isolates were sensitive to gentamicin, ceftazidime, ciprofloxacin, levofloxacin, and sulfa-trimethoprim. Three of the five Klebsiella pneumonaie isolates were resistant to penicillin.
The patient initially treated with anterior chamber tap and intracameral antibiotics, one patient initially treated with vitreous tap and injection, and one patient initially treated with pars plana vitrectomy demonstrated clinical improvement and did not require further intraocular treatment. Final visual acuity in these three patients was 20/25, 20/60, and 20/70, respectively. One patient who underwent initial vitreous tap and injection showed no clinical improvement. This patient underwent subsequent pars plana vitrectomy 3 days after presentation with no evidence of persistent infection on repeat vitreous culture and had a good post-operative result with final visual acuity of 20/70. Two patients who underwent initial vitreous tap and injection developed panophthalmitis and underwent evisceration and enucleation, respectively, within one week of presentation with the evisceration specimen culture showing persistent infection. One patient who underwent initial pars plana vitrectomy demonstrated clinical worsening and eventually underwent enucleation 1 month after presentation for the blind painful eye. All three patients undergoing evisceration or enucleation had endogenous endophthalmitis. Two of these patients received systemic antibiotics. One patient, a diabetic woman with multiple myeloma, received intravenous ceftazidime for 14 days. The patient with the liver abscess received intravenous ceftriaxone for 7 days and oral gatifloxacin for 14 days concurrently with resolution of orbital cellulitis and the liver abscess.
Discussion
Klebsiella-specific virulence factors contribute to the organism's propensity for ocular involvement. Klebsiella species possess a polysaccharide capsule with specific capsular serotypes conferring resistance to phagocytosis by neutrophils.20 Specifically, Klebsiella pneumonaie serotypes K1 and K2 have increased virulence and decreased susceptibility to intracellular destruction by neutrophils than other Klebsiella serotypes. This ability to avoid phagocytosis among K1 and K2 serotypes has been demonstrated to be enhanced in diabetes mellitus patients with poor glycemic control.21 In fact, diabetes mellitus is a significant risk factor for endogenous endophthalmitis caused by Klebsiella as well as a poor visual prognostic factor in patients with ocular involvement.5,8,22 Two of the three patients in the current series with endogenous endophthalmitis were diabetic and had poor visual outcomes. Other known risk factors for ocular involvement include systemic immunocompromise, disseminated intravascular coagulation, and delayed treatment of systemic Klebsiella bacteremia.4
The high incidence of endogenous endophthalmitis caused by Klebsiella in Asia is at least partially attributed to the relatively high incidence of Klebsiella bacteremia in the Asian population, although genetic susceptibility has been suggested as a contributing factor as well.5 In recent years it has been recognized that the K1 and K2 serotypes of Klebsiella pneumonaie constitute the majority of endogenous endophthalmitis cases in Asia, representing a significant public health challenge.23
In contrast, only a small number of cases of endophthalmitis caused by Klebsiella, endogenous or non-endogenous, have been reported in the USA.14-19 Chen and Adelman24 reported Klebsiella species growth in only 3.1% of all vitreous samples reviewed over a 21 year period at a large tertiary referral center in New England. Okada et al25 and Schiedler et al26 independently reported large domestic series of endogenous endophthalmitis with an incidence of endophthalmitis caused by Klebsiella of 3.6% and 5%, respectively. Of note, none of the cases in the ‘Endophthalmitis Vitrectomy Study’ were due to Klebisella species.27
