

Abstract
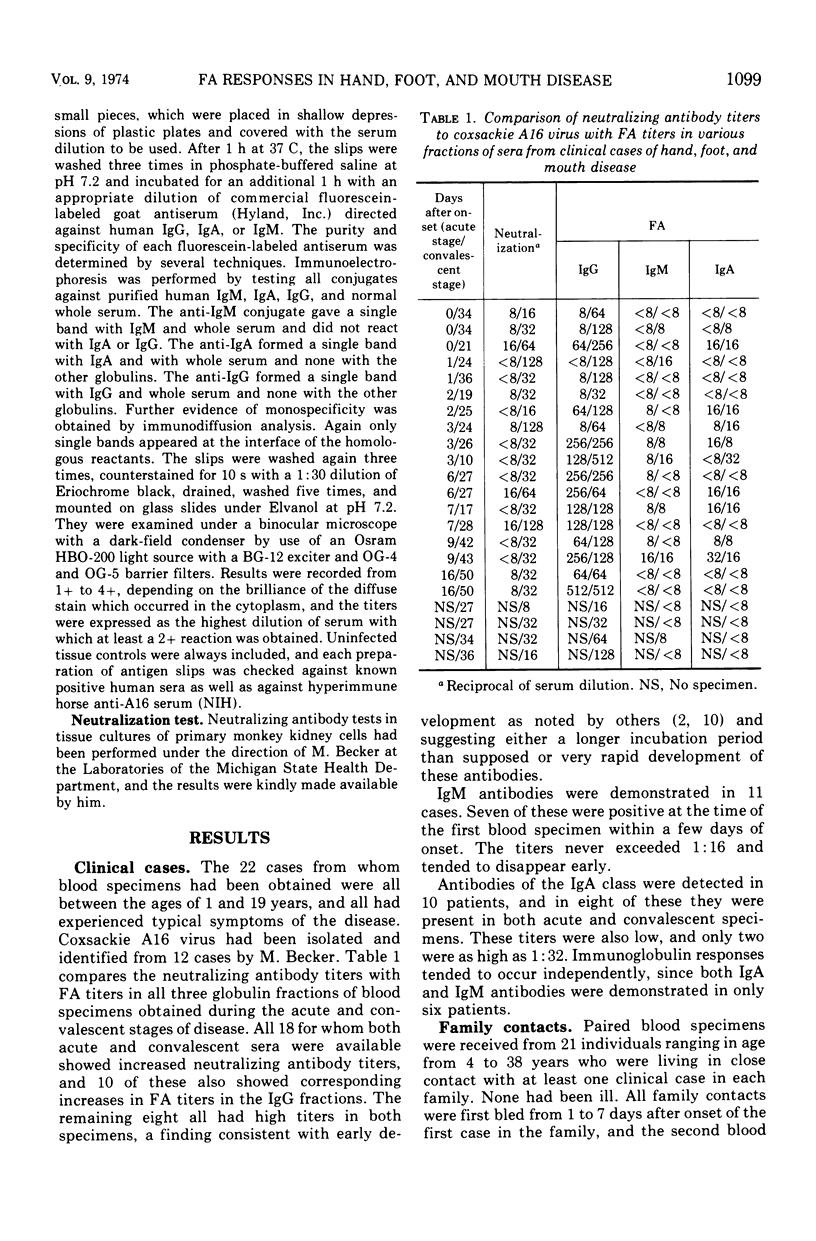
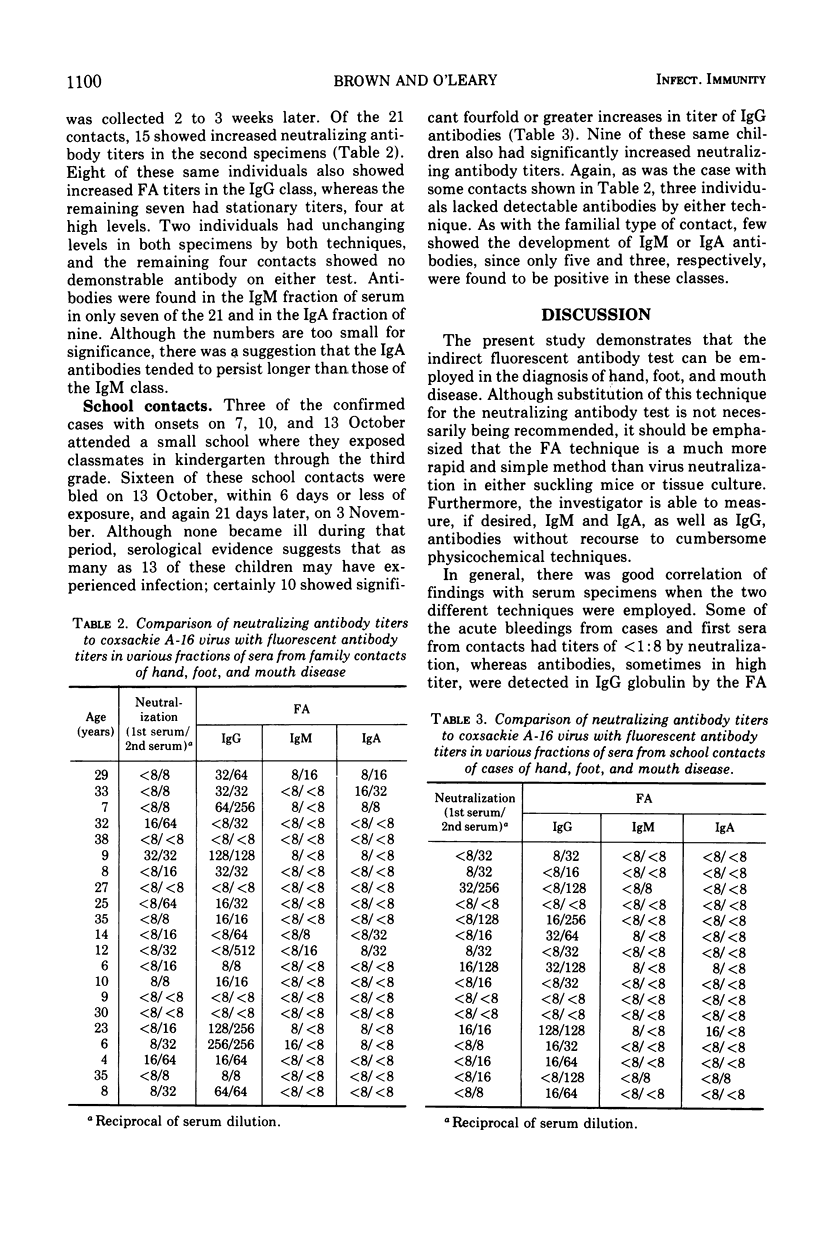
Paired sera from clinical cases, familial contacts, and school contacts of hand, foot, and mouth disease were tested by indirect immunofluorescence against a strain of coxsackie A16 virus which had been adapted to human fibroblast tissue-cultured cells. All of the 22 clinical cases developed immunoglobulin (Ig) G antibodies, and 11 responded with IgM and 10 with IgA antibodies. Seventeen of 21 familial contacts of cases showed subclinical infection as determined by development of IgG antibodies. Only seven and nine, respectively, of these had demonstrable IgM and IgA antibodies. Thirteen of 16 school classmates of three clinical cases were shown to have experienced subclinical infection by the development of IgG antibodies. Only five had antibodies in the IgM fraction, and three had antibodies in the IgA fraction. A comparison of IgG titers with those obtained by neutralization tests provides further evidence that the indirect fluorescent antibody technique represents a rapid diagnostic procedure for this disease.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ALSOP J., FLEWETT T. H., FOSTER J. R. "Hand-foot-and-mouth disease" in Birmingham in 1959. Br Med J. 1960 Dec 10;2(5214):1708–1711. doi: 10.1136/bmj.2.5214.1708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adler J. L., Mostow S. R., Mellin H., Janney J. H., Joseph J. M. Epidemiologic investigation of hand, foot, and mouth disease. Infection caused by coxsackievirus A 16 in Baltimore, June through September 1968. Am J Dis Child. 1970 Oct;120(4):309–314. doi: 10.1001/archpedi.1970.02100090083005. [DOI] [PubMed] [Google Scholar]