In the largest prior series from the USA, five patients were seen at the same institution as patients in the current series15. In that series, one patient had endogenous endophthalmitis and underwent enucleation, similar to the results found for the endogenous cases in the current series. Visual acuity ranged from 20/60 to light perception in the remaining cases. Klebsiella isolates in that series were sensitive to aminoglycosides, 3rd-generation cephalosporins, 2nd, 3rd, and 4th generation fluoroquinolones, and sulfa-trimethoprim. This prior sensitivity profile is essentially identical to the sensitivity data in the current series. By contrast, there appears to be a worldwide increase, primarily reported in Asia, of Klebsiella pneumonaie species with variable resistance to 3rd-generation cephalosporins and fluoroquinolones.28
Several reported series have demonstrated extremely poor visual acuity outcomes with high rates of enucleation or evisceration in cases of endogenous endophthalmitis caused by Klebsiella despite adequate treatment. In a large series of endogenous cases, final visual acuity of 4/200 or worse was reported in 77.5% of eyes and 26.8% of eyes ultimately had evisceration10. In addition, Yang et al13 reported final visual acuity of light perception or worse in 89% of study eyes with 41% undergoing evisceration or enucleation and patients with hypopyon having significantly worse outcomes. Klebsiella pneumonaie has been shown in vitro to induce a significant pro-inflammatory response in human retinal pigmented epithelium, likely contributing to the rapid progression and poor prognosis of associated endophthalmitis.29 Similar inflammatory response has been shown in animal models for Klebsiella oxytoca.30 In concordance with the Asian studies, all three patients in the current series with endogenous endophthalmitis ultimately underwent evisceration or enucleation. In contrast, the other four patients all had final visual acuity of 20/70 or better. Only case reports and small cases series have described outcomes of non-endogenous Klebsiella endophthalmitis with variable results.14,31 It is unclear why there was a substantial difference in the outcomes between endogenous and non-endogenous cases in the current series. The authors hypothesize that only more virulent serotypes, such as the K1 and K2 Klebsiella pneumonaie serotypes, are able to break through the blood-retinal barrier and produce endogenous endophthalmitis whereas any serotype, regardless of virulence, may gain access to the eye either after trauma or surgical manipulation. Thus, endogenous cases may progress much faster and result in poorer visual outcomes.
It has been proposed that early vitrectomy may be preferred in endogenous cases given the fulminant nature of these infections. Yoon et al12 reported 10 eyes, 8 of which underwent vitrectomy within one week of onset of symptoms. At final follow-up no eyes were enucleated, 5 eyes had count fingers vision or better, and the retina was attached in all cases. Similarly, Yarng et al32 reported a patient with bilateral endogenous Klebsiella pneumoniae endophthalmitis who underwent vitrectomy in one eye with improved visual outcome compared to the fellow eye. It is hypothesized that surgical intervention aids in the clearance of purulent material and the penetration of intravitreal antibiotics.
In conclusion, endophthalmitis caused by Klebsiella is an increasingly prevalent entity both worldwide and in the USA. In endogenous cases it is associated with poorest outcomes and high rates of evisceration or enucleation.
Summary Statement: A 22-year retrospective review of patients with endophthalmitis caused by Klebsiella species at a large tertiary academic center is presented. This report demonstrates the poorest visual outcomes in endogenous cases.
Acknowledgments
This study is supported in part by NIH Center Core Grant P30EY014801, Research to Prevent Blindness Unrestricted Grant, Department of Defense (DOD-Grant#W81XWH-09-1-0675).
Footnotes
The authors have no proprietary or financial interest in any of the work discussed in this manuscript.
Dr. Flynn is a consultant for Santen and Vindico. Otherwise, there are no disclosures for any author.