- Baublis J. V., Brown G. C. Specific response of the immunoglobulins to rubella infection. Proc Soc Exp Biol Med. 1968 May;128(1):206–210. doi: 10.3181/00379727-128-32979. [DOI] [PubMed] [Google Scholar]
- Brown G. C., Baublis J. V., O'Leary T. P. Development and duration of mumps fluorescent antibodies in various immunoglobulin fractions of human serum. J Immunol. 1970 Jan;104(1):86–94. [PubMed] [Google Scholar]
- Duff M. F. Hand-foot-and-mouth syndrome in humans: coxackie A10 infections in New Zealand. Br Med J. 1968 Jun 15;2(5606):661–664. doi: 10.1136/bmj.2.5606.661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- FLEWETT T. H., WARIN R. P., CLARKE S. K. 'Hand, foot, and mouth disease' associated with Coxsackie A5 virus. J Clin Pathol. 1963 Jan;16:53–55. doi: 10.1136/jcp.16.1.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Froeschle J. E., Nahmias A. J., Feorino P. M., McCord G., Naib Z. Hand, foot, and mouth disease (Coxsackievirus A16) in Atlanta. Am J Dis Child. 1967 Sep;114(3):278–283. doi: 10.1001/archpedi.1967.02090240092006. [DOI] [PubMed] [Google Scholar]
- MAGOFFIN R. L., JACKSON E. W., LENNETTE E. H. Vesicular stomatitis and exanthem. A syndrome associated with Coxsackie virus, type A16. JAMA. 1961 Feb 11;175:441–445. doi: 10.1001/jama.1961.03040060015004. [DOI] [PubMed] [Google Scholar]
- ROBINSON C. R., DOANE F. W., RHODES A. J. Report of an outbreak of febrile illness with pharyngeal lesions and exanthem: Toronto, summer 1957; isolation of group A Coxsackie virus. Can Med Assoc J. 1958 Oct 15;79(8):615–621. [PMC free article] [PubMed] [Google Scholar]