References
- 1.Chang FY, Chou MY. Comparison of pyogenic liver abscesses caused by Klebsiella pneumonaie and non-K. pneumonaie pathogens. J Formos Med Assoc. 1995;94:232–7. [PubMed] [Google Scholar]
- 2.Chan KS, Yu WL, Tsai CL, et al. Pyogenic liver abscess caused by Klebsiella pneumonaie: analysis of the clinical characteristics and outcomes of 84 patients. Chin Med J (Engl) 2007;120:136–9. [PubMed] [Google Scholar]
- 3.Chung DR, Lee SS, Lee HR, et al. Emerging invasive liver abscess caused by K1 serotype Klebsiella pneumonaie in Korea. J Infect. 2007;54:578–83. doi: 10.1016/j.jinf.2006.11.008. [DOI] [PubMed] [Google Scholar]
- 4.Sng CC, Jap AA, Chan YH, Chee SP. Risk factors for endogenous Klebsiella endophthalmitis in patients with Klebsiella bacteraemia: a case-control study. Br J Ophthalmol. 2008;92:673–7. doi: 10.1136/bjo.2007.132522. [DOI] [PubMed] [Google Scholar]
- 5.Sheu SJ, Kung YH, Wu TT, et al. Risk factors for endogenous endophthalmitis secondary to klebsiella pneumonaie liver abscess: 20-year experience in Southern Taiwan. Retina. 2011;31:2026–31. doi: 10.1097/IAE.0b013e31820d3f9e. [DOI] [PubMed] [Google Scholar]
- 6.Jackson TL, Eykyn SJ, Graham EM, Stanford MR. Endogenous bacterial endophthalmitis: a 17-year prospective series and review of 267 reported cases. Surv Ophthalmol. 2003;48:403–23. doi: 10.1016/s0039-6257(03)00054-7. [DOI] [PubMed] [Google Scholar]
- 7.Lee SS, Chen YS, Tsai HC, et al. Predictors of septic metastatic infection and mortality among patients with Klebsiella pneumonaie liver abscess. Clin Infect Dis. 2008;47:642–50. doi: 10.1086/590932. [DOI] [PubMed] [Google Scholar]
- 8.Wong JS, Chan TK, Lee HM, Chee SP. Endogenous bacterial endophthalmitis: an east Asian experience and reappraisal of severe ocular affliction. Ophthalmology. 2000;107:1483–91. doi: 10.1016/s0161-6420(00)00216-5. [DOI] [PubMed] [Google Scholar]
- 9.Chen YJ, Kuo HK, Wu PC, et al. A 10-year comparison of endogenous endophthalmitis outcomes: an east Asian experience with Klebsiella pneumonaie infection. Retina. 2004;24:383–90. doi: 10.1097/00006982-200406000-00008. [DOI] [PubMed] [Google Scholar]
- 10.Ang M, Jap A, Chee SP. Prognostic factors and outcomes in endogenous Klebsiella pneumonaie endophthalmitis. Am J Ophthalmol. 2011;151:338–44. doi: 10.1016/j.ajo.2010.08.036. [DOI] [PubMed] [Google Scholar]
- 11.Lee S, Um T, Joe SG, et al. Changes in the clinical features and prognostic factors of endogenous endophthalmitis: fifteen years of clinical experience in Korea. Retina. 2012;32:977–84. doi: 10.1097/IAE.0b013e318228e312. [DOI] [PubMed] [Google Scholar]
- 12.Yoon YH, Lee SU, Sohn JH, Lee SE. Result of early vitrectomy for endogenous Klebsiella pneumonaie endophthalmitis. Retina. 2003;23:366–70. doi: 10.1097/00006982-200306000-00013. [DOI] [PubMed] [Google Scholar]
- 13.Yang CS, Tsai HY, Sung CS, et al. Endogenous Klebsiella endophthalmitis associated with pyogenic liver abscess. Ophthalmology. 2007;114:876–80. doi: 10.1016/j.ophtha.2006.12.035. [DOI] [PubMed] [Google Scholar]
- 14.Harris EW, D'Amico DJ, Bhisitkul R, et al. Bacterial subretinal abscess: a case report and review of the literature. Am J Ophthalmol. 2000;129:778–85. doi: 10.1016/s0002-9394(00)00355-x. [DOI] [PubMed] [Google Scholar]
- 15.Scott IU, Matharoo N, Flynn HW, Jr, Miller D. Endophthalmitis caused by Klebsiella species. Am J Ophthalmol. 2004;138:662–3. doi: 10.1016/j.ajo.2004.04.051. [DOI] [PubMed] [Google Scholar]
- 16.Dodson D, Stewart R, Karcioglu Z, et al. Klebsiella pneumonaie endophthalmitis secondary to liver abscess presenting as acute iridocyclitis Ophthalmic Surg Lasers Imaging. 2009;40:522–3. doi: 10.3928/15428877-20090901-17. [DOI] [PubMed] [Google Scholar]
- 17.Kashani AH, Eliott D. Bilateral Klebsiella pneumonaie (K1 serotype) endogenous endophthalmitis as the presenting sign of disseminated infection. Ophthalmic Surg Lasers Imaging. 2011;42 doi: 10.3928/15428877-20110203-02. Online:e12-4. [DOI] [PubMed] [Google Scholar]
- 18.Sachdev DD, Yin MT, Horowitz JD, et al. Klebsiella pneumonaie K1 liver abscess and septic endophthalmitis in a U.S. resident. J Clin Microbiol. 2013;51:1049–51. doi: 10.1128/JCM.02853-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kashani AH, Eliott D. The emergence of Klebsiella pneumonaie endogenous endophthalmitis in the USA: basic and clinical advances. J Ophthalmic Inflamm Infect. 2013;3:28. doi: 10.1186/1869-5760-3-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lin JC, Chang FY, Fung CP, et al. Do neutrophils play a role in establishing liver abscesses and distant metastases caused by Klebsiella pneumonaie? PloS One. 2010;5:e15005. doi: 10.1371/journal.pone.0015005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lin JC, Siu LK, Fung CP, et al. Impaired phagocytosis of capsular serotypes K1 or K2 Klebsiella pneumonaie in type 2 diabetes mellitus patients with poor glycemic control. J clin Endocrinol Metab. 2006;91:3084–7. doi: 10.1210/jc.2005-2749. [DOI] [PubMed] [Google Scholar]
- 22.Margo CE, Mames RN, Guy JR. Endogenous Klebsiella endophthalmitis. Report of two cases and review of the literature. Ophthalmology. 1994;101:1298–301. doi: 10.1016/s0161-6420(94)31176-6. [DOI] [PubMed] [Google Scholar]
- 23.Fang CT, Lai SY, Yi WC, et al. Klebsiella pneumonaie genotype K1: an emerging pathogen that causes septic ocular or central nervous system complications from pyogenic liver abscess. Clin Infect Dis. 2007;45:284–93. doi: 10.1086/519262. [DOI] [PubMed] [Google Scholar]
- 24.Chen X, Adelman RA. Microbial spectrum and resistance patterns in endophthalmitis: a 21-year (1988-2008) review in northeast United States. J Ocul Pharmacol Ther. 2012;28:329–34. doi: 10.1089/jop.2011.0204. [DOI] [PubMed] [Google Scholar]
- 25.Okada AA, Johnson RP, Liles WC, et al. Endogenous bacterial endophthalmitis. Report of a ten-year retrospective study. Ophthalmology. 1994;101:832–8. [PubMed] [Google Scholar]
- 26.Schiedler V, Scott IU, Flynn HW, Jr, et al. Culture-proven endogenous endophthalmitis: clinical features and visual acuity outcomes. Am J Ophthalmol. 2004;137:725–31. doi: 10.1016/j.ajo.2003.11.013. [DOI] [PubMed] [Google Scholar]
- 27.Endophthalmitis Vitrectomy Study Group. Microbiologic factors and visual outcome in the Endophthalmitis Vitrectomy Study. Am J Ophthalmol. 1996;122:830–46. doi: 10.1016/s0002-9394(14)70380-0. [DOI] [PubMed] [Google Scholar]
- 28.Chiu SK, Wu TL, Chuang YC, et al. National Surveillance Study on Carbapenem Non-Susceptible Klebsiella pneumonaie in Taiwan: The Emergence and Rapid Dissemination of KPC-2 Carbapenemase. PLoS One. 2013;8:e69428. doi: 10.1371/journal.pone.0069428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pollreisz A, Rafferty B, Kozarov E, Laila E. Klebsiella pneumonaie induces an inflammatory response in human retinal-pigmented epithelial cells. Biochem Biophys Res Commun. 2012;418:33–7. doi: 10.1016/j.bbrc.2011.12.102. [DOI] [PubMed] [Google Scholar]
- 30.Meyers-Elliot RH, Dethlefs BA. Experimental Klebsiella-induced endophthalmitis in the rabbit. Arch Ophthalmol. 1982;100:1959–63. doi: 10.1001/archopht.1982.01030040939015. [DOI] [PubMed] [Google Scholar]
- 31.Becker HM, Yoganathan P, Berger AR. Endophthalmitis post complicated cataract surgery associated with Klebsiella pneumonaie. Ann Ophthalmol (Skokie) 2009;41:189–90. [PubMed] [Google Scholar]
- 32.Yarng SS, Hsieh CL, Chen TL. Vitrectomy for endogenous Klebsiella pneumonaie endophthalmitis with massive subretinal abscess. Ophthalmic Surg Lasers. 1997;28:147–50. [PubMed] [Google Scholar